
Abstract
Electrochemotherapy (ECT) has emerged as an effective local treatment for cancer in dogs and cats. This technique consists of the transient and reversible permeabilization of cell membranes through the application of an electric field. The transient permeabilization increases the uptake of hydrophilic chemotherapeutic agents (bleomycin, cisplatin) into tumor cells, thereby enhancing their cytotoxic effect. ECT is primarily indicated for cutaneous and subcutaneous tumors of various histological types, including squamous cell carcinomas, mast cell tumors, and soft tissue sarcomas. It is also applied to tumors located in the oral cavity, sinonasal region, urinary bladder, and perianal area. ECT may be used as monotherapy, in the surgical bed following tumor excision, or as an adjuvant therapy when complete surgical margins are not achievable. Additionally, it can be employed as a neoadjuvant treatment, followed by surgical resection. Adverse effects are predominantly local and transient, including erythema, edema, pain, and necrosis. Thus, toxicity is generally mild, with most patients exhibiting good tolerance. For optimal outcomes, individualized follow-up is essential to assess therapeutic response, monitor adverse effects, and detect potential tumor recurrence. The aim of this review is to present the principles for the use of the technique in small animal clinical practice, including its indications, clinical applications, contraindications, adverse effects, and follow-up.
Introduction
Veterinary medicine has seen continuous growth as pet owners increasingly seek safe and effective treatments for their animals. This rising demand for optimal care has driven the development of various specialties within the field, including oncology. 1 One of the main challenges in oncological therapy for small animals is the local control of solid tumors, which may exhibit rapid progression or recurrence following treatment. 2 Additionally, the size and location of tumors can limit the effectiveness of surgical approaches. 3 In this context, electrochemotherapy (ECT) has emerged as a valuable tool in clinical practice, enabling the destruction of neoplastic cells while preserving surrounding healthy tissues. ECT enhances the local effects of hydrophilic chemotherapy agents, bleomycin and cisplatin, through the application of high-intensity electric fields. 4 The increasing adoption of ECT in veterinary medicine can be attributed to its advantages, including efficacy, low morbidity, and cost-effectiveness. 5 The objective of this review is to present the principles of ECT in small animal oncology, including its indications, clinical applications, contraindications, adverse effects, and follow-up.
Theory of Electroporation
The model of the electroporation phenomenon is the most widely accepted to explain the increased permeability in membranes subjected to an electric field. Electroporation consists of the formation of aqueous pores in the cell membrane, which has been exposed to a specific electric field. 6 This electric field is generated through high-intensity electric field with pulse (μs) amplitude from the range 100–3000 V.6,7 The electric pulses are typically delivered via a high-power generator (electroporator), and the electrodes transfer energy to the biological tissue. The electrodes have negative and positive poles, generating an electric field between them. 8
The transmembrane potential (TMP) is the difference in electrical potential between the extracellular and intracellular spaces, resulting from the balance between ion fluxes from the extra- and intracellular environments, facilitated by pores, ion pumps, and channels located in the plasma membrane (e.g., Na+ and K+ pumps). The resting TMP of cells ranges from −70 to −40 mV. 9 When the cell is exposed to an electric field, a TMP is induced, and if it exceeds a critical threshold (∼200 mV), rearrangement of the lipid bilayer occurs, leading to the formation of aqueous pores in the plasma membrane. 10
Kotnik et al. 9 reviewed the five phases of electroporation: initiation, expansion, partial recovery, resealing, and memory. Initiation is characterized by an increase in conductivity and cellular permeability after the TMP exceeds a critical threshold due to the application of an electric field. Expansion occurs when the TMP remains above the critical threshold, resulting in persistent and/or intensified conductivity and permeability until the electric pulse is interrupted. During partial recovery, the TMP decreases below the critical threshold, leading to a rapid reduction in membrane conductivity and permeability; however, transmembrane diffusion of ions and molecules is still possible. Resealing is characterized by the gradual recovery of membrane impermeability. However, resealing does not occur after irreversible damage, resulting in loss of cellular viability. Memory involves changes in cellular physiological processes, even after complete membrane sealing, before the cell returns to its normal state.
Electroporation can occur in a reversible or irreversible form, depending on the intensity, duration, and number of electric pulses. Reversible electroporation (RE) is responsible for the transient increase in cell permeability, allowing the passage of water, ions, and water-soluble molecules (e.g., DNA, drugs) into the cytosol. 10 Electrical pulses usually include eight square wave pulses of 100 μs, with an amplitude of 100–1000 V. 7 In contrast, irreversible electroporation (IRE) causes permanent changes in the membrane, resulting in loss of homeostasis and cell death. 11 For IRE, more pulses (at least 80–100 pulses) and a higher amplitude (up to 3000 V) are required. 7
IRE was introduced into oncology by Davalos et al. 12 The technique is capable of causing a cytotoxic effect on tumor cells, without thermal injury, through the application of an intense electric field. 7 The mechanisms of cell death include a combination of apoptosis and necrosis. 13 The formation of permanent pores in the cell membrane results in chemical and osmotic stress due to the excessive transport of ions and molecules. Additionally, the critical expansion of the pores may lead to complete cell dissolution. 14
Electrochemotherapy
ECT is a local antineoplastic treatment that combines RE with chemotherapy. 15 The electric pulses for electroporation are generated by a device known as an electroporator and delivered to the cells through electrodes. Ideally, the device should measure the parameters of the pulses delivered and provide warnings in case of malfunction or incorrect operation. 16 The geometry of the electrodes determines the distribution of the electric field. The main electrodes used are needle electrodes (invasive) and plate electrodes (noninvasive). 17 Another type of electrode, in the form of a single needle, is available for treatment in bone cavities, particularly the nasal cavity. This tetrapolar single-needle electrode consists of four conductive strips of gold-plated copper arranged longitudinally within an insulating solid silicone tube. This configuration allows for the generation of electric fields between the conductive segments, producing a well-distributed and controlled electric field in confined anatomical sites such as bone cavities. The electrode was validated with an operating voltage range of up to 650 V. In a nasal cavity tumor model, the electrode was capable of generating a circular electric field with an approximate radius of 3 mm and an electric current of 14.1 A at 500 V. These parameters are compatible with established ECT standards and commercial equipment, ensuring effective field coverage while minimizing damage to surrounding tissues. 18
Needle electrodes can be arranged in two rows (parallel) or a circular (hexagonal) arrangement. They are suitable for treating most tumors and can penetrate tumor tissue, generally up to 3 cm. 19 Plate electrodes can be employed in the therapy of superficial or exophytic lesions. 20 However, they require the use of a conductive gel to increase the contact surface with the tumor, and the pulses must be delivered in two parallel planes to form a homogeneous electric field.21,22 ECT typically delivers a sequence of eight electric pulses with a duration of 100 μs and a pulse repetition rate of 1–5 kHz. The voltage-to-distance ratio is 1000 V/cm with needle electrodes or 1300 V/cm with plate electrodes.23,24 Treatment at a frequency of 5 kHz reduces the number of involuntary contractions triggered by the electric pulses to one, without altering the clinical outcome. 25
The intensity of the electric field is greatest between the electrodes and rapidly decreases with increasing distance between them. Thus, the tumor and its margins must be completely covered by the application of the electric pulses for the success of the therapy.8,26 The electrodes must remain parallel, as a deflection of the needles by ±2 mm can negatively affect the distribution of the electric field and consequently the clinical outcome. 27
Mechanisms of action
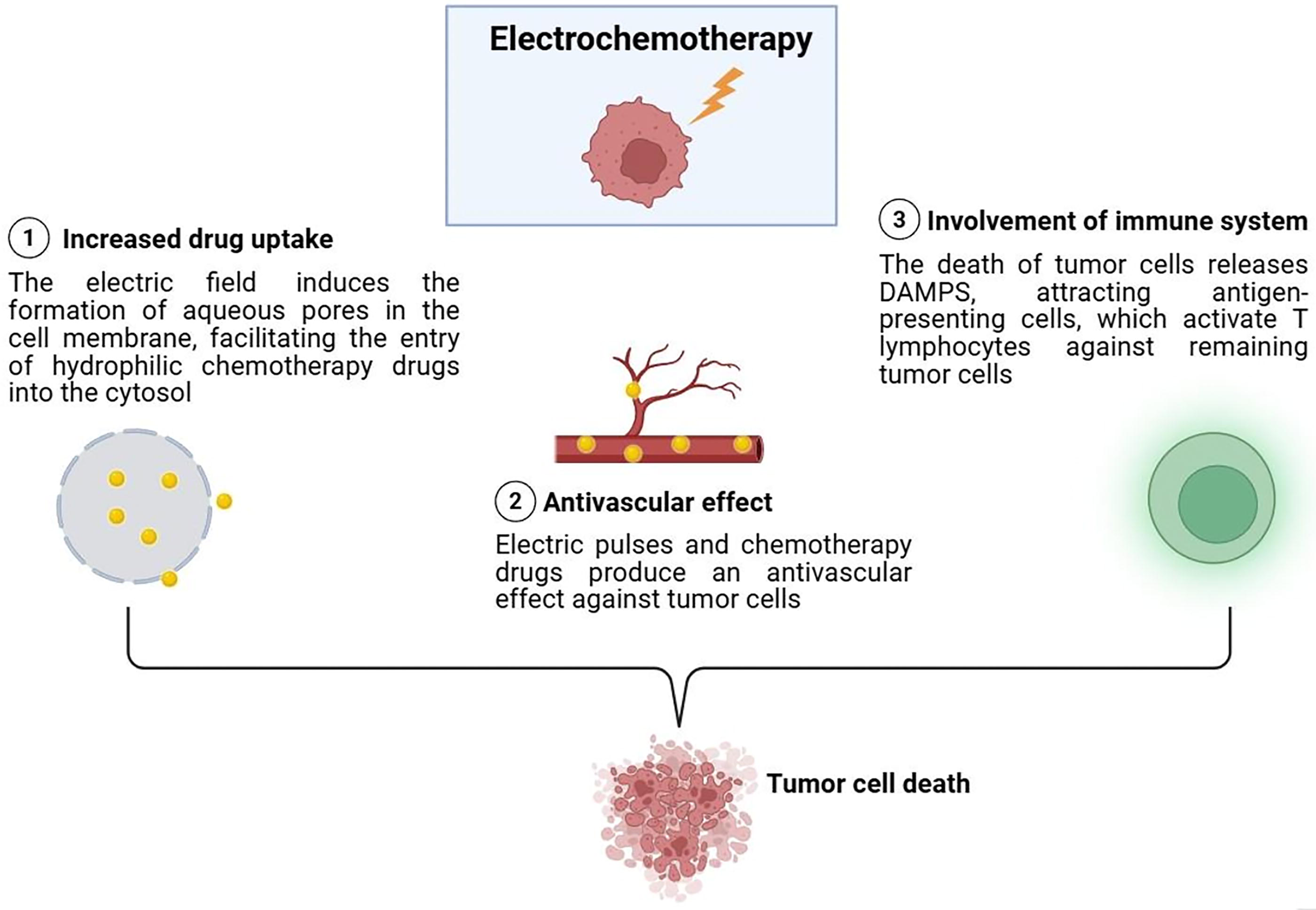
The main mechanism of action of ECT is the potentiation of the cytotoxic effects of drugs via electroporation, leading to tumor cell death through apoptosis and necrosis. 28 The treatment also involves a combination of antivascular effects and is capable of inducing immunogenic cell death. 29
The electric pulses result in rapid vasoconstriction (vascular blockade), followed by the disruption of cytoskeletal structures and impairment of the endothelial cell barrier function. Vascular blockade causes entrapment of the chemotherapy agent within tumor blood vessels, initiating direct damage to the tumor vasculature and a reduction in blood supply within hours of treatment. The tumor cells that survive are induced to undergo secondary death due to hypoxia within days.30–32 Electroporation also induces an increase in the permeability of bleomycin and cisplatin in endothelial cells, exerting a direct antivascular effect against tumor cells33,34 (Fig. 1).

Dog undergoing intraoperative electrochemotherapy for the treatment of a mast cell tumor. The circle indicates the occurrence of vascular stasis, resulting in reduced blood flow and a change in the color of the muscle tissue. Created by the authors.
ECT acts by eliminating residual tumor cells through a specific immune response. 29 This phenomenon is mediated by the release of damage-associated molecular patterns (DAMPs), which act as a danger signal to the immune system, activating various pattern recognition receptors, including Toll-like receptors and NOD-like receptors. The immune response triggered is typically linked to the formation of immunogenic memory. 35 DAMPs are normally present in the intracellular environment; however, when released from cells (e.g., trauma or other states of increased cellular permeability), they trigger enhanced innate and adaptive immune responses. 36 ECT induces the release of DAMPs such as adenosine triphosphate (ATP) and High-Mobility Group Box 1 (HMGB1), as well as the translocation of calreticulin to the cell surface. This is followed by the migration of antigen-presenting cells to the site, such as macrophages and dendritic cells, which present tumor antigens and activate T lymphocytes against remaining tumor cells.37,38 A systemic immune response is rarely observed; however, there are reports of an abscopal effect, which refers to the remission of metastatic disease following local treatment. 39 The exact mechanism of action remains unknown 35 (Fig. 2).
Mechanism of action of electrochemotherapy. DAMPS, damage-associated molecular patterns. Created with BioRender.com.
Cytotoxic drugs
The ECT requires the hydrophilic cytotoxic drug to reach a peak concentration in the tumor before the electric pulses are applied to the region. 19 The two most commonly used drugs are bleomycin and cisplatin, as they are potentiated by electroporation by 700 and 70 times, respectively.40,41 The routes of administration for chemotherapy in ECT are intravenous (bleomycin) and intratumoral (bleomycin and cisplatin). 10
Cisplatin
Cisplatin is a platinum-based anticancer drug. The molecules of this drug cross the plasma membrane 50% by passive diffusion and 50% by facilitated diffusion. 42 Its primary mechanism of action is the interaction with purine bases (cross-linking both inter- and intrastrand), inducing DNA damage and activation of various signaling pathways that result in apoptosis.43,44
Bleomycin
Bleomycin is a cytotoxic antibiotic. This drug does not cross the cell membrane by passive diffusion, requiring uptake via endocytosis. 45 Bleomycin has two mechanisms of action, depending on the number of molecules internalized. The internalization of only a few thousand drug molecules induces a G2-M phase cell cycle arrest, causing the cells to become enlarged and multinucleated before dying, a phenomenon known as “mitotic cell death.” On the other hand, when several million bleomycin molecules are internalized, morphological changes identical to those normally associated with apoptosis are observed, as well as rapid DNA fragmentation into oligonucleosomes. 46 The intravenous administration of bleomycin is sufficient to induce “mitotic cell death,” but it does not result in metabolic cell death. Thus, normal cells that are quiescent remain spared, and systemic side effects are typically not observed. 47
Routes of administration
Intravenous Route
The intravenous route is exclusively used with bleomycin, being the route of choice, particularly for large or multiple tumors. 48 Bleomycin is administered at a dose of 15,000 IU/m2, after dilution with saline solution, in a bolus over ∼30 s.22,49 The advantages of the intravenous route include homogeneous distribution of the drug, no areas with insufficient drug concentration due to incorrect intratumoral application, increased safety for the operator by avoiding extravasation and direct contact with the chemotherapy agents, and greater selectivity against neoplastic cells.47,50 The therapeutic window is between 8 and 40 min. 48 It is considered acceptable to continue administering pulses beyond the recommended window, as clinical efficacy may still persist even after 40 min, particularly in elderly patients or those with impaired renal function. Lesions treated outside this interval should be marked to enable appropriate follow-up.48,50
Intratumoral Route
The intratumoral route can be used with either bleomycin or cisplatin. It is an option when there are no more than seven tumors, with sizes smaller than 3 cm. 51 After the tumor is infiltrated with the drug, treatment should preferably be performed within 1–10 min. 48 A combination of the intravenous and intratumoral routes can be used for large tumors, which are predisposed to abnormal vascularization and, consequently, areas that are not reachable by systemic circulation. 52
The use of bleomycin via the intratumoral route requires dilution to a concentration of 1,000 IU/mL, and the dose depends on the tumor volume. For lesions <0.5 cm³, bleomycin is administered at a dose of 1 mL (1000 IU)/cm³; for lesions ≥0.5 cm³ and <1 cm³, the dose is 0.5 mL (500 IU)/cm³; and for tumors >1 cm³, the dose is 0.25 mL (250 IU)/cm³. 48 Cisplatin is infiltrated into the neoplasm at a concentration of 1 mg/mL. 53 The drug volume is determined as follows: tumors >1 cm³ are treated with a dose of 0.5 mL (0.5 mg)/cm³, while lesions ≥0.5 cm³ and ≤1 cm³ should be treated with a dose of 1 mL (1 mg)/cm³. Lesions smaller than 0.5 cm³ are treated with a dose of 2 mL (2 mg)/cm³. 19
Indications
ECT can be used for both curative and palliative purposes, aiming to improve the quality of life of patients. 19 The technique is primarily indicated in the treatment of primary and metastatic skin and subcutaneous tissue tumors of all histological origins. 54 ECT is also used for oral, 55 nasal, 56 and urinary bladder tumors. 49 It is considered an effective and safe alternative when standard treatment techniques are declined by the pet owner or are limited by patient comorbidities or tumor characteristics such as size, location, and multifocal involvement. 57 Treatment is carried out following a definitive tumor diagnosis, with the patient under general anesthesia. The animal is preevaluated through a complete blood count, renal profile, liver profile, and imaging tests, including chest radiography and abdominal ultrasound for disease staging and to rule out underlying conditions.22,50
In monotherapy, ECT achieves a complete response rate of 60–70% for tumors up to 3 cm in diameter after a single session. 48 Larger and/or infiltrative tumors should be treated in combination with surgical excision for local disease control. 50 ECT may therefore be applied to the surgical bed after tumor excision or in compromised postoperative scars, aiming at controlling microscopic disease and expanding surgical margins. 58 The use of ECT in a neoadjuvant setting is possible, but less frequent. 59 Table 1 summarizes clinical studies on the use of ECT in small animal oncology.
Summary of Clinical Studies on Electrochemotherapy in Dogs and Cats
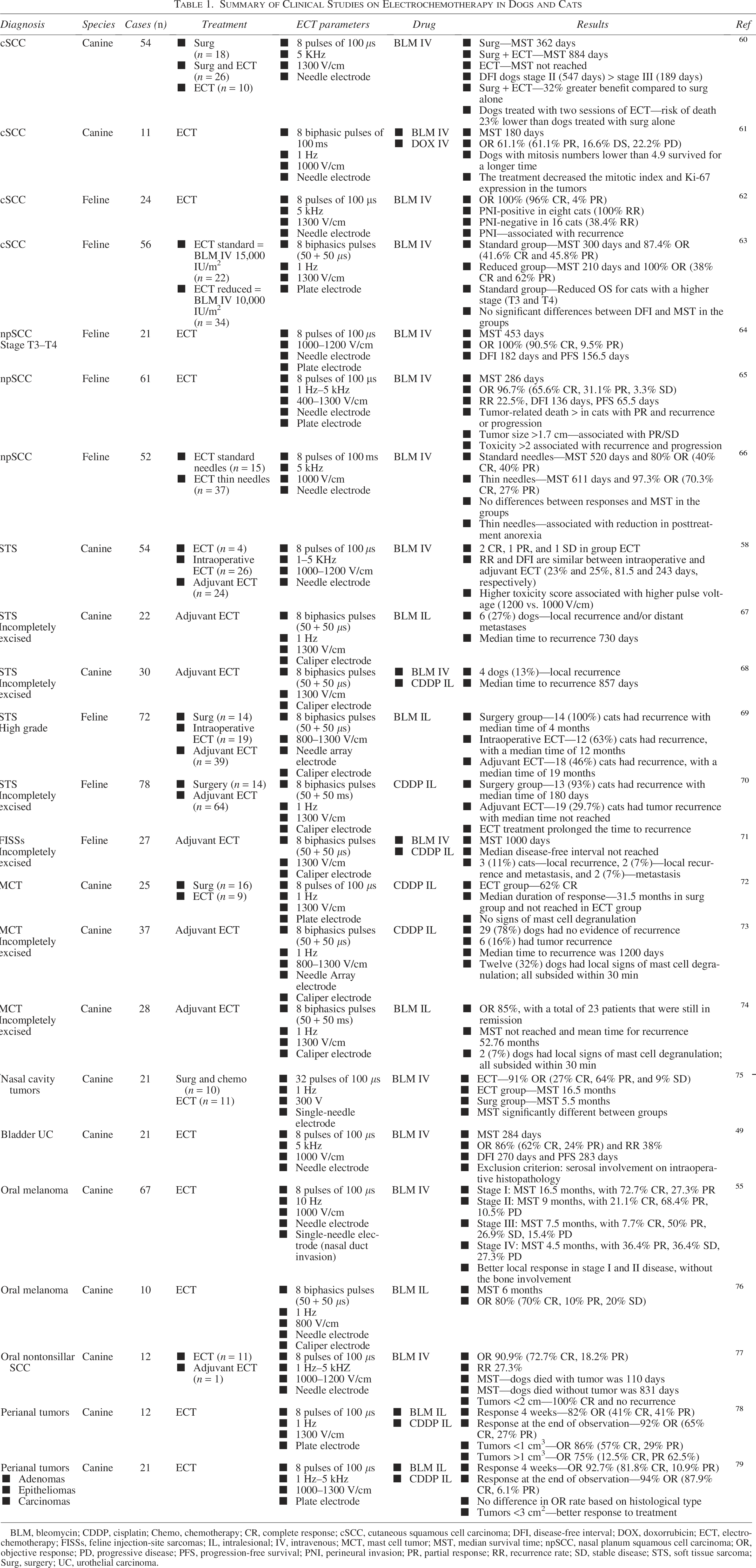
BLM, bleomycin; CDDP, cisplatin; Chemo, chemotherapy; CR, complete response; cSCC, cutaneous squamous cell carcinoma; DFI, disease-free interval; DOX, doxorrubicin; ECT, electrochemotherapy; FISSs, feline injection-site sarcomas; IL, intralesional; IV, intravenous; MCT, mast cell tumor; MST, median survival time; npSCC, nasal planum squamous cell carcinoma; OR, objective response; PD, progressive disease; PFS, progression-free survival; PNI, perineural invasion; PR, partial response; RR, recurrence rate; SD, stable disease; STS, soft tissue sarcoma; Surg, surgery; UC, urothelial carcinoma.
Clinical applications
Squamous Cell Carcinoma
Cutaneous squamous cell carcinoma (SCC) is a neoplasm resulting from the malignant proliferation of keratinocytes. It is associated with an invasive behavior, making local treatment an essential measure for disease control.80,81 The development of these tumors is commonly linked to chronic sun exposure, affecting primarily animals with white fur in depigmented and hairless areas such as the ventral and inguinal regions in dogs, 82 and the ears, temples, eyelids, and nasal planum in cats. 83
Anjos et al. 61 observed a clinical response in 60% of canine SCC cases treated with ECT. The median survival time of patients was 180 days, with a mitotic index cutoff of 4.9 being a prognostic factor. In parallel, Cunha et al. 60 identified the clinical stage as a prognostic factor, with treatment response rates of 89% and a median survival time of 884 days. ECT combined with surgery provided a 32% greater survival benefit in dogs compared to surgery alone. Moreover, patients undergoing at least two sessions of ECT had a 23% lower risk of death compared to those receiving only surgical treatment (Fig. 3).

Dog with actinic keratosis and squamous cell carcinoma treated with electrochemotherapy. (A) Pretreatment. (B) 290 days posttreatment. Created by the authors.
ECT is used to treat feline SCC in various facial locations, including the ears, temples, nasal planum, eyelids, and lips. 62 It is considered an effective first-line treatment for early-stage tumors. 65 However, patients with locally advanced tumors may also benefit from treatment. 64 Complete response rates are observed in 96% 62 to 40% 66 of tumors. The main prognostic factors include clinical stage,63,84 tumor size, treatment response, 65 and perineural invasion, which predisposes to recurrence. 62 Tumors at stage T4 84 or larger than 1.7 cm 65 are associated with a lower probability of complete response after treatment. Cats with complete remission show significantly superior overall survival compared to animals with partial response or stable disease 65 (Fig. 4).
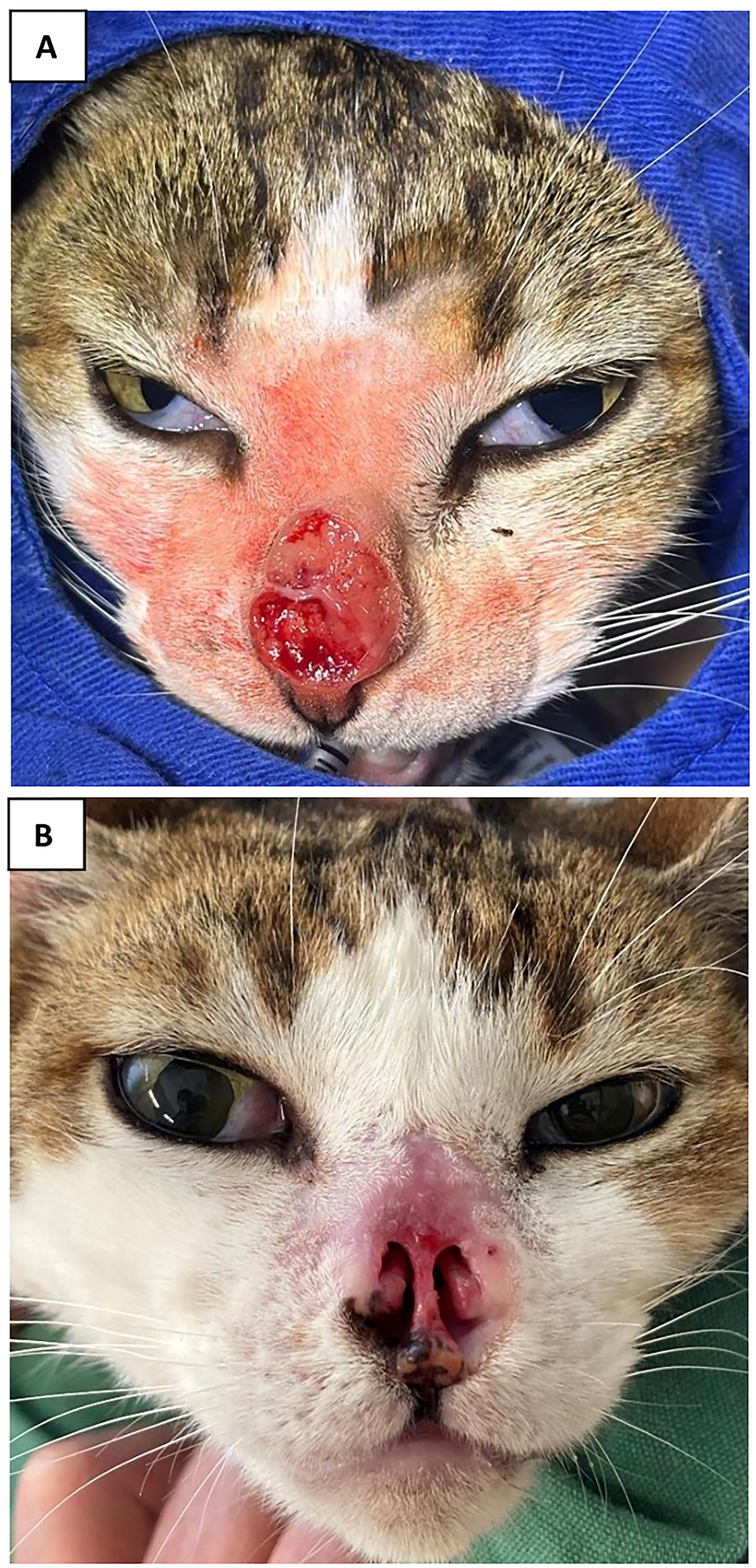
Cat with stage T4 squamous cell carcinoma on the nasal planum treated with electrochemotherapy. (A) Pretreatment. (B) 60 days posttreatment. Created by the authors.
Soft Tissue Sarcomas
Soft tissue sarcomas are a group of malignant tumors originating from mesenchymal cells, commonly affecting the skin and subcutaneous tissue in dogs and cats. They frequently arise in the limbs and exhibit invasive behavior, with local recurrence being a major clinical challenge.85–87 The primary goal of treatment is to achieve complete surgical excision with histological confirmation. However, obtaining clear margins is often difficult due to anatomical limitations, as these tumors tend to arise in the limbs and other areas that complicate wide surgical resection. 88 Cats may present sarcomas at vaccine injection sites or other areas of trauma that induce chronic inflammation. 89 These tumors have a high potential for infiltration. 90
ECT is used in the treatment of soft tissue sarcomas to eliminate residual tumor cells at the surgical bed or in compromised scars.58,67,68 Monotherapy should be avoided as a first option, as some tumors may only show a partial response or remain stable.58,91 In dogs, intraoperative or postoperative treatment for sarcomas with compromised margins results in similar recurrence rates, 23% 58 and 25%, 68 respectively. For cats with sarcomas, combining surgery with ECT has provided better local disease control. The median time to recurrence in cats treated with surgery alone was 180 days, compared to the median not reached with adjuvant ECT. 70 In another study evaluating surgery alone, intraoperative ECT, and adjuvant ECT, the median time to recurrence was 4, 12, and 19 months, respectively. 69 Spugnini et al. 71 treated only cats with injection-site sarcomas with adjuvant ECT and observed a recurrence rate of 18.5% and a median survival time of 1000 days.
Mast Cell Tumors
Mast cell tumors are common skin tumors in dogs. About 50–60% develop on the trunk, 25–40% on the limbs, and 10% on the head and neck. 92 Mast cell tumors exhibit variable biological behavior, ranging from benign to aggressive. The tumor’s behavior directly influences the occurrence of distant metastases, local recurrences, patient survival, and the need for systemic adjuvant therapy.93,94 Surgical treatment involves excising the tumor with safety margins, which are often difficult to achieve due to location and peritumoral inflammation. 95
ECT can be indicated as a monotherapy for tumors <3 cm with limited surgical access due to location or the presence of multiple tumors. This technique can be used intraoperatively when obtaining wide surgical margins is challenging or postoperatively when surgical margins are narrow or compromised. Electrodes should be directed from the periphery to the center to induce peripheral vasoconstriction and prevent mast cell degranulation. 94
ECT as monotherapy has demonstrated response rates similar to surgery, proving to be an effective and safe technique for treating small mast cell tumors. 72 For incompletely excised mast cell tumors, ECT offers a high local control rate, varying between 78% with a median time to recurrence of 1200 days 73 and 85% with a mean time to recurrence of 52.76 months. 74
Sinonasal Tumors
Sinonasal tumors are relatively common in dogs, and they often present with clinical signs such as epistaxis, nasal discharge, sneezing, stertor, nasal obstruction, epiphora, nasal congestion, and dyspnea. Patients with advanced disease may also show facial deformity, exophthalmos, and neurological signs such as seizures and behavioral changes. 96 The treatment of choice is typically radiation therapy, either alone or in combination with cytoreductive surgery, which helps prolong survival and improve quality of life.96,97 Lack of treatment or palliative therapy is associated with short survival times due to rapid disease progression. 98
ECT can be considered for intranasal tumors in cases where radiation therapy is declined by pet owners. The treatment can be performed minimally invasively using a single-needle electrode 75 or after rhinotomy and cytoreductive surgery. 56 ECT as a minimally invasive treatment for sinonasal tumors resulted in 91% objective response and a significantly superior median survival compared to a group of dogs treated with surgery and chemotherapy (16.5 vs. 5.5 months, respectively). 75 The insertion depth of the probe electrode should be carefully planned based on computed tomography imaging to avoid inadvertent passage through the cribriform plate. 75
Bladder Tumors
Urothelial carcinoma, also known as transitional cell carcinoma, is the most common cancer of the urinary bladder in dogs. It is a highly invasive neoplasia, with a metastasis rate of 14–16% at diagnosis and with local progression that leads to obstruction of the urinary tract. 99 Surgical resection is rarely indicated, as these tumors typically affect the bladder trigone and the proximal urethra, making wide surgical excision challenging. 100 Treatment usually involves chemotherapy and/or cyclooxygenase inhibitors. 101 The prognosis is poor, mainly due to local progression. 102
ECT can be used in the management of canine urothelial carcinoma through laparotomy and cystotomy, followed by the application of electric pulses to the tumor tissue and the entire internal bladder wall. Postoperative monitoring includes ultrasound evaluation to assess potential adverse effects and classify the response to treatment. 49 One previous study reported a clinical response in 86% of bladder tumors treated with ECT. To ensure safety and minimize complications, the authors excluded dogs with tumors staged as T2 with serosal invasion. Intraoperative histopathological examination was used to evaluate the degree of invasion. In these cases, the main complications observed were cystitis and temporary urinary incontinence. Two patients in the study developed ureteral stenosis and required surgical correction. 49 Another study (case series), which did not apply these safety criteria, found more severe postoperative complications, including vesical fistula, uroabdomen, hydronephrosis, and acute renal failure. A large tumor burden in the bladder wall was proposed as a potential risk factor for necrosis and loss of cellular cohesion. 103
Oral Tumors
The most common oral tumors in dogs are melanoma, carcinoma, and fibrosarcoma. In cats, carcinomas are more frequent, followed by fibrosarcomas. 104 Surgery is considered the primary treatment modality for local control of oral tumors, followed by radiation therapy. 105 However, aggressive oral surgery can be technically challenging, affecting both the animal’s oral function and aesthetic appearance. 106 In felines, some animals may not regain the ability to eat spontaneously and may require esophageal tubes for nutritional support. 107 Therefore, ECT can be offered to owners who refuse the financial burden of radiation therapy or the aesthetic and functional outcomes associated with surgery. 108 ECT can also be part of a multimodal treatment approach, combined with surgery, immunotherapy, and chemotherapy, to increase treatment success rates. 109
ECT can be indicated for tumors in any location within the oral cavity, provided the principles of the technique are followed. Tumors surrounded by teeth should not be treated before dental extractions to avoid interference with the distribution of the electric field and ultimately affect clinical outcomes. 50 While oral tumors without bone involvement present a better prognosis after ECT, an in-silico model has demonstrated the technique’s potential for treating tumor microinfiltration in bone tissue using plate electrodes and conductive gel in direct contact with the bone.4,108
ECT in monotherapy resulted in a clinical response in 70% 55 to 80% 76 of canine oral melanomas. Disease in stages I and II, along with the absence of bone involvement, are considered positive prognostic factors for local disease control. 55 For nontonsillar oral carcinomas, a response rate of 90% and complete remission of all tumors up to 2 cm were reported. 77 On the other hand, clinical studies specifically assessing feline oral tumors are lacking; isolated results demonstrate complete remission of early-stage oral carcinoma after a single session of ECT, despite its aggressive nature and difficulty in control. 62 A complete response to an oral anaplastic sarcoma and a partial response to an oral carcinoma have also been reported. 110
Perianal Tumors
Perianal gland tumors (hepatocellular) are common in dogs, with benign adenomas accounting for up to 81% of cases.111,112 Affected dogs are typically male, elderly, and intact, as these tumors have androgen and estrogen receptors. 112 The primary treatment is a combination of castration and surgical removal of the tumor. 111
ECT has been proven effective in treating perianal tumors, with objective response rates ranging from 82% 78 to 94%. 79 The advantages of ECT include its simplicity, short treatment duration, minimal adverse effects, and the absence of a need for hospitalization. 78 Tumors up to 3 cm2 show a better response to treatment than larger tumors. While larger tumors may also respond, the likelihood of complete remission is lower, and the area of necrosis following treatment tends to be larger. 79
Contraindications
Tellado, Mir, and Maglietti 50 compiled situations in which ECT as a sole modality (without surgery, for example) may require caution or where success rates may be reduced: (i) tumors near the larynx, which may cause edema and airway obstruction, necessitating temporary or permanent tracheostomy; (ii) tumors on the tongue, which may induce necrosis of its rostral portion due to vascular blockade, indicating the combination of ECT with cytoreductive surgery; and (iii) tumors affecting the cribriform plate, retro-orbital region, and other structures that are difficult to access with electrodes, increasing the chances of treatment failure.
The technique is contraindicated for pregnant or lactating females, as well as for patients with hypersensitivity or allergy to chemotherapy agents. 48 Bleomycin should not exceed a cumulative dose of 200,000 IU/m2 in dogs due to the risk of pulmonary fibrosis. 113 No established cumulative dose value exists for cats. 50
Adverse effects
The adverse effects of ECT are local, including involuntary contractions, pain, erythema, edema, and necrosis. 114 Pet owners must be informed in advance about the risk of extensive necrosis, particularly in large tumors, which may result in anatomical defects that can either be asymptomatic or require surgical correction. 115 The treated area may exhibit hyperpigmentation/hypopigmentation and alopecia after healing. 116
Monotherapy with ECT often results in erythema and edema within the first week, followed by necrosis and scab formation. 117 Treatment in the surgical bed may be accompanied by local inflammation and occasional dehiscence.60,69 The primary complication related to the use of this technique in the postoperative period is some degree of transient inflammation. 71 Lowe et al. 118 developed a 6-point local toxicity scale for ECT: 0: no toxicity; 1: mild edema; 2: edema/necrosis <1 cm; 3: severe edema; 4: deep necrosis; and 5: severe edema and tissue loss. Mild local toxicity (score ≤2) was observed in 66.7% and 53% of dogs with soft tissue sarcomas and mast cell tumors (MCTs), respectively.58,118 For canine oral melanoma and oral nontonsillar carcinoma, toxicity was ≤2 in 95% and 91.7% of cases, respectively.77,115 In cats with SCC, ECT toxicity was ≤2 in 51% of cases, while those with toxicity >2 had a higher probability of tumor recurrence or progression. 65
Follow-up
Patients are typically discharged with a prescription for anti-inflammatory drugs, opioids, and broad-spectrum antibiotics. 118 Healing after monotherapy with ECT occurs by second intention within 4 to 8 weeks, depending on the tumor size and response to treatment. 119 The response is classified according to the criteria of the Veterinary Cooperative Oncology Group 120 as follows: complete response when total lesion disappearance occurs; partial response when there is a reduction ≥30% in tumor volume; progressive disease when new lesions appear or there is a ≥20% increase in tumor volume; and stable disease when there is a reduction of <30% or an increase of <20% in lesions (Fig. 5).

Illustration of the electrochemotherapy process for a canine skin tumor. Created with BioRender.com.
In monotherapy, ECT achieves a complete response rate of 60–70% for tumors up to 3 cm in diameter after a single session. 48 Additional sessions may be required in cases of partial response or recurrence. The recommendation for a new session of ECT generally does not occur in less than 4 weeks, as this is the period for assessing the treatment response.52,65
Follow-up for patients is planned individually and is necessary for classifying toxicity, assessing treatment response, and identifying potential recurrences. Patients should return at least at 15 days, 1 month, 2 months, 4 months, and 6 months. 50 In intensive schedules, patients return weekly during the first month, monthly until 6 months, and then every 3–6 months. 84 Patients with malignant tumors may benefit from extended follow-up periods to monitor for potential recurrences or metastases.
Perspectives
Future directions in veterinary ECT should focus on prospective, controlled studies aimed at identifying prognostic factors and evaluating the comparative efficacy and potential synergistic effects of ECT in combination with established treatment modalities. A lack of robust comparative studies is evident even in human medicine. For instance, a recent systematic review failed to directly compare outcomes between ECT and radiotherapy in the treatment of primary cutaneous malignancies or cutaneous metastases, primarily due to inherent biases and significant heterogeneity among the included studies. These limitations prevented a consolidated synthesis of clinical outcomes between the two approaches. 121 At the preclinical level, evidence suggests a potential synergistic effect when ECT is combined with radiotherapy. This combination has consistently demonstrated superior tumor response rates compared to either treatment alone, supporting its clinical rationale. However, conclusive evidence regarding a specific ECT-induced radiosensitization effect remains unavailable. 122
Moreover, recent case reports in veterinary medicine have highlighted possible clinical benefits from combining ECT with other therapies. For example, a case of feline progressive histiocytosis achieved complete remission through a multimodal protocol involving toceranib, chlorambucil, and ECT. 123 Similarly, a nonoperable oral SCC in a dog showed clinical improvement following palliative treatment with ECT and toceranib. 124 Although these findings are encouraging, they are anecdotal and emphasize the need for well-designed clinical trials to validate the efficacy of multimodal treatment strategies.
Technological advancements, particularly in electrode design and image-guided treatment planning, may further expand the clinical applications of veterinary ECT for deep-seated tumors that are not suitable for curative surgery. In human oncology, studies have demonstrated the safety and feasibility of laparoscopic electrode use for the treatment of liver 125 and pancreatic 126 cancer, as well as image-guided percutaneous electrode placement126,127 for the treatment of liver tumors. 127 This type of minimally invasive approach may contribute to faster patient recovery and reduced hospitalization costs. To the best of the authors’ knowledge, there are no reported cases of laparoscopic ECT in veterinary medicine and only one report describing the percutaneous use of ECT for the treatment of a deep-seated tumor. The case involved a cat with a thymoma whose owner declined surgery and radiotherapy. The animal was treated with two sessions of ultrasound-guided ECT and achieved a partial response, which was maintained for at least 14 months at the time of publication. 128
Conclusions
ECT has been considered an effective and safe treatment for local tumor control in dogs and cats. This therapy combines electroporation with hydrophilic chemotherapeutic agents, such as cisplatin and bleomycin, to enhance the cytotoxic effects of these drugs. It can be used as a standalone treatment or in combination with surgery, either intraoperatively or postoperatively, to eliminate residual disease.
Clinical studies have demonstrated promising results of ECT in the treatment of cutaneous and subcutaneous tumors, including SCC, mast cell tumors, and soft tissue sarcomas. The treatment has been offered either as a first-line therapy or when pet owners decline other treatment modalities, such as surgery or radiation therapy. Tumors smaller than 3 cm may be effectively treated with ECT alone when there is no infiltration into deeper tissues. Larger and/or infiltrative tumors require a combined approach involving surgical resection. Individualized treatment planning based on patient comorbidities, tumor location, degree of infiltration, and histological type is recommended.
ECT has been employed for a range of tumors, not limited to cutaneous and subcutaneous lesions. Dogs with oral tumors, such as SCC and melanoma, may achieve good local control with ECT. However, bone infiltration is considered a poor prognostic factor when monotherapy is employed, and further studies on the use of combined therapies are needed. For intranasal tumors, only one clinical study has been published to date, showing promising results using a minimally invasive approach with a single-needle electrode. The application of ECT in bladder tumors requires additional caution during patient selection, as serosal infiltration may result in uroperitoneum due to necrosis of the bladder wall. Intraoperative histopathological assessment is essential to ensure the safety of the procedure. In addition, ECT alone is a simple, short, and low-toxicity option for perianal tumors, mainly indicated for small benign lesions.
Robust studies are needed to better understand the clinical, morphological, and molecular factors of tumors influencing treatment response, to compare outcomes with other therapeutic modalities, and to collect clinical data on the effectiveness of multimodal approaches. In the future, the development of new electrode designs may enable the expansion of ECT for the treatment of deep-seated tumors, using laparoscopic or image-guided percutaneous techniques.
Authors’ Contributions
A.G.A.H.: Writing—original draft preparation and conceptualization. M.M.M.R. and G.F.d.Q.: Writing—review and editing. J.M.M.: Writing—review and editing and supervision.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001.