
Abstract
Background:
Biobanks form key research support infrastructures that ensure the highest sample quality for scientific research. Their activity must align closely and proportionally to the interests of researchers, donors, and society. Informed consent (IC) is a central tool to guarantee the protection of donors' rights and interests.
Aim:
This study aimed to analyze the challenges of obtaining IC for biobanking in clinical settings and ways to improve this process.
Methods:
Biobank Bellvitge University Hospital HUB-ICO-IDIBELL in Barcelona received 8671 IC forms between 2017 and 2020. The mistakes that caused IC forms to be rejected by the Biobank were analyzed. In addition, interventions aimed at physicians to improve the IC process were evaluated through a calculation of the relative risk (RR). Finally, physicians who submitted samples to the Biobank, most of whom are involved in research activities, were surveyed about the barriers to collecting IC and how to improve this process.
Results:
During 2017–2020, 19.6% of IC forms were rejected. The most relevant cause of rejection was the use of outdated IC forms, followed by missing patient information or mistakes having been made by the physician. Evaluation of the rejection rates before and after interventions to improve the IC process suggests significant improvement (27.7% before interventions (January 2017–May 2018) compared to 9.6% after interventions (February–December 2020), RR 0.4 95% CI 0.34–0.47; p < 0.0001). According to the physicians, the most important barrier to collecting IC is the time constraint, and they consider digitalization as a viable solution.
Conclusions:
Our research offers a view of the less well-understood practical challenges that physicians and biobanks face when collecting IC in clinical settings. It suggests that, despite multiple challenges, continuous monitoring, training, and information programs for physicians are key to optimizing the IC process in clinical settings.
Introduction
Shifts in scientific practice and improved technological capacities have made the collections held by biobanks increasingly attractive and valuable, consolidating the role of biobanks as sources of material and data for biomedical research.1,2 In parallel to the inherent scientific objectives, biobanks also hold responsibilities toward donors and society. Because biobanks rely on solidarity to obtain samples, they depend on the citizens' trust to donate samples and on their consent to use the material for biomedical research.3,4 Accordingly, biobanks' internal procedures and governance continuously strive to align their scientific objectives with the interests of donors and society. 5 In particular, informed consent (IC) is designed to protect donors' rights, for example, their rights to information and autonomy. 6
Biobanks and the challenges of obtaining IC in clinical settings
A significant number of biobanks function in close collaboration with health care institutions, such as the Biobank Bellvitge University Hospital (HUB)-Hospital Duran i Reynals (ICO)-IDIBELL in Barcelona (https://idibell.cat/). This biobank manages samples from the HUB, the ICO, and the Hospital of Viladecans. These institutions offer secondary and tertiary care to the South Metropolitan region of Barcelona.
In general, “hospital-based” or “hospital-integrated” biobanks benefit from more straightforward access to human samples generated in clinical settings and to clinical data. Donation of surplus tissues from clinical procedures eliminates the need to expose donors to additional risks or burdens associated with obtaining the samples and optimizes health care and economic resources, among other advantages. However, the particular context, in which they are embedded, poses specific challenges to the IC process, for example, tensions can arise from the fact that the donation is requested in a clinical setting and by the treating physician.7,8 These issues go beyond the traditional challenges associated with IC, such as questions about the validity of broad consent, and about the quality, accessibility, and comprehension of the information provided to facilitate a truly informed decision-making process.5,9–12
Continuous efforts are made to improve IC forms and the IC process, but in practice the aforementioned issues have not yet been overcome. 13 Furthermore, more research is necessary to address the practical problems associated with obtaining IC in clinical settings. In the specific case of the hospital-based HUB-ICO-IDIBELL Biobank (hereinafter “the Biobank”), the challenges of obtaining IC in clinical settings were at least partially reflected by the large number of rejected IC forms, which was the starting point of this project. The main goal of this study was to identify and analyze the particular practical issues associated with the IC process in clinical settings through the evaluation of the IC forms received by the Biobank, to improve this process.
Moreover, the study examined the interventions carried out by the Biobank to improve the IC process and interpreted the results in terms of the total number of IC forms received, and the fraction of IC forms accepted or rejected by the Biobank. Finally, physicians' perceptions about the challenges of obtaining IC and opportunities to improve this process were explored.
Methods
IC forms
In Spain, National Law and the corresponding laws of the different Autonomous Communities establish the content of IC forms and offer guidelines regarding the IC process, according to EU standards.14–17 The IC form of the Biobank has been designed according to these requirements (including the General Data Protection Regulation [GDPR], Regulation [EU] 2016/679) (Supplementary Information S1).18,19 Therefore, and for the purpose of this article, we have assumed that the IC form (i.e., quality, relevance, and accessibility of the information) is adequate for the particular setting at hand. This study was approved by the Ethics Committee of the HUB.
Obtaining IC in clinical settings
Before the collection of biological samples for a clinical test, or after a medical intervention, the physician requests the patient's IC for donating the excess of biological material to the Biobank. During this process the physician provides the patient with an explanation of the objectives of the donation and the Biobank's procedures, putting an emphasis on the patient's rights. Physicians have been trained to provide patients with the IC form and the accompanying information sheet (both documents are publicly available), to give patients enough time to read the documents and to ask if there are further questions.18,19
If the patients consent, they will be given a copy of the IC form with their own and the physician's signature on it. The IC form is then sent to the Biobank where it is manually evaluated. An analysis of the quality of the IC form used by the Biobank and patients' perceptions about it are beyond the scope of this article.
Rejection rate and interventions to improve the IC process
This study analyzed IC forms from the HUB, the ICO, and the Hospital of Viladecans. An IC form was rejected by the Biobank when its legal validity was compromised, that is, the document used was outdated (this can happen as a result of the periodical updates), or when the information requested from the physician or patient was incorrect, incomplete, or missing. In 2018, the rejection rate of 2017 was quantified. As a result, interventions were carried out during 2018 with the objective of increasing donations, improving the IC process, and reducing the number of IC forms being rejected.
First, six sessions were organized for physicians at the HUB and ICO (the medical centers which donate the majority of samples to the Biobank) between June 2018 and February 2020. During these sessions, the Biobank's personnel explained to physicians the importance of effective communication with patients and how to adapt to donors' health literacy (e.g., simplifying technical and legal terms). Physicians were also shown how to fill out the IC forms to ensure legal validity, and explained the process of updating the IC form according to current guidelines.
In addition, in August 2018, an electronic information campaign was carried out to reach physicians from all associated medical centers. Physicians were reminded via email about the relevance of the communication process when requesting IC and how to fill out the forms. Moreover, they were informed about the impact of the GDPR on the Biobank's activities, and about a new version of the IC form that had been released. Although an overall improvement was observed, IC forms from a small group of physicians were still being rejected. To address this issue, 24 physicians were individually contacted by phone between June and December 2018. During the call, Biobank staff personally discussed with these physicians the importance of IC, the specific errors being made, and how to avoid them.
The effect of these interventions was assessed using the relative risk (RR, 95% confidence). The rejected IC forms received during the pre-intervention period (January 2017–May 2018) were compared to those of the post-intervention period (February 2020–December 2020). RR <1 indicates a reduction in risk, while RR >1 shows an increase in risk. Statistical analysis was performed using MedCalc v20.106 (MedCalc Software, Ostend, Belgium).
Characterization of mistakes in IC forms
To better understand the reasons behind the rejection of IC forms, errors found in IC forms received between January 2018 and December 2020 were characterized (these data are not available for 2017). Mistakes were classified as (1) use of outdated versions of IC forms, (2) error generated by the donor, (3) error generated by the physician, or (4) indeterminate error.
The use of outdated versions refers to the utilization of obsolete versions of the IC form that do not comply with current legal requirements (e.g., GDPR). Errors generated by the donor are reflected on IC forms as missing information, that is, no donor's authorization, no personal information (i.e., name, national ID number, age), or no signature. Errors reported as generated by the physician included missing signature or personal information (i.e., name, national ID number, age), and the copy of the IC form not given to the donor. Finally, a missing date was considered an “indeterminate error” because it could have been recorded by either the physician or the donor, or both. These data were analyzed using descriptive statistics.
Physicians' views on the issues associated with obtaining IC
In June 2020, a survey was sent via email to 112 physicians who had obtained IC from patients between 2017 and 2020. The survey was designed taking into account the most frequent challenges in the literature regarding the IC process, with the goal of identifying practical barriers and opportunities to improve the process in our particular context.20–22 The survey consisted of a brief description of the study's goal and six multiple-choice questions. Questions included general, personal, and professional information (i.e., age range and if they carry out scientific research), and their perception and knowledge about the Biobank and the IC process (Supplementary Information S2).
Results
Number of IC forms received by the Biobank and rejection rate
Between January 2017 and December 2020, a total of 8671 IC forms were received by the Biobank. One thousand four hundred seventy-nine IC forms were received in 2017, 2460 IC forms in 2018, 2531 IC forms in 2019, and 2201 IC forms in 2020 (Fig. 1). Of the total number of IC forms received, 19.6% (1703 forms) were rejected because of errors that compromised their legal validity. The Biobank rejected 31.4% (465/1479) in 2017, 29.0% (714/2460) in 2018, 12.2% (309/2531) in 2019, and 9.8% (215/2201) IC forms in 2020 (Fig. 2).

Number of total IC forms received by the Biobank during the pre-intervention period, the intervention period (where specific IC training was directed to physicians), and post-intervention period. IC, informed consent.
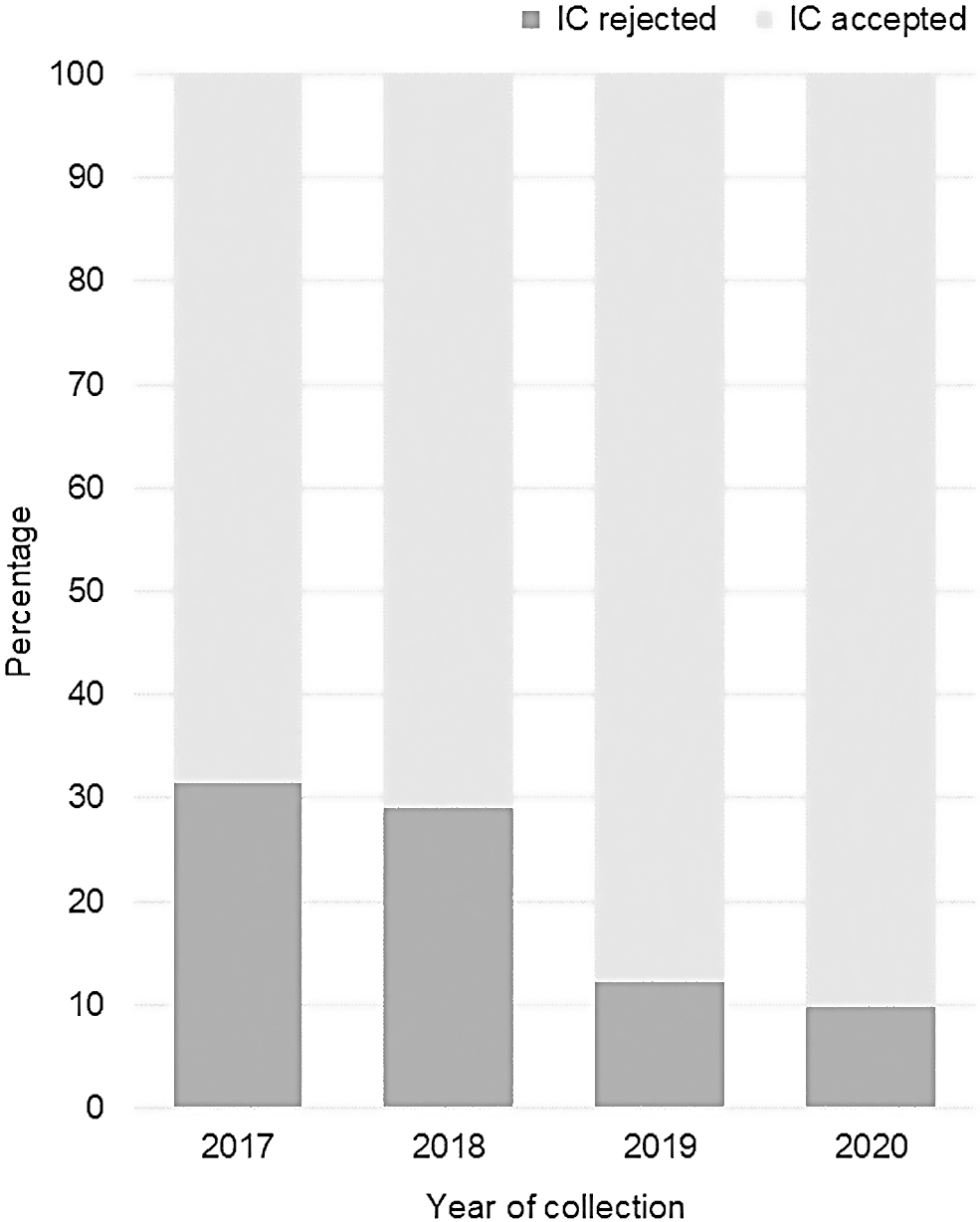
Percentage of IC forms rejected by the Biobank between January 2017 and December 2020.
Characterization of errors in IC forms
The most common error detected was the use of outdated IC forms, which constituted 58% of the total errors detected (968 of the total 1673) (Fig. 3A). The data set contained three different outdated versions dated 2013, 2015, and 2017. During the in-person sessions, the Biobank team asked physicians about the use of outdated IC forms. It was found that outdated IC forms were printed by health care staff and were kept in their offices and/or stored digitally on their computers. In addition, physicians indicated that the turnover of health care staff, for example, in the case of medical residents, represents a challenge to standardize the procedures for collecting IC, including the use of the valid IC form.
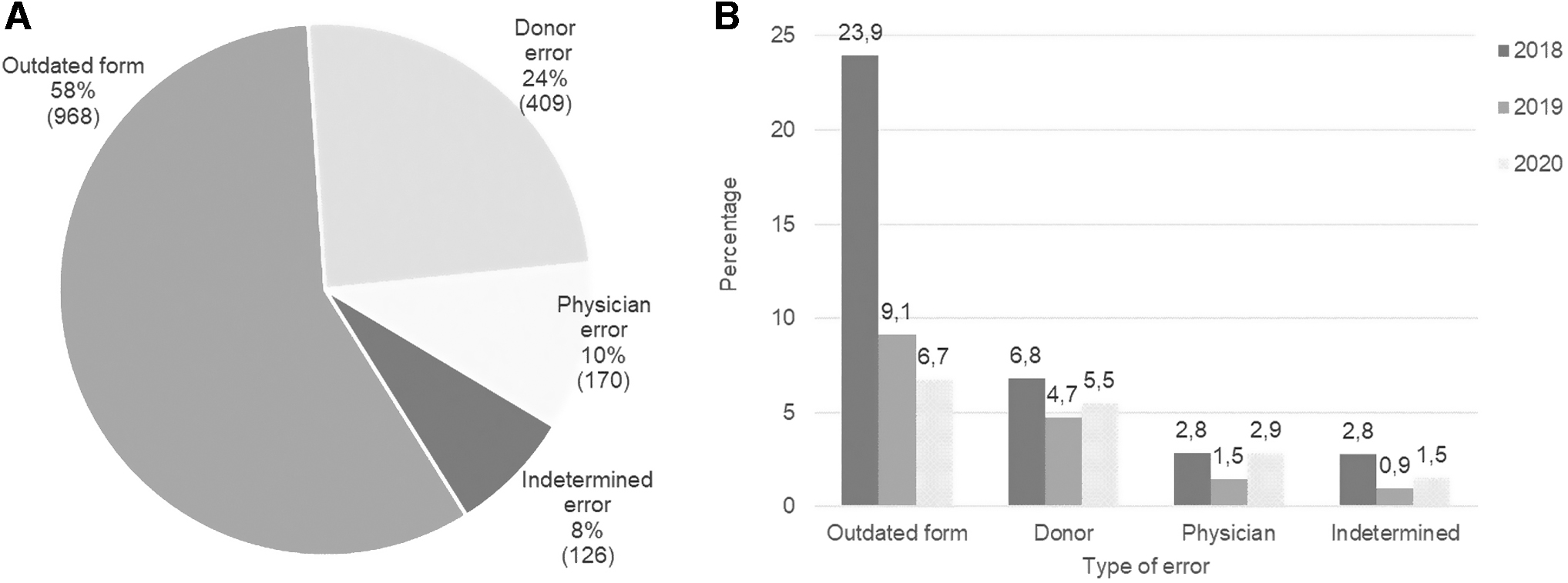
Types of errors detected in IC forms.
The Biobank's staff recognized that there were limited opportunities to train staff who temporarily rotate through the different departments and collect samples for the Biobank. The use of outdated forms decreased from 2018 to 2020 (23.9% of the total errors in 2018, 9.1% in 2019 and 6.7% in 2020).
Twenty-four percent of the total errors detected between 2018 and 2020 were made by donors (409/1673), 10% of the errors were made by physicians (170/1673), and 8% were indeterminate errors (126/1673) (Fig. 3A). Donors' mistakes caused the rejection of 6.8% of the IC forms received in 2018, 4.7% in 2019, and 5.5% in 2020. Physicians' mistakes invalidated 2.8% of the IC forms received in 2018, 1.5% in 2019, and 2.9% in 2020. Finally, an indeterminate error was found in 2.8% of the IC forms received in 2018, 0.9% in 2019, and 1.5% in 2020 (Fig. 3B). The IC forms that contained donors', physicians', and indeterminate errors decreased from 2018 to 2019, but a slight increase was observed in 2020. It is important to point out that more than one error could be made on the same IC form.
Evaluation of the Biobank interventions
The total number of IC forms received by the Biobank increased after the interventions started in 2018. In 2018, there was a 66.3% increase in comparison with 2017. This trend was maintained during 2019. In 2020, once the interventions were stopped, there was a 13% decrease in comparison with 2019 (Fig. 1).
The analysis of the impact of interventions was carried out as a comparison of two periods, the pre-intervention period (January 2017–May 2018), and the post-intervention period (February 2020–December 2020). Of IC forms, 27.7% were rejected during the pre-intervention period (644 nonvalid forms of the total 2329) compared to 9.6% (188 of the total 1961) during the post-intervention period (Fig. 4). Our results suggest that the interventions decreased the risk of rejecting IC forms by 60% (RR 0.40; 95% CI 0.34–0.47; p < 0.0001).

Percentage of IC forms rejected by the Biobank during the pre-intervention period (January 2017–May 2018) and post-intervention period (February 2020–December 2020).
Physicians' views regarding IC and the Biobank
The survey's response rate was 50.9% (57 out of 112 physicians). Of the correspondents, 40.4% were male and 59.6% were female. Of the respondents, 3.5% were younger than 30 years old, 29.8% participants aged 31–40, 43.8% aged 41–50, and 22.8% were older than 50 years. All respondents reported being aware of the Biobank's aim and activities (Fig. 5). The large majority of respondents (98.25%) carried out scientific research and all of them considered the donation of surplus tissue to the Biobank to be an important activity (Fig. 5).

General perspectives of physicians about biobanking.
The most important barrier that physicians reported facing when obtaining IC from their patients was the insufficient time during medical appointments (59.6%, 34 out of 57 respondents) (Fig. 6). Other issues include the complexity of IC forms (10.5%, 6 respondents) and the lack of clarity of the information that must be communicated to patients (14.0%, 8 respondents). Only a very low percentage of surveyed physicians considered the following issues relevant: the unwillingness of patients to donate because of the clinical context, in which the donation takes place (3.5%, 2 respondents), the inability of patients to understand the IC and related information (3.5%, 2 respondents), the lack of patient's interest to donate (1.8%, 1 respondent), and having insufficient knowledge to adequately inform patients (1.8%, 1 respondent). None of the surveyed physicians reported not being interested in obtaining IC for donating samples to the Biobank.
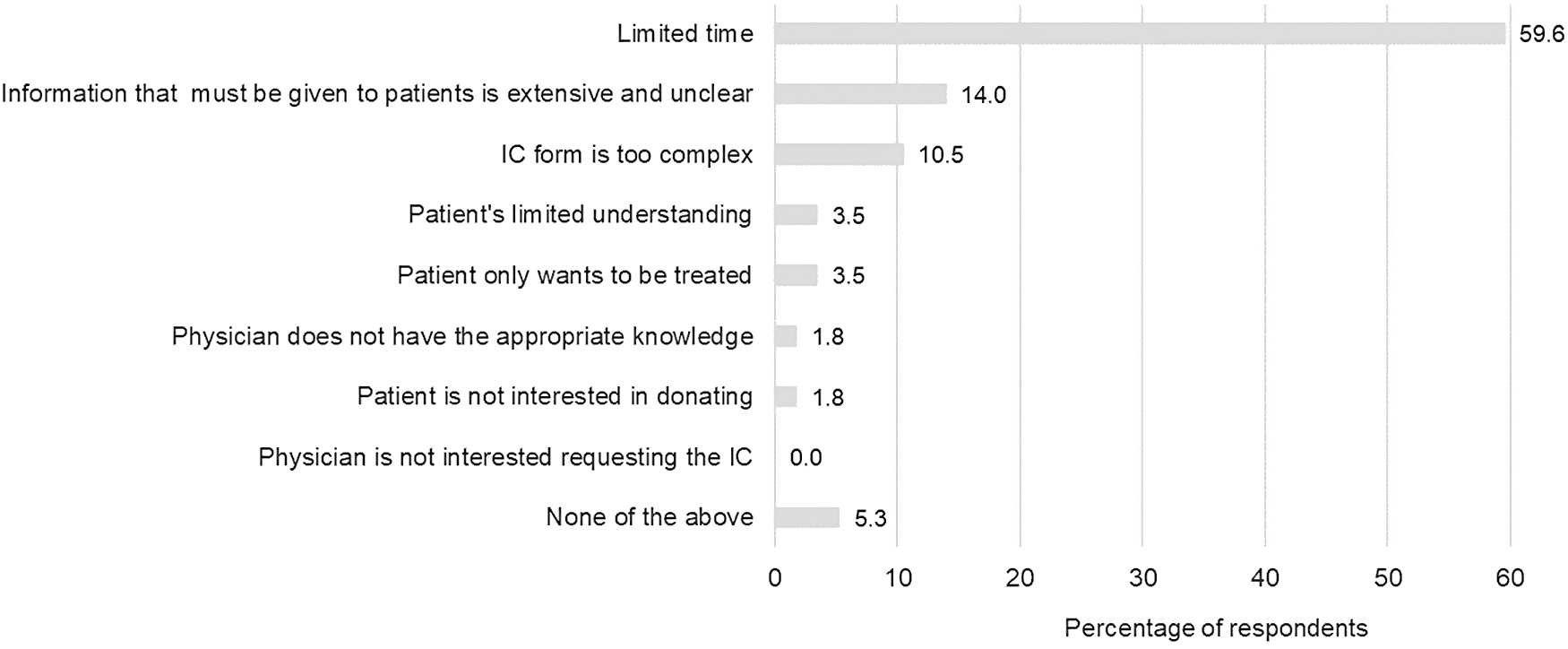
Factors that negatively impact the process of obtaining IC according to physicians.
Physicians were also surveyed about ways to improve the IC process (Fig. 7). Notably, 89.5% of respondents chose the options that suggested digitalization strategies. Specifically, 50.9% (29 respondents) preferred the option of promoting the digitalization of the IC form and its integration into the electronic health record system, and 38.6% (22 respondents) chose the option of implementing an e-consent system. Only 8.8% (5 respondents) selected the option of improving the IC process through training programs for physicians.
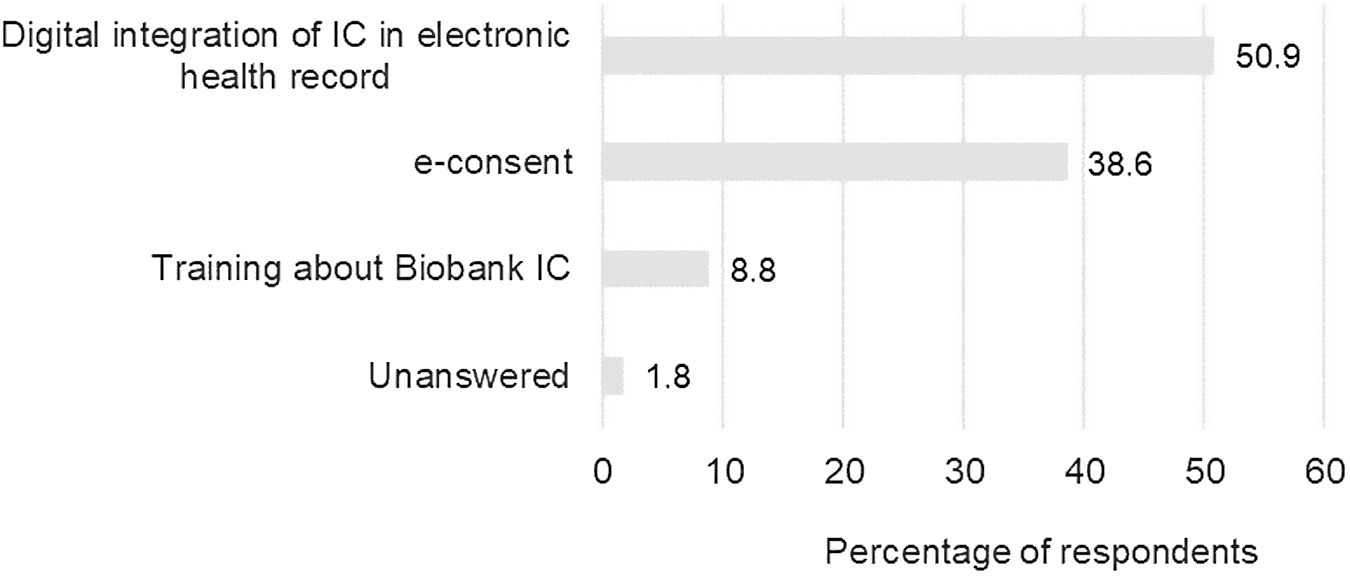
Aspects that physicians consider that the Biobank could improve to facilitate the IC process.
Discussion
A great amount of effort has been put into improving the content of IC forms and the IC process in contexts exclusively dedicated to research or clinical activities.22,23 This article addresses the less understood practical challenges of obtaining IC in clinical settings and how to solve them.
The practical setting where this research took place introduced limitations to the study design. For example, different interventions were carried out at the same time (e.g., training and information emails) not allowing us to discern the individual effect of each intervention. In addition, the IC process and the corresponding IC rejection rates may have been influenced by unknown factors and/or uncontrolled events, such as the COVID-19 pandemic, which influenced the health care system as a whole. The pandemic did not cause the complete closure of the departments that donate samples to the Biobank, but it caused the reallocation of staff, and it postponed normal care.
Nevertheless, the present study offers valuable insight into the real daily challenges of obtaining IC for research in clinical settings. Even when IC forms are designed following standard guidelines and are considered to be of very high quality, if physicians are not given sufficient support for engaging with the donors appropriately, the IC process can be strongly hindered. This is also true in settings such as this one, where most physicians carry out scientific research. Specifically, our findings contribute to the body of evidence that indicates that communication interventions can improve the IC process. 23 Our results suggest that direct engagement with and continuous training of physicians are effective strategies for increasing the overall number of IC forms received by the Biobank and the rate of IC forms being accepted.
The main cause of rejection in this study was the use of outdated versions of the IC forms. This problem decreased but persisted after the interventions. Our results highlight the challenges of a multicenter organization, which is especially relevant when it comes to fragmented health care environments constituted by multiple medical centers, such as the one in which the Biobank is embedded. They emphasize that a careful adaptation and harmonization of protocols for obtaining IC need to take place in all involved institutions, and involve all medical staff. It is, therefore, not sufficient to adopt the general guidelines solely at an administrative level.
Another significant reason why IC forms were rejected was because of mistakes made by physicians or patients, which together amounted to 34% of the total errors. These mistakes diminished from 2018 to 2019, but increased slightly in 2020. We suspect that the interruption of the interventions organized by the Biobank and the significant extra burden exerted by the COVID-19 pandemic had a combined negative effect. We were, however, not able to evaluate these assumptions within the scope of this project.
Previous studies have also referred to the complexity of improving the IC process for biobanking in health care settings.23–25 Similar to our study, Kasperbauer et al. found that the limited time of clinical consultations affected the IC process. 23 It is to be expected that physicians are limited by an environment that impedes the communication process necessary for obtaining IC. This issue is aggravated if we take into account that almost a quarter of the surveyed physicians considered that the information to be given to patients is extensive and unclear or that the IC form is complex. These challenges have been widely reported elsewhere.20,26,27
In our particular setting, physicians are not only responsible for their patients' clinical outcomes, but are also responsible for the IC process. For this purpose, they need to establish in a short time an efficient dialogue, ensure that donors have understood the provided documentation and verbal information, and confirm that the IC form is filled out correctly. We suspect that patients' mistakes are probably avoidable through an improvement of the communication process. This point needs to be followed up, taking into account patients' views. 28 Further research is also necessary to determine if the documentation can be improved and if the communication process has been sufficient from the patient's point of view.
Despite the physicians' perception that training is not the most desirable intervention to improve the IC process, our results suggest that this type of intervention positively impacts the total number of IC forms received by the Biobank and reduces the rejection rate. These findings are similar to those reported by Simon et al. where face-to-face interventions increased confidence, understanding, and enrollment in Biobank research. 29 For generating a trustworthy IC process in clinical settings, it is crucial that physicians are well informed about biobanking activities and the IC process, and to provide them with enough time during the clinical consultation. 30
In our study, physicians regarded digitalization as the most attractive option to improve the IC process. Our interpretation is that given the high workload, digitalization is seen as a way to save time by automating at least part of the process and making the IC form readily accessible. In addition, automatic data validation strategies can be built (e.g., detection of missing fields) to diminish mistakes. From the Biobank's perspective, digitalization could also ease the administrative burden. Most physicians preferred to integrate the IC form with the electronic health record, allowing them to check if patients have previously provided IC and preventing unnecessary reconsent.
The second choice of the surveyed physicians was to adopt a digital consent system (e-consent), which would allow donors to easily change their preferences. e-consent may promote the autonomy and involvement of donors, providing patients with the opportunity to play a more active role in the donation of their samples and data for research. 31 Despite the advantages, the integration of IC for biobanking or e-consent into the electronic health records would require overcoming significant technical and organizational challenges, especially when implemented in multicenter health care environments (e.g., interoperability and management), in addition to its costs and accessibility. 32 These options should be carefully considered by all the involved health care institutions.
Recommendations
Based on the findings of this study, a set of recommendations were drawn. These need to be carefully adapted to other contexts, for example, take into account that the majority of physicians who participated in this study carried out scientific research.
Invest in person-to-person interventions
Person-to-person interventions such as group trainings, digital information campaigns, and one-to-one coaching of health care staff can significantly improve the IC process in clinical settings. We recommend that biobanks invest in continuously carrying out these types of activities. Challenges regarding this recommendation are inherent to the problems commonly faced by health care systems, which include understaffing, increasing costs, and higher workloads. The Biobank has very little influence over these factors, but can help physicians optimize their time and communicate with their patients more effectively.
Invest in the evaluation of interventions
The decision of biobanks to carry out information or training campaigns involves costs. To optimize resources, it is necessary to understand which types of interventions are most effective for the particular context at hand, and when and/or where they are necessary. The evaluation of the interventions' effectiveness is necessary to guide an optimal intervention plan.
Invest in the standardization of the IC process across all institutions involved
Effective standardization procedures may come with a cost, but will optimize the IC process in the long run. Digitalization may be a valuable tool in this respect, especially when biobanks' IC is acquired in multiple medical centers. For example, the incorporation of the IC form into the electronic health record can prevent health care staff from using outdated versions and may save time and improve the IC process.
Conclusion
IC is a key pillar of scientific research with human subjects, samples, and/or sensitive information. It is probably not surprising that the IC process is constantly adapting to scientific, technological, and societal changes. Striving to establish the best means to obtain IC is therefore a difficult task that must be accompanied by constant evaluation and improvement of the quality of IC forms and how IC is obtained. To our knowledge, there is very limited published data similar to those presented in this article, where the rejection of IC forms for donating surplus of clinical samples and interventions to improve the IC process were analyzed. This work is an important contribution to the wider discussions about how to optimize and improve the collection of IC and specifically, IC for biobanking obtained in clinical settings.
Footnotes
Acknowledgments
We want to particularly acknowledge the Biobank colleagues and clinicians for their contribution to this study and the Biobank HUB-ICO-IDIBELL (PT20/00171) for its support. The authors express their sincere gratitude to prof. Dr. F. García López, Carlos III Health Institute, for his valuable input and discussions.
Authors' Contributions
Both authors contributed to and made critical revisions related to the intellectual content of the article. L.A.E. contributed to the collection of the data. L.A.E. and M.V.Q. contributed to the analysis of data, and drafted and revised the article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was funded by the Spanish Biobank and Biomodels Platform, and the Carlos III Health Institute (PT20/00171).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.