
Abstract
We support the notion that the neural connections of the tumor microenvironment (TME) and the associated ‘bioelectricity’ play significant role in the pathophysiology of cancer. In several cancers, the nerve input promotes the cancer process. While straightforward surgical denervation of tumors, therefore, could improve prognosis, resulting side effects of such a procedure would be unpredictable and irreversible. On the other hand, tumor innervation can be manipulated effectively for therapeutic purposes by alternative novel approaches broadly termed “electroceuticals.” In this perspective, we evaluate the clinical potential of targeting the TME first through manipulation of the nerve input itself and second by application of electric fields directly to the tumor. The former encompasses several different biophysical and biochemical approaches. These include implantable devices, nanoparticles, and electroactive polymers, as well as optogenetics and chemogenetics. As regard bioelectrical manipulation of the tumor itself, the “tumor-treating field” technique, applied to gliomas commonly in combination with chemotherapy, is evaluated. Also, as electroceuticals, drugs acting on ion channels and neurotransmitter receptors are highlighted for completeness. It is concluded, first, that electroceuticals comprise a broad range of biomedical tools. Second, such electroceuticals present significant clinical potential for exploiting the neural component of the TME as a strategy against cancer. Finally, the inherent bioelectric characteristics of tumors themselves are also amenable to complementary approaches. Collectively, these represent an evolving, dynamic field and further progress and applications can be expected to follow both conceptually and technically.
Introduction
Cancer is a complex disease characterized by the deregulation of a range of genes and associated cellular activities, including proliferation, apoptosis, (de)differentiation, migration, and invasion. 1 In most cases, it is metastasis that is the main cause of death from cancer. Traditional treatment modalities, such as chemotherapy, radiotherapy, and biological therapies, and even emerging ones like immunotherapy, are of limited effectiveness and can have serious, undesirable side effects. Accordingly, cancer pharmaceuticals are constantly being refined so as to be better targeted and be more effective in patient-specific settings. A more novel area of increasing prominence is centered around cancer cells' bioelectrical characteristics.2–4 Such characteristics manifest themselves in a variety of ways, including as membrane potentials, field potentials, cell surface charge, body electrolytes, tissue bioimpedance, and associated mechanisms. 2
More recently, tumors have been shown to be physically innervated with nerves actively contributing to tumorigenesis, as explored extensively in our previous article. 5 Furthermore, chronic neural activity (blocked by a local anesthetic) could be recorded from breast tumors induced in mice. 6 The tumor microenvironment (TME), in which intrinsic and extrinsic nerve connections occur, is heterogenous, also containing innate immune cells (e.g., macrophages, natural killer cells, and myeloid-derived suppressor cells), adaptive immune cells (e.g., T and B lymphocytes), endothelial cells, and fibroblasts, in addition to cancer cells and cancer stem cells themselves. 7 Nerve fibers derived from the sympathetic and parasympathetic nervous system (SNS and PNS) provide active inputs to tumors and can exert significant impact upon tumorigenesis through the release of their chemical messengers. 5 SNS fibers release norepinephrine/epinephrine, which act through adrenergic receptors (ARs), while acetylcholine is the primary neurotransmitter of the PNS and activates nicotinic and muscarinic acetylcholine receptors (nAChRs and mAChRs). The consequences of the neural inputs to tumors have been investigated (1) in vitro using the corresponding neurochemicals (catecholamines and acetylcholine) and/or receptor agonists and antagonists, as well as (2) in vivo animal models through denervation studies (both surgical and chemical). Thus, both SNS and PNS fibers have been shown to be involved in tumorigenesis, the exact contributions of the inputs varying from cancer to cancer. 5 Such variations are likely to reflect the differences in basal SNS and PNS connections to given organs. In particular, PNS input from the vagus nerve (VN), the most extensive of the cranial nerves, appears to play an important role in regulation of tumor progression.5,7 Importantly, the impact of nerve inputs can also vary temporally as the cancer progresses, with different effects being observed at the initiation, early tumorigenesis (proliferation), and late tumorigenesis (invasion and metastasis) stages. 5 Of note, classic studies of denervation in insects and rabbits showed that the absence of normal nerve input can promote the initiation of tumor formation.8,9 Whether these studies represent an anti-cancer effect of nerves or simply a pathological phenomenon remains unclear. Nevertheless, the role of tumor innervation is undoubtably complex. In a previous article, we reviewed, in detail, the pathophysiology of the nerve input to tumors, both generally and as regard several specific carcinomas. 5 In addition, a number of other recently published reviews explore the role of nerves in cancer.10,11 Therefore, this perspective will not consider the mechanism(s) of the nerve-cancer interaction in any further depth.
Overall, the available evidence from both animal models and human patients suggests that nerve input to tumors can, in some cases, promote the cancer process. The most direct clinical evidence is for prostate cancer, the incidence of which was found to be significantly reduced in men with spinal cord injuries. 12 Such evidence raises the possibility of controlling cancer by manipulating its nerve input. While directly denervating tumors surgically could achieve anticancer effects, as shown in animal models, such surgical procedures would not (yet) be readily viable in humans and could result in unpredicted and irreversible side effects. Instead, nonsurgical approaches could enable novel and convenient means of manipulating tumor innervation in cancer therapy.
In this perspective, we discuss possible ways in which the ‘bioelectricity’ of cancer may be exploited clinically. Our initial aim was to uncover potential approaches to induce change in the activity of tumor-impinging nerves. Technically, this can be achieved by physical contact with bioelectronic effectors (e.g., implantable bioelectronic devices, nanoeffectors, or electroactive polymers) or remotely (e.g., using optogenetics or chemogenetics). Interestingly, such techniques could also allow the direct manipulation of cancer cells, an approach that could have therapeutic effects, given that cancer cells themselves show altered bioelectrical properties. 13 Indeed, applying an electric field to tumors to manipulate their bioelectricity has already been approved as a clinical treatment. Therefore, we include tumor-treating fields (TTFs) as a special case for completeness. Broadly, these approaches together encompass “electroceuticals”. This term was coined originally to represent therapy by means of electrical stimulation of a nerve driving the physiological system/organ in question, that is, achieving therapy using electricity as a core treatment modality.14–16 The definition of electroceuticals continues to evolve and has already been expanded beyond the traditional use of stimulating electrodes to include approaches such as optogenetics and chemogenetics.17,18 In this perspective, we have broadened the initial definition further by including all bioelectric phenomena and means of achieving therapy. A complementary review reporting progress was published earlier. 19
Bioelectronic Effectors
Static implantable devices
Implantable bioelectronic devices have been used since the development of the first cardiac pacemaker in 1958. 20 Over the past 60 years, such “static” devices have been developed further and approved for treatment of various medical conditions. For example, stimulation of the VN is used in the treatment of depression, epilepsy, inflammatory syndromes, and multiple heart conditions.21–23 In the case of treatment-resistant depression, stimulation of the afferent cervical VN by an implanted electrode has been approved for clinical use by the US Food and Drug Administration. 24 Similar methods could be used to stimulate other branches of the VN known to contribute to particular cancers.
Overall, stimulating electrodes can act through two reaction mechanisms, depending on the conductive material employed. One mechanism involves a “faradaic current”, whereby electrons are transferred across the electrode-electrolyte interface resulting in reduction or oxidation of a chemical substance at the electrode surface. By contrast, “capacitive” (or “non-faradaic” or “double layer”) current simply relies on the accumulation or removal of electrical charge at the electrode, rather than any charge transfer. This makes the latter more desirable because no chemical reaction takes place and no chemical species are generated or removed. 25 Unfortunately, many existing devices can only be used to deliver electrical current for a short duration because they have the potential to cause tissue damage due to (1) accumulation of toxic electrochemical products generated by faradaic redox reactions and/or (2) harmful changes in the local microenvironment (e.g., oxygen depletion and disruption to ionic gradients) as a result of prolonged neuronal activation. 26 Thus, such implantable devices would have undesirable side effects, especially where large, extensively branched nerves (e.g., the vagus) with pleiotropic roles are involved. 27 Furthermore, when the therapeutic goal is to reduce neuronal activity, the technique typically must be used indirectly by activating a pathway that is inhibitory to the intended neurons. 28 Such limitations are being tackled in several respects, as follows:
Ionic direct current
Here, electronic pulses delivered to the metal electrode are converted to an ionic current at the output of the device. This prevents the occurrence of unwanted electrochemical reactions and the production of toxic by-products. 29 Unlike early implantable devices, ionic direct current (iDC) electrodes (e.g., in the form of microcatheters) can directly modulate the membrane potential to either excite or inhibit the neuron(s). Anodic iDCs inhibit neuronal activity by promoting membrane hyperpolarization, while cathodic iDCs are excitatory. 30 Such iDCs can manipulate neuronal activity and have successfully been used to modulate the vestibular system.30,31 In principle, this method could also be applied to the control of nerve input to tumors. However, it should be noted that the ionic current experienced at the output of such a device would not only influence neurons but also other cells in close proximity, including cancer cells, immune cells, and stromal cells within the TME.
Miniaturization
If cancer is to be controlled electrically using implantable devices, it is essential that surgery can place the given device precisely at the desired location, close to the associated neuron(s) or the tumor itself, without causing damage. In the former case, this would not be easy with complex nerves like VN and its many branches. Miniaturization of implantable devices can also improve targeting, that is, spatial specificity. One way in which miniaturization has taken place is through the replacement of rigid metal electrodes with new soft bioelectronic materials, such as a conductive hydrogel. 32 In addition, wireless inductive power transfer has been incorporated into several devices instead of bulky batteries. 33 More recently, further miniaturization has been facilitated using wide dipole antennas. 34 The latter use capacitive coupling to improve power transfer efficiency in miniaturized devices. Finally, some of the difficulties associated with static implantable devices, particularly targeting hard-to-reach areas and specific cells, can be overcome using “nanotechnology,” as discussed in the next section.
Motile effectors: nanoparticles and nanorobots
Nanotechnology can take a variety of formats and cover wide-ranging applications in cancer.35,36 Essentially, nanoparticles (NPs) are “motile effectors” measuring some 1–100 nm in size, tiny enough to enter human tissues and cells. NPs can enable tumor-specific targeting and localization for both improved imaging and therapeutics, while reducing side effects associated with off-target toxicity. 37 Targeting can be specific to different components of the TME, including vasculature, extracellular matrix, and stroma, as well as the nerves, immune cells, and cancer cells themselves. Nano/microrobots (NRs) are more elaborate synthetic “machines” measuring some 0.1–10 μm (with nm components) and could also target individual cells.38,39 Both NPs and NRs can move through the body in an autonomous manner guided by (1) external dynamics such as magnetic fields, electrical fields, or light or, in some cases, by (2) internal dynamics based on biological or chemical reactions, commonly the decomposition of hydrogen peroxide. 40 Hybrid devices have also been produced by combining synthetic components with biological ones, namely chemotactic cells such as sperm or neutrophils, to generate the desired movement. 40
Target specificity can be achieved by coupling NPs or NRs with monoclonal antibodies (mAbs) or aptamers. Several ion channel and receptor mAbs exist, which, in principle, could be used to direct NRs to neurons (or immune cells) associated with cancer and/or the cancer cells themselves to manipulate their electrical activity. The latter could exploit the oncofetal nature of ion channel expression in cancer.41–43 Aptamers are produced from a “DNA origami”, whereby a large single-stranded DNA molecule is forced to fold into a unique three-dimensional structure of a desired shape through interaction with hundreds of computer-designed oligonucleotides (“staples”).44,45 Thus, aptamers can bind to a specific target, which can be a cell-surface protein. 46 Accordingly, an aptamer is essentially a “nucleic acid antibody.” This approach has been used to target NRs to tumors using an aptamer which binds to nucleolin on tumor-associated endothelial cells. 44 Such technology can also be used alongside other treatment modalities such as immunotherapy. 47
In the context of tumor innervation, it has been shown for several cancers that the density of the nerve input to tumor tissue is correlated with disease progression and, hence, can give prognostic and/or therapeutic insights. 5 Nanotechnology is already being explored in peripheral nerve repair and regeneration.48,49 Hence, it is conceivable that NPs and/or NRs could also be used to target tumor-associated neurons for cancer management. Recently, suparamagnetic iron oxide NPs have been applied in vivo for both imaging and therapeutic targeting of nerves in prostate cancer PC-3 orthotopic xenografts in BALb/c mice. 50 Using magnetic resonance imaging of such NPs, density of tumor innervation could be measured quantitatively with low background noise and high sensitivity. 50 Using phage display, a peptide (“NP41”) was generated as a specific binder of neural laminins, which are expressed at high levels in the prostate. This peptide enabled accumulation of NPs in the tumor tissue after intravenous administration. Such NPs can be used to directly target the tumor-nerve interaction therapeutically by enabling targeted delivery of nerve blocking agents (e.g., β-blockers) to the TME. In the same study, propranolol was conjugated to NPs to selectively block sympathetic innervation within the TME. 50 This led to increased survival rates in the cohort receiving propranolol-conjugated NPs compared to control (83% vs. 11%) after 45 days in PC-3luc xenograft mice model of prostate cancer. Translation of these methods to the clinic could facilitate treatment of cancer, especially where nerve density is a key prognostic factor. NPs could also be used to achieve therapeutic effects by changing the membrane potential of target cells, including cancer cells. 51
Several cancer therapies that use NPs as drug delivery systems have already been approved and many more are currently in clinical trials. 52 Most recently, VYXEOS, a liposomal NP carrying a combination of cytarabine and daunorubicin, has been approved for treatment of acute myeloid leukemia. 52 While previous NPs have targeted the tumor to enhance chemotherapy, the novel approach of using NPs to target cancer-associated neurons will require higher levels of specificity, to avoid off-target effects. This will be particularly important when the target is a sub-branch of a large, pleiotropic nerve such as the VN.
Conductive polymer-based systems
Another route of bioelectrical control being investigated is the use of polymer-based systems, such as organic electronic ion pumps (OEIPs) and self-assembling conductive polymers.
Organic electronic ion pumps
To avoid the challenges associated with implant-to-tissue interface devices (i.e., implantable electrodes), the conductivity of conjugated polymers has been exploited to produce OEIPs. 53 Thus, the conducting polymer poly(3,4-ethylenedioxythiophene) was doped with the anionic polyelectrolyte poly(styrenesulfonate) to produce PEDOT:PSS with the two polymers providing electronic and ionic conductivity, respectively. 54 Such a material could be arranged into electrode-like structures (ELSs) joined by an overoxidized region, which acts as a connecting “ion channel”. Following the application of a voltage between the two ELSs, cations are transported from the anode to the cathode. 53 This allows for precise spatiotemporal delivery to cells of positively charged ions or biomolecules, including certain neurotransmitters.55–57 For example, a PEDOT:PSS-based OEIP system has been used to deliver the inhibitory neurotransmitter gamma-aminobutyric acid (GABA) to hippocampal neurons in a mouse brain slice model, thereby leading to reduced epileptic activity. 57 OEIPs could be applied to tumors in two ways. First, a source electrolyte containing K+ could be used to depolarize (activate) the nerve input. Second, using an electrolyte source of a positively charged neurotransmitter (e.g., acetylcholine), the nerve input can be mimicked. This technology, acting at an intersection between synthetic biology and bioelectronic devices, continues to be improved.58,59 For example, machine learning approaches are now being used to generate closed-loop systems in which bioelectronic devices, such as OEIPs, are able to sense and respond to real-time changes in biological systems.60,61 When considering the use of OEIPs to control the nerve input to cancer, closed-loop technologies could allow restoration of normal neuronal activity once a tumor has been eliminated. Encouragingly, in 2016, the US FDA approved the first clinical use of a conductive polymer material, a PEDOT-based device coating called “Amplicoat”. 62
Self-assembling electroactive polymers
More recently, the potential to stimulate cells to produce an autonomous bioelectrical material as an effector has become conceivable. Thus, a bioelectronic device could be generated by in vivo synthesis of electronically and ionically conductive polymers to modulate the membrane potential and activity of cancer-associated neurons. Such a polymer was used to address glial scarring in brain machine interfaces, which prevents interaction between a probe and target neurons, an issue associated with long-term use. Synthesis of poly(3,4-ethylenedioxythiophene) was achieved in vivo in rat hippocampal neurons and this reduced the impedance of the implantable electrodes by enabling bridging of the scar tissue. 63 The monomer was attached directly to the dorsal hippocampus through a surgically implanted microcannula/electrode system and the electrode itself was used as a source of oxidative current to promote electrochemical polymerization. 63
Alternatively, it is possible to genetically target an anabolic enzyme (e.g., ascorbate peroxidase Apex2) to be expressed in desired cell types, including neurones, to influence their membrane potential directly. 64 These cells can subsequently be directed with specific reactant monomers (e.g., aniline), which, through activity of the enzyme therein, undergo cationic polymerization. The polymers are then deposited onto the target cell surface and are electroactive, allowing the passage of ions and electrons. Such a ‘device’ has been developed in rats and could promote or inhibit the activity of target neurons, depending on the applied monomer (Fig. 1). 64 Ultimately, such progress in the field of biomaterials could expand the scope of bioelectronics into self-propagating devices. Such devices could be used to manipulate neuronal activity controlling tumorigenesis.

Using genetically targeted assembly of conductive and insulating polymers to control action potential firing in neurons. Rat hippocampal neurons were transduced with an adeno-associated virus carrying a humanized Apex2 gene. Following the provision of appropriate monomers, the Apex2 enzyme catalyzed the production of
Optogenetics
Optogenetics is a technique that uses opsins (light-activated transmembrane proteins) to spatiotemporally control cellular signaling. 65 As regard the membrane potential, depending on the type of opsin employed, the protein modulates a light-evoked change in ion flux to either depolarize (“excite”) or hyperpolarize (“inhibit”) the neuronal networks in which it is expressed. 66 Use of optogenetics has three essential features: (1) the opsin itself, either an excitatory channel rhodopsin or an inhibitory archaerhodopsin or halorhodopsin; (2) a method for specific targeting of the opsin gene into a desired cellular population; and (3) a method for precisely timed delivery of light to specific regions to activate the opsin. 67
Optogenetics has proved to be a successful technique in animal models, particularly in the dissection of neuronal circuitry underlying various diseases and behaviors.68–70 For example, in murine models of Alzheimer's disease, selective stimulation of cortical projection neurons in the lateral entorhinal cortex was achieved using stabilized step-function opsin, a long-lasting channel rhodopsin. 70 Such optogenetic manipulation led to the finding that chronic hyperexcitation of the targeted neurons could augment deposition of amyloid-β, a peptide associated with disease onset. 70
Early technologies relied on the provision of visible light through a fiber optic cable, which needed some surgery to be installed.71,72 More recently, internalized wireless devices have been developed for peripheral neuromodulation in rodents. For example, microscale diodes that emit 540 nm light were used to control sensory afferents of the bladder. 73 Another approach involves using “upconversion nanoparticles” capable of converting highly penetrable near-infrared light (provided by a laser) into localized visible light of the desired wavelength. This method has been applied successfully to human cell cultures, as well as in vivo models of mice and zebrafish.74–76
With the ongoing technical improvements and expanding applications (mainly in the neuroscience area), optogenetics could readily be expanded to management of human cancers. In a promising study on a Xenopus model, activation of (1) ChR2D156A, a cation channel opened by blue light, or (2) Arch, a green light-activated proton pump, significantly reduced the formation of KRAS-induced tumor-like structures. 77 Importantly, the same study showed that activation of ChR2D156A after tumor formation could increase the frequency of tumor regression (tissue normalization). 77 Both opsins promote the hyperpolarization of cells, which, given that cancer cells are generally depolarized relative to normal cells, provides a potential therapeutic mechanism to override cancer-causing mutations. We should note, however, that optogenetically induced polarizations could be reduced by repetitive stimulation, limiting the long-term applications of this technique. 78
Optogenetic therapy has also been considered for the direct killing of cancer cells. An optogenetic system driven by blue light has successfully been used to activate an apoptosis pathway in mouse B16 melanoma cells, both in vivo and in vitro, leading to significantly reduced (by up to 80%) tumor volume (Fig. 2A). 79 This optogenetic pathway does not simply activate a protein, but rather promotes a protein-protein interaction between the transmembrane receptor Fas and the “Fas-associated protein with death domain” (FADD), consequently initiating an apoptotic caspase cascade. 79 Another optogenetic approach has been used to enhance antitumor immunotherapy. 80 Thus, a light-activated chemokine receptor (CXCR4) has been engineered into T cells. CXCR4 is a rhodopsin-chemokine hybrid and, upon illumination with 505 nm green light, the induced downstream Ca2+ and cAMP signaling resulted in increased T cell migration in vitro. When these in vitro activated T cells were injected into a mouse carrying a heterotopic xenograft of B16 melanoma, there was a significant decrease (>80%) in tumor volume compared to controls (Fig. 2B). 80

Direct and indirect optogenetics in anticancer therapeutics.
Attempts to apply optogenetics to human therapeutics clinically are ongoing. One application, which has so far shown promise and is currently being tested in a phase I/II clinical trial, is restoration of vision in advanced retinitis pigmentosa (ClinicalTrials.gov NCT02556736). Importantly, since the eye is responsive to visible light, the natural stimulus is sufficient for opsin activation without the need for an extra light delivery device. The two main challenges in optogenetic therapy are finding a suitable vector for targeting of opsins to desired cells and delivering appropriate light noninvasively. 71
The emerging roles of innervation and inherent bioelectricity of tumors would make these highly promising targets for optogenetic control of cancer. Encouragingly, selective optogenetic stimulation of vagal sensory afferent subtypes has already been successful in mice using Cre-expressing strains. 81 P2ry1 and Npy2r are cell surface biomarkers, which define subpopulations of vagal sensory afferents innervating the lung. Channelrhodopsin2 was engineered into P2ry1-ires-Cre and Npy2r-ires-Cre mice and subsequent light exposure activated the desired subpopulations, resulting in differential effects on respiration. 81
Optogenetics is proving particularly applicable to controlling cellular processes dependent on Ca2+. 82 The latter is pivotal to the cancer process. 83 In a recent application, use of light-activatable complexes of calcium release-activated channels (CRACs) enabled “remote” photic stimulation of the cells of the immune system to elicit spatially and temporally distinct signaling and immune responses, including transcriptional reprogramming, in a zebrafish model of Stormorken syndrome. 84 Such approaches could also be adapted to be used against cancer and its innervation. Finally, a further promising application of optogenetics to cancer biology is in relationship to development of light-activatable complexes of receptor tyrosine kinases (e.g., neurotrophin receptors), which play a significant role in cancer.85,86
Pharmacology and Chemogenetics
Modulators of neurotransmitter receptors and ion channels can be considered possible “liquid” electroceuticals and there are already several examples of these.17,87 For example, voltage-gated sodium channel blockers have been proposed as antimetastatic drugs.43,88,89 Pharmacological approaches for targeting the SNS and PNS specifically involve adrenergic and cholinergic agents, respectively, such as the use of β-AR antagonists or clinical “beta blockers”. 90 Long-term use of the beta-blocker atenolol, for example, was associated with lower incidence of prostate cancer and improved prognosis. 91 Importantly, however, the effect of such drugs may depend on the type and stage of cancer as well as the beta-blocker used. Indeed, a meta-analysis of non-small cell lung cancer (NSCLC) patients failed to find any significant difference in overall survival between users of beta-blockers and nonusers. 92 Nonetheless, the possibility of repurposing drugs that are already approved for clinical use remains a desirable and promising approach for targeting cancer-associated neuronal activity.
Alternatively, chemogenetics provides the potential to combine genetic and pharmacological approaches to manipulate neuronal activity. In chemogenetics, neurons are genetically engineered to express “Designer Receptors Exclusively Activated by Designer Drugs” (DREADDs). These are mutant mAChRs (G protein-coupled receptors), which no longer respond to acetylcholine, but instead respond to the synthetic drug clozapine-N-oxide (CNO). 93 Neuronal excitation can be achieved using hM3Dq, a mutant form of the human heart muscarinic M3-AChR, which is coupled to a Gq protein. Upon administration of CNO, activation of hM3Dq leads to Ca2+ influx and depolarization. Alternatively, membrane hyperpolarization leading to neuronal inhibition can be achieved using hM4Di, a mutant form of the M4-AChR, which is coupled to Gi protein and induces hyperpolarization through the opening of inwardly rectifying K+ channels. 94 Chemogenetic activation of dopaminergic neurons in the ventral tegmental area has been shown to significantly reduce tumor growth in C57BL mouse models of Lewis lung carcinoma and B16 melanoma with up to 50% reduction in tumor weight (Fig. 3).95,96 Further investigation found that this antitumor effect was mediated by the SNS with a decrease in norepinephrine levels in the bone marrow, which would subsequently decrease the immunosuppressive function of myeloid-derived suppressor cells.95,96 Chemogenetic control of cancer could readily be applied to patients since CNO is relatively inert and has already been administered to humans with no apparent side effect. 97 As with optogenetics, the main challenge in applying this technique to patients in the clinic will be finding a method for genetic engineering of the desired neurons as well as determining appropriate combinations of receptor and ligand.94,98
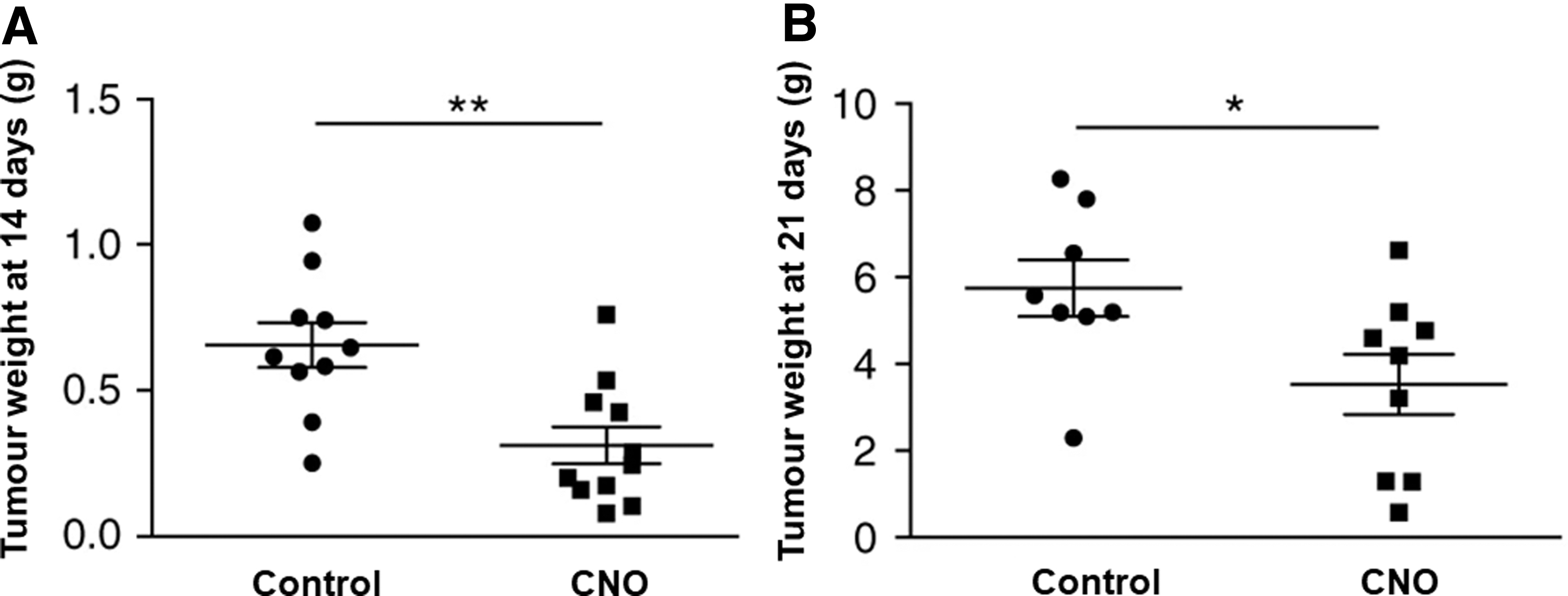
Chemogenetic activation of the VTA reduces tumor growth. Adeno-associated viruses were used to transduce dopaminergic neurons of the VTA with the stimulatory designer receptor exclusively activated by designer drugs, hM3Dq, in mice with
Tumor-Treating Fields
TTFs are a special case of electroceuticals, whereby an electric field is applied direct to the tumor or tumor bed. TTFs comprise low-intensity alternating electric currents, which can induce apoptosis and suppress cellular proliferation, migration, and invasion.99,100 Unlike chemotherapy and radiotherapy, which aim to inhibit the cell cycle in interphase, TTFs target mitosis and cytokinesis directly. 101
The alternating electric field is applied optimally (low intensity, 1–2 V/cm, and 100–300 kHz) so as not to affect nondividing, healthy cells and minimize off-target toxicity without stimulating the surrounding nerves.102,103 Several insulated metal electrodes can be used to apply the TTF from a personalized wearable transducer array attached to a portable battery pack, allowing patients to receive treatment for up to 18 h a day.104,105 According to electromagnetic theory, dipolar molecules inside cells (e.g., tubulin and septin) will rotate continually according to the alternating charge of TTFs, a process known as “dipole alignment.” 106 This disrupts the cytoskeleton, preventing polymerization of mitotic spindles and microtubule stabilization, thereby impeding progression of dividing cells into anaphase and impairing chromosome separation (Fig. 4).107,108 Another phenomenon, known as “dielectrophoresis”, follows formation of the cleavage furrow during telophase resulting in the field becoming nonuniform. Consequently, organelles and polar macromolecules accumulate at the mitotic furrow, thus also impeding cell division. In addition to antiproliferative effects, TTFs can also induce cytotoxicity by increasing cytosolic Ca2+, mainly through Cav1.2 channel activity.99,100,109 More recently, mathematical modeling has suggested that TTFs could also impact the cell membrane potential. 110 This model suggests that due to the higher membrane conductivity of tumor cells, TTFs will induce a greater depolarization in cancer cells compared to healthy cells (∼17% vs. 3%). Cancer cells are already known to have a relatively depolarized membrane potential (ca. −25 mV). While such a compounded depolarization could be a factor in inducing selective death of cancer cells by TTFs, this model has yet to be tested.
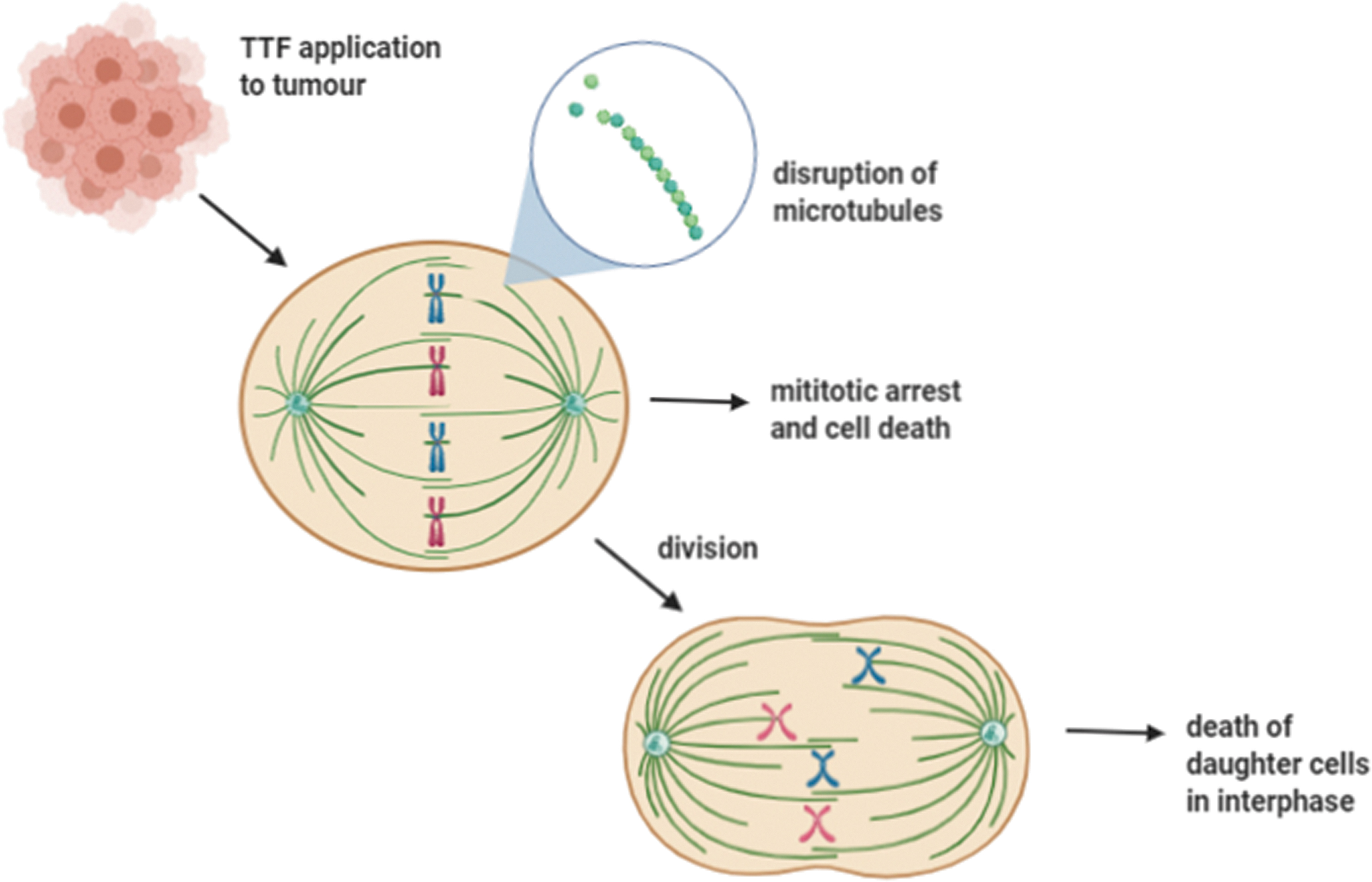
Mechanism of TTFs. Schematic representation of the effect of TTFs on the cell cycle of cancer cells. Alternating electric fields cause dipole misalignment of dipolar particles causing disruption of tubulin microtubules required for spindle formation during mitosis. This leads to improper chromosome separation, which can result in mitotic exit and cell death. If the cell successfully divides after such aberrant chromosome separation, the daughter cells will die in anaphase. TTFs, tumor-treating fields.
Currently, TTFs are used most commonly to treat glioblastoma, often in combination with chemotherapy.106,111 Clinical trials on newly diagnosed glioblastoma patients showed an increase in progression-free survival by 3.1 months (ca. 30%), as well as an increase in overall survival when treated with TTFs and temozolomide (TMZ) in comparison to the control group treated with conventional chemotherapy alone (Fig. 5A, B). 112 Another study on patients with recurrent glioblastoma similarly showed that TTF and TMZ co-treatment led to some 2.7-month (ca. 68%) longer progression-free survival and increased overall survival compared to TMZ treatment alone. 113 More recently, application of TTFs in combination with lomustine (an alkylating chemotherapy drug) and TMZ treatment proved safe and the observed survival outcomes suggested potential beneficial effects. 114
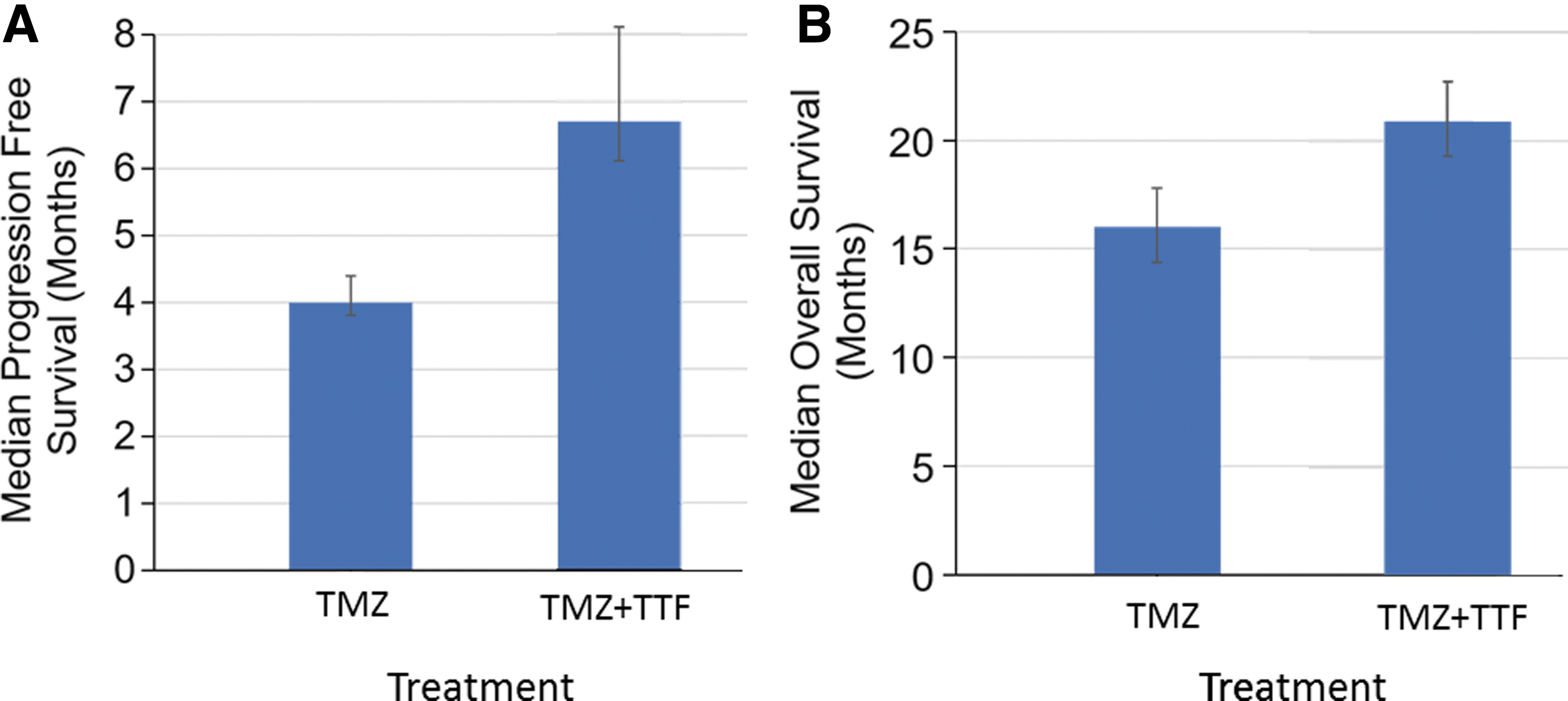
Use of TTFs alongside chemotherapy improves glioblastoma survival. Kaplan-Meier curves showing median progression-free survival
The therapeutic potential of TTFs has also been investigated in several other solid malignancies: in vivo studies of the effects of TTFs on mouse models of malignant melanoma, NSCLC, and pancreatic cancer.115–117 Application of TTFs resulted in decreased proliferative activity and tumor growth, resulting in significantly longer survival times. Phase II clinical trials combining TTFs with chemotherapy in NSCLC, ovarian, and pancreatic cancer patients showed increased overall survival and slower tumor progression, compared with treatment with chemotherapy alone.118–120 In an extended approach, phase III trials have adopted TTFs in combination with chemotherapy or immunotherapy against solid malignancies, including breast, colorectal, cervical, lung, and ovarian cancers.106,121
More recently, NPs have been investigated as a potential co-therapy with TTFs. In vitro studies on multidrug-resistant breast cancer cell lines suggested that administration of barium titanate NPs (BTNPs) sensitized the cells to TTF treatment. 122 BTNPs were not cytotoxic alone, but, coupled with TTF application, accumulated in the cytosol leading to modulation of signaling pathways, including cell cycle apoptosis, thus promoting cell death. BTNPs have a high dielectric constant allowing them to be manipulated by TTFs. In addition, TTFs have been shown to increase cell membrane permeability in glioblastoma cell lines by pore formation, which could also be a factor in driving cytoplasmic accumulation of BTNPs. 123 If successfully translated in vivo, such a combined treatment could significantly enhance the therapeutic potential of TTFs.
In conclusion, TTFs are an effective “electroceutical” modality, especially when applied in combination with conventional cancer therapies or other synergistic agents. This has significant potential in targeting solid malignancies, in addition to its current application to glioblastoma. In particular, TTFs have promise in targeting chemoresistant or difficult-to-treat cancers, such as pancreatic cancer. 120
Ultrasound
Focused ultrasound (FUS), which can penetrate deep tissues, has been shown to be an effective way of blocking action potentials in nerves. 124 More recently, high-frequency ultrasound was found to inhibit or excite neural activity depending on frequency. 125 Based on such effects, the “Surround System” utilizing externally delivered ultrasound has been used to achieve effective renal denervation as a means of treating hypertension in humans. 126 It would seem conceivable, therefore, that FUS could be used to manipulate the activity of the nerve input to tumors. Interestingly, somewhat analogous to TTFs, direct sonodynamic therapy can be used in cancer treatment where ultrasound is combined with a sonosensitizer to synergistically kill cancer cells. 127 More recently, an ultrasound-powered neural stimulating implantable device has been designed based on “neural dust” technology. 128 “Neural dust” is a wireless, submillimeter brain-machine interface, which can be implanted noninvasively in patients and enables long-term, high-fidelity neural recordings. 128 Upon receiving ultrasound waves, an integral piezoelectric crystal reflects and modulates the wave properties according to the neural activity, which is then recorded as an output through a receiver outside of the body. Ultrasound has a shorter wavelength than generic electromagnetic waves normally used in this technology, thus enabling miniaturization of the device and giving it greater bandwidth and resolution, as well as deeper penetration and lower power requirement, thereby improving safety. Based on the same principle, a submillimeter wireless neural stimulation device has been developed and used successfully in vivo to stimulate the sciatic nerve in murine models. 128 With further development, this technology could be used to target the peripheral nerves innervating tumors in humans without the need for any invasive procedure or genetic engineering.
Conclusion and Future Perspective
In overall conclusion, the nerve inputs to tumors play a significant role in the pathophysiology of cancer and a range of electroceutical techniques offer much potential in controlling the cancer process (Fig. 6). Such devices are mostly ‘solid state’, but can also be ‘liquid’, with respective advantages and disadvantages. Some of these techniques can be operated even remotely and in combination with conventional treatments. The approaches discussed vary in their stages of development and feasibility for use in the clinic. For example, TTFs have already been approved for therapeutic use in the treatment of glioblastoma, whereas chemogenetics and optogenetics require additional refinements. In particular, finding feasible and ethical methods of genetically engineering cancer-associated neurons and/or cancer cells remains a major hurdle in these approaches. In addition, while these techniques could allow the manipulation of cancer-associated nerves, it should be noted that prolonged stimulation or inhibition or neurons could also cause unwanted secondary effects, a possibility yet to be widely explored or quantified. Importantly, however, many of the approaches covered in this perspective would aim to inhibit the growth or progression of tumors, rather than kill cancer cells. Indeed, this is an ideal strategy since increasing evidence suggests that indiscriminate killing of cancer cells (e.g., by chemotherapy) could, in the long run, make cancer worse.129,130 In part, this is probably due to the inherent stemness of cancer. All the signs are that the field of “cancer electroceuticals” will progress through further applications of biophysics/electrophysiology, bioengineering, and molecular biology. It seems just a matter of time, therefore, that practical exploitation of the nerve inputs to tumors becomes a clinical reality.

Clinical exploitation of tumor bioelectricity. Schematic overview of electroceutical techniques with therapeutic potential in cancer treatment. Such devices can be used to exploit the nerve-cancer crosstalk by stimulating an impinging nerve or target the tumor directly by techniques such as TTFs. The latter use an alternating current to impede cancer cell division by directly interrupting mitosis and cytokinesis without impact on the surrounding nerves. Targeting of the impinging nerve can be achieved by nanotechnology, including nanoparticles, nanorobots, and “neural dust” technology. Implantable devices include conventional static electrodes, as well as more sophisticated ionic direct current devices. Alternatively, ion channel complexes, with appropriate pharmacology, can modulate the membrane potential of the nerves; such complexes can encompass chemogenetics and self-assembling electroactive polymers. Optogenetics are a special case of ion channel complex where a channel rhodopsin can be genetically engineered into a neuron to enable light-evoked ion flux. Finally, focused ultrasound is capable of both exciting or inhibiting neural activity depending on wave characteristics.
Footnotes
Acknowledgment
We thank Professor George Malliaras for his critical reading of the article.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
Our research—neuroscience solutions to cancer—is supported by the Pro Cancer Research Fund (PCRF).