
Abstract
Background:
Parallel to the rapid advancement of biological and information technologies, the role and forms of biobank research have been constantly changing. The ethical, legal, and social implications of consent in biobank research are in a state of flux. This study aimed to clarify current Japanese public preferences regarding the consent model and explore how public attitudes are determined.
Methods:
We conducted an online, population-based quantitative survey among Japanese residents aged between 20 and 69 years. Statistical analyses consisted of univariate and multivariate logistic regression.
Results:
Of the 1580 respondents, 60.9% preferred autonomy-based consent (specific or dynamic consent) and 23.9% preferred broad-type consent (opt-out or broad consent). Marital status, gender, and privacy concerns were significantly associated with the preference for a consent model.
Conclusions:
Our results demonstrated the public's current preference for autonomy-based consent, including dynamic consent. However, our findings also revealed that approximately half of the respondents considered broad consent as somewhat preferable.
Introduction
Biobank research has been gaining popularity worldwide since around the year 2000. This aspect of bioscience research infrastructure plays an important role in the development of medicine, from a basic understanding of diseases to developing new drugs, and has recently become a driving force for personalized medicine in particular. 1 However, because of the innovative and sometimes controversial nature of biobank research, the issue of consent inevitably arises. Conventional study-specific informed consent cannot be applied to biobank research because most studies will be planned and implemented in the future; therefore, donors cannot be informed about the details at the time of donation. Thus, “broad consent,” a consent model for an unspecified range of future research with some degree of oversight, 2 has been adopted in major biobanks; however, this raises several ethical and social issues. The main question is whether donor autonomy is retained in the broad consent. Many ethicists, sociologists, medical researchers, and other biobank stakeholders have joined the argument, with views ranging from philosophical to empirical standpoints.2–8
The issue has also been discussed from a legal perspective, and two major updates have recently come into effect. One is the 2018 revision of the Federal Policy for the Protection of Human Subjects (Common Rule) in the United States, which introduced broad consent as a new category of informed consent for human subject research, and the other is the 2018 European General Data Protection Regulation (GDPR), which is regarded as supporting broad consent. While leaving some margin for argument, both the Common Rule and GDPR can be interpreted as allowing for the broad type of consent, but only under certain circumstances.9,10
Over the last decade, rapid advancements in biological and information technologies have caused several changes in the debate around broad consent. Alternative consent models have also been presented. In addition to the tiered consent model, which gives donors various options for participation in biobank research, such as research areas or objectives, range of data sharing, and public or commercial use,11,12 a more technology-dependent model—dynamic consent—has been coming to maturity and increasing in popularity. This consent model utilizes Internet-based infrastructure to respect donors' decisions as far as possible.13–15 Another model, meta consent, is a hybrid of dynamic and broad consent with additional options for blanket consent and refusal.16,17 These models aim at participant-centric and flexible research to overcome the autonomy issue often raised for broad consent.
Novel technologies have facilitated innovative medical studies. For example, studies involving the creation of chimeric animals or cerebral organoids or the use of genome editing technology have been made possible by recent developments in medical technologies; nevertheless, all of these studies involve ethical issues to a greater or lesser degree.18–20 Recently, a study examining the chimeric competency of human stem cells integrated into monkey blastocysts sparked ethical concerns.21,22 Greely and Farahany implied that this study might be the type of research in which specific consent from cell donors should be required owing to its particularly controversial aspects. 18
Previous empirical studies have shown mixed results on public attitudes regarding consent. A literature review on public attitudes toward biobanking by Domaradzki and Pawlikowski discovered that attitudes toward the preferred type of consent varied by country. 23 However, the review contained little to no data from Japan. Furthermore, multiple other literature reviews on related topics show that the existing research is particularly lacking in terms of empirical data derived from population-based, general public samples, and investigations of quantitative data on consent model preferences in the context of biobank research are limited.7,24,25
Considering the changing circumstances around the broad consent issue, as well as our concerns regarding the ethical, legal, and social aspects of biobank research in Japan, we aimed to explore current public preferences toward consent models and discover how those attitudes are determined.
Methods
An online questionnaire survey was conducted in September 2019. We asked a research company to recruit ∼1500 participants, implement the online survey, and collect the data. Respondents were randomly selected from the over 1 million individuals registered with the survey company, with distribution adjusted to reflect the composition of the Japanese population in terms of gender, age, and residential area. To ensure that the survey represented the attitudes of lay people, we excluded workers from the drug manufacturing industry, drug wholesale/retail industry, and medical field. We also excluded people who had studied medicine or worked in related fields.
At the beginning of the questionnaire, we briefly explained biobank research with examples of “biospecimens” and “data” to facilitate respondents' understanding. The survey included questions assessing public concerns regarding biobank research, as well as consent model preference (Table 1). We presented five types of consent options with concise descriptions/scenarios of each model: opt-out, broad consent, tiered consent, specific consent, and dynamic consent (Table 2). Preferences for each type of consent model were examined by asking participants their most-preferred consent model and the degree of preference for each model. A four-point Likert scale was used for the responses.
Explanation and Questions of the Survey
Options and Descriptions for Consent
Before the question about consent models, the following explanation was provided to the respondents: In medical research that uses samples and information, at the time of collecting them from patients or volunteers, researchers inform donors specifically how their samples and information will be managed and what research it will be used for and obtain their consent before the research begins. Consent can be obtained in five ways, as described below.
Statistical analyses
Differences among attitudes toward biobank-research concerns were assessed using the Wilcoxon signed-rank test. To examine the difference between the outcome and expected distribution of data for the most-preferred consent model, the chi-square goodness of fit test was performed. In addition, the Wilcoxon signed-rank test was used to analyze the difference between the preference for broad and specific consent.
We performed univariate and multivariate logistic regression analyses to explore how preferences for a consent model were determined. For this purpose, we categorized opt-out and broad consent as “broad-type” consent and specific and dynamic consent as “autonomy-based” consent because they allow for greater autonomy for donors. We considered tiered consent to have both broad and specific aspects; thus, it was excluded from the analysis.
After categorizing all respondents into broad type, autonomy based, and uncategorized, in accordance with their responses to the most-preferred consent model, we used broad type and autonomy based as the dependent variables. Independent variables for the analysis were selected from the respondents' characteristics, experiences, and concerns that could predict their consent model preference. In the process of selecting these variables, we observed the Spearman's rank correlation coefficient of each variable to eliminate the possibility of multicollinearity. In addition, the variance inflation factor (VIF) was used to check for multicollinearity. The Hosmer–Lemeshow test was used to assess the goodness of fit for the model.
The threshold for significance was set at p < 0.05. All statistical analyses were conducted using IBM SPSS for Mac version 27.0 (IBM Corp., Armonk, NY).
Results
Demographics
In total, survey data from 1580 participants were included in the analyses. Table 3 shows the demographic characteristics of the respondents.
Demographic Characteristics of Respondents
Public concerns regarding biobank research
Figure 1 shows the degree of concern regarding privacy infringement, social discrimination, family harm, and group harm. Results reveal that respondents considered potential family harm as the most important issue. Privacy infringement and social discrimination were considered slightly less important. However, both issues were regarded as important or somewhat important by >85% of the respondents. Group harm was the least important of the four issues; nevertheless, 78% respondents reported concerns about it. The Wilcoxon signed-rank test revealed significant differences among the participants' attitudes toward privacy infringement, family harm, and group harm (p < 0.001).

Concerns regarding biobank research.
Most-preferred consent model and attitudes toward each model
Table 4 presents participants' most-preferred consent models. One in three respondents preferred specific consent (33%). Dynamic consent ranked second (27.9%), followed by tiered consent (15.2%), opt-out (12.6%), and broad consent (11.3%). The distribution significantly differed from the expected outcome (20% each) as determined by the chi-square goodness of fit test (p < 0.001). When grouped as two broader options, excluding tiered consent, 60.9% of the respondents preferred autonomy-based consent, while 23.9% preferred broad-type consent.
Most-Preferred Consent Model
n = 1580.
Figure 2 shows participants' attitudes toward each consent model on the four-point scale. While specific consent was (somewhat) preferred by 83% of the respondents, broad consent was (somewhat) preferred by 53.1%. Statistical difference between the attitudes toward the two models was confirmed by the Wilcoxon signed-rank test (p < 0.001).
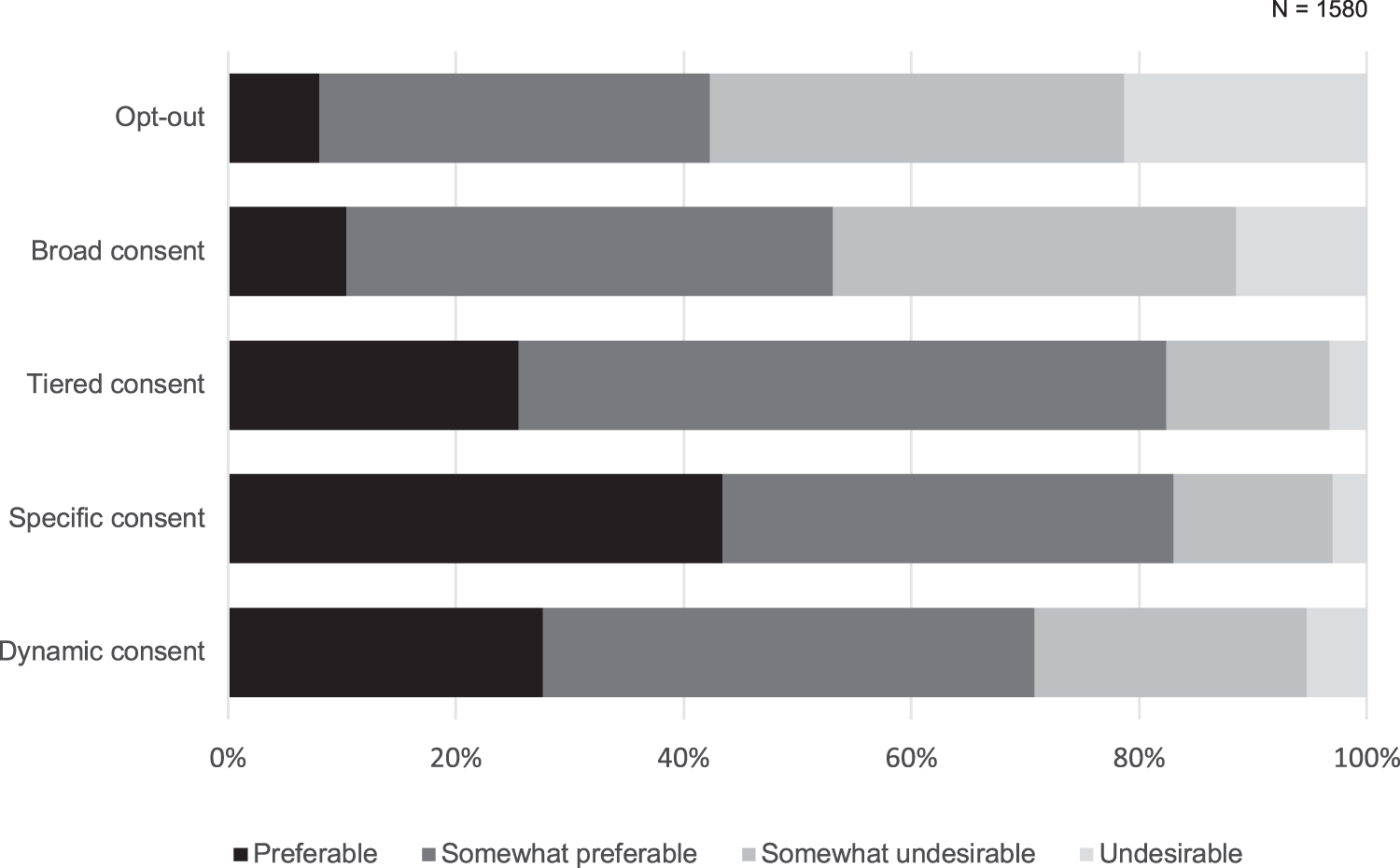
Attitudes toward each consent model.
Variables affecting preference for a consent model
Table 5 shows the logistic regression analysis results of the variables affecting consent model preference. Multivariate analysis revealed that only marital status (being married) was statistically related to the preference for broad-type consent (adjusted odds ratio [aOR] = 1.488; confidence interval [95% CI], 1.037–2.136; p = 0.031). Being female (aOR = 0.479; 95% CI, 0.353–0.651; p < 0.001) and having concerns about privacy infringement (aOR = 0.806; 95% CI, 0.672–0.967; p = 0.020) were associated with a preference for autonomy-based consent.
Logistic Regression of Variables Affecting the Preference for Broad-Type Consent
1 − 5; lower to higher.
1–4; lower to higher.
Spearman's rank-order correlation coefficients (ρ) for each independent variable were <0.4, and none of the VIF values reached 2.0, indicating no multicollinearity in the model. The Hosmer–Lemeshow test yielded a p value of 0.643, and the model's calibration was satisfactory. Although univariate analysis demonstrated that the other three concerns (social discrimination and family/group harm) were associated with a preference for autonomy-based consent, they were excluded from the multivariate analysis as they were broadly similar concepts and their correlations with each other were relatively high (|ρ| ≥ 0.464).
Discussion
In the present research, we implemented a quantitative survey to examine the Japanese public's attitudes toward consent, as well as public concerns regarding biobank research. Most respondents showed substantially high concerns about each issue presented: privacy infringement, social discrimination, and family/group harm. Approximately 60% the respondents preferred autonomy-based consent, while 25% preferred broad-type consent (15% chose tiered consent, containing aspects of both types from the perspective of donor autonomy). However, when examining each consent model, broad consent was supported by a slightly higher majority of respondents. Gender and marital status predicted consent-model preference. In addition, people who prioritized their privacy were likely to prefer autonomy-based consent.
A previous systematic review of empirical surveys on consent concluded that, in the presence of other options, such as tiered or specific consent, only a minority of respondents favored broad consent; meanwhile, when broad consent was the only choice offered, a majority often expressed support toward it. 26 Another recent literature review on the same topic reported that many donors accepted broad consent; however, if available, other options such as dynamic consent were preferable. 23 Our results were consistent with these conclusions, in that, while broad consent was acceptable to the respondents, other options such as specific, dynamic, or tiered consent were more preferable.
The logistic regression analysis results for the variables affecting consent-model preference suggested that people who were more careful about their privacy were more likely to prefer autonomy-based consent. This finding was consistent with a previous study 27 and intuitively understandable given the nature of biobank activities, which inherently include information risk, such as invasions of privacy or genetic discrimination.28,29 Under broad consent, people might be seriously concerned about the inappropriate use of their specimens and data outside their conscious awareness.
In the debate over consent, perception of the risks associated with biobank research is an important issue; an argument is whether the information risk is minimal enough to abandon study-by-study consent.8,30,31 The minimal risk argument is one justification for broad consent and is supported by the assumption that the risk of harm from biobank research is low and the system is sufficiently well-controlled by a secure coding system and privacy laws. 3 Some people oppose this optimistic view, pointing to cases of reidentification of seemingly anonymous data when several public databases are combined.32,33 Metcalf and Crawford, who examined several contentious cases of research harm in data science, highlight that ethical frameworks for data science research are highly contested and the potential harms are unpredictable. 34
Furthermore, information risk in biobank research may affect not only donors themselves but also their family members or their groups, such as local, national, ethnic, and racial affiliations. 29 Interestingly, the present study demonstrated that for potential donors, family harm was statistically more important than their individual privacy concerns. In contrast, group harm was less important than individual privacy concerns. This finding could be partially interpreted from the cultural background or national character perspective.35,36 However, the exact factors that affected the results remain unclear. The family's influence and role in informed consent in clinical practice have been considered in the Japanese cultural context, for example, the family-facilitated approach by Akabayashi and Slingsby. 37 However, a donor's concerns regarding the influence of biobank research participation on their family, as well as its impact on the informed consent process, have not been fully appreciated. Our result suggests the need for further investigation on this matter.
In contrast to family harm, group harm was less important for some respondents. Group harm related to biobank research has been recognized and discussed in the context of stigma, discrimination, and cultural harm to specific communities.38–40 The sample case shown to the respondents in our survey was the Havasupai tribe case in the United States, 41 which might have affected their responses, as minority ethnic issues are not a very familiar topic for many Japanese individuals, and therefore, they might have been unable to think of other forms of group harms. However, our survey did not present enough data to assert this assumption. The regression analyses also did not provide any definitive results; however, the univariate analyses suggest the possibility of an association between these public concerns and autonomy-based consent.
Notably, autonomy-based consent does not fully prevent these informational harms. However, at least the risk of dignitary harm,39,42 the risk of their donated specimens being used for purposes that the donor objects due to, for example, their religious or moral beliefs, can be prevented by autonomy-based consent. Furthermore, we can suppose that even the risk of family/group harm, to some extent, could be reduced by carefully choosing the research in cases where donors understand the specific research details. As such, pursuing autonomy-based consent—practically, dynamic, or meta consent—would help realize an ideal form of biobank research. However, some important issues stemming from these consent models, such as digital divide, must be addressed.15,43,44
In contrast, high public concerns regarding biobank research observed in our study, particularly privacy infringement and social discrimination, seem to be considered, in part, to reflect people's distrust toward some activities of biobanking, because these concerns are thought to mainly come from people's worries or senses of distrust about the handling of their specimens or data. In fact, information-related matters are likely to occur due to improper management by the institution or a researcher's unauthorized use of materials. Less public trust toward insurance or for-profit companies than toward public institutions involved in biobank research, which has been demonstrated in several studies,45–47 is indicative of this kind of concern about inappropriate or unacceptable handling of their materials.
Furthermore, given that “trust” has been shown to be associated with a preference for broad consent,27,45,48 fostering trust and trustworthiness for biobank research would help address potential donor's concerns. This would strengthen public engagement with biobank research, even if the biobank is operated under broad consent. Theoretical analyses of the ethical and social implications of biobank research have emphasized the importance of public trust on the relationship between the research body and the public for the sustainability of biobank research. Experts consider that broad consent in the context of biobank and genomic research has its limitations; therefore, there has been a call for emphasis on biobank governance for promoting trust.49–51 Therefore, the other way is to place, under broad consent, appropriate governance measures that promote public trust.
Although the importance of biobank governance appears to be broadly recognized, the governance measures that should be implemented remain unclear. This issue is being currently addressed by experts in different countries. Some highly suggestive empirical studies, based on the theory of deliberative democracy, have been conducted in United States, Canada, Australia, and other countries, seeking appropriate governance models and its principles.51–53 However, such studies are rarely conducted in Japan, and therefore, very little is known about this issue from Japanese perspectives. The present study also could not cover this issue, and thus, it remains to be addressed in the future.
Limitations
Our data represent a public opinion about the concerns of biobank activity in a general setup. Yet, in the real world, each biobank has a particular background and objective. If respondents were to be involved in a biobank in actuality, some would likely act and respond differently from what they might indicate in their responses to such online surveys. This is because the relationship between the biobank and the respondent would be unique at that particular time depending on the nature or objective of the transaction.
Moreover, the explanations of the survey given to the respondents, as well as the description of each consent model, might have resulted in biased outcomes. Furthermore, this could be a barrier for comparison with other similar research findings, although the wording and expressions were carefully chosen to improve respondents' understanding.
Conclusions
Our empirical research demonstrated that Japanese people were inclined to be attracted to autonomy-based consent, including dynamic consent. This result may be partially associated with sensitivity to privacy and other public concerns related to information risk. However, the data also revealed that approximately half of the respondents regarded broad consent as somewhat preferable. Additional studies are needed to determine whether implementing appropriate governance measures could further improve the social acceptability of broad consent in the Japanese population.
Footnotes
Acknowledgments
The authors thank Dr. Taichi Hatta at the Shizuoka Graduate University of Public Health for his helpful advice on the statistical methods implemented in this study. The authors also acknowledge fellow members of the Department of Biomedical Ethics of the University of Tokyo for their useful comments on the initial draft of the questionnaire. The authors thank the anonymous reviewers whose comments and suggestion helped improve the article.
Authors' Contributions
M.O.: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Writing—original draft preparation, Funding acquisition. Y.T.: Conceptualization, Methodology, Writing—review and editing, Supervision, Funding acquisition. A.A.: Writing—review and editing, Supervision.
Ethics Approval
The study protocol was approved by the Ethics Committee of the Graduate School of Medicine and Faculty of Medicine, The University of Tokyo (2019029NI) and Center for iPS Cell Research and Application, Kyoto University (20-05).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Uehiro Foundation of Ethics and Education and the Japan Agency for Medical Research and Development (15653106 and JP20dm0107567).