
Abstract
Although infectious diseases continue to present a major health care problem in Africa, the incidence of cancer is increasing rapidly on the African continent and this merits an increased investment in cancer research in low to medium resource settings. Esophageal squamous cell carcinoma (ESCC) has a high incidence in Eastern and Southern Africa, with late clinical presentation and a very poor prognosis. There is limited research on the molecular pathology of this cancer in Africa, partly as a result of a lack of infrastructure for biobanking and sample processing in many African countries. The aim of this study was to establish a practical and robust workflow to collect, store, and process esophageal cancer samples such that both the tissue architecture and quality of the samples would be preserved and suitable for future genomic research. We developed a workflow that allows storage of fresh biopsy tissue in sterile Eppendorf tubes containing RNAlater, an efficient RNAse inhibitor. We collected 142 ESCC biopsy samples and showed that storage in RNAlater for up to 18 months did not alter tissue morphology, thus allowing histologic assessment by experienced pathologists and determination of tumor content in each biopsied sample. DNA and RNA extracted from tissue samples was assessed for purity, molecular size, and yield. The quantity and quality of nucleic acids obtained were suitable for genomic applications, and whole-exome sequencing of DNA from tumor tissues produced sequence data with a high proportion of both usable reads and correct base calling. We conclude that this workflow may be applicable to a wide range of malignancies for future genomic research in low-resource settings.
Introduction
Cancer is a growing health care problem worldwide and particularly in Africa, which is predicted to be the continent with the fastest increase in cancer incidence over the next decade.1,2 Despite this, the focus of research in Africa has been mainly on communicable diseases, such as Acquired Human Immune Deficiency Syndrome and tuberculosis.3,4 Noncommunicable diseases in Africa have enjoyed less attention, although this appears to be changing.5,6 Health care systems in Africa are largely geared toward addressing the impact of communicable diseases, leaving them ill equipped to deal with the ever-increasing burden of chronic diseases. 7 Even among publications on noncommunicable diseases, cancer-related research is less prolific than cardiovascular-related research. 8
Esophageal cancer, particularly esophageal squamous cell carcinoma (ESCC), is considered to be endemic in certain parts of Africa.9,10 A corridor, which extends along the eastern side of Africa from Ethiopia to South Africa, is known as a high-incidence area of esophageal cancer, with ESCC as the predominant subtype. 11 Despite the high prevalence, there is limited literature on clinical studies of ESCC and of genomic profiles of ESCC tumors in Africa.12–14 In contrast, significant progress has been made in genomic research in ESCC in non-African countries, particularly in China. 15 The success of these studies is based on (1) large sample sizes, which have the power to identify the potential driver genes, that is, genes which have significant rates of somatic mutations in tumors, and (2) application of high-throughput genomic technology such as whole-exome and RNA sequencing of tumors.
South Africa (SA) and other African countries, on the other hand, face major challenges which stem largely from resource constraints. These challenges include a lack of human resources dedicated to research, inadequate infrastructure for biobanking, and most importantly, very limited funding. 16 The establishment of a biobank with nationally accepted, validated protocols, and quality control measures is still an emerging concept in Africa, and as a result, there is a lack of protocols for biobanking that are validated in this setting.17,18
Following protocols established by facilities in first-world countries, while desirable, may not be feasible in an African setting. There is, therefore, a need to develop research protocols that are functional but also feasible to follow in a resource-constrained environment. Establishing robust workflows for biobanking of esophageal cancer tissue samples in South Africa would provide essential tools to facilitate good-quality translational research and contribute to improving the quality of care for patients afflicted with this devastating disease. It could also serve as a template for the collection and processing of tissue samples for genomic research in other African cancers.
We set out to assess the feasibility of performing genomic studies in patients with esophageal cancer from centers with significant resource constraints in two provinces in South Africa by establishing procedures for collection, storage, transport, and processing of tumor samples collected from patients with squamous cell carcinoma of the esophagus. We also assessed the quality of the genetic material obtained from tissue samples with the aim to develop a workflow for sampling and processing that is feasible in this setting.
Materials and Methods
Patient recruitment
Patients were recruited from two centers in two provinces of SA, namely Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) in Gauteng, which is a high-resource setting, and Grey's Hospital (GH) in KwaZulu-Natal, a low-resource setting. CMJAH offers a range of tertiary and specialized services and also serves patients from neighboring provinces. ESCC patients recruited from CMJAH mainly reside in the urban areas of Gauteng. GH is a tertiary hospital providing health care to one of three areas in KwaZulu-Natal. The area covers the western part of KwaZulu-Natal and has a population of about three million, of which approximately two-thirds are from rural areas.19,20
Potential ESCC patients arriving for endoscopy at CMJAH and at GH were eligible for recruitment into this study. Only patients with histologically confirmed ESCC were then enrolled. The purpose of the study was explained to each patient in their native language. Informed consent was obtained from each patient, who then completed a study questionnaire before their consultation with the surgeons. A research nurse facilitated the patient enrollment, consenting, and compiling the study questionnaire at CMJAH, while the study clinician (L.F.) and research assistant facilitated the same processes at GH. Ethics clearance for this study was obtained from the Human Research Ethics Committee (Medical) at the University of the Witwatersrand (Wits) (Certificate number M170871) and from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (UKZN) (Certificate number BF270/15).
Sample collection and storage
The International Agency for Research and Cancer (IARC) protocol was used as a guideline for collecting and processing ESCC biospecimens at CMJAH and GH. 21
Figure 1 illustrates the procedure used to collect, process, and store ESCC biopsies from CMJAH and GH.
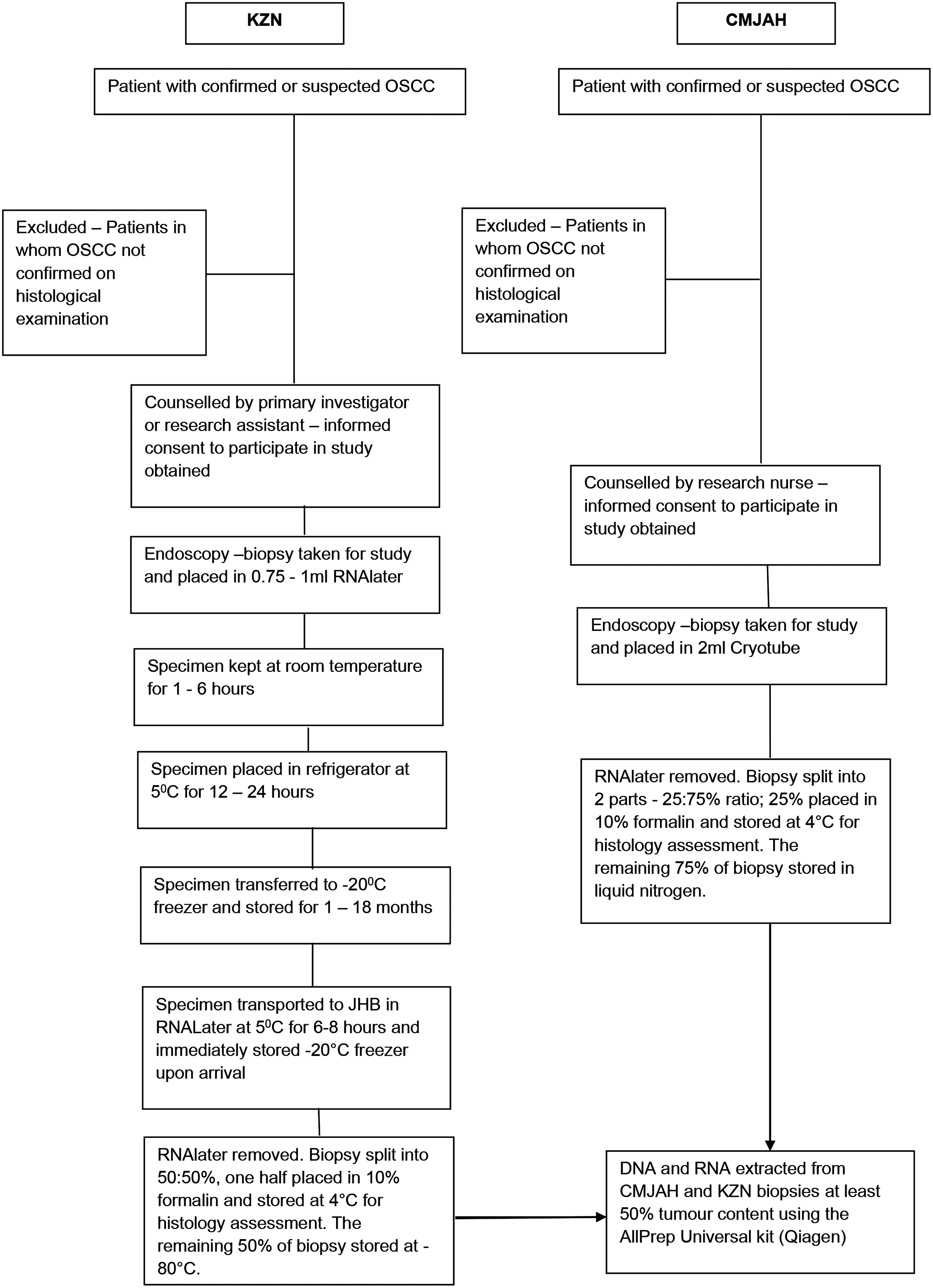
Protocols followed by the two sites for collection, storage, and processing of samples.
Routine biopsies of esophageal tissue were taken from patients suspected to have ESCC for diagnostic purposes. For this study, additional tissue specimen biopsies were obtained during the routine procedure. At CMJAH, an additional biopsy specimen in the esophagus of each suspected tumor was obtained. At GH 2–3 additional biopsy specimens from the suspected tumor were obtained.
Histology preparation for FFPE and Frozen section
Biopsy specimens from the CMJAH samples were placed in a 2-mL Cryotube immediately after extraction and the Cryotube was then immersed in a vacuum flask containing liquid nitrogen. The biopsy was then placed in optimal cutting temperature (OCT) compound (Tissue-Tek®) and stored at −80°C. Biopsies were transported in batches of 10, in liquid nitrogen, to a histopathology laboratory off-site for histological processing. Each tissue specimen was divided into two pieces (25%:75%), with the 25% portion being cut from the OCT embedded frozen block and used for histology. The remaining biopsy (75% of the OCT embedded frozen block) was stored at −80°C until nucleic acid extraction.
A different protocol was used for the GH samples. Tissue specimens were placed immediately into 0.75–1 mL of RNAlater (Qiagen) and kept at room temperature for 30 minutes to 6 hours and then stored overnight in RNAlater at 5°C before being transferred to a −20°C freezer. The specimens were stored at −20°C for 1 to 18 months, then batched, and transported at 5°C (temperature controlled) to CMJAH. Upon arrival at CMJAH, the specimens were stored at −20°C. Before processing, the specimens were taken out of the −20°C freezer, kept at room temperature for 24 hours, after which the RNAlater was removed. Each biopsy specimen was cut into two equal (50%:50%) portions in sterile conditions. One-half of the specimens were placed in 10% buffered formalin and batched for transportation to an offsite histopathology laboratory for histological processing. The other half was immediately placed in a 1.5-mL Eppendorf tube and stored at −80°C for nucleic acid extraction.
For histological processing, all tissue specimens fixed in formalin (at 6–8°C) were washed repeatedly in different levels of ethanol of increasing concentrations from 70% to 100%. Xylene was then added to each specimen, followed by paraffin wax at 60°C. The tissue specimen was then cooled to allow solidification. The tissue was embedded into a cassette and serial sections cut at 5 μm and placed on a single glass slide and stained with Hematoxylin and Eosin (H&E). The ESCC tissue specimens were sectioned in a Leica microtome cryostat using OCT compound to embed the tissue samples. Four sections of 10 μm each were mounted onto a single glass slide and stained with H&E.
All tissue sections were then examined microscopically by two experienced histopathologists. The tissue sections were evaluated for the following parameters: tissue type, tumor percentage, necrosis, inflammation, ulceration, and the presence or absence of overlying surface epithelial dysplasia. The percentage of surface epithelial dysplasia was quantified. The tumor was assessed for the degree of differentiation and the presence or absence of lymphovascular invasion. A consensus assessment was rendered for each case.
All biopsy specimens from both sites were stored in an upright position. All refrigeration equipment at the CMJAH site was monitored daily with an alarm-linked notification system. Backup refrigeration equipment was available if primary refrigeration equipment failure occurred. At GH there was no alarm system or back-up refrigeration equipment, but the refrigeration equipment was connected to a backup generator and uninterrupted power supply device.
Tissue DNA and RNA isolation
Tissue DNA (tsDNA) and tissue RNA (tsRNA) was extracted from a subset of tissue specimens with substantial tumor content. All tissue specimens were extracted using the Qiagen AllPrep® Universal Kit (Qiagen) according to the manufacturer's protocol. This kit was chosen for its ability to extract high-quality nucleic acid, which is needed for molecular applications such as next-generation sequencing (NGS). The entire remaining tissue biopsies were used for tsDNA and tsRNA extraction.
Tissue from each specimen was added to 350 μL Qiagen buffer RLT (Qiagen) and lysed at 30 mhz for 45 seconds using the TissueLyser II (Qiagen®). The lysate was pipetted onto an AllPrep DNA spin column (Qiagen) for tsDNA binding. The column was centrifuged at 8000 × RCF for 1 minute to collect the flow-through tsRNA in the collection tube. Since RNA is more sensitive to degradation, the tsRNA was extracted before the tsDNA. RNA flow through was transferred to an RNeasy spin column. Both nucleic acid specimens were extracted according to the Qiagen Allprep DNA/RNA/miRNA Universal Kit (Qiagen). The tsDNA was eluted in 35 μL of elution buffer and the tsRNA was eluted in 60 μL of buffer.
Assessment of tsDNA and tsRNA quality
Nucleic acid quantity and quality were assessed with the Qubit (Thermo Scientific), the 2100 Bioanalyser (Agilent Technologies, CA), and the NanoDrop™ 1000 (Thermo Scientific) spectrophotometer. Qubit was used to determine DNA and RNA concentrations. The NanoDrop 1000 was used to determine the absorbance ratios at 260 and 280 nm. A 260/280 ratio of >1.8 for DNA and >2 for RNA was used to indicate good purity. The Agilent 2100 Bioanalyser was used to determine RNA quality. RNA was extracted from a total of 49 biopsies, which were prioritized as having substantial proportions of tumor or dysplasia content. RNA quality was measured using the LabChip GX RNA Assay (PerkinElmer ) according to the manufacturer's instructions, using the RNA integrity number equivalent (RINe) score, which has a scale of 1–10 with 10 being the highest quality. 22 tsRNA and tsDNA samples were stored at −80°C.
Whole-exome sequencing
Exome sequencing of tumor DNA with matched germline DNA was performed on samples from six ESCC patients. A total amount of 500 ng of DNA from each sample was used as the starting material. DNA was fragmented using the Covaris shearing system (Covaris). Fragments that were generated ranged between 180 and 280 bp. Exonucleases removed 5′ and 3′ ends to ensure that each fragment had a blunt end. DNA was end-repaired after adenylation of the 3′ ends. Adapter molecules were ligated to both ends to ensure that DNA fragments were enriched in a polymerase chain reaction (PCR).
The exonic region of each sample was captured, enriched for PCR, and indexed to prepare for hybridization using the SureSelect Human All Exon V6 (Agilent Technologies). NGS of the library was performed on the Illumina HiSeq 2500 sequencer (Novogene, United Kingdom). The quality of the sequence data was assessed by calculation of the percentage of usable reads and the Phred Q score. A sequenced fragment is considered “usable” if it maps uniquely to the genome and remains after removing PCR duplicates. The Phred Q score is the quality score of a base, which is an integer value representing the estimated probability of an error. If P is the error probability, then P = 10−Q/10, and Q = −10 log10 (P).
Personnel resources
GH, KwaZulu-Natal: Patients were consented and biopsies were collected and stored by one of the authors (L.F.) or one of two additional endoscopists (see Acknowledgments section). Biopies for research were collected at the same time as diagnostic biopsies and placed in RNALater in the endoscopy suite. Samples were then placed in a refrigerator overnight and in a −20°C freezer the next morning by L.F. Thereafter, the specimens were transported in batches to the laboratory in Gauteng.
CMJAH, Gauteng: Patients were consented by one research nurse and biopsies were collected by one of three endoscopists (see Acknowledgments section). Samples were processed for histology and DNA/RNA extracted and subjected to quality control by a medical laboratory scientist (M.M.). Slides were assessed for tissue morphology and tumor content by two consultant histopathologists (R.W. and C.A.W.).
Statistical analysis
The Kruskal–Wallis nonparametric test was used to assess for differences in tsDNA and tsRNA quality (A260/280) between study sites, and between tissue storage media (RNAlater vs. liquid nitrogen). Spearman's rank-sum test was used to assess if there was any correlation between the number of days of sample storage and the quality of the tsDNA and tsRNA. The Mann–Whitney U test was used to assess differences in RNA quality score by sample storage method.
Results
A total of 142 patients were recruited into the study from the two study sites. Histological examination was performed on tissue samples from all patients, and nucleic acids (DNA and RNA) were extracted from a total of 49 samples with substantial content of tumor or dysplastic tissue as part of our ongoing study on the genomic analysis of African esophageal cancer. The total number of biopsies collected at each site with the storage method and histology profile is shown in Table 1. Important differences between protocols followed at the two different sites included storage time, temperature, and storage medium. Samples at the GH were stored for long periods (several months) in RNAlater before downstream processing, while biopsies collected at the CMJAH were stored for shorter periods (minutes to hours) in liquid nitrogen before downstream processing.
Number of Biopsies Collected at Each Site with Histology Profile, Nucleic Acid Yield, and Quality for Tissue DNA and Tissue RNA Isolated from Tissue Specimens
CMJAH, Charlotte Maxeke Johannesburg Academic Hospital; GH, Grey's Hospital; RINe, RNA integrity number equivalent; tsDNA, Tissue DNA; tsRNA, tissue RNA.
Histological analysis of the tumor content of all biopsy samples was obtained and evaluated as described in the Methods. The quality of cellular morphology from all 142 ESCC specimens from CMJAH and GH and both the frozen section and RNAlater protocols was sufficient to allow assessment of all the required parameters, including tissue type, tumor percentage, and the percentage of surface epithelial dysplasia. As shown in Table 1, the GH protocol (RNAlater) produced a higher percentage of samples with histology positive for squamous cell carcinoma compared with the protocol followed at CMJAH (frozen section/liquid nitrogen). A substantial proportion of the research biopsy samples from CMJAH (50%) were assessed as dysplasia rather than invasive carcinoma, although all patients had a clinical diagnosis of ESCC.
Representative photomicrographs of biopsy tissues from both centers are shown in Figure 2. The panels on the left half of the image (A, C, E, G) show a squamous cell carcinoma from a frozen section tissue biopsy while the panels on the right half (B, D, F, H) show, at the same set of magnifications, a squamous cell carcinoma that was placed in RNAlater. An extensive freeze artefact is apparent in images on the left panel, which restrict areas suitable for histopathological assessment. A freeze artefact with distortion of cellular detail is best shown in image E (3 thin arrows). The freeze artefact causes blurring of the epithelial/stromal interface, making assessment of invasion difficult. Also, there is no clarity of nuclear detail, which is critical for a definitive diagnosis of malignancy, and identification of mitoses is problematic. The panels on the right show islands of tumor cells with clear cellular morphology and well-formed keratin pearls (2 thin arrows in H).

Composite photomicrograph of esophageal invasive squamous cell carcinomas at increasing magnifications. Panels
Table 1 shows the yield (amount) and quality of the genetic material obtained from samples from the two centers. The yield of nucleic acids obtained from the GH samples was more than twice that of the CMJAH samples. This is likely due to the size of the biopsies obtained from GH, approximately twice the size of biopsies obtained from the CMJAH.
There were no statistically significant differences between the quality (A260/280) of tsDNA (p = 0.072) and tsRNA (p = 0.625) from the two study sites. The tsDNA from both sites was of good quality, with a mean A260/280 ratio of 1.91 and 1.96 for CMJAH and GH, respectively, and mean A260/280 ratios of 2.02 and 2.03 for tsRNA. The mean RINe scores for RNA samples for both protocols were over 8 and were not significantly different, with 43 of 49 (88%) of samples meeting the generally accepted metric (>7) required to produce high-quality RNA sequencing libraries. 22 An example of the gel electrophoresis of the tsDNA samples is shown in Figure 3. High-molecular-weight tsDNA was obtained from all samples from both study sites.

DNA samples extracted from tumor tissues on a 1% agarose gel.
DNA extracted from a subset of six tissue samples and their paired germline DNA was submitted for whole-exome sequencing to determine whether the samples were of sufficient quality for genomic studies. The quality control analysis of the sequence data is shown in Table 2. The average number of usable sequence reads across the six tissue samples was 97.4%. The average proportion of bases called with a Phred score of Q30, which indicates a 99.9% probability that the base was called correctly, was 92.6%. These metrics indicate good-quality next-generation sequence data,23,24 which was similar between samples sequenced from both sites. Furthermore, the quality of the sequence data from the tissue samples was very similar to DNA extracted from paired blood samples (data not shown).
Quality Control Statistics for DNA Exome Sequencing Data from the Tissue DNA Samples
The personnel required to execute the two protocols are described in the Methods. The additional effort required over and above that needed for a standard diagnostic workflow is taking additional biopsies at the same time as the diagnostic biopsies (endoscopist), then either freezing the research biopsy in liquid nitrogen and storing it at −80°C or placing it in RNAlater. The freezing protocol requires a trained laboratory assistant. Preparation and analysis of slides is required for both protocols and is done by histopathologists. Extraction of DNA and RNA from the tissue samples is done by a laboratory scientist. An estimate of the costs of reagents, personnel, and equipment for the two protocols in our two institutions is shown in Table 3. This shows that the running costs per sample are very similar for the two protocols. However, the frozen section protocol requires a substantial initial investment for equipment. The methods for extraction of DNA/RNA and subsequent quality control of the extracted nucleic acids are identical for the two protocols.
Cost Per Sample Breakdown for the Two Protocols. Exchange Rate of 1 USD = 13.7400 ZAR Was Used
Sample shipment when relevant is estimated at USD 365 per batch of 100 samples.
Discussion
This study was undertaken to ascertain whether genomic research could be carried out successfully in centers and study sites with significant resource constraints. In our study, one of the centers had no on-site genetic laboratory or staff, no on-site histopathology service and relied on a refrigerator/freezer, a supply of RNAlater, specimen collection tubes, and clinical staff to collect and store specimens. Despite these limitations, substantial proportions of tumor tissue could be identified in the majority of specimens on histological assessment, and genetic material (both DNA and RNA) could be extracted with acceptable quality and quantity, with the DNA being used successfully for NGS.
The first important consideration when performing genomic studies on tumor tissue is ensuring that tissue samples taken are representative of the tumor. Histopathological confirmation of tumor content in biopsy specimens is an essential step in successful biobanking. 25 Since a wide disparity in tumor content may occur between biopsies, each specimen should be evaluated by a pathologist to confirm the presence of a substantial fraction of tumor tissue before using samples for costly genomic research. 26 This is further illustrated by our study, where tumor content varied from 15% to 100% between different samples. One of our initial concerns was that biopsies stored in RNAlater for long periods (>12 months) would lose the integrity of the tissue and thus their morphology and would not be suitable for histological analysis. However, histology results were obtained successfully from all 142 ESCC specimens from CMJAH (high resource) and GH (low resource) indicating that esophageal biopsies stored for up to 18 months did not affect the integrity of the biopsies so they could still be used for histological assessment. A previous study showed that storing tissue biopsies in RNAlater or OCT compound for 24 hours did not compromise histological, immunochemical, and genomic qualities. 27 However, another study reported that 45% of RNAlater samples had poor nuclear morphology preservation, rendering pathological evaluation challenging. 28 The protocol followed for samples collected at GH, where specimens were immersed in RNAlater and kept at room temperature for several hours, then at 5°C overnight before being stored at −20°C, still in RNAlater, may offer improved protection of tissue morphology.26,29 Another important consideration when using RNAlater for storage is the size of the biopsy specimen since RNAlater has been shown to interfere with histological assessment in smaller samples.25,28
A major difference between the two centers was the method of specimen storage, with liquid nitrogen being preferred at CMJAH while RNAlater was used exclusively at GH. In our experience, the logistics used for storing and extracting nucleic acids from liquid nitrogen was more challenging compared with RNAlater. Liquid nitrogen must be available at the biopsy site, careful handling is needed to prevent injury to research staff, and a long-term liquid nitrogen storage facility must be available to maintain frozen sections. Somewhat surprisingly, we found that the quality of the nuclear morphology was superior in the RNAlater samples compared with the samples prepared in liquid nitrogen. The use of liquid nitrogen can make histological assessment more difficult since specimens are fragile and more difficult to section. 26 In our study, we found that certain samples had freeze artefacts, which can lead to an inconclusive interpretation. 30 RNAlater is also easier to use within a busy clinical environment and a low-resource setting where clinicians would not always have immediate access to refrigerators or freezers.
There was a difference in the percentage tumor content between the two centers. As shown in Table 1, specimens from GH had a substantially higher rate of squamous cell carcinoma-positive cases (63%) compared with patients from CMJAH (32%). The reason for the higher tumor content from GH samples may be related to the biopsy size, since samples from GH were larger than those from CMJAH despite the same-size forceps being used at both centers (Table 1). Another possible reason may be the experience of the endoscopist performing the biopsy. At GH, the biopsies were collected either by the primary investigator or by one of two other endoscopists, all of whom have several years of endoscopy experience. In contrast, at CMJAH, biopsies were collected by several different clinicians and in most instances by trainee surgeons with less experience, who might have been less effective in deep sampling of the core of the tumor.
Quality control of DNA and RNA samples extracted from tumor tissue showed similar A260/280 ratios between the two centers, while the mean yield of DNA and RNA extracted from GH cases was about twice as high as compared with yields obtained from CMJAH cases. This could also be explained by the fact that biopsies from GH were larger (0.5–1 cm for KZN compared with 0.3–0.5 cm for CMJAH). As mentioned previously, this is most likely due to the fact that the majority of biopsies were taken by a single very experienced endoscopist at GH (L.F.) in contrast to less experienced endoscopists at CMJAH. However, the quality and quantity of DNA and RNA from both sites were adequate for genomic studies such as NGS.
There was a marked difference in the storage time of the tissue from the two different sites (Table 1), which was necessary since samples at GH were batched for shipment to CMJAH. Our study demonstrates that despite a storage time of several months, the quality of genetic material is not compromised. This is an important consideration in centers without on-site laboratories such as GH. The absence of these facilities does not, therefore, preclude genomic research. The quality scores from the exome sequencing data are an indication that DNA extracted from tissue samples at both sites generated high-quality sequences whether biopsies were stored in RNAlater or liquid nitrogen.
The personnel resources required for the two protocols are very similar, except that a trained laboratory assistant is required for freezing samples in liquid nitrogen, whereas the biopsies can be placed in tubes containing RNAlater by the endoscopist. Also, although the use of liquid nitrogen has a slightly lower consumable cost than RNAlater, it requires a substantial initial investment for equipment. The only equipment required for storage in RNAlater by GH is a −20°C freezer, thus the RNAlater protocol has a significant advantage in settings, where there is a lack of any existing storage facilities. This is particularly common in resource-constrained settings. However, these estimates come with the caveat that they are based on our institutions and may vary considerably in other settings.
In conclusion, our results indicate that it is possible to produce good-quality samples for genomic research in an environment lacking on-site laboratory facilities geared toward this type of research without compromising important preanalytical variables that may influence results. The use of RNAlater, the availability of a standard refrigerator, and −20°C freezer, as well as collaboration with a center with the appropriate laboratory facilities and staff are essential. A recommended workflow for tissue biobanking in centers with limited resources is shown in Figure 4. We suggest that this workflow is both practical and cost-effective, and thus feasible for use in resource-constrained settings. It may also be applicable to other types of tissues and tumors, subject to the outcome of the kind of quality control assessments outlined in this study.
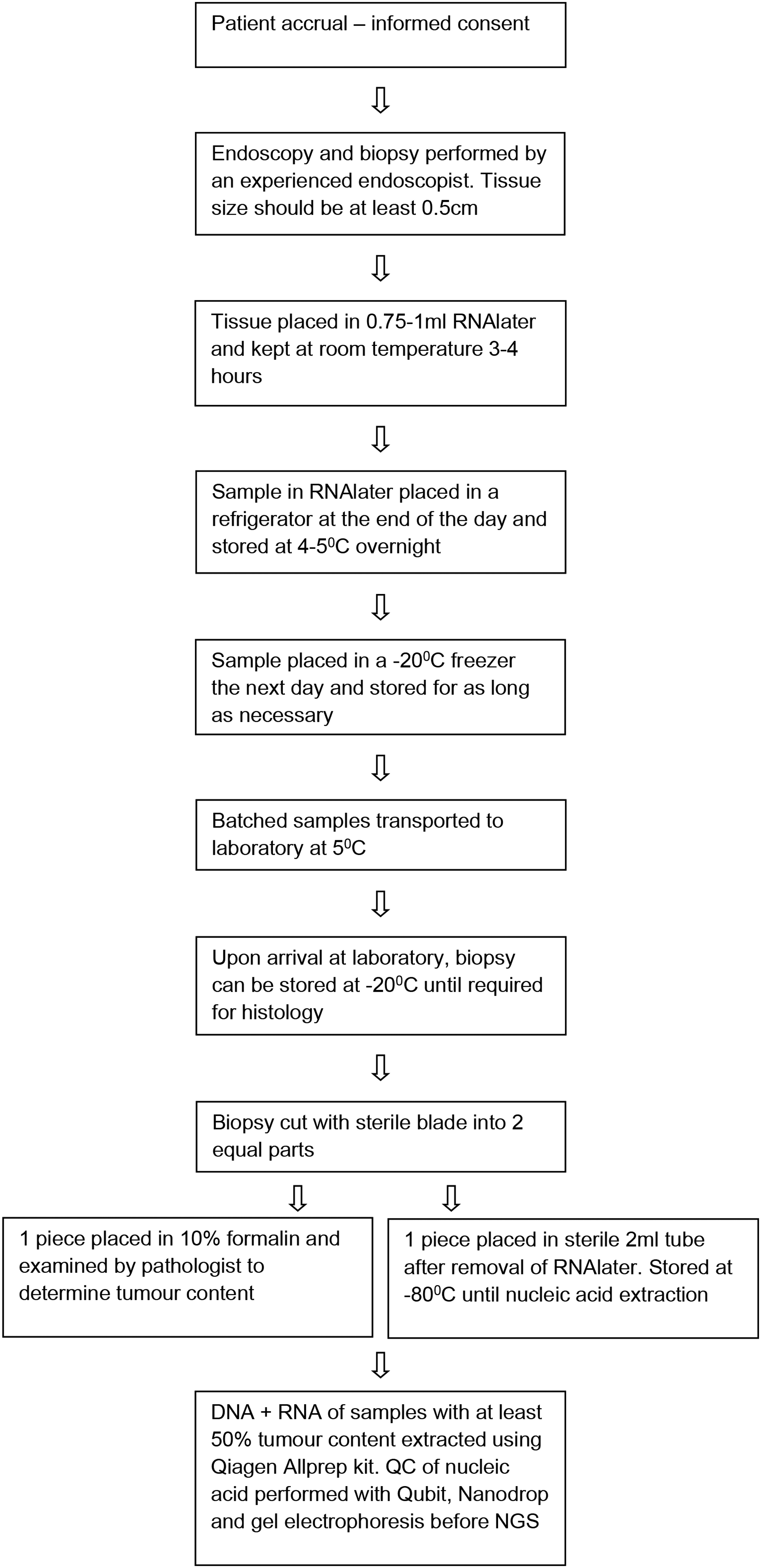
Recommended operational workflow for tissue collection in a low-resource setting.
Footnotes
Acknowledgments
The authors thank Sister Gloria Mokwatle and Surgeons Dr. U Khan, Dr. LM Prodehl, and Dr. TK Marumo for recruitment of patients at the Charlotte Maxeke Johannesburg Academic Hospital. They thank Dr. M Govender and Dr. V Nair for assistance with obtaining tissue samples at Grey's Hospital.
Authors' Contributions
M.M. received and processed samples for nucleic acid extraction, curated sample information, and contributed to the article; L.F. recruited patients, performed biopsies, and wrote the article; W.C.C. assisted with the logistics of sample collection, transport and processing, statistical analyses, and the editing of the article; R.W. and C.A.W. reviewed the histopathology of samples and the article; P.W. oversaw sample quality, database curation, and contributed to the article; M.I.P. contributed to study design, funding, and review of the article; C.G.M. contributed to the study design, supervision of the study, and the writing of the article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was supported by grant #046 (M.I.P., C.G.M., M.M., P.W.) from the South African Medical Research Council (SAMRC) with funds received from the South African National Department of Health, the Medical Research Council (United Kingdom) with funds from the UK Government's Newton Fund and GSK; Self-initiated research grant from the SAMRC (L.F.); National Research Foundation (SA) Thuthuka grant (W.C.C.); and the Cancer Association of South Africa—CANSA (C.G.M.).