
Abstract
In 1984, the National Institute on Aging developed the Alzheimer's disease centers program. The main goal of these centers is to advance the understanding of Alzheimer's disease and related dementias (ADRD) through comprehensive patient evaluations and cutting-edge research in pathology, laboratory medicine, education, and scientific discovery. The neuropathology core of the Alzheimer's Disease Research Centers (ADRCs) collects postmortem brain tissue from consented donors ranging from cognitively normal individuals to those with late-stage dementia, whose samples and data can be shared around the world to further advance knowledge, diagnosis, and to eventually find cures for ADRD. Although recommended guidelines for biorepositories exist, we aimed to understand the current practices within neuropathology cores across the ADRCs. A survey was developed that focused on information related to sample processing methods, biospecimen requests, financial costs related to the repository, and data management. This survey was distributed to 28 current and former ADRC neuropathology cores. The survey obtained a response rate of 82% (23/28). Although most centers were consistent in responses related to sample processing and storage, they varied widely in processes by which neuropathological samples are shared and cost recovery mechanisms. The results of this survey provide benchmark data on practices within neuropathology cores across ADRCs and the overlap with biorepository best practices. Future studies focused on understanding factors that may influence current practices (such as available funds and personnel) are need to aid in minimizing barriers to optimally follow best practices. Sharing these data among ADRCs will allow for improvement in workflows and working toward cures for ADRD.
Introduction
While the concept of biobanking has been around for >100 years, the term first came about in 1996 and the concept has progressed since, with sequencing of the human genome and the increase in demand for well-annotated properly preserved human specimens.1–4 Biobanking in the United States has drastically changed over time; starting with individual biorepositories at universities for specific populations to more centralized or government-supported repositories.5,6
With research and biorepositories becoming more and more globalized, it is critical that specimens are processed and maintained in a standard way to reduce sources of variability as well as to preserve the integrity of the specimens.7,8 Throughout the years, there have been guidelines put forth by different entities such as the National Institutes of Health's (NIH) National Cancer Institute (NCI).9,10 The NCI first published its NCI Best Practices for Biospecimen Resources in 2007, and has revised it multiple times to stay current with practices, and to include new sections on topics such as conflicts of interest and informed consent. 9 This document has established a framework for maintaining a biorepository.
In 1974, Congress passed the Research on Aging Act, which led to the new National Institute on Aging (NIA), making Alzheimer's disease and related dementias (ADRD) a top priority.11–13 In response to a congressional directive, knowledge of ADRD pathophysiology emerging from work funded by the NIH and others, and subsequent increases in research funding, allowed for the NIH's NIA to establish the first federally funded Alzheimer's Disease Research Centers (ADRCs) by 1985; currently there are >33 ADRCs.11,14–17
The ADRCs seek to advance the understanding of ADRD through comprehensive clinical evaluations and translation of cutting-edge research into improved diagnosis, treatment, and a way to prevent ADRD. 18 ADRCs are expected to contribute to development of shared resources that support ADRD research. 19 All data collected through the ADRCs are gathered into a database, developed and maintained by the National Alzheimer's Coordinating Center (NACC), which was formally established in 1999 by the NIA.20,21
One core component of the ADRCs is the neuropathology core. Historically, the aims of the neuropathology core related to collection, diagnosis, and distribution of postmortem brain tissue from donors ranging from cognitively normal individuals to those with late-stage dementia. Biomarker cores were officially incorporated into ADRCs in 2018, and there has been increasing effort for in vivo collection of blood samples, cerebrospinal fluid, and DNA for genomics.22,23 The data from these biorepositories can be shared among qualified investigators around the world to further advance knowledge, diagnosis, and eventually find a cure for ADRD. 24 Furthermore, studies have focused on deeper phenotyping of ADRD to have a foundation for precision medicine approaches (see review 25 ).
Guidelines for uniform data collection of ADRD within ADRCs have been established, including the most current guidelines for neuropathological assessment published in 2012 from the National Institute on Aging-Alzheimer's Association.26–29 In addition, each ADRC has a unique focus (Supplementary Table S1); for example, UC Davis (UCD) focuses on ethnoracially diverse brain specimens as a result of tailored recruitment efforts across multiple locations throughout Northern California.30,31 Consequently, tissue samples from cases having a variety of ethnoracial backgrounds may be ample at the UCD-ADRC but this diversity may be sparse in other locations (e.g., Kentucky, USA); this can be due to population differences in addition to recruitment methods.32,33
This note is especially important given the current scarcity of autopsy materials from patients from diverse backgrounds, including diversity in socioeconomic, cultural, and ethnoracial status (see review 34 ). Depending on research questions and focus, researchers may gravitate to certain ADRC; for example, there can be differences in genetic marker distribution in select cohorts. 35 To track specimens and assure documentation of resource origins (i.e., listing specific grant funding in publications), a specific set of standards needs to be maintained and/or implemented. 36 Although recommended guidelines for biorepositories exist, we aimed to further understand current practices within the neuropathology cores across ADRCs, to ultimately provide a standardized guide to best practices for optimizing and maintaining a brain bank biorepository. 37
Materials and Methods
To assess current biorepository practices across ADRC neuropathology cores, a survey was developed, containing 13 questions, focused on items related to the following overall topics: sample processing, sample sharing, data, storage, and financial costs (Supplementary Data). The survey was converted to a digital format, using SurveyMonkey.com (Momentive.ai, San Mateo, CA), for ease of answering. This survey was done in accordance with the UCD Institutional Review Board (IRB) protocols and was determined to be exempt, since it did not involve human subjects.
The survey was electronically distributed to the listed neuropathology core leaders of 28 current and past ADRCs (2019) (Supplementary Table S1), on April 23, 2019, and was closed for responses on May 3, 2019. Responses for questions 2, 5, 7.2, and 10 were not mutually exclusive. Data were compiled and analyzed using Prism (GraphPad Prism 9.2.0). Figures were created using (BioRender.com).
Results
The survey obtained a response rate of 82% (23/28). The survey covered five main categories of running and maintaining a biorepository: sample processing, sample sharing, data, storage, and financial costs (Fig. 1). The surveyed centers were mostly in agreement with responses related to sample processing and storage, whereas they varied widely in processes by which neuropathological samples are shared and data are quality checked and managed as well as cost recovery mechanisms.

Survey results and question categories. Survey questions covered five main categories of biorepository management: sample processing, sample sharing, data, storage, and financial costs (complete survey questions are given in Supplementary Data). The results of each survey question (numbered according to order in the survey; in the top left corner of each corresponding pie chart) are shown in each pie chart. FFPE, formalin-fixed paraffin-embedded; MTA, material transfer agreement; QC, quality control; QR code, quick response code.
For example, the majority of ADRC neuropathology cores perform an integrity check on their tissue (20/22) and follow a specific dissection protocol for their center (23/23). Differences were noted in the standard protocol for brain processing after removal with 13 of 23 respondents stating that one hemisphere of the brain is placed in a fixative solution and the other hemisphere is frozen, whereas 9 of 23 respondents said they followed a different processing protocol.
In addition, the neuropathology core brain tissues were generally available to other researchers as formalin-fixed paraffin-embedded (FFPE) cut sections on glass slides (22/74), FFPE blocks (13/74), frozen as blocks (22/74), and/or fixed in cryoprotectant (9/74); although these responses were not mutually exclusive (i.e., totals being total responses submitted), they show the variety of ways samples are distributed. With regard to the sharing tissues, 14 of 21 neuropathology cores require a material transfer agreement (MTA) for external researchers, whereas 4 of 21 require an MTA whether the researcher is external or internal—3 of 21 did not require one at all.
There were similar differences in data management software with 12 of 23 respondents saying they use Excel, 7 of 23 use OpenSpecimen (biobanking laboratory information management systems; Krishangi, LLC, St. Louis, MO), 1 of 23 uses Freezerworks (biobanking laboratory information management systems; Dataworks Development, Inc., Mountlake Terrace, WA), and 7 of 23 said they use a different software entirely. Hence, the main data management software was Excel. The greatest difference between ADRCs was how data are quality controlled.
In total, 15 of 57 respondents said their ADRC had dedicated personnel to manage data, some centers also denote to have internal controls such as flagging incompleteness (11/57), data cleansing (9/57), flagging inconsistencies (8/57), restricted inputs (8/57), field redundancy (4/57), and 2 of 57 respondents said they have another form of checking data; again, although these responses were not mutually exclusive (i.e., totals being total responses submitted), they highlight the diversity in data management controls.
Lastly, there was high agreement among the ADRC responses as to how samples are stored. 22 of 23 respondents denoted their neuropathology core freezers had emergency backup power. Only one respondent (1/23) said they did not have backup power for freezers in case of an emergency; in addition, 4 of 31 respondents said they use off-site freezers, 3 of 31 said they use liquid nitrogen, and 5 of 31 said they use an alternative method—again these responses were not mutually exclusive. With respect to cost recovery for sharing samples, 13 of 23 respondents said their ADRCs did not have a method in place.
Discussion
In 2020–2021, the NIA convened multiple working groups to update the guidance on best practices for the ADRCs—these best practices are intended to be a resource for new ADRCs and for centers venturing on a new line of research. 37 Our survey focused on select topics within the ADRC best practices, which was published after our survey was conducted. Many factors may influence current practices (available funds, personnel, etc.), of which additional research is needed to fully understand where each ADRC can improve their workflows and continue to improve standardization of each biorepository in a sustainable feasible manner.
The compiled results from this exploratory survey provide benchmark data on the current biorepository practices across ADRCs. These results revealed ADRCs were most similar with respect to sample processing and sample storage; the majority of ADRCs fix one half of the brain, whereas the other half is frozen, and keep their freezers on backup electrical power. However, the biggest difference was with sample sharing; samples are shared in multiple forms ranging from FFPE blocks, FFPE cut slides, fixed cryoprotected tissue, flash frozen blocks, or in some additional form.
This variation of sample deployment likely reflects differences in available resources, as well as the mission and goals of the research being done—this practice is common and well documented in the NCI Best Practices. 9 In addition, there was variation in administrative items associated with sample sharing—varying lengths in MTAs and whether or not they are executed and to what extent. Lastly, more than half of the polled ADRCs did not have a cost recovery system in place for sample requests; this is a well-documented dilemma of running and maintaining a biorepository. 38
Historically, neuropathology cores of each ADRC are funded through NIA P30 or P50 grants over 5-year cycles. Before 2019, each ADRC could request a budget of up to $1.1 million dollars in direct costs for the first year to cover all cores including not only the neuropathology core, but also administrative, clinical, data management and statistics, outreach, and recruitment, as well as the research and education component. 39 The year 2019 was the start of a new cycle for ADRCs, where applications could request a budget of up to $2 million in direct costs per year, and with this increase in potential budget also came the addition of biomarker cores.
Funding for each core can vary among ADRCs—in 2019 (the year the survey was conducted), using https://reporter.nih.gov and having key words of “Alzheimer's Disease Research Center,” “Neuropathology,” “P30,” “P50,” and “2019,” revealed 18 ADRCs neuropathology cores' total cost per year ranged from $134,208 to $419,138, with the average being $240,149 per fiscal year. This large range may be due to some ADRCs being underneath the new structure, whereas some remained on the older structure. Funding for neuropathology cores not only needs to cover materials and supplies related to neuropathology diagnoses, collection, and distribution of materials, but also staffing.
Within the ADRC's best practices, it is recommended for brain donation to have an on-call autopsy coordinator(s), autopsy technician(s), and tissue bank technician(s), so collection can occur as rapidly as possible after death. 37 With respect to case volumes of neuropathology cores, in 2019, 737 ADRC participants passed, with the average number of deaths across ADRCs being 23 (min = 3, max = 54). Of the 737 participants, 456 had a neuropathology form submitted (which included detailed information on pathological diagnoses as well as available inventory on each case), with the average number of forms being 14 (min = 1, max = 37) (communications with the National Alzheimer's Coordinating Centers, May 2022).
The overall workflow of a biorepository, as suggested by Vaught and Lockhart, can be broken down into three main categories: Technical best practices (collection, processing and storage guidelines, management, informatics, economic recommendations, and quality assurance), Ethical, Legal, and Social Issues (governance and custodianship, informed consent, protection of participant privacy, and intellectual property), and Challenges Ahead (international collaboration and standardization). 36 These criteria should be outlined in detail for a biorepository and altered to meet their specific needs. A reduced visual form of this is shown in Figure 2.
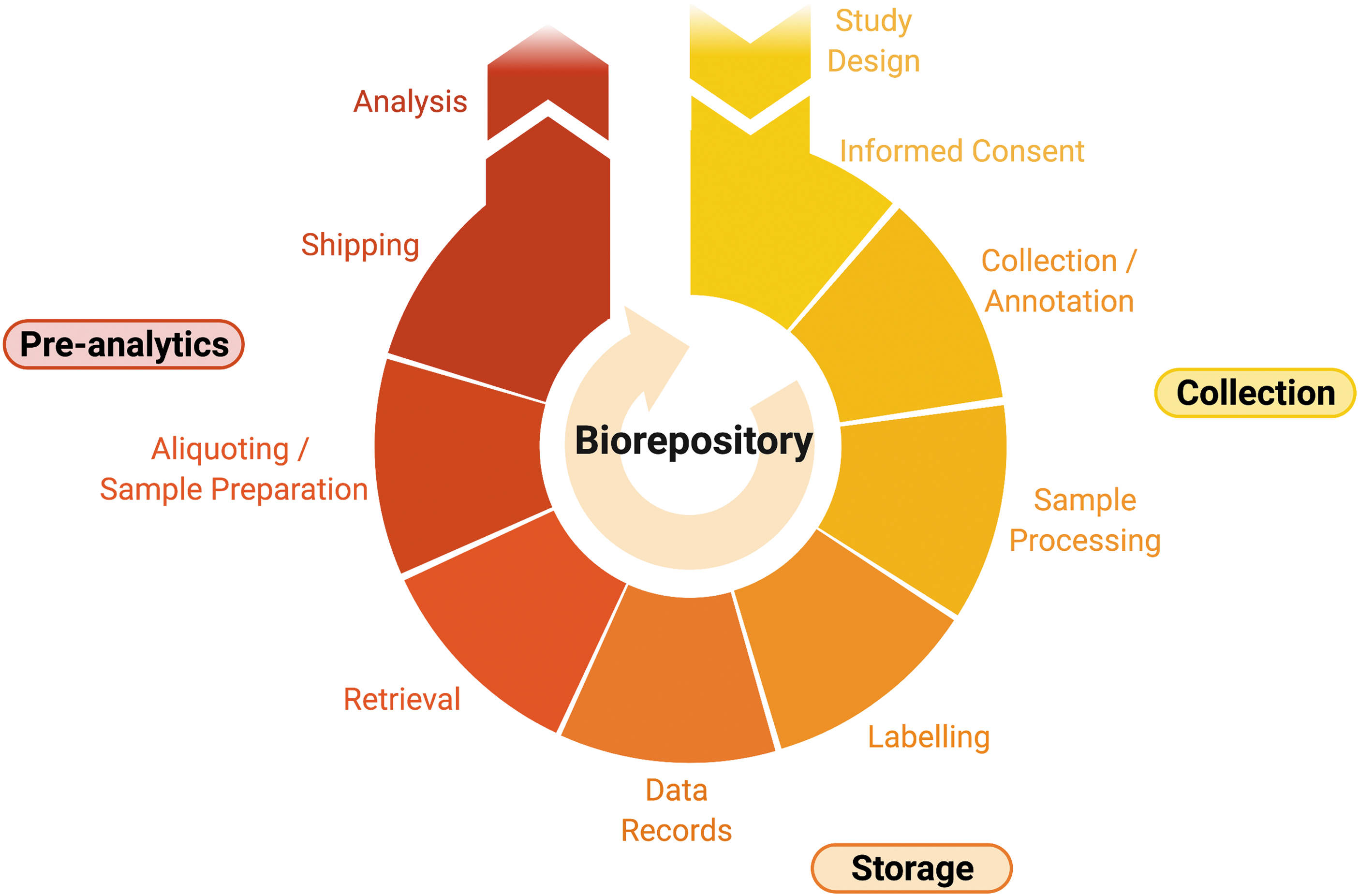
Biorepository workflow. A simplified version of the overall workflow of a biorepository, as suggested by Vaught and Lockhart 36 —identifying critical stages throughout the process of maintaining a rigorously maintained biorepository (figure created with BioRender.com).
Furthermore, although there are many sources and guidelines for biorepositories, such as accreditations like those put forth the College of American Pathologists, these may not be feasible to implement within ADRCs given the amount of documentation involved and their research focus. 40 ADRC neuropathology cores mainly revolve around postmortem procurement of brain specimens and may not procure/process specimens from living patients (although some may serve in partnership with clinical services for biopsies, etc.), hence there may not be a need for certain accreditations.
Given that research is a focus of ADRCs, extensive external standards may not be practical to obtain and maintain. There are guidelines, such as those put forth by the NIA-AA related to diagnoses and through steering committees within the NACC.28,29,37 Even with current guidelines, although it is stated for specific stains, specific antibodies/protocols are not given, thus there is room for interpretation given the nature of each neuropathology core's specific research questions.
Without high-quality highly characterized human tissues for translational research, the tissues being studied can lead to poor quality results, the results can affect research leading to conclusions that are misleading or artifactual, resulting in publications that may not be reproducible. Biomedically relevant data and materials are critical to academic, commercial, and clinical-driven research, aimed at diagnosing, treating, and preventing rare and common human diseases. Advancing the diagnosis, treatment, and prevention of diseases requires access to well-structured and rigorously maintained biospecimen collections, and thus it is critical for biobanking procedures to be standardized, yet maintain some flexibility to allow for incorporation of innovation.
This dilemma was strongly recognized as part of the problem and cause for the “Valley of Death” 6 or the great divide between biomedical research and getting treatments to patients; so much so that institutions like the NCI formed the Office of Biorepositories and Biospecimen Research to coordinate and develop tissue resources and capabilities. 41 The need for access to high-quality and well-characterized tissues is not unique to cancer groups, but has been widely cited by others as well (neuroscience research, genomics, personalized medicine, etc.).6,42 Lastly, the biospecimens should only be available for scientifically and ethically appropriate research that is expected to yield relevant discoveries to increase knowledge and enhancing breakthroughs.
Conclusion
Our survey served to generate current benchmarks within ADRCs, and did not delve into the underlying reasons for each ADRC's workflow. Some factors such as diversity in available resources within instructional/ADRC structures (staffing/space) as well as research interests may play a role; more research is needed to understand these divergent approaches. To further knowledge and biomedical research, it is critical that biorepositories are not only in existence, but that they are also rigorously maintained, through accurate and detailed phenotyping, and continuous funding. Biorepositories are critical to the success of biomedical research, and the development of treatments for not only ADRD, but also for a wide variety of other diseases (cancer, rare disorders, etc.).
Footnotes
Acknowledgments
The authors thank the ADRCs' neuropathology cores for their participation in this endeavor. In addition, we thank Kathryn Gauthreaux from the NACC for assistance with collecting metric data on all ADRCs in 2019. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any public health agency of California or of the U.S. government.
Author Disclosure Statement
No potential conflicts of interest relevant to this article exist.
Funding Information
This study was supported by the NIA of the NIH under Award Nos. AG062517, AG010129, and AG072972, the University of California Office of the President (MRI-19-599956), and supported by the California Department of Public Health Alzheimer's Disease Program with partial funding from the 2019 California Budget Act.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.