
Abstract
This publication reports, for the first time, the birth of a healthy child after intracytoplasmic sperm injection (ICSI) of motile spermatozoa after conventional (“slow”) freezing of epididymal spermatozoa using 5% polyvinylpyrrolidone (PVP) of high molecular weight (360 kDa). Cryopreservation solution with 10% PVP was added to 30 µL of spermatozoa suspension in a 1:1 ratio, with a final PVP concentration of 5%. Then, polycarbonate capillaries for oocyte denudation with a diameter of 170 µm were filled with 60 µL of the resulting sperm suspension. After that, the capillaries were placed for 10 minutes at a height of 15 cm above liquid nitrogen and immersed into liquid nitrogen. To warm the spermatozoa, the capillaries were immersed in a water bath at a temperature of 40°C for 30 seconds. Oocyte fertilization was performed by ICSI. Zygotes were cultured in vitro for 5 days to the blastocyst stage. More than 100 spermatozoa were obtained after percutaneous epidydimal sperm aspiration, of which 80% were motile. After cryopreservation, storage for 3 months in liquid nitrogen, and thawing, 72% of the total sperm cells remained motile. Ten oocyte–cumulus complexes were found after follicle puncture, and eight metaphase II stage oocytes were fertilized using ICSI. After 18 hours, two pronuclei were found in seven (88%) of the oocytes. An analysis of the morphological characteristics of 5-day-old embryos showed that four (57%) of them reached the blastocyst stage. One embryo was transferred, and the remaining embryos were cryopreserved (vitrified). The onset of pregnancy was detected on the 14th day after embryo transfer, and one healthy girl (3300 g) was born at term.
Introduction
It is known that human spermatozoa with abnormal spermatogenesis (oligoastenoteratozoospermia) are extremely sensitive to the negative effects of permeable cryoprotectants.1,2 In recent years, researchers have been trying to invent new methods for cryopreservation of both epididymal and oligoasthenoteratozoospermic spermatozoa, if only a few male spermatozoa can be detected in the ejaculate.3,4
Previously, comparative studies of two cryopreservation technologies for spermatozoa of men with oligoasthenoteratozoospermia have been conducted: standard conventional freezing with 5% glycerol and freezing with 5% high molecular weight (360 kDa) polyvinylpyrrolidone (PVP). 5 It has been shown that for low-quality spermatozoa, the use of a nonpermeable cryoprotectant is preferable to the “standard” traditional cryopreservation with a permeable cryoprotectant (in this case, glycerol). 5
The purpose of this publication is to report, for the first time, the birth of a healthy child after intracytoplasmic sperm injection (ICSI) of motile spermatozoa after conventional (“slow”) freezing of epididymal spermatozoa using 5% PVP with high molecular weight (360 kDa).
Materials and Methods
All studies were performed in accordance with the principles of the Helsinki Declaration of Human Rights, the European Union Convention on Human Rights and Biomedicine, European Society of Human Reproduction and Embryology, and American Society for Reproductive Medicine recommendations, and approved by the Institutional Bioethics Committee No. 4, 2016, and No. 1, 2021. Written informed consent was obtained from both participants.
The 33-year-old male patient underwent a general andrological examination: semen analysis, hormone tests, and cytogenetic analysis of peripheral blood lymphocytes. After percutaneous epididymal sperm aspiration (PESA), the obtained aspirate was placed in semen preparation medium (Cook Medical LLC, Bloomington, IN, USA) to collect progressively motile fractions. Sperm preparation was carried out by density gradient separation according to the Sydney IVF Protocol (Cook Medical), followed by an ascent procedure.
Cryopreservation solutions were prepared with the protein-free, HEPES buffered base medium LGGH-500 (CooperSurgical, Ballerun, Denmark). This cryopreservation solution, containing 10% PVP, was added to 30 µL of spermatozoa at a 1:1 ratio (final PVP concentration, 5%). Then, polycarbonate capillaries for oocyte denudation with a diameter of 170 μm (Cook Medical) were filled with 60 μL of the resulting sperm suspension using an oocyte stripper (Cook Medical). The capillaries were detached from the stripper, and both free ends were sealed with medical clay (Becton Dickinson Co., Franklin Lakes, NJ, USA). The sealed capillaries were then placed in 5 mL cryovials (Thermo Fisher Sci., Schwerte, Germany) at 5 capillaries/cryovial, exposed to room temperature for 10 minutes, suspended 15 cm above liquid nitrogen for 10 minutes, and then immersed in the liquid nitrogen.
To thaw the spermatozoa, the cryovials were opened in liquid nitrogen, the capillaries removed, and then immersed in a water bath at 40°C for 30 seconds. Both sealed ends of the capillaries were cut, and the sperm suspension was pushed into a 1.5 mL microtube (Eppendorf, Wesseling-Berzdorf, Germany).
Oocytes at the metaphase II (MII) stage were retrieved from the female patient (30 years old). Ovarian stimulation commenced on the second day of the menstrual cycle with follicle-stimulating hormone (Gonal F®, Merck Serono Int., Genf, Switzerland) and gonadotropin-releasing hormone antagonist (Cetrotide®, Merck Serono Int.). Oocyte fertilization was performed by ICSI. The zygotes were cultured in vitro for 5 days to the blastocyst stage in LifeGlobal® culture medium (CooperSurgical, Los Angeles, CA, USA) in four-well Nunc® plates (Merck GmbH, Darmstadt, Germany).
Results
More than 100 spermatozoa were obtained after PESA (Fig. 1, upper left), of which 80% were motile. After cryopreservation and storage for 3 months in liquid nitrogen and thawing, the proportion of motile spermatozoa was 72%.
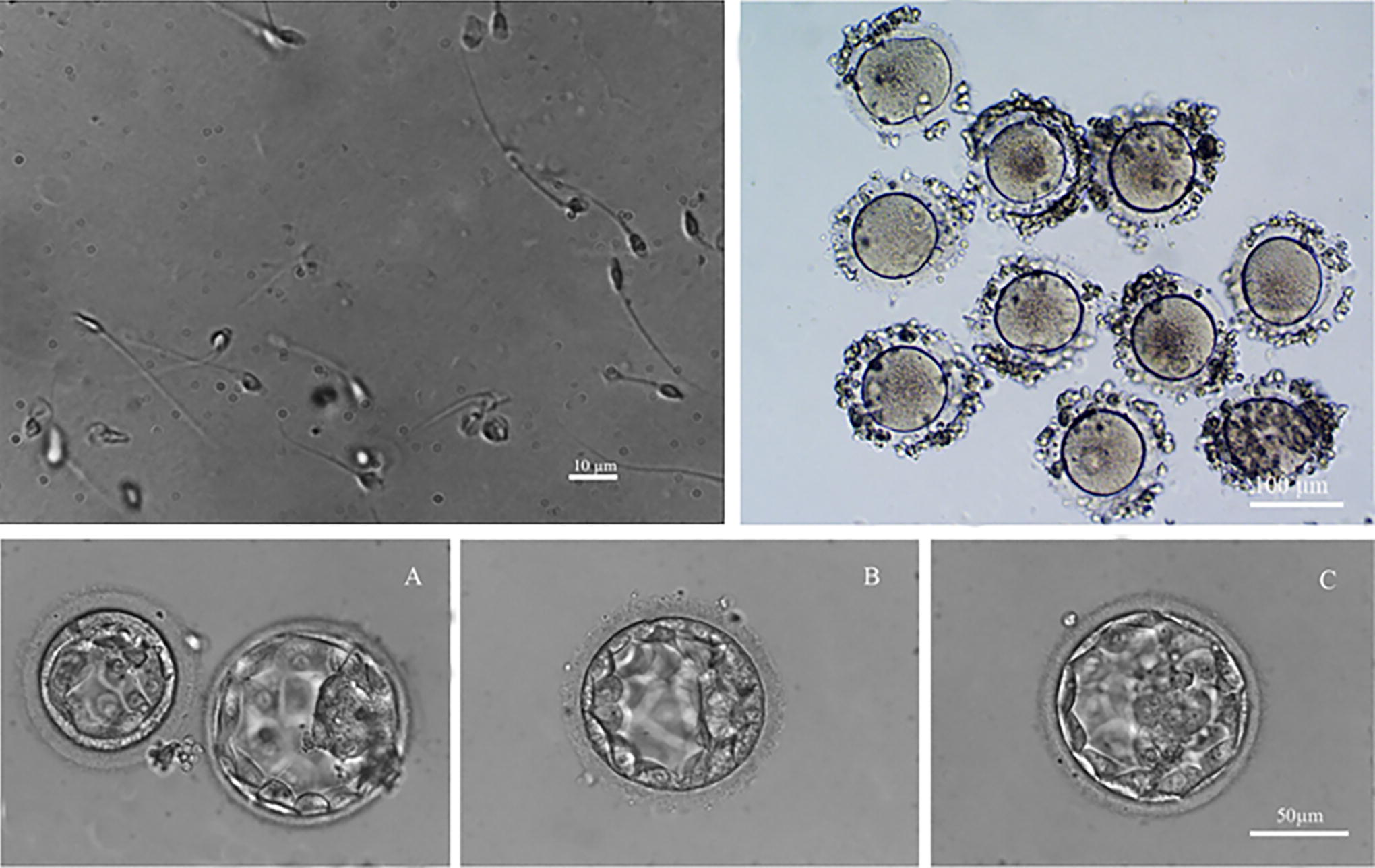
Patient M: Results after cryopreservation of spermatozoa. (Upper left) Epididymal spermatozoa of Patient M. after cryopreservation. (Upper right) Ten oocytes of Patient M. after maturation: eight of them were matured to MII stage. (Below) Day 5 embryos of Patient M. obtained after fertilization of MII oocytes with cryopreserved spermatozoa of the husband (Patient M.). (A right) Transferred blastocyst. (A left, B, C) rest of cryopreserved (vitrified) embryos. MII, metaphase II.
Ten oocyte–cumulus complexes were found after follicle puncture in the patient (Fig. 1, upper right), and eight MII oocytes were fertilized using ICSI. After 18 hours, two pronuclei were found in seven (88%) of the oocytes. An analysis of the morphological characteristics of 5-day-old embryos showed that four (57%) of them reached the blastocyst stage (Fig. 1A–C). One embryo (Fig. 1A, right) was used for transfer, and the remaining embryos were cryopreserved (vitrified) (Fig. 1A, left, B, C). The onset of pregnancy was detected on the 14th day after embryo transfer, and one healthy girl (3300 g) was born at term.
Discussion
PVP has been used in medicine since it was first synthesized in 1939. It belongs to the class of artificial polymers and is a polymerization product of vinylpyrrolidone. The dehydration properties of PVP are a consequence of the substance’s chaotic spiral configuration, which facilitates the binding of water molecules to prevent ice formation. 6 When used in a cryopreservation medium, this polymeric substance stabilizes the cell membrane because intracellular components are protected from ice crystal formation (osmotic stress). 7
Standard 10% PVP with a molecular weight of 360 kDa is routinely used in artificial reproductive technologies using ICSI. It has been shown that PVP is neutral for cells and does not lead to irreversible changes in the cellular structure. All these features of PVP make it promising for use as a cryoprotectant for freezing spermatozoa with reduced morpho-kinetic characteristics. PVP is approved for use in medical practice by the European Medicines Agency and the Food and Drug Administration, USA.
Most commonly used cryoprotectants are permeable. The four most widely used are glycerin, ethylene glycol, propylene glycol (three high molecular weight alcohols), and dimethyl-sulfoxide (DMSO). Permeable cryoprotectants penetrate the cell and bind water, preventing the formation of intracellular crystals.
There are also many nonpermeable cryoprotectants that work by dehydrating the cell and thereby indirectly prevent the formation of intracellular ice crystals. In addition, there are other types of cryoprotectants that mechanically bind extracellular water and also indirectly prevent the formation of intracellular crystals. The main difference between permeable and nonpermeable cryoprotectants is that the latter a priori do not have a toxic effect on intracellular organelles. Nonpermeable cryoprotectants include many sugars and polymeric high-molecular structures (including proteins). In principle, the cytoplasm of a cell is saturated with nonpermeable cryoprotectants, and it is generally impossible to find a cell free of nonpermeable cryoprotectants. This can explain the increased cryo-resistance of enveloped viruses. 8
This is the first report of the birth of a healthy baby after ICSI using motile epididymal spermatozoa, thawed after conventional (“slow”) freezing in 5% high molecular weight (360 kDa) PVP cryopreservation medium.
Footnotes
Authors’ Contributions
Conceptualization and visualization by M.P., and V.I. Methodology and investigation by M.P., T.Y., V.P., E.I., G.R., P.M., and V.I. Resources, writing, review, editing, and funding acquisition by V.I. and M.P. Data curation, writing, original draft preparation, supervision, and project administration by M.P., P.M., K.R., and V.I. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study has not financial supporting.