
Abstract
Introduction:
The onset of precision medicine has led to the integration of traditional morphologic tissues evaluation with biochemical and molecular data for a more appropriate pathological diagnosis. The preanalytic phase and, particularly, timing of cold ischemia are crucial to guarantee high-quality biorepositories of formalin-fixed paraffin-embedded (FFPE) tissues for patients' needs and scientific research. However, delayed fixation using the gold-standard and carcinogenic fixative neutral-buffered formalin (NBF) can be a significant limitation to diagnosis and biopathological characterization. HistoCold (patented; Bio-Optica Milano S.p.A., Milano, Italy) is a nontoxic, stable, and refrigerated preservative solution for tissue handling. This study examined HistoCold's potential role in improving the preanalytic phase of the pathological diagnostic process.
Materials and Methods:
Breast, lung, or colorectal cancers (20, 25, and 10 cases, respectively) that were to be surgically resected were recruited between 2019 and 2021. Once specimens were surgically removed, three residual samples for each patient were first promptly immersed into HistoCold for 24, 48, and 72 hours and then FFPE. These were compared with routine specimens regarding morphologic features (hematoxylin and eosin) and tissue antigenicity (immunohistochemical stains).
Results:
Good concordance regarding both the morphologic characteristics of the neoplasms and their proteins expression between the routine and HistoCold handled tissues were found. The tissue handling with the solution never affected the histopathological diagnosis.
Conclusions:
The use of HistoCold for samples transporting is easy, allows for improving the management of cold ischemia time, and monitoring the fixation times in NBF, resulting in good quality tissue blocks for biobanking. Moreover, it could be a candidate to eliminate formalin from operating theaters. HistoCold looks very promising for the preanalytic phase of human tissues handling in the era of precision medicine, to provide the best service to patients, and to scientific research.
Introduction
The advent of the era of precision medicine has given the pathologist new tasks both in terms of researching specific biomarkers for the personalization of therapies and in terms of protecting the integrity and quality of tissues. In particular, it is now mandatory that tissue samples, formalin-fixed and paraffin-embedded (FFPE), must have specifications capable of guaranteeing high-quality biospecimens that can be profitably used in the future, both for the patients' needs and for scientific research.1,2
This last aspect is strictly connected to the concept of a biobank because the biorepositories of FFPE are an integral and fundamental part of such an infrastructure. The search for new diagnostic, prognostic, and therapeutic biomarkers, which constitute the main objectives of a biobank, can only be achieved strictly using selected cells and tissues through standardized preanalytic procedures. The resulting corollary is that every effort must be made to obtain the best possible conservation of the tissues taken from patients for diagnostic and therapeutic purposes. 3
These new requirements need rigorous management of biological samples, with a careful control of the preanalytic variables,4,5 which are essential for the preservation of morphologic characteristics and nucleic acids, proteins, and other signal molecules. 2
Unfortunately, in the real life of scientific research, many studies conducted using FFPE tissues have proved to be unreliable, owing to poor sample quality attributable to a defective preanalytic phase and, particularly, to delayed fixation. 6 In this context, the time of cold ischemia is a crucial point.2,7
Therefore, inadequate tissue handling, particularly regarding the delayed fixation with the traditional—and carcinogenic8,9—fixative, neutral-buffered formalin (NBF), can constitute a significant limitation or impediment to the diagnosis and biopathological characterization.
Nevertheless, NBF still represents the gold standard fixative used in pathology departments, as it retains the morphologic and architectural characteristics of the tissue, on which both the histopathological diagnostic criteria and the laboratory procedures are universally based. Furthermore, most of the commercially available antibodies for immunohistochemistry are produced to recognize antigenic sites whose conformation is modified by formalin fixation 10 and NBF is internationally recommended for histological, immunohistochemical (IHC), and molecular applications.
In this context, the transport medium HistoCold (CE IVD, patent number 102016000077232; Bio-Optica Milano S.p.A., Milano, Italy) is a nontoxic, stable, and refrigerated preservative solution, presenting physiological pH and osmotic pressure, designed for avoiding tissues shock and allowing their safe handling, preservation, and transport from the operating theater to pathology department. This is owing to the synergy of its patented formulation with the action of cold, which inhibits microbial activity, preserves the pH, the physiological osmolarity, and slows the action of proteolytic enzymes.
In particular, the solution is ready-to-use and is cooled when the tissue sample is immersed into it—either through its own refrigerated dispenser or in a prefilled biologic container, stored at 3°C–5°C—to reach the pathology department, where it can be fixed and processed according to standard internal protocols.
Moreover, HistoCold contains neither the carcinogenic formaldehyde nor alcohols such as methanol or ethanol. Although the latter are used worldwide as fixative tissue solutions, their improper use, especially regarding fixation times, can cause irreversible damage because of their chemical composition, not only to the morphology of the tissue, but also to the proteins and nucleic acids integrity, preventing irreparably their IHC or molecular analysis.8–10
Although HistoCold has been tested on swine tissues as regards the tissutal morphology aspects and preliminary data on human specimens was promising, both concerning retained morphology and immunohistochemistry interpretation compared with tissues processed using NBF, 11 a real validation process considering both the morphologic and antigenic features of human tissues has not been carried out yet.
The aim of this study was to fill this gap, comparing tissue characteristics of breast carcinomas (BCs), non-small cell lung cancers (NSCLCs), and colorectal carcinomas (CRCs) transiently immersed in HistoCold before NBF fixation, with those of the same samples immersed directly and routinely in NBF. Therefore, the primary objective of the study was to establish the absence of damage to tissue integrity using HistoCold as a temporary storage medium and, consequently, its candidacy as a means for eliminating formalin from operating rooms. The aim was also to test the capability of breaking down discretion and variability with which the surgical specimens are immersed in formalin after their excision and, last but not the least, fully attributing to the pathologist the process of the fixation in NBF and the control of the relative timing. We describe the results obtained from the comparison between morphologic and immunophenotypic analysis of tissues that underwent both HistoCold and NBF handling.
Materials and Methods
A comparative prospective observational study on morphologic, antigenic, and molecular features of tissues was performed on a series of patients undergoing surgery for BCs, NSCLCs, or CRCs between 2019 and 2021 at Santa Maria della Misericordia Hospital of Perugia, Italy. The study was approved by the local ethics committee, N. 3569/19 of September 26, 2019.
The patients eligible for the study were preselected to recruit only the cases for which the neoplastic tissue was sufficient to perform both the routine management and the current study. Particularly regarding BCs and NSCLCs, patients were enrolled with neoplasms presenting a minimum tumor diameter of 10 and 15 mm, respectively. Concerning CRCs, those macroscopically invading at least the muscularis propria layer were included in the research. All patients enrolled in the study signed a specific informed consent; none of them received neoadjuvant therapy.
Two expert pathologists (L.T., M.M.) monitored the cold ischemia, personally going to the operating room, freshly transporting the specimen to the pathology department within 30 minutes after the surgical sample excision. Afterward, the pathologist did the sampling, identifying the tumor, verifying the compliance with the recruitment criteria, and taking for the study a sample of representative but leftover neoplastic tissue, which was not used for the diagnosis.
The samples collected were divided in three fragments (Supplementary Fig. S1), which were placed in the same quantity of HistoCold solution (the ratio between the tissue fragment volume and the solution was 1:10), at constant temperature of 4°C for 24, 48, and 72 hours, respectively. The rationale for the chosen times is linked to the typical intervals between the activities of the surgical departments and the production rhythms of the histopathology laboratories, providing up to 72 hours for a sample taken during a surgery on Friday and accepted only the following Monday morning. At the end of every single time step, the tumor sample was moved into 4% neutral-buffered (pH 7) formaldehyde, in a ratio of 1:10, for 24 hours. Following the usual internal processing protocols, three paraffin tissue blocks and the corresponding slides needed for formulating a complete histopathological diagnosis were then obtained.
Afterward, the morphologic features of these samples were analyzed, with particular regard to mitotic count and histopathological grading (Table 1)—BCs: Elston and Ellis modified Scarff–Bloom–Richardson grade 12 ; as regards NSCLCs, for adenocarcinomas (ADCs) the pathologists evaluated the tumor architecture, particularly noting the main growth pattern present, which has been widely demonstrated to influence patient's prognosis.13–15 For squamous cell carcinomas (SQCCs) the analysis was based on the identification of keratinizing, nonkeratinizing, and basaloid subtypes of the neoplasms. 16 Concerning CRCs, the current histological grading systems were used, which divided the neoplasms into a low grade (encompassing both the well and moderately differentiated tumors, according to the glandular formation) and high grade (already the poorly differentiated neoplasms). 17
Morphologic Parameters Analysis
The grading was determined as follows: BCs: according to Elston and Ellis modified Scarff–Bloom–Richardson grade 12 a score was given by the sum of tubular/gland formation (points 1–3), nuclear pleomorphisms (points 1–3), and mitotic count (points 1–3). NSCLCs: the main growth pattern of ADCs13–15 and the histological subtype of SQCCs 16 were used to determine the NSCLCs grading. CRCs: according to the current histological grading systems. 17
ADCs, adenocarcinomas; BCs, breast cancers; CRCs, colorectal cancers; HPF, high-power field; NSCLCs, non-small cell lung cancers; SQCCs, squamous cell carcinomas.
Analysis of tissue antigenicity was evaluated by IHC stains, choosing monoclonal antibodies commonly used for diagnostic, prognostic, or predictive purposes for those specific types of tumors. The analysis focused on the percentage of tumor cells stained, and the intensity of the stains, as appropriate, the latter graded as mild, moderate, or strong. The IHC stains used are reported in Table 2. Concerning HER2 and PD-L1 interpretation, the guidelines in force at the time of the study were used.18,19
Immunohistochemical Antibodies
ER, estrogen receptor; PgR, progesterone receptor; RTU, ready to use.
Thereafter, the pathologists committed to the study (L.T. or M.M.) appropriately recovered from the specimens used for the official diagnosis the same parameters evaluated for the samples treated with HistoCold.
Afterward, the analysis of the tumor samples after 24, 48, and 72 hours of exposure in HistoCold produced a diagnosis, which was blinded to the official one. Then a comparative analysis between the two groups of diagnosis (HistoCold vs. routine) was performed. In the event of discrepancies, an expert pathologist in the field of neoplasms enrolled (R.C., R.D.S., G.B., or A.S.) convened to compare the discrepant diagnoses.
Descriptive statistics were performed using frequencies, percentages, frequency tables for categorical variables and the mean ± standard deviation for quantitative variables.
The data obtained from FFPE treated tissues, which represents the gold standard in pathology departments practice, and from samples evaluated after HistoCold handling were compared using Cohen's kappa coefficient (κ; absence of, poor, fair, good, and excellent agreement if κ value <0, 0–0.4, 0.4–0.6, 0.6–0.8, or 0.8–1, respectively) or the pairwise Pearson correlation method with Sidak adjustment to counteract the problem of multiple comparisons (ρ; weak, moderate, or strong correlation if 0 < |ρ| < 0.3, if 0.3 < |ρ| < 0.7, or if |ρ| > 0.7) and the Bland–Altman method, as appropriate if qualitative or quantitative variables had to be analyzed. The results were graphically rendered (GraphPad Prism 8 or Microsoft Excel 365). A value of p < 0.05 was considered to indicate statistical significance. Statistical analyses were performed using STATA 16.1 (Stata Statistical Software: Release 16, College Station, TX, USA).
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Comitato Etico Regionale Umbria (CER Umbria) (Protocol Code No. 3569/19, date of approval: September 26, 2019).
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
According to the internal rules of both the University of Perugia and the Hospital of Perugia, it was considered only the biological material that the patients expressed his/her specific informed consent to use, such as material for research purposes. All rules concerning confidentiality and protection of personal data were observed, in accordance with European Union, International, and National rules.
Results
Patients' series
Fifty-five (100%) cases were enrolled for the study: 20 (36%) of 55 were BCs, 15 (28%) lung ADCs, 10 (18%) lung SQCCs, and 10 (18%) CRCs. A total of 165 tissue blocks were prepared, after the tissue samples stayed in HistoCold for 24, 48, and 72 hours, for the subsequent morphologic, immunophenotypical, and molecular analyses. Fifty-five formalin-fixed tissue blocks, which were representative of the tumors, were selected and used as the gold standard for the comparative study.
Morphologic features: mitotic count
As regards the BCs, the correlation between the mitotic count of routine examined specimens (mean = 19.85 ± 16.75) and that treated with 24, 48, and 72 hours of HistoCold permanence (mean = 13.90 ± 14.86, 12.25 ± 15.13, and 8.9 ± 8.05, respectively) showed a statistically significant strong (ρ = 0.799; p < 0.001), strong (ρ = 0.836; p < 0.001), and moderate positive (ρ = 0.702; p = 0.003) relationship, respectively (Fig. 1a).

Morphologic features, mitotic count, and histopathological grading.
Concerning the NSCLCs, there were positive, strong, statistically significant correlations between the routine mitotic count (ADCs mean = 6.00 ± 7.46; SQCCs mean = 12.30 ± 5.81) and all the three times of HistoCold exposure (ADCs mean = 4.53 ± 5.82, 3.20 ± 4.83, 3.27 ± 4.25, respectively; SQCCs mean = 9.60 ± 7.06, 7.60 ± 6.38, 6.70 ± 5.98, respectively; Fig. 1a), among the ADCs group (ρ = 0.831, 0.789 and 0.815 for 24, 48, and 72 hours of HistoCold stay vs. routine, respectively; p < 0.001 for 24 hours and p = 0.002 and 0.001 for 48 and 72 hours of HistoCold permanence considered vs. routine). As regards the SQCCs series, there was a strong correlation, statistically significant, only between the mitotic count obtained from specimens treated for 24 hours with HistoCold stay and the routine ones (ρ = 0.818; p = 0.022).
The CRCs mitotic count showed a positive strong correlation, statistically significant only between the routine specimens (mean = 24.00 ± 8.92) and the ones treated for 48 hours with HistoCold (mean = 23.90 ± 9.60; ρ = 0.840; p = 0.014; Fig. 1a).
Morphologic features: histopathological grading
Among the BC series, there was a fair concordance between the routinely analyzed tissues and the HistoCold-treated ones (κ = 0.481, 0.438, and 0.460 after 24, 48, and 72 hours of HistoCold permanence, respectively; Fig. 1b).
An excellent agreement between the grading evaluation of routine specimens and the HistoCold-treated ones was demonstrated for the ADC series, regardless of the hours spent in the refrigerated solution (κ = 0.872 for all the three-time steps contemplated by the study; Fig. 1b). As regards the SQCCs, the agreement between the grading assessed analyzing the routinely prepared tissues and the specimens after 24, 48, and 72 hours of HistoCold permanence was either good or excellent (κ = 0.697, 0.697, and 1, respectively; Fig. 1b).
Concerning the CRC grading, all the findings of the tissues treated with HistoCold showed an excellent agreement (κ = 1) with the results obtained from routinely handled ones, showing 8 (80%) low-grade and 2 (20%) high-grade neoplasms as the routine specimens (Fig. 1b).
Overall, the morphologic artifacts have never been so serious as to hinder, even minimally, the correct diagnostic interpretation (Fig. 2a, b).
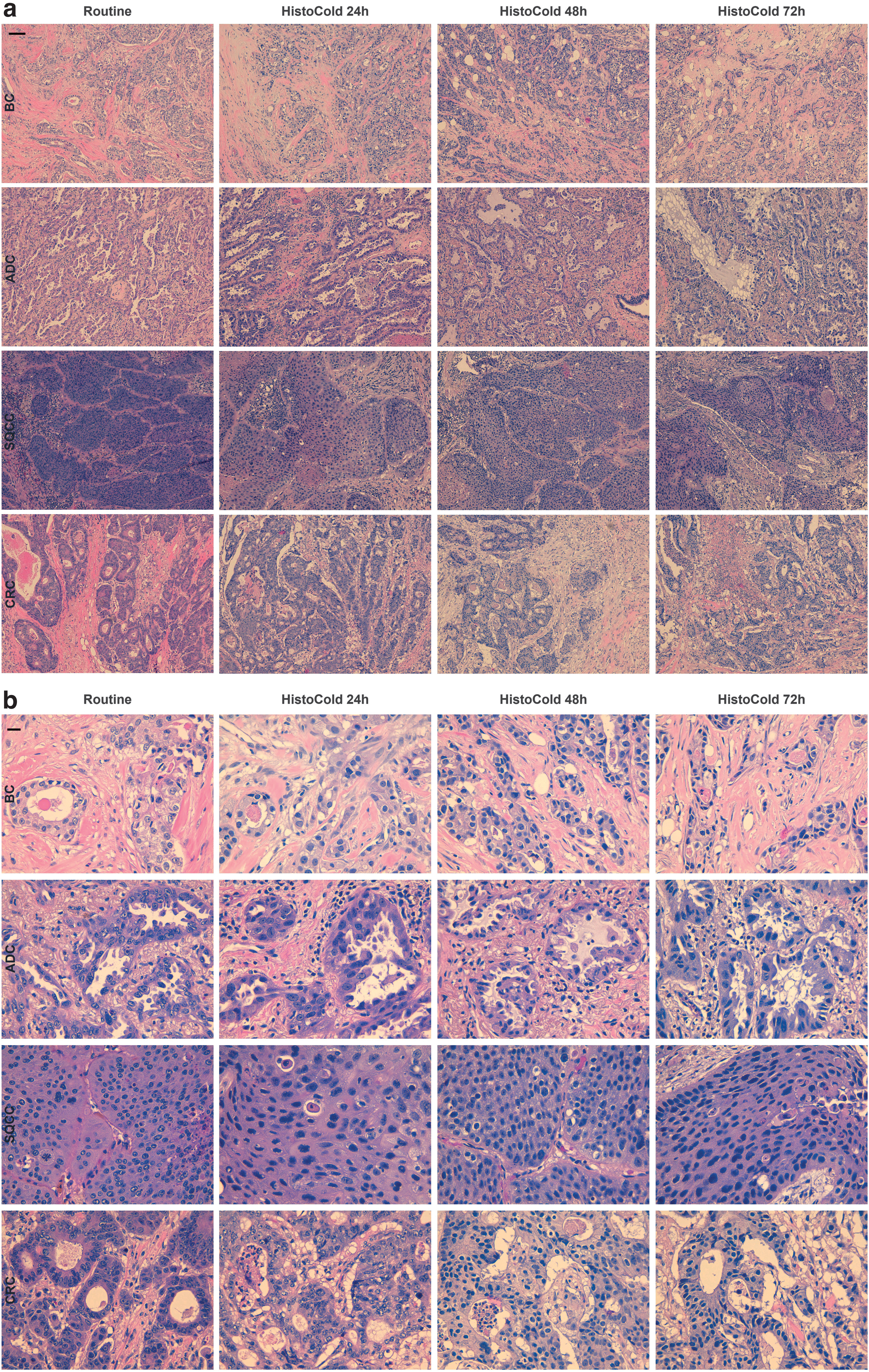
Morphologic features, histology.
Antigenic analysis
BCs: estrogen and progesterone receptors, Ki-67 proliferation index, and HER2 IHC analysis
There was an excellent concordance between the specimens routinely examined and the HistoCold-treated ones when the estrogen receptor (ER) class of expressions (<1% of tumor cells labeled = negative, 1%–10% = low positive, and >10% = positive 20 ) was considered for comparison (κ = 1; Fig. 3a), for all the 24, 48, and 72 hours of HistoCold exposure versus routinely treated tissues.

BCs antigenicity, analysis of ER and PgR.
Regarding progesterone receptor (PgR) expression, an excellent or good concordance between routinely handled tissues and the HistoCold-treated ones was found for this biomarker (κ = 0.875, 0.761, and 1.000, respectively for 24, 48, and 72 hours of HistoCold permanence vs. routine; Fig. 3b).
Concerning the evaluation of Ki-67, the correlation between the percentage of tumor cells labeled after 24 and 48 hours of HistoCold permanence (mean = 29.75 ± 17.43, 32.40 ± 15.35, respectively) and after routine processing (mean = 29.90 ± 16.08) was strong and statistically significant (ρ = 0.890 and 0.750; p < 0.001 and p < 0.001, respectively, for 24 and 48 hours of HistoCold permanence vs. routine; Fig. 3c).
When the concordance assessment shifted to HER2 status, the agreement between the results obtained after HistoCold treatment and routinely processed tissues went from good to fair with the passing of time in HistoCold (κ = 0.712, 0.578, and 0.485 for 24, 48, and 72 hours of HistoCold permanence vs. tissues routinely treated, respectively; Fig. 4).
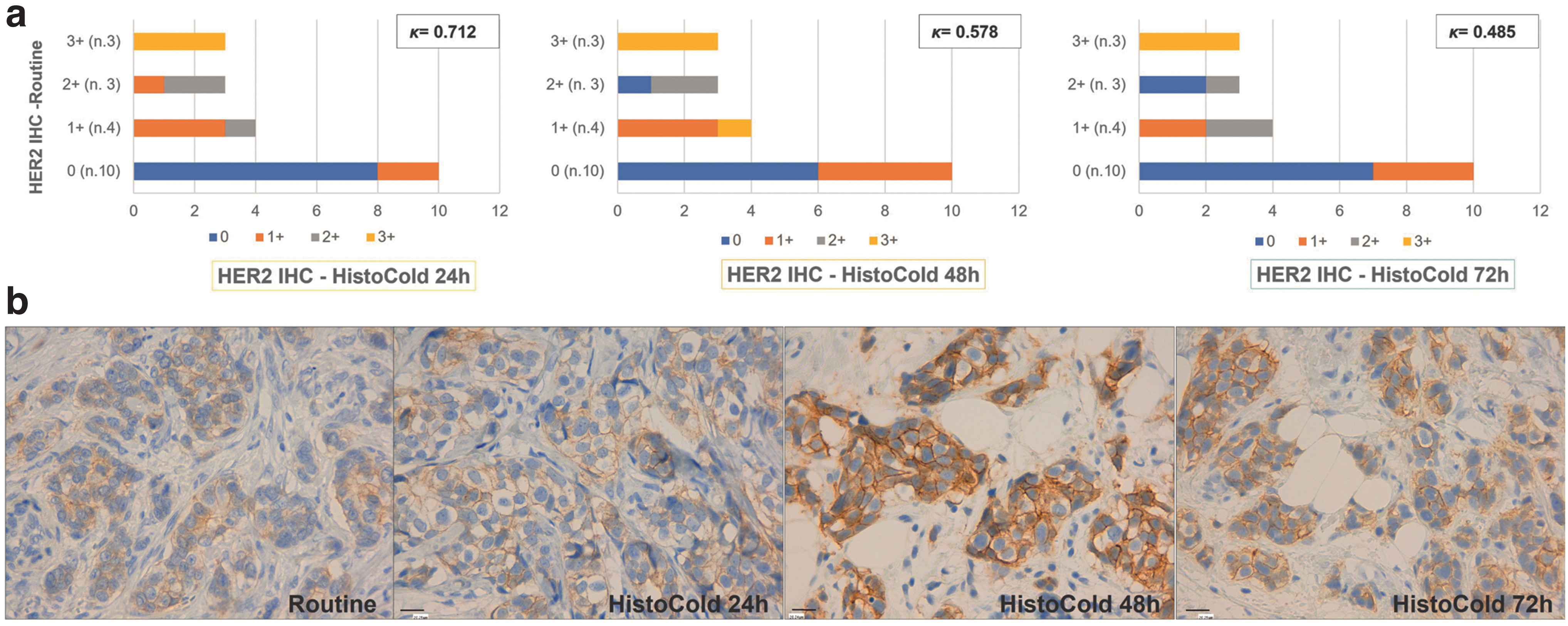
BCs antigenicity, analysis of HER2.
NSCLCs: TTF-1, p63, and PD-L1 IHC assessment
The TTF-1 assessment of ADCs after HistoCold treatment had a poor agreement with the results obtained from routinely processed specimens, of which one case (7%) resulted negative for this immunomarker after 24, 48, and 72 hours of HistoCold permanence (κ = 0 for all 24, 48, and 72 hours of HistoCold permanence vs. routinely processed specimen; Fig. 5a).

Antigenic analysis, NSCLCs.
On the contrary, all the 10 (100%) SQCCs examined presented p63 positivity after all HistoCold times of permanence when compared with the routine specimens (κ = 1; Fig. 5a).
The evaluation of the PD-L1 class of expression on ADCs gave good to excellent results regarding the agreement between the analysis of HistoCold-treated versus routine specimens (κ = 0.886, 0.783, and 0.783 after 24, 48, and 72 hours of HistoCold permanence vs. routine, respectively; Fig. 5b).
On the contrary, there was a fair agreement between the classes of PD-L1 expression determined in HistoCold-treated SQCCs tissues and those that resulted from the analysis of routine specimens (κ = 0.600, 0.600, and 0.455, after 24, 48, and 72 hours of HistoCold permanence vs. routine, respectively; Fig. 5b).
CRCs: CDX2 and MMR protein IHC determination
As regards the CDX2 IHC expression, the analysis of concordance (Fig. 6a) between cases resulted in CDX2 positives at routine examination (10 cases, 100%) and the ones positive after HistoCold treatment (10 cases [100%], 9 [90%], and 10 [100%] after 24, 48, and 72 hours of HistoCold permanence) gave excellent results for tissues treated with HistoCold both for 24 and 72 hours (κ = 1.000). Of note, the sample that had a negative result after 48 hours of HistoCold treatment was from the same patient who presented only 10% CDX2-positive tumor cells at routine examination.
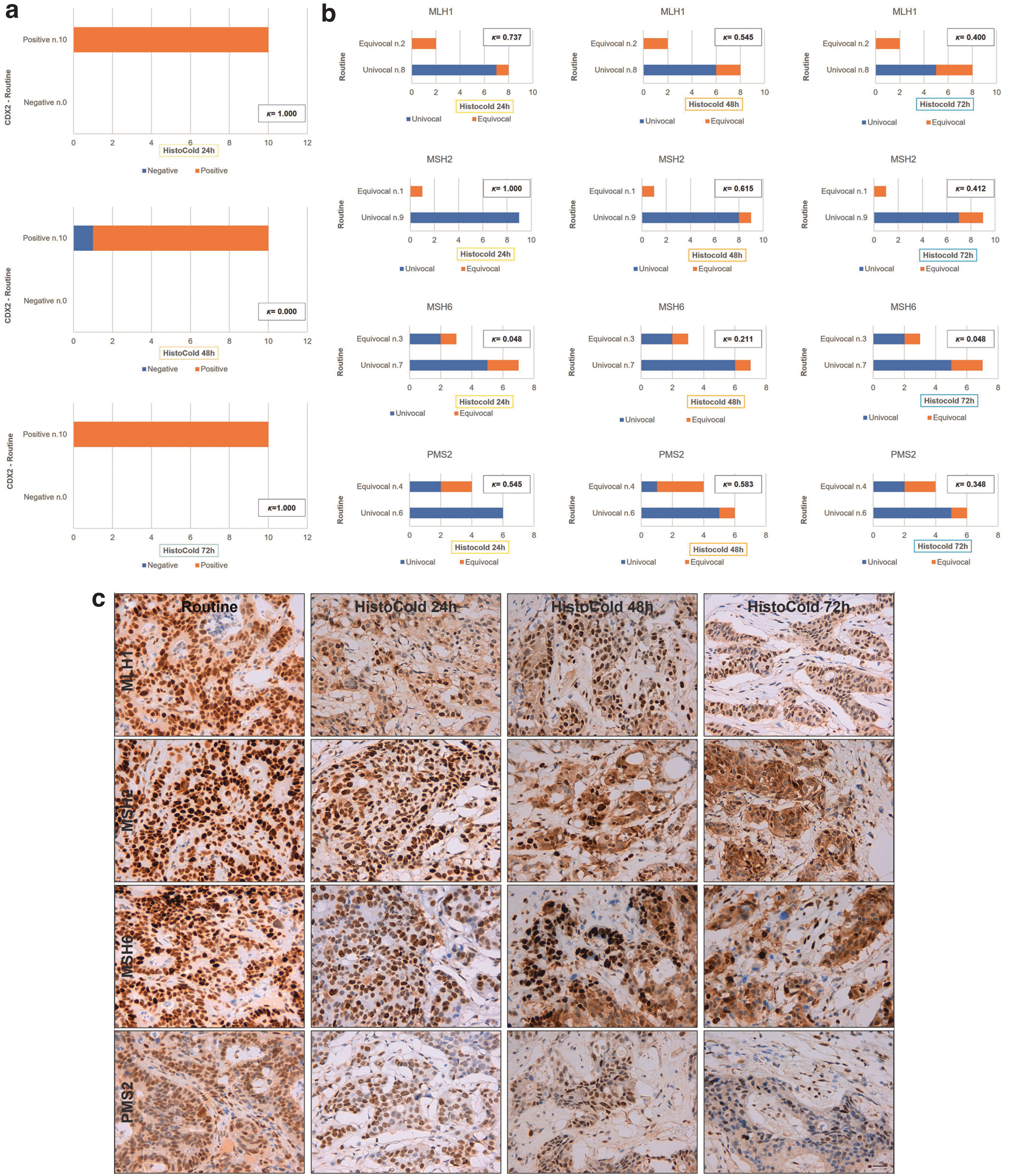
Antigenic study, CRCs.
The analysis of the expression of MMR proteins produced contrasting results, with better ones reached for the IHC analysis of MLH1 and MSH2 expression. For these two markers, the concordance of the results obtained from routine specimens was excellent or good, particularly when the tissues treated with HistoCold for 24 and 48 hours were compared with the diagnostic ones (κ = 0.737 and κ = 1 for both MLH1 and MSH2 analysis after 24 hours of HistoCold permanence, compared with routine, respectively; κ = 0.615 for MSH2 expression after 48 hours of HistoCold treatment compared with routine specimens; Fig. 6b).
Discussion
In the era of precision medicine, adequate tissue collection, fixation, handling, and storage is mandatory, both to ensure an accurate diagnosis and optimal sample biobanking.1–3 Unfortunately NBF, although believed to be the gold standard of tissue fixation, is far from the perfect fixative. In fact, in addition to the well-known problems related to cross links of nucleic acids and proteins, with potential negative impact on many assays, it is a recognized carcinogen,8,9 and the safety regulations in the workplace require a drastic reduction of exposure of health care workers to formalin vapors. Many attempts have been made to replace NBF but no reliable alternative has been identified. 21 A further and not least important problem related to NBF is that its use is not standardized and there is no obligation to identify preanalytic variables in routine clinical practice. In fact, the only recommendations about this issue that exist require only voluntary compliance.1,21
With this background, neither the time to, nor the time of, fixation are traced, therefore both over-fixations and under-fixations are very frequent with potential consequences in consistency and reproducibility of IHC and molecular assays conducted on FFPE samples.
In this scenario, this study compared the morphologic and antigenic characteristics of human tissues from BCs, NSCLCs, and CRCs pretreated with HistoCold solution or directly immersed into NBF during the preanalytic phase, to validate this nontoxic, stable, and refrigerated preservative solution, which was designed for avoiding tissue stress and allowing samples to be handled securely for preservation and transport to the pathology department.
As concerns the tissue morphology, although the correlations between the mitotic count obtained from routine specimens and HistoCold-treated ones were mostly strong and statistically significant, generally an underestimation of this parameters was found, particularly for longer stays in the solution and for BC samples. This affected the underestimation of histological grading of BCs, which is, in addition to other parameters, strictly related to the mitotic count. 12 However, for the evaluation of the mitotic count, the tumor heterogeneity must be considered, and the fact that its reproducibility is generally poor. 22 Counting a single less mitosis can determine the transition from one score to another, especially as concerns BCs, 12 and thereafter determine another histological grade. On the whole, the correlations obtained from the analysis of the mitotic count and the concordance between the resulting grading of routine and HistoCold-treated specimens were acceptable, allowing us to consider HistoCold as a valid potential substitute to NBF for tissue transport from the surgical rooms to the pathology departments.
Concerning the preservation of tissue antigenicity when HistoCold was used, encouraging results were reached. Regarding the class of expression of ER in BCs, 20 the concordance between those biomarkers determined after routine treatment and those resulting from HistoCold permanence was excellent, providing further evidence of the maintenance of tissue antigenicity after treatment with the HistoCold solution. Regarding PgR-positive BCs, 20 the agreement between the results determined on routinely managed tissue and the Histocold-treated ones were also strong, particularly with the passing of time, resulting in PgR determination completely in agreement with routine ones after 72 hours of HistoCold treatment.
However, some issues about hormone receptors expression in BCs must be considered, particularly when the percentage of tumor cells labeled is very low. In fact, the cutoff for the clinical benefit of endocrine therapy is 1% for both the receptors, 20 with a gray area concerning the ER expression (range of expression 1%–10% of tumor cells), which should be reported to the clinician as a warning that probably the patient may not benefit from the hormone therapy and the neoplasm could have a gene expression profile more similar to ER-negative cancers, unfortunately requiring chemotherapy as the appropriate treatment. Nevertheless, in our series, there were no cases that were low positive regarding ER, owing to the rarity of these neoplasms described in the literature (∼2%–3% of all ER-positive BCs 20 ). Consequently, further studies on a larger series seem appropriate to confirm data on hormone receptor expression obtained by tissues where HistoCold is used.
The results about the analysis of Ki-67 on BC tissues highlighted the good correlation between the percentage of tumor cells labeled after both NBF and HistoCold management, especially when the specimens experience a shorter time in this solution. After 48 hours of HistoCold exposure instead, the correlation, although still statistically significant, decreased and more specimens showed a higher percentage of Ki-67–positive cells. This aspect is of note, because there are still presently no universal cutoffs for Ki-67 percentage to be used to guide the BC patients' therapeutic choices, especially as regards chemotherapy by the identification of “luminal A” and “luminal B” breast cancer subtypes.23–26 In addition, the evaluation of Ki-67 suffers from intra- and interobserver poor reproducibility and validated automated methods for counting it do not exist at the moment.27,28 Furthermore, the immunomarkers tested for biopathological characterization of BCs depend on the tumor heterogeneity, which could explain the not completely overlapping results obtained from tissues processed routinely or with HistoCold.24,29,30
As regards the IHC evaluation of the crucial prognostic and predictive biomarker HER2 in BCs, 18 the comparison did not always produce good results, particularly for specimens treated for longer times with HistoCold. However, it should be specified that HER2 is usually a critical biomarker and a less stable antigen, which is already affected by problems during the preanalytic phase, such as delayed or prolonged fixation.31,32 In addition, most BCs present with a subset of genetic heterogenic HER2/Neu, which could contribute to positivity or negativity of IHC.24,29–31 This aspect should be considered in our series, in which the HER2 IHC analysis was performed on a different portion of the same neoplasms, although all derived from the same patient.
Moreover, HER2 IHC interpretation is very operator dependent, despite various attempts at its standardization have been made over the years with the constant update of international guidelines, and even if specimens were treated with the gold standard NBF during the preanalytic phase.18,33,34 Therefore, additional studies are needed to understand if the poor agreement of the results obtained is actually due to a negative effect of HistoCold on the HER2 protein expression, or is imputable to all the above-mentioned variables, which account for issues and controversies about HER2 IHC interpretation for decades.
Similarly, the results obtained comparing the antigenicity evaluation of NSCLCs either routinely treated or HistoCold managed were promising, particularly as regards the SQCCs. In those cases, testing nuclear antigens (p63 and TTF-1) and the lack of the need to report a percentage of IHC-labeled cells/immunolabeling scoring for these neoplasms could explain the better results obtained among these groups of patients.13,16 On the contrary, more variability was registered comparing PD-L1 expression of routine specimens and HistoCold-treated ones, a very useful biomarker in determining the eligibility of the patient suffering from NSCLCs to immunotherapy.35,36 This could be explained by the membrane staining of the tumor immunolabel and by the intrinsic heterogeneity of PD-L1 expression by tumor cells,35,37,38 which makes this biomarker susceptible to variations of intra- and interobserver interpretation, even in samples routinely processed with NBF.
The differences registered should be attributed to the tumor heterogeneity rather than a different expression of the biomarker owing to the different handling of specimens. Moreover, particularly as regards SQCCs, among which, routinely, no case of high expression of PD-L1 was found, the fair agreement reached comparing these cases with HistoCold-treated ones could be explained by the fact that was already demonstrated that pathologists are a source of variability in assessing PD-L1 expression, which should be considered especially regarding the low-expression PD-L1 category. 36
As mentioned previously concerning the nuclear antigens investigated on NSCLCs specimens, similar considerations can be made regarding the evaluation of CDX2 for CRCs, whose characteristic strong, diffuse nuclear staining in this type of cancer39,40 was found both in routine-handled tissues and HistoCold-managed ones, leading to an excellent agreement between its expression registered on these two types of materials.
Concerning the IHC analysis of mismatched repair proteins, important prognostic and predictive biomarkers in CRCs, 41 the data were variable, resulting in good to excellent concordance regarding MLH1 and MSH2 and a poor one for MSH6 and PMS2. Of note, our laboratory routinely experienced a more heterogeneous labeling, especially for PMS2 antibody and, consequently, difficulties in the IHC interpretation, according to the literature reports. In fact, incomplete data are available to propose clear guidelines on the interpretation of heterogeneous or discordant MMR IHC,41–43 although many efforts in organizing quality assessment programs have been made to overcome the issues related to a reduced/weak staining of MMR IHC resulting from suboptimal fixation.43,44 Despite the fact that a reduced series of CRCs has been examined in the current study, it could be speculated that the discordant results related to IHC assessment of MMR proteins are intrinsic in the method of analysis rather than in the procedure applied for transportation and fixation of the samples.
Conclusions
From the results obtained, bearing in mind the intrinsic limitations of the study linked both to the necessarily limited number of cases recruited and to the type of tumor sampling which, for ethical reasons, used the left over, with possible bias related to tumor heterogeneity, it could be said that:
The use of HistoCold as a means of sample transport from the operating room to the pathology department is easy and, together with surgeons' collaboration, it would improve the management of the cold ischemia time and the monitoring of the fixation times in NBF. The encouraging results reached in terms of conservation of tissue morphology and antigenicity are acceptable from the pathologist's point of view and do not undermine the diagnosis and the related biopathological characterizations. The need to eliminate formalin from operating theaters—unfortunately not from pathology departments!—should allow health workers to consider HistoCold as a useful aid in the daily activities of a hospital, in compliance with work safety regulations.
In conclusion, human tissues in the era of precision medicine are too precious to be mistreated in the preanalytic phase. On the other hand, even pathology must increasingly be a precision pathology, to provide the best possible service to patients and to scientific research. According to the results obtained, the use of HistoCold seems very promising in this regard.
Data Availability Statement
The datasets analyzed in this article are not publicly available, to respect the confidentiality and protection of patients' data, in compliance with the processing of data covered and protected by the Italian Privacy Law and by the GDPR (General Data Protection Regulation, EU regulation No. 2016/679). However, requests for access to a properly anonymized dataset of this article can be directed to M.M. (
Footnotes
Authors' Contributions
M.M., C.P., E.C., and A.S. performed study concept and design; M.M., L.T., C.P., E.C., and A.S. performed development of methodology; F.B., A.R., R.P., F.P., E.R., A.D., A.P., and P.B. provided informed consent and surgical resections; M.M., L.T., R.C., R.D.S., G.B., and A.S. performed histopathological and IHC analyses; C.F., C.P., and E.L. provided technical and material support; M.M. and L.T. performed acquisition, analysis, and interpretation of data; A.G. and M.M. performed statistical analysis; M.M., C.P., and A.S. performed writing, review, and revision of the article. All the authors read and approved the final version of the article.
Disclaimer
The funders had no role in the design of the study, or in the collection, analyses, or interpretation of data, in the writing of the article or in the decision to publish the results.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
The study received a nonconditional research grant from Bio-Optica Milano S.p.A. for the project entitled “Validazione del sistema di conservazione con soluzione refrigerata ‘Histocold,’ ” number of the project CBIO20ASID.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.