
Abstract
Objectives:
The aim of this study was to determine the cause of elevated serum potassium levels when blood collection tubes containing separating gel are stored under refrigeration.
Methods:
Fifty-seven hospitalized patients and 11 healthy volunteers were recruited. Venous blood samples were obtained using Insepac II, Neotube, and Venoject® II, without anticoagulant. After centrifugation under different processing conditions, the capped tubes were stored at 4°C without aliquoting, and serum potassium levels were measured for up to 14 days. Correlation between the increase in potassium levels and blood cell counts was assessed. Furthermore, serum was replaced with a saline solution and potassium levels were determined after refrigeration.
Results:
Refrigerated samples stored in Insepac II tubes had significantly higher serum potassium levels on day 14 than on the day of blood collection. The increase in serum potassium levels was positively correlated with the number of red blood cells, but not white blood cells and platelets in venous blood. Furthermore, potassium levels were elevated when serum was replaced with a saline solution. Using Venoject II, which has a larger tube diameter and thicker separating gel than those of Insepac II and Neotube, did not increase serum potassium levels after storage. Increase in the serum potassium level was markedly suppressed by centrifugation at 2330 g for 15 minutes relative to other processing conditions.
Conclusions:
Potassium levels increase when serum is refrigerated in collection tubes containing separating gel. This can be attributed to contamination of the serum layer by blood cell components beyond the separating gel.
Introduction
Serum specimens are usually stored in clinical laboratories where additional tests may be requested later. This is convenient because it eliminates the need to recollect blood from the patient. Conversely, the gold standard for achieving this objective is to aliquot and cryopreserve serum for different tests. However, the procedures for specimen preservation are not uniform and vary among facilities.
Serum gel tubes are shown to be more beneficial than plain serum and plasma tubes for specimen storage, 1 and most serum components showed no change for about 14 days after refrigerated storage.2,3 Particularly, Ikeda et al. 3 dispensed serum into multiple tubes, stored them at a given temperature, and evaluated the changes in each constituent. While this method can correctly assess changes in serum samples over time, it is difficult to implement such a method for multiple samples. In practice, facilities refrigerate serum in serum gel tubes without dispensing it into other tubes. In this study, serum and blood cells coexist in the same tube, separated by a separating agent.
Intracellular levels of the potassium ion (K+) are greater than extracellular levels, and hemolysis leads to a false positive impact. 4 Therefore, serum potassium in blood samples is unstable and samples should be centrifuged soon after blood collection. After serum separation, samples can be stored for 6 weeks if refrigerated. 5 Nevertheless, Dimeski et al. 6 showed an increase in serum potassium levels under prolonged storage of the tubes for 168 hours at 2°C–8°C; however, the cause is unclear.
In this study, we focused on the increased serum potassium when blood collection tubes containing the serum gel separator were refrigerated. We used methods simulating real-world conditions that could be implemented for specimen storage in hospitals. We hypothesize that this phenomenon is caused by hemolysis of red blood cells (RBCs) and aim to clarify whether it is due to (i) the RBCs in serum or (ii) the blood cell layer (blood clots) below the separating agent. We discovered that this could be attributed to contamination of the serum layer by blood cell components beyond the separating agent.
Materials and Methods
Subjects
Fifty-seven hospitalized patients [68 ± 15 years old (years ± standard deviation)] receiving medical care at the Hyogo Prefectural Rehabilitation Center at Nishi-Harima in Japan and 11 healthy volunteers [40 ± 7 years old] were included (Table 1 and Supplementary Table S1). All study participants provided informed consent.
Profile of Participants in This Study
SD, standard deviation.
The study was approved by the ethics committee of the Hyogo Prefectural Rehabilitation Hospital at Nishi-Harima (No. 2022) and performed in accordance with the principles of the Declaration of Helsinki.
Serum isolation and measurement of potassium and sodium levels
Venous blood samples were obtained using Insepac II (SMD750SQ; Sekisui Medical), Neotube (NP-SP0725; Nipro), and Venoject® II (VP-AS104K; TERUMO), without anticoagulant, as appropriate. These were mixed by inverting the tubes, left to stand at room temperature (between 15°C and 25°C) for at least 30 minutes, and then centrifuged at 2330 g for 7 minutes.
Primary serum potassium and sodium levels were measured using an automatic biochemical analyzer (TBA-120FR; Canon Medical Systems) (T0d, used for reference measurement). Thereafter, the capped tubes were stored at 4°C without aliquoting, and the same parameters were measured after 1, 3, 7, and 14 days (T1d, T3d, T7d, and T14d, respectively). The samples were not hemolytic, icteric, or lipemic.
RBC count in serum
Venous blood samples were collected using Insepac II tubes. Serum was separated by centrifugation using the method described above (2330 g for 7 minutes) and poured directly into a new conical tube. To collect all the RBCs remaining above the separator, 2 mL of fresh saline was added into the Insepac II tube, mixed by gentle inversion, and then poured into the conical tube.
The above steps were repeated, and the total volume (almost 6 mL) of the sample in the conical tube was centrifuged at 1400 g for 5 minutes. The supernatant was discarded, the pellet was suspended in 1 mL of saline, and the number of cells was counted using a Fuchs–Rosenthal counting chamber (Supplementary Fig. S1).
Measurement of potassium concentration in RBCs
Blood was drawn from a vein using a heparinized blood collection tube (BD Vacutainer, Becton, Dickinson and Company), and the RBC count was measured using an automated hemocytometer (XN-1000; Sysmex). Furthermore, the erythrocytes were diluted with saline and subjected to freeze–thaw cycles at −30°C to hemolyze erythrocytes. The potassium level in RBCs was measured using TBA-120FR.
Evaluation of the increase in potassium under different centrifugation conditions
Venous blood was collected in blood collection tubes containing a separator and centrifuged under specified conditions (1500 g for 10 or 15 minutes; 1710 g for 10 or 15 minutes; or 2330 g for 7, 10, or 15 minutes) using a centrifuge (5420; KUBOTA). Serum potassium levels were measured using a TBA-120FR clinical chemistry analyzer at T0d and T14d. Capped sample tubes were stored upright at 4°C.
Replacement of serum with a saline solution
Blood was collected intravenously in blood collection tubes containing a separator and centrifuged under specified conditions (1710 g for 10 minutes and 2330 g for 7, 10, and 15 minutes). Because the RBCs remaining in the serum at the top of the separator must be completely hemolyzed, the serum layer was discarded, replaced with 2 mL of sterile water, mixed, and allowed to stand for 6 hours at room temperature.
The upper layer was discarded and then 2 mL of saline solution was added to the tubes. The upper layer was used as the sample. The samples were then stored at 4°C for 14 days, and potassium levels were measured using TBA-120FR (Supplementary Fig. S2).
Cell count in venous blood
Blood was collected in an ethylenediaminetetraacetic acid (EDTA-2K) blood collection tube (BD Vacutainer, Becton, Dickinson and Company), and RBC, white blood cell (WBC), and platelet (PLT) counts were estimated using XN-1000.
Statistical analyses
The correlation coefficient ‘r’ was evaluated using the Pearson correlation method. We also assessed statistical significance using Student's t test, Dunnett's test, or Tukey's test, as appropriate, and considered a probability of <5% (p < 0.05) to be statistically significant. The statistical analyses were performed using EZR software, version 1.36, based on R and R commander. 7
Results
Serum potassium levels change after refrigerated storage
We first examined the changes in serum components after refrigerated storage (up to T14d) in blood collection tubes without dispensing serum. In this study, the serum potassium levels were significantly increased compared with that at T0d. To assess whether this increase was due to enrichment, changes in sodium levels of the same sample were examined. There was no change in serum sodium levels (Fig. 1) or the other parameters (data not shown).
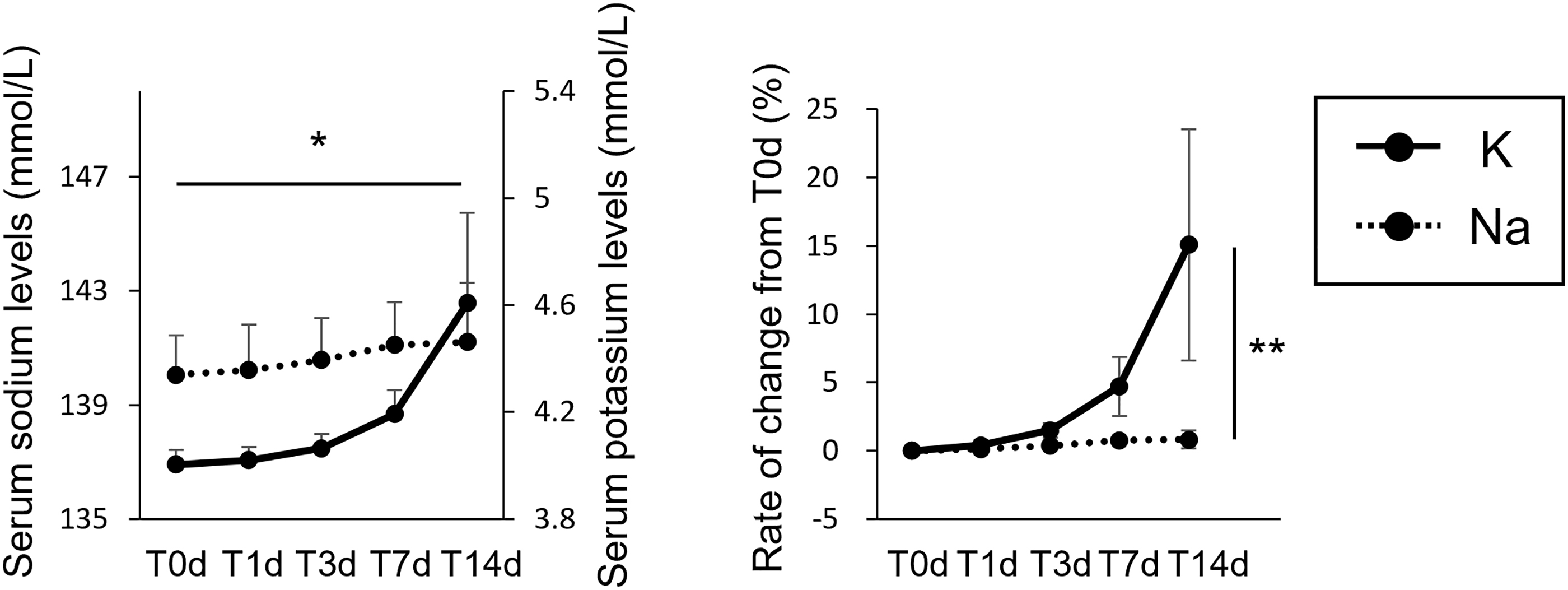
Change in serum potassium/sodium levels (mM) (left) and rate of change (%) (right) from the day of blood collection (T0d) up to T14d after refrigerated storage (N = 5). Values are shown as means ± standard deviations (SDs). Statistical significance was determined using Dunnett's test. *p < 0.05 (vs. serum potassium levels at T0d). **p < 0.05 (vs. the rate of change from T0d to T14d in serum sodium levels).
We next expected the serum layer to not be sufficiently separated due to inadequate coagulation caused by the antithrombotic medication, leading to an increase in serum potassium after refrigerated storage. However, the increase in serum potassium levels after refrigerated storage was stronger in nonusers than in users of antithrombotic drugs, and both groups showed a clear increase in serum potassium levels after refrigerated storage (Supplementary Fig. S3).
Therefore, this phenomenon may be independent of enrichment by evaporation and antithrombotic medications; however, these results need further validation due to the small sample size.
Relationship between the increase in serum potassium levels and number of serum RBCs
Next, we hypothesized that the increase in serum potassium levels during refrigerated storage was due to hemolysis of RBCs. We confirmed the presence of fresh RBCs after centrifuging the serum again (Fig. 2A); however, there was no correlation between the amount of increase in serum potassium levels and the number of serum RBCs (r = 0.014, Fig. 2B).
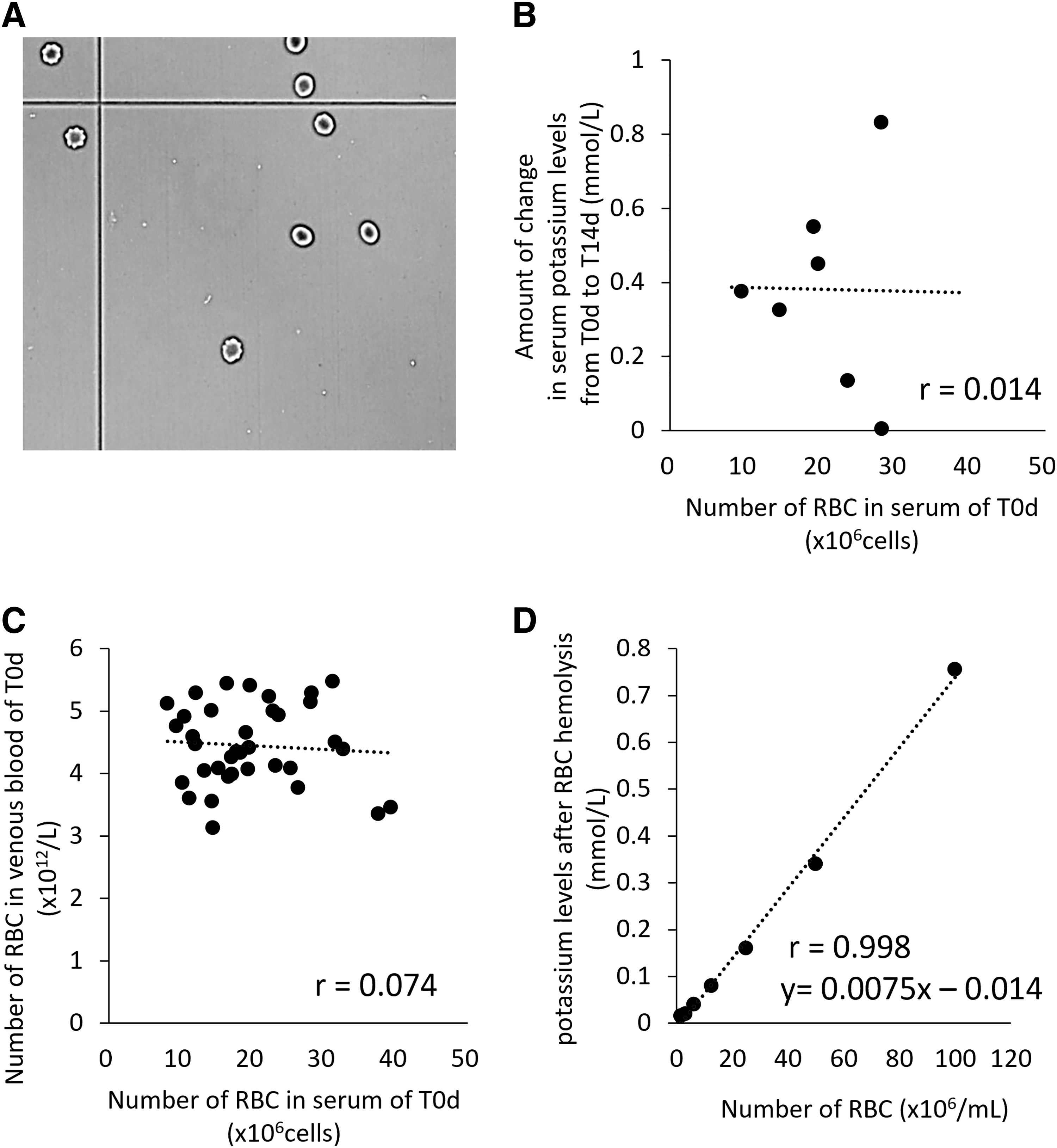
Relationship between the increased serum potassium levels from the day of blood collection (T0d) up to T14d and the number of RBCs in serum.
Furthermore, heparinized blood was serially diluted to determine the amount of potassium due to erythrocyte hemolysis. The potassium value (mM) is expressed as [0.0075 × erythrocyte count (cells/mL) −0.014] (Fig. 2D). Because the mean serum RBC count was almost 20 × 106 cells (Fig. 2C), even when all of the cells were hemolyzed, the calculated potassium level due to hemolysis was less than 0.15 mM (Fig. 2D).
In this experiment, RBCs were suspended in 1 mL of saline, but assuming that the Insepac II blood collection tube could collect ∼2 mL of serum, the levels of potassium would have been further reduced. These results suggest that the increased serum potassium levels were not due to hemolysis of RBCs in serum.
Relationship between the increase in serum potassium levels and number of RBCs in venous blood
We further speculated that a part of the blood cell layer (blood clots) might have passed through the separating gel into the serum, leading to an increase in serum potassium. Indeed, there was a positive association between the amount of increase in serum potassium levels and the number of RBCs (r = 0.366), but not WBCs and PLTs (r = 0.014 and r = 0.044, respectively), in venous blood (Fig. 3).
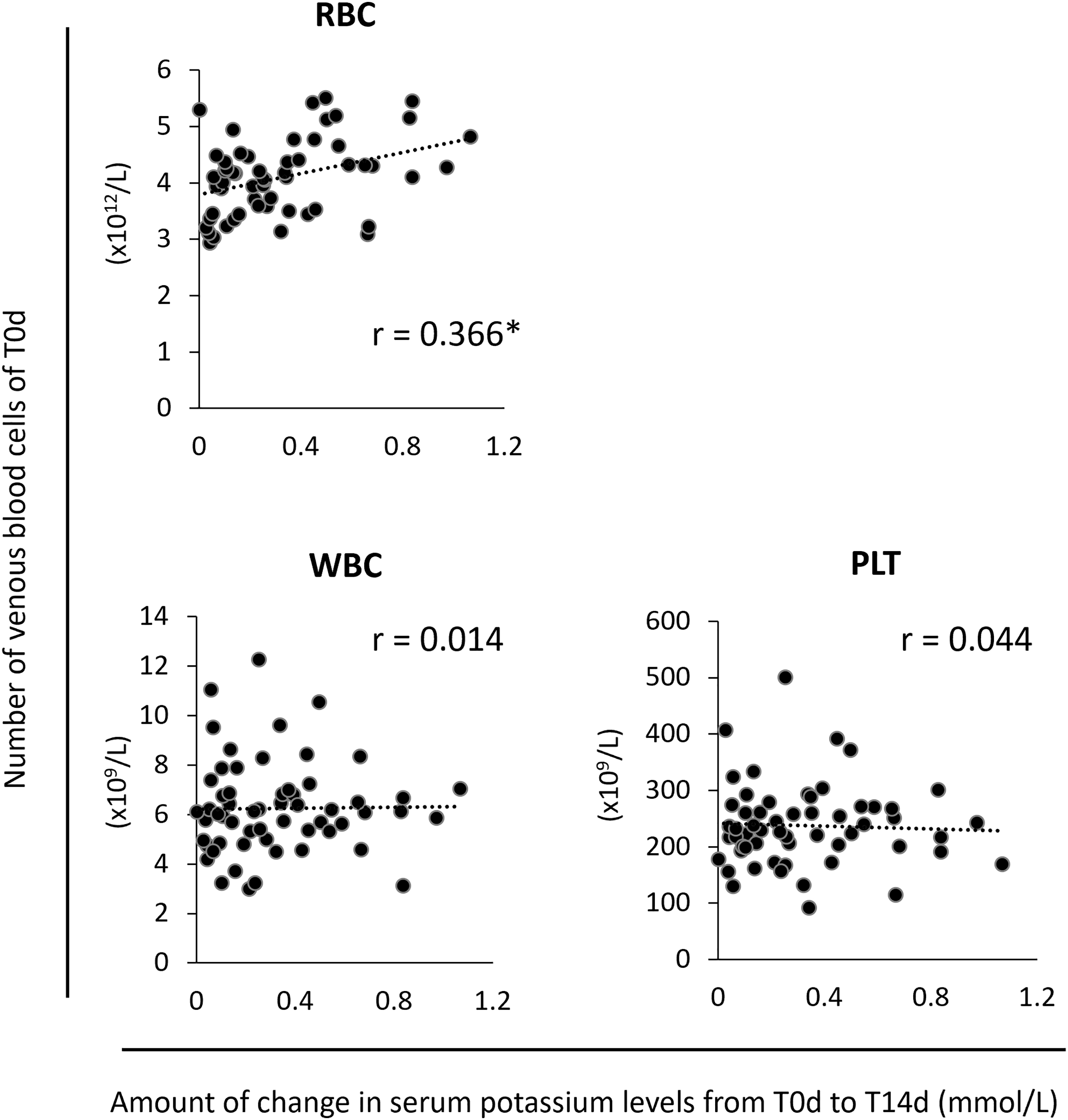
Correlation between the amount of change in serum potassium levels from T0d to T14d and the number of venous blood cells (RBCs, WBCs, and PLTs) at T0d (N = 57). Statistical significance was determined using the Pearson correlation method. *p < 0.05. PLT, platelet; WBC, white blood cell.
Conditions that prevent an increase in serum potassium levels after refrigerated storage
Next, we examined whether the increase in serum potassium level could be suppressed by changing centrifugation conditions from 2330 g for 7 minutes to 1500 g, 1710 g, or 2330 g for 10 minutes or 15 minutes. The increase in the serum potassium level was markedly suppressed by centrifugation at 2330 g for 15 minutes compared with other conditions, including 2330 g for 7 minutes and 10 minutes and 1500 g for 10 minutes (Fig. 4A).
Differences in the increase in serum potassium levels due to centrifugation and type of blood collection tube. The experiments were conducted using healthy volunteers, values are shown as means ± standard deviations (SDs), and statistical significance was evaluated using Tukey's test. *p < 0.05.
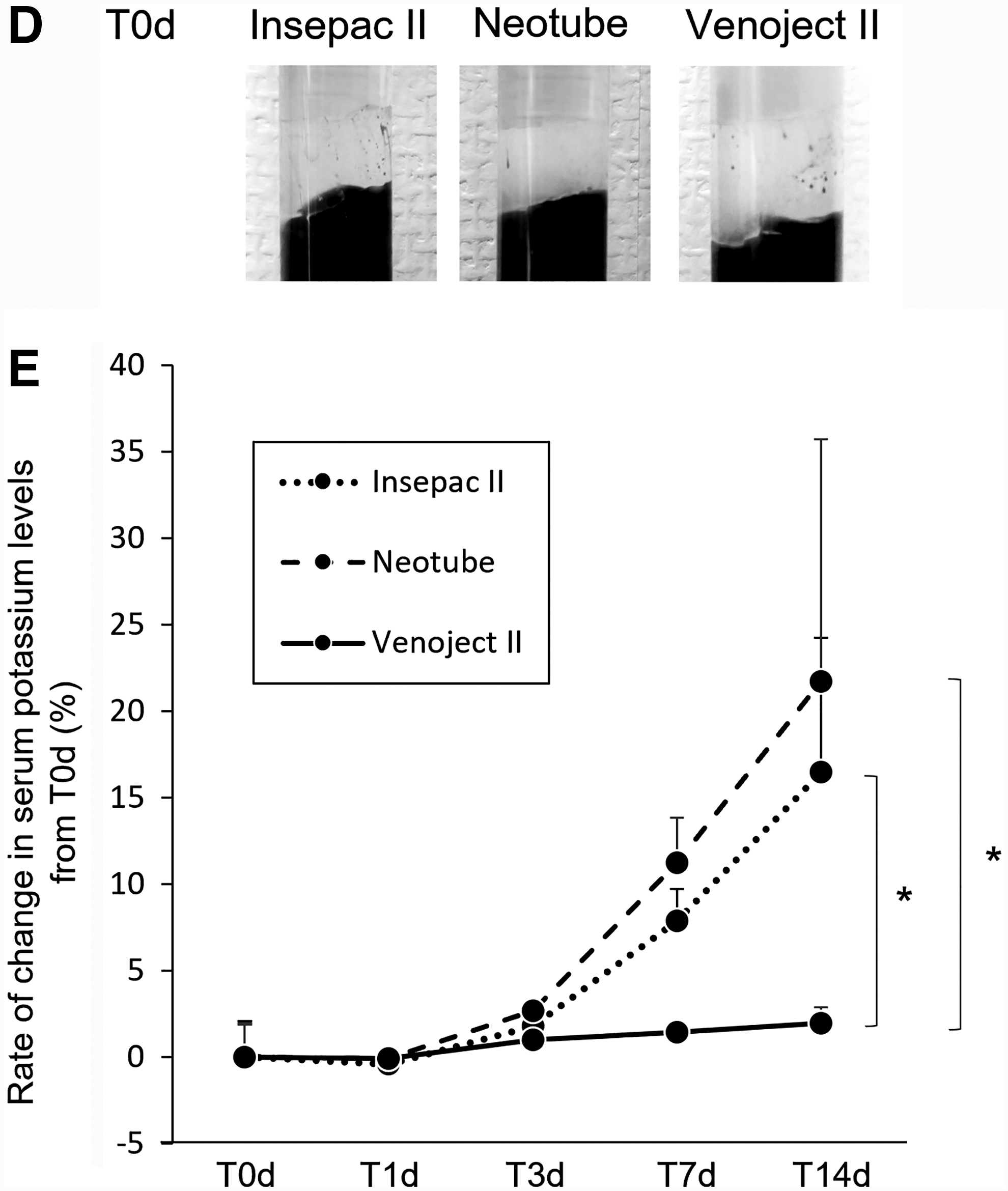
Next, the serum layer on top of the separator was discarded, the sample was washed, and serum was replaced with a saline solution to examine whether the components of the blood cell layer passed through the separating agent. The sample was then refrigerated for 14 days, and the change in potassium level was measured. Although nothing abnormal was observed immediately after washing, after 14 days of refrigerated storage, the hemoglobin pigment was visually observed under the separating gel (Fig. 4B).
The potassium concentration in this sample was increased, but the increase was suppressed in the sample centrifuged at 2330 g for 15 minutes (Fig. 4C). Therefore, we focused on the amount of separating gel in blood collection tubes (Fig. 4D). Similar to Insepac, mainly used in this study, the increase in serum potassium levels after refrigerated storage was also observed in Neotube, in which the thickness of the separating gel was comparable with that of Insepac.
In contrast, samples stored in Venoject II tubes, in which the diameter of the tube was wider and the separating gel layer was thicker than those of Insepac and Neotube tubes, did not show an increase in serum potassium levels (Fig. 4E).
Discussion
Serum potassium levels increase when serum is refrigerated in blood collection tubes. In this study, we showed that this increase is caused by mixing of blood components from the blood cell layer with the serum beyond the separating agent.
On the other hand, Ikeda et al. 3 reported that serum potassium levels did not change after refrigerated storage for up to 14 days. Serum components were evaluated over time by dispensing and freezing serum in separate containers, dissolving it for each measurement, and quantifying it at each time point. 3 This method can evaluate changes in serum components only; however, in actual clinical laboratories, serum is often stored in vacuum collection tubes without dispensing it.
Conversely, Kift et al. 8 reported a significant increase in serum potassium after 4 days of storage at 4°C without a lid. An increase in sodium levels was also observed; hence, we consider this to be a significant effect of enrichment due to evaporative concentration. In contrast, we found that the serum potassium level increased over time, while that of sodium remained unchanged, when the tubes were refrigerated with the lid on and not aliquoted. The difference between our storage conditions and that of the others is that serum is not dispensed into a separate container, but is stored in the blood collection tube without dispensing it.
Therefore, we first speculated that the cause of the increased serum potassium level is hemolysis of RBCs. We expected hemolysis of RBCs in serum. However, when the number of RBCs and the corresponding change in potassium level were assessed, the actual increase in potassium level was not found. Moreover, there was no correlation between the number of RBCs in serum and increase in potassium. Therefore, we inferred that the increase in serum potassium was not due to hemolysis of RBCs in serum.
Next, we focused on the blood cell layer that existed below the separator. A positive correlation was found between the whole blood RBC count and increased serum potassium levels, but not WBCs and PLTs. Furthermore, we then centrifuged venous blood, replaced the serum layer above the separator with a saline solution, and measured potassium levels after refrigerated storage for 14 days.
We could not visually observe any obvious change in the top of the separating gel after replacement of the saline solution and refrigeration for 14 days; however, potassium was detected. This suggested that the increased serum potassium level was due to contamination from the blood cell layer beyond the separating agent into the serum.
It remains unclear why this phenomenon occurred in this study. However, we speculate that some of the components that should have been separated as serum remain in the blood cell layer due to the rather low centrifugal strength (e.g., 2330 g for 7 minutes). Consequently, these components pass through the separating gel and enter the serum layer, while potassium released by hemolysis in the blood cell layer during refrigeration may have entered the serum layer simultaneously.
Practically, the depth of the serum layer was significantly greater when centrifuged at 2330 g for 15 minutes than at 2330 g for 7 minutes; conversely, it was significantly less in the clot layer (Supplementary Fig. S4). This result suggested that the centrifugation condition of 2330 g for 7 minutes is insufficient for the amount of serum that should be obtained.
Measures taken to control this phenomenon showed that the increase in potassium levels could be suppressed by performing centrifugation and by selecting blood collection tubes that contained a large amount of separating agent. The serum separator materials include acrylic, polyolefin, and polyester, and these compounds affect blood drug concentrations.9,10
The three types of blood collection tubes used in this study were polyolefin based for Insepac and Venoject and polyester based for Neotube. In this study, the increase in serum potassium levels on refrigeration was observed for Insepac and Neotube, but not for Venoject, suggesting that this phenomenon was not due to the material of the serum separator.
Furthermore, in this study, the centrifugation condition of 2330 g for 15 minutes was effective in suppressing the increase in potassium levels after refrigerated storage. Although WHO guidelines recommend centrifuging the sample for at least 10 minutes at a minimum speed of 1500 g, 5 in this study, the potassium level was significantly increased after 14 days of refrigerated storage (Fig. 4A).
Further studies are needed to determine if this phenomenon occurs with other acrylic blood collection tubes and centrifugation conditions.
Similar to potassium, lactate dehydrogenases, especially LDH1 and LDH2, are clinical chemistry parameters that are increased by hemolysis. 11 Although an isozyme analysis was not performed in this study, it is possible that these also increase with refrigeration, and we plan to assess the effect of refrigeration on isozyme levels in future studies.
This study has some limitations. The sample size for this study was small. We believe that further study needs to be conducted with a larger sample size. The centrifuge we used in this study does not have a cooling function, and we did not examine the increase in chamber temperature due to increased centrifugation time.
However, since the increase in serum potassium values after refrigerated storage was suppressed by the strongest centrifugation conditions, we think that the temperature in the centrifuge had little effect on this phenomenon. We have not included all blood collection tubes in our study. The material and volume of the serum separator in blood collection tubes vary among manufacturers, and the tubes used vary among the facilities.
In addition, there were seven different centrifugation conditions and times tested in this study, and we concluded that 2330 g for 15 minutes was the most ideal among them, but more suitable conditions may be found by setting detailed parameters. It is necessary to determine the extent to which the results of this study occur, that is, the increase in serum potassium levels due to refrigerated storage, depending on the tubes and centrifugation conditions used at each facility.
In conclusion, we showed that serum potassium levels increase when serum is refrigerated in the collection tube, which can be attributed to contamination of blood cell components in serum beyond the separating gel.
Footnotes
Acknowledgments
Authors' Contributions
All authors were involved in drafting the article and revising it critically for important intellectual content. All authors approved the final version of the manuscript to be published. K.Y. has full access to all of the data in the study and takes responsibility for the integrity of data and accuracy of the data analysis. Study concept and design were done by K.Y. Acquisition of data was done by K.Y., H.T., S.N., and S.Y. Analysis and interpretation of data were done by K.Y.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partly supported by the KUROZUMI MEDICAL FOUNDATION (to K.Y.).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.