
Abstract
Oocyte vitrification is widely used for female fertility preservation. However, the efficacy of this procedure may depend on the women's age. The aim of the study was to compare the morphology, viability of cryopreserved oocytes, and their fertilization outcomes (fertilization, blastulation rate, level of embryo chromosomal aneuploidy—preimplantation genetic testing for aneuploidy [PGT-A]) in women of different reproductive ages. The studied oocytes were divided into groups depending on the age of patients: up to 30 years (group 1), 30–35 years (group 2), 36–40 years (group 3), and older than 40 years (group 4). It has been shown that in women of older reproductive age, the number of oocytes with polymorphism of endo- and extracytoplasmic structures was higher compared with younger patients. This could reflect on their cryosurvival rate, which was the highest in group 1 (98.1%) and the lowest was in group 4 (47.4%). With increasing age, the fertilization rate of cryopreserved oocytes and subsequent blastulation was decreased. However, the number of embryos with an aneuploid chromosome set number was increased. The chromosome set number euploidy rate of the embryos obtained from cryopreserved oocytes of advanced age women (group 4) did not differ from the fresh group with the same age (31.2% vs. 24.4%, p > 0.05), but the number of euploid embryos per patient was less than one (0.8 ± 0.1). Therefore, the decision to cryopreserve the oocytes of a patient of older reproductive age should be made individually for each situation, taking into account the prospects of obtaining full-fledged embryos and the chances of pregnancy.
Introduction
There is a trend toward an increase in the average age of mothers. In many cases, modern women plan to realize their career potential first, and postpone the creation of a family and childbirth to a later date. Therefore, cryopreservation of oocytes of patients at younger reproductive age, and storage of gametes in a cryobank for further transfer to the uterine cavity of these patients at older age is of great practical and psychological importance for achieving the desired pregnancy.1,2 In addition to social indicators, women of reproductive age can resort to cryopreservation of oocytes in connection with gonadotoxic treatment, when conducting a donation program of oocytes in severe cases of infertility, when donating cytoplasm of oocytes in case of mitochondrial dysfunction or hereditary genetic abnormalities within the context of specialist reproductive technologies.3–5
In many of these cases, the age of patients may be older, in contrast to those who resort to oocyte cryopreservation for social reasons. 3 It is known that women after 30 years old have a reduced likelihood of conception, 6 which is associated with oocyte quality.7,8 Endocrine changes in older women may lead to decreased morphological and functional characteristics of oocytes. During cryopreservation, this can adversely affect their cryoresistance and the genetic competence of subsequently produced embryos. Therefore, the age of women who resort to oocyte cryopreservation is crucial. Thus, there are age restrictions for oocyte donors of 35 years old, and although oocyte cryopreservation is not recommended for women older than 38 years, there may be cases where a preliminary assessment of ovarian reserve justifies the procedure.9,10
Therefore, data on the oocyte quality, the results of their fertilization and the development of genetically normal embryos are very important for predicting the effectiveness of oocyte cryopreservation in women of different reproductive ages.
The aim of the current study was to compare the morphological characteristics of oocytes, their survival after cryopreservation, in vitro fertilization, blastulation rates and the level of embryo chromosomal aneuploidy in women of different reproductive ages.
Materials and Methods
The work was carried out at the IGR Medical Center, the ART Clinic of Reproductive Medicine and the Institute of Cryobiology and Cryomedicine of the National Academy of Sciences of Ukraine.
All the manipulations of gametes and embryos were performed according to the report of the Steering Committee on Bioethics (CDBI) on “The Protection of the human embryo in vitro” CDBI-CO-GT3 (Strasbourg, June 19, 2003) with an informed patient consent and the decision of the Committee in Bioethics of the Institute for Problems of Cryobiology and Cryomedicine of the NAS of Ukraine.
A retrospective cohort study of 323 cycles of infertility treatment by ART in women of different reproductive age was conducted. The first group consisted of patients under 30 years, the second—30–35 years, the third—36–40 years, and the fourth—patients over 40 years.
The endocrine status of patients was assessed by the level of antimullerian hormone (AMH) and follicle-stimulating hormone (FSH) enzyme-linked immunosorbent assay (ELISA) kit (Abcam) by ELISA.
Stimulation of superovulation was performed using a short protocol with gonadotropin-releasing hormone antagonists and recombinant FSH. Follicle aspiration was performed under the control of an ultrasound scanner (Olympus IX-11) 36 hours after the ovulation trigger introduction.
The isolated oocyte-corona cumulus complexes were cultured in medium (Global total; CooperSurgical). Oocytes were cryopreserved according to the W. Kuwayama two-step Cryotop method with slight modifications of the volume of equilibration solutions (50 μL) 11 after denudation and maturity assessment.
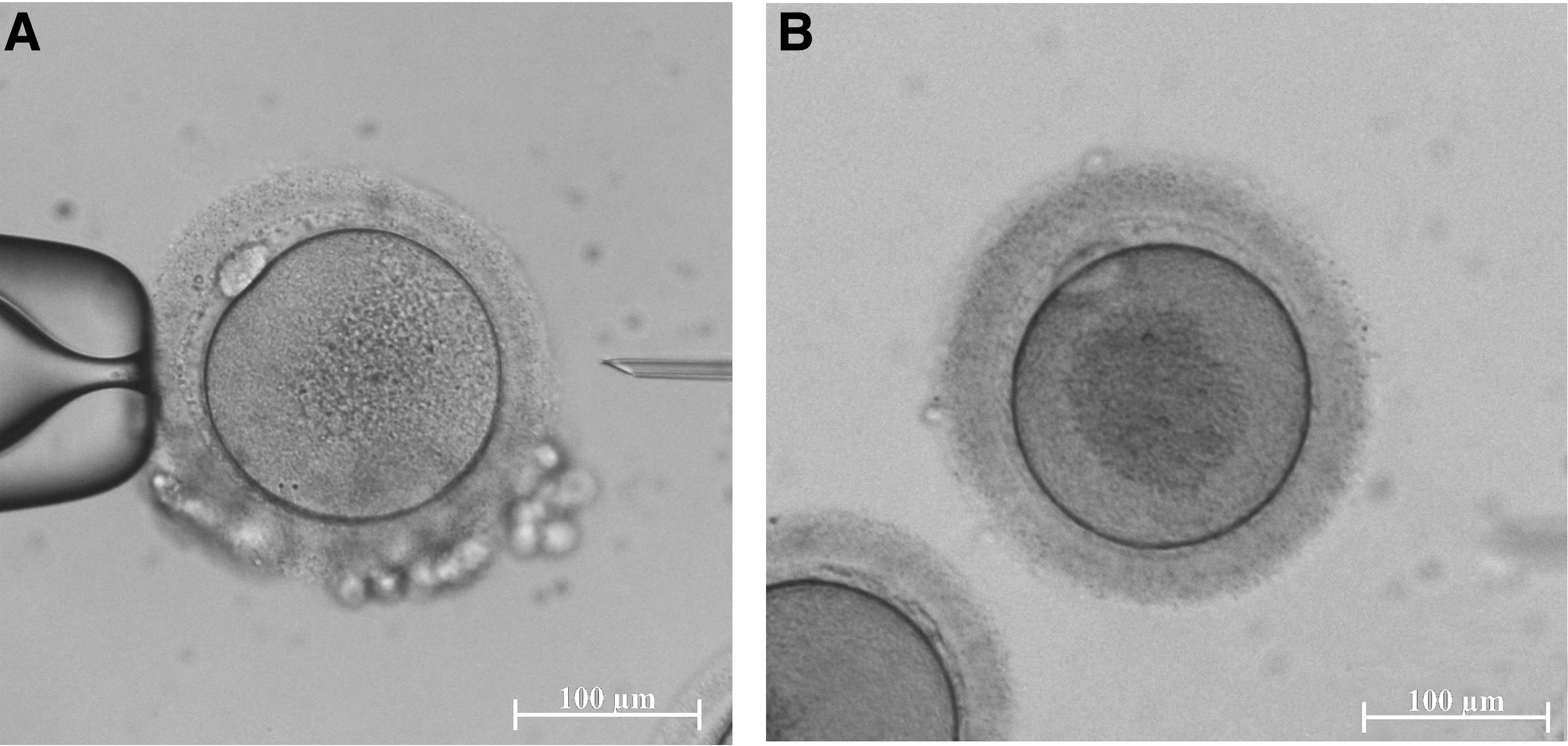
The morphology of oocytes and embryos was evaluated according to the Istanbul consensus. 12 There is evidence that optimal oocyte morphology is a spherical structure enclosed by a uniform Zona Pellucida (ZP), with a uniform translucent cytoplasm free of inclusions and a size-appropriate polar body (PB) (Fig. 1A). The oocytes with extracellular and intracellular abnormalities were discarded from the cohort for fertilization. An example of the oocyte with intracellular abnormality (smooth endoplasmic reticulum clustering) associated with the risk of significantly abnormal outcomes is shown in Figure 1B.
Good
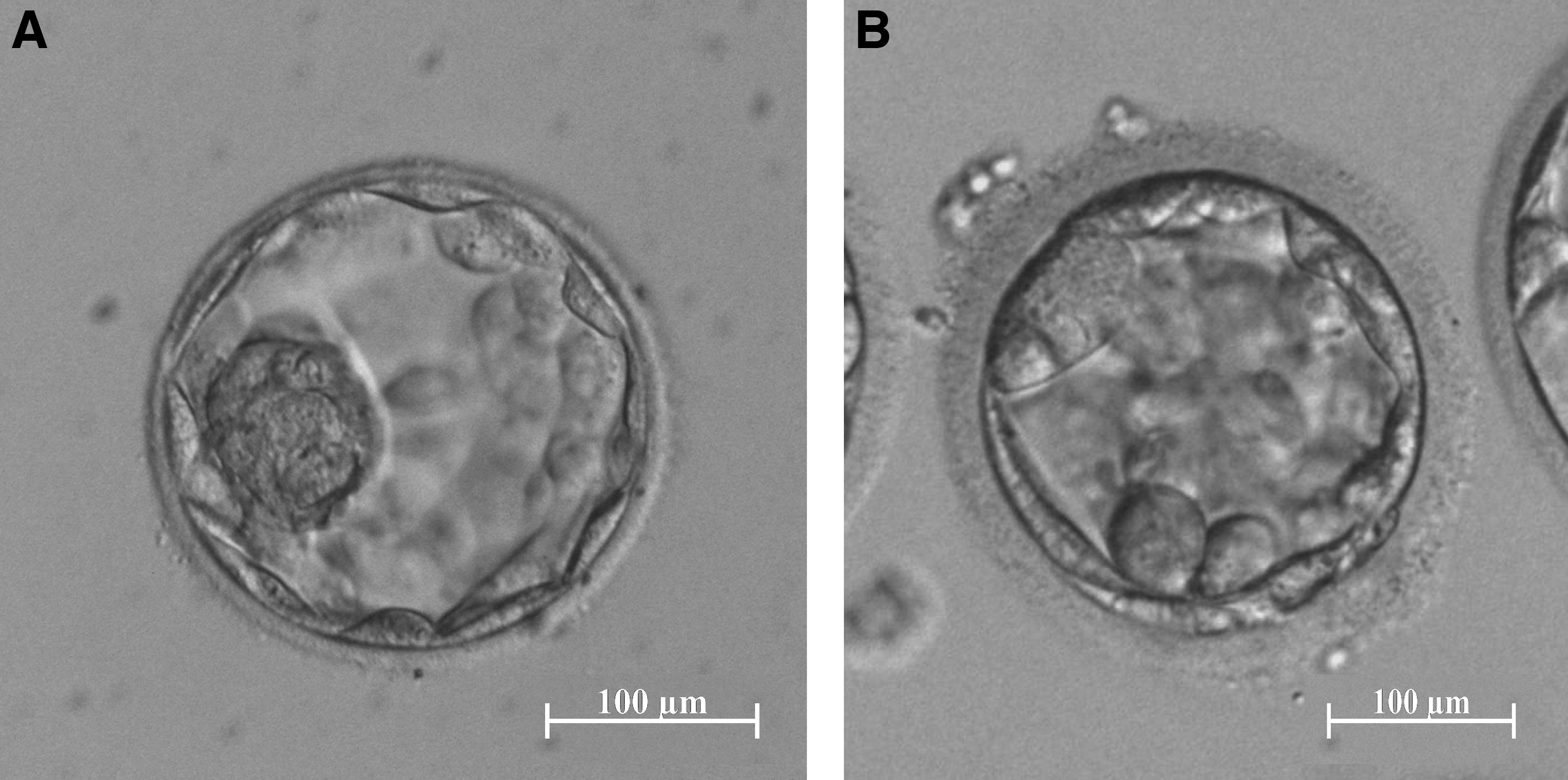
We also assessed the morphology of day 5 blastocysts by the quality of inner cell mass (ICM) and trophectoderm cells (TE). According to the Istanbul consensus, 12 it was considered that good quality ICM has to be prominent, easily discernible, with many cells that are compacted and tightly adhered together, and good quality TE has to have many cells forming a cohesive epithelium (Fig. 2A). Poor quality embryos (Fig. 2B) were discarded from the preimplantation genetic testing (PGT) and embryo transfer.
Good
The survival rate of cryopreserved oocytes was assessed by their ability to reexpand to the original volume and morphological features after warming: degeneration and darkening of the ooplasm; increased cytoplasmic granularity; ooplasm vacuolization; aggregates of smooth endoplasmic reticulum; increased size of perivitelline space; its excessive granularity; fragmentation of the first PB; and abnormalities and rupture of the ZP.
Fertilization of cryopreserved oocytes was performed by intracytoplasmic sperm injection (ICSI) 2 hours after warming. 13 Spermatozoa for ICSI were obtained from fresh sperm of a patient's partner with normozoospermia by centrifugation in Percoll density gradient media. Fertilization was assessed by the presence of pronuclei after 18–20 hours. Embryos were cultured up to 5 days in medium (Global total; Cooper Surgical) at 37°C and 5.5% CO2.
According to the ESHRE guidelines 14 PGT was performed using only embryo TE cells biopsies to avoid ICM damaging and embryo development decreasing. It was carried out on day 5 of embryo development. Four to five TE cells were cut off using a Saturn laser device (Research Instruments), an inverted Nikon TI-U microscope (Nikon), micromanipulators (Narishige), and micropipettes with an inner diameter of 17 μm (Cook) for fixed content of embryos and micropipettes for trophectoderm biopsy with a diameter of 23–27 μm (Origio). Preimplantation genetic testing for aneuploidy (PGT-A) for chromosomes 13, 16, 18, 21, 22, X, and Y was performed using commercial PB MultiVysion and CepX/CepY Kits (Abbott) according to the manufacturer's instructions. Analysis of hybridization signals was performed using a fluorescence microscope Olympus BX 51 (Olympus), equipped with an appropriate set of filters and an automatic image processing program ISIS (Meta Systems).
Verification of the distribution of quantitative dates for compliance with the law of normal distribution was performed by the methods of Shapiro–Wilkie and Kolmogorov–Smirnov. Comparisons of arithmetic means were performed by Student's methods. Statistical hypotheses were tested using t criteria, χ 2 at significance levels p < 0.05, p < 0.01.
Results and Discussion
Analysis of clinical and anamnestic data of patients showed that the mean age of patients was 27.6 ± 3.5, 32.8 ± 1.6, 37.7 ± 1.4, and 41.7 ± 1.1 years for groups 1–4, respectively (Table 1). The main physiological role of AMH in the ovary is associated with the suppression of the early stages of follicle development. 13 AMH levels decreased significantly with increasing patient age.
Clinical and Anamnestic Indicators of Patients of Different Age Groups
Differences are significant in comparison with the indicators of group 1, p < 0.05.
Differences are significant in comparison with the indicators of group 1, p < 0.01.
AMH, antimullerian hormone; FSH, follicle-stimulating hormone.
The same pattern associated with the age of the patients was also found for the number of oocytes obtained by follicle aspiration after the superovulation induction. Thus, more than 10 oocytes were retrieved for patients younger than 35, the number gametes were twofold less after 35 years old, and were no more than 3 oocytes for woman older than 40.
After denudation, the morphological characteristics of the ooplasm and extracytoplasmic structures were evaluated. The older age group was characterized by high rates of oocyte dysmorphism (Table 2). It was noted that the number of oocytes with thickened ZP, nuclear membrane polymorphism, and denser nucleoplasm increases with age.
Morphological Characteristics of Oocytes of Patients of Different Age Groups
Differences is significant in comparison with the indicators of group 1, p < 0.05.
PB, polar body; ZP, Zona Pellucida.
Previous studies have shown that oocyte quality may be related to a woman's age, 15 but the effect of this parameter on cryoresistance of oocytes has not been studied. Our results showed that the highest oocyte survival rate (98%) was in group 1 (Table 3). The cryoresistance of oocytes decreased with increasing of age and was the lowest (47.4%) in group 4 (Table 3). It is likely that the low level of normal morphology (33.3% ± 3.3%) in the oocytes of group 4 (Table 2) reflects a violation of the functional characteristics of the gametes. Therefore, such “weak” gametes with dysmorphism of extra- and intracytoplasmic structures have a reduced survival rate after cryopreservation, which is accompanied by a sharp change in osmotic pressure, exposure to high concentrations of cryoprotectants, and low temperatures.
Survival, Fertilization, and Blastulation Rates of Fresh and Cryopreserved Oocytes of Patients of Different Age Groups
Differences are significant compared to group 1, p < 0.05.
Differences are significant compared to group 2, p < 0.05.
Differences are significant compared to group 3, p < 0.05.
Subsequent studies of oocyte in vitro fertilization and blastulation rates showed a significant difference between the groups (Table 3). It was found that the fertilization rate and blastulation rates of fresh and cryopreserved oocytes of women older than 30 years was significantly reduced compared to younger ones. The lowest fertilization rate was in group 4 of fresh (60.4%) and cryopreserved oocytes (59.3%). We have not found any significant difference in fertilization and blastulation rates between the fresh and cryopreserved oocytes of woman of different ages. Nevertheless, a significant reduction of fertilization rate of fresh oocytes occurred in group 3 compared to group 2, while in cryopreserved oocytes, there were no such differences and a decrease was noted only in group 4 compared to group 3. A similar effect was noticed regarding the blastulation rate.
There was no significant difference between groups 3 and 4 of cryopreserved oocytes while there was a significantly decreased blastulation rate of fresh oocyte group 4, compared to the younger age group 3. It can be assumed that certain improvements of the fertilization and blastulation rates of oocytes of the older age group occur due to the fact that the most complete cells with higher functional characteristics survive after cryopreservation, compared to fresh gametes. In our opinion, this precise cryoselective effect occurs with oocytes of the older age group. However, it should be emphasized that due to the small sample number in group 4, there were no significant differences between embryos obtained from fresh and cryopreserved oocytes.
Considering that the morphology of blastocytes largely reflects their chromosomal status, 16 we also compared the morphology of the developed blastocyst obtained either from fresh or cryopreserved oocytes of patients with different ages (Table 4). We have evaluated the number of blastocysts with good quality ICM and TE. There were no statistically significant differences between all patient age groups of fresh and cryopreserved oocytes. The number of embryos with good quality ICM obtained from fresh oocytes decreased in patients older than 36 years.
Morphological Characteristics of Blastocysts Obtained from Fresh and Cryopreserved Oocytes of Patients of Different Age Groups
Differences are significant compared to group 1, p < 0.05.
Differences are significant compared to group 2, p < 0.05.
ICM, inner cell mass; TE, trophectoderm cells.
However, it was also revealed that there was no difference in the number of this indicator for embryos of groups 2 and 3 obtained from cryopreserved oocytes, in contrast to fresh ones. The number of blastocysts with good quality of TE did not differ between age groups and did not depend on cryopreservation. The data from group 4 did not show any significant differences with other groups due to a very small sample in group 4.
The rest of the embryos which did not reach the blastocyst stage stopped their development at day 2 or 3. It is known that the initial blastomere cleavage occurs due to the oocyte genome. Then, embryonic genome activation occurs in three stages: 2-cell, 4-cell and 8-10-cell embryo stages, and the final stage represents the highest level of transcriptional activity and usually occurs at day 3. However, most embryo aneuploidy occurs due to the chromosome segregation disruption during oogenesis. These cause abnormalities in embryo development, including cessation of their development. 17
Therefore, the next step of the study was to assess the level of chromosomal aneuploidy of embryos derived from fresh and cryopreserved oocytes of women of different ages.
The data showed that the number of embryos obtained after fertilization of fresh oocytes is reduced in women of older reproductive age (Table 5). The level of embryo chromosomal euploidy was 53.3% in the group of patients younger than 30 years of age and decreased in groups where women were older than 30 years. The lowest rate was determined in group 4 (24.5%), and therefore in this group, there was the lowest number of euploid embryos per 1 patient (1.1 ± 0.3). The mosaicism and polyploidy rates showed no significant differences between the studied groups.
Chromosomal Analysis of Embryos Derived from Fresh Oocytes of Patients of Different Age Groups
Differences is significant in comparison with the indicators of group 1, p < 0.05.
Differences is significant in comparison with the indicators of group 1, p < 0.01.
PGT-A, preimplantation genetic testing for aneuploidy.
PGT-A of embryos derived from cryopreserved oocytes showed that the level of chromosome euploidy depends on the patient age and was the highest in group 1—54.4%, and the lowest in group 4—31.2% (Table 6). There was a significant decrease in the number of euploid embryos starting from group 2 as in the groups of embryos obtained from fresh oocytes. It was found that the lowest number per patient of euploid embryos derived from cryopreserved oocytes was in group 4 (0.8 ± 0.1), which makes pregnancy impossible in some cases. We did not note any cryopreservation effect on the polyploidy and mosaicism rates of embryos of patients in any of the age groups.
Chromosomal Analysis of Embryos Obtained from Cryopreserved Oocytes of Patients of Different Age Groups
Probability in comparison with the indicators of group 1, p < 0.05.
Probability in comparison with the indicators of group 1, p < 0.01.
Our study has shown decreases not only in the morphological characteristics of oocytes and the fertilization rate, but also in the number of embryos and the blastulation rate with increasing patient age. We noted such changes already in patients in the group older than 30 years. Considering that the ICM grade and TE grade are associated with pregnancy outcomes and that ICM grade is the strongest predictor of live birth, 18 the decrease in the number of embryos with good quality ICM in women older than 36 years of age may indicate a negative impact on the live birth rate. Meanwhile, cryopreservation of oocytes did not result in an additional effect of this parameter.
The survival rate of oocytes after cryopreservation depended on the age of the patients and significantly decreased in patients older than the age of 40 years. These results confirm data from another private in vitro fertilization center in Sweden, which also reported no pregnancy in this patient age group. 19 Our studies supplement this finding by arguing that although the quality and blastulation rate in this age group did not differ from the group of embryos obtained from fresh oocytes, the number of euploid embryos per patient in this group was less than one (0.8 ± 0.1). This may explain the lack of pregnancy in this age group.
The risks of aneuploidy are thought to be associated with delayed meiosis I, which occurs before ovulation. 20 However, even mature oocytes without prior chromosome segregation disruption may be adversely affected during cryopreservation because the meiotic spindle microtubules are very sensitive to temperature fluctuations, and subsequent fertilization of such oocytes can cause chromosomal aneuploidy in embryos. 21 We have previously shown that despite this, the level of chromosomal aneuploidy in embryos derived from either cryopreservation or oocytes did not have significant differences. 4 It should be noted that such results were obtained in the study of women with a mean age of 27.6 ± 4.8 years.
Taking into account that in women of older reproductive age, the oocyte survival rate was the lowest and was characterized by increased dysmorphism and morphological abnormalities of development, which are signs of impaired functional value of gametes, 22 we can assume that in this case, cryopreservation imposed a positive selective factor and after thawing survived as more functionally complete oocytes. This assumption should be tested on larger numbers of samples, but given that the number of patients in this age group is limited in the practice of one clinic, the study should be multicenter. It should be noted that the number of embryos of advanced reproductive age women who are available for transfer may be less than one due to the reduced morphology, fertilization, blastulation, and their euploidy rates.
Therefore, the decision to cryopreserve the oocytes of a patient of older reproductive age should be made individually for each situation, taking into account the prospects of obtaining full-fledged embryos and the chances of pregnancy.
Conclusions
Qualitative and quantitative oocyte characteristics, fertilization rate, and number of developed embryos with a euploid chromosome set number decrease with women's age. Oocytes of women of advanced reproductive age are more sensitive to cryopreservation factors compared to oocytes obtained from younger women, which is manifested by a low survival rate (47.4%). However, there was no negative effect of cryopreservation of oocytes on the morphology and level of aneuploidy of the resulting embryos in all patient age groups. The results of the study are important when consulting patients of different reproductive ages who, due to social or medical reasons, plan to preserve reproductive potential by oocyte cryopreservation.
Footnotes
Authors' Contributions
M.P. and B.F. conceived and designed the article. M.P. and T.Y. wrote the article. N.B., J.G., I.I., and V.P. performed data collection. All authors modified the article, read, and approved the final version.
Author Disclosure Statement
Authors declare no conflict of interest.
Funding Information
This work was funded by National Academy of Sciences of Ukrainian program “Support priority scientific research directions development” 0120U100378.