
Abstract

1. Introduction
The COVID-19/SARS-CoV-2 pandemic presents an unprecedented and extraordinary challenge to global health. Cases, as well as mortality, continue to increase globally. To prevent the spread of disease and control the pandemic, numerous studies involving human participants are performed and many COVID-19 vaccine candidates, including multivalent ones, are currently in development. These vaccines are based on various platforms, including mRNA and DNA technologies, including viral vectors, subunit, inactivated, and live attenuated vaccines. 1 Thus, vaccines to protect against COVID-19 are critical to mitigate the SARS-CoV-2 pandemic and to prevent future disease outbreaks.
Given the speed at which vaccine development is occurring, researchers may be tempted to compromise quality control and rigor in a desperate race to find a cure and vaccine. However, crises are not a reason for lowering the bar of high ethical and scientific standards and ethicists have warned scientists not to cave into bad science. 2 Unethical experiments involving human participants are disturbing; however, considering them is instrumental in understanding the consequences of these historical atrocities and their destruction of public trust and confidence in scientific developments. 3
Currently, there are COVID-19 vaccine rollouts in many countries, including Australia. However, there is no guarantee that these new and emerging vaccines are entirely effective and safe. Further, it remains uncertain as to how long the protection/immunity lasts for those who receive the vaccine. 4 Thus, there is a strong and urgent need to continue conducting studies and clinical trials on COVID-19 vaccines to improve their ongoing safety and efficacy, especially since COVID-19 vaccines for children under age 12 continue to be a work in progress and trials involving younger populations will require ongoing attention.
This paper explores and critically analyzes the current regulation and governance of studies and clinical trials for the COVID-19 vaccine (with a focus on the Australian regulation) and examines whether and to what extent it ensures ethical treatment of all human trial participants in these studies.
2. Clinical Trials and Phases to Ensure Research Rigor
Epidemics and pandemics are a regular feature in the 21st century ranging from SARS to MERS, HINI and Ebola. Thus, it is critical to continue conducting clinical studies and trials. Often, there are various concerns expressed about whether the new vaccines or drugs are safe and effective.
Most medical discoveries require years or decades of research pursued by universities, research institutes, and private organisations. 5 They require a tedious, costly, and slow process that progresses from basic research to clinical research and phase 1, 2, 3, and 4 trials. An accepted medical treatment is peer-reviewed, safety proven through large-scale clinical trials and regulated by government regulatory bodies.
Clinical research trials are defined by the WHO as “any research study that prospectively assigns human participants or groups of humans to one or more health-related intervention(s) to evaluate the effects on health.” 6 Clinical trials are essential in determining whether new interventions are effective or safe, including new drugs, vaccines, cells and other biological products, surgical procedures, radiological procedures, devices, behavioral treatments, education interventions, screening or diagnostic tests, and/or preventative care. Human participants are essential throughout this testing, as computer simulation and animal testing are “no substitute for testing in a living human being'” 7
Around the world, clinical trials are assessing investigational COVID-19 vaccines in tens of thousands of human study subjects to generate scientific data and other information to determine safety and effectiveness. 8 It is stressed that these clinical trials are performed according to strict, rigorous standards. Clinical trials require a broad range of human participants; they include healthy individuals, patients exposed to the illness or disease the intervention is targeting, individuals experiencing different levels of disease severity, and recovered individuals, as well a diversity of age, sex, race and ethnicity, socioeconomic status, medical comorbidities, etc.
Typically, in phase 1 of the clinical trial, the vaccine is provided to a small number of generally healthy participants to evaluate its safety at increasing doses and obtain early data regarding how well the vaccine works to induce an immune response in humans. In the absence of safety concerns in phase 1 studies, it progresses to phase 2, which includes more people, where different dosages are tested on hundreds of people with varying health statuses and from different demographic cohorts in randomized-controlled studies. These studies provide extra safety information on the common short-term side effects and risks, analyze the link between the dose administered and the immune response, and provide early data about the vaccine's effectiveness. During phase 3, the vaccine is generally administered to thousands of people in randomized, controlled studies involving broad demographic cohorts (i.e., the population intended to use the vaccine) and generates vital information on the effectiveness and additional crucial safety data. In addition, this phase provides further data regarding the immune response in people who receive the vaccine compared to those who receive a control, e.g., a placebo.
While there are COVID-19 vaccine rollouts in several nations and governments have signed deals to purchase hundreds of millions of doses of various vaccines being developed, it is noted with caution that these vaccines are not 100% safe and it is expected that there are side effects, mostly mild, experienced by some individuals, as with most vaccines. Disturbingly, however, there were also severe side effects reported involving blood clots and fatalities. For instance, several countries suspended using the Oxford-AstraZeneca COVID-19 vaccine as a precautionary measure after receiving reports of blood clots and deaths. 9 On 10 March 2021 the European Medicine Authority (EMA) said that the Austrian government had decided to discontinue using the AstraZeneca vaccines after one person suffered multiple thromboses and died ten days after receiving the vaccination. 10 The regulatory bodies are investigating whether there is sufficient evidence to link the vaccination to thromboembolic events. Indeed, such decisions are a further setback for the vaccination programme, which has struggled to pick up speed, partly because of delays in delivering the AstraZeneca vaccine. In Australia, there have been similar fears about getting the AstraZeneca vaccine and clinics have seen an increase in cancellations from concerned people booked for their second dose. 11
3. The Need to Continue Further Studies and Treatments for COVID-19
Historically, vaccines have taken multiple years to develop, with the fastest previous development spanning four years for Mumps in the 1960s. 12 However, in early 2020, when the scientific world turned to the development of a COVID-19 vaccine, the process took less than a year. Scientists capitalised on decades of research into both RNA and DNA vaccines culminating in a range of viable vaccine options by January 2021. The below graphic demonstrates the timeline to develop the SARS-CoV-2 vaccine relative to other significant vaccines in the 18th and 19th centuries.
Timeline to develop vaccines
As of October 1, 2021, over 6.1 billion COVID-19 vaccines had been administered across the world. 14 However, there is no guarantee that these new vaccines are entirely safe and effective. 15 Thus, there is a strong and urgent need to continue with further clinical trials on covid-19 to improve its safety and efficacy.

Vaccine Development Timeline (Ball 2020). 13
Currently, there are 123 COVID-19 vaccines in clinical trials, and 194 vaccines in pre-clinical trials, each utilising different techniques and target proteins. 16 The vaccines largely vary in the protection offered, and it is not yet clear which one is considered the “best” vaccine against the present pandemic, as exemplified in the table below. However, it is critical to note that the effectiveness, and level of protection of a specific vaccine is dependent on the strain of COVID-19 that it is meant to protect against.
Varying protection of the different vaccines
The Pfizer/BioNTech vaccine was the first to complete the Phase 3 trial. An additional COVID-19 vaccine may have a different safety profile for a particular risk group or be more cost-effective or easier to transport, etc. These factors only become apparent when vaccines are researched in safety trials. The mRNA platform that Pfizer used for their vaccine was initially developed as an Ebola vaccine. Had this research not been undertaken, the platform may not have allowed the rapid development of these new covid vaccines.
Vaccine Efficacy by Vaccine Type, and Continent
(Cohen 2021b). 17
Moreover, there is no COVID-19 vaccine yet for children under age 12. 18 Several companies have begun enrolling children as young as age 12 in COVID-19 vaccine clinical trials. 19
In recent news, a scientific team from Scripps Research, California, announced that they had developed a novel HIV vaccine approach that shows promise. Their next step is to use mRNA technology that could expedite HIV vaccine development, as it did with the vaccine for COVID-19. 20 Indeed, it is often beneficial to research additional vaccines as the data gathered can benefit vaccine development down the track. Currently, scientists are researching a broadly protective vaccine (called pan-coronavirus vaccine) that promises to protect against the different types of coronaviruses that could avoid another pandemic in the future. 21 In addition, a later generation COVID-19 vaccine could be effective against variants (like an endless game of whack-a-mole) of the virus.
4. Improving Clinical Trials Amid a Pandemic while Ensuring the Ethical Treatment of Participants
The current pandemic has paved the way to improve how clinical trials are performed. As a result, at a previously inconceivable speed, clinical trial research has occurred all over to address the public health crisis.
Clinical trials are expensive. Despite huge costs, conventional clinical trial drawbacks include time-consuming recruitment and consent processes, tedious event adjudication, and limited generalisability. These have collectively limited their capacity to provide speedy answers to clinical questions and burden trial participants. Thus, initiatives have been created to tackle these drawbacks. For instance, the Clinical Trials Transformation Initiative was founded to generate novel methods to improve clinical trials' quality and efficiency. 22 However, despite the introduction of this, the application of innovative strategies has remained limited.
Gaba and Bhatt suggest various innovative patient-friendly changes while also ensuring participants' ethical treatment, including the following. 23 Firstly, the recruitment of diverse cohorts of participants. This has been a continuous challenge for principal investigators running clinical trials. However, many sites care for patients of different ethnicities and socioeconomic statuses, the participants who complete trials are less diverse, which have the effect of hampering trial generalisability. The use of social media has been recommended to reach a more extensive and diverse cohorts. While this approach has been successful to an extent, there are trials that continue to struggle to enroll various patient-participants. Especially for COVID-19, this issue becomes critical for medical conditions that affect people unevenly according to race, gender, and socio-economic background. Amidst the pandemic, social media and digital health platforms have been leveraged in novel ways to enroll heterogeneous cohorts of participants. The social media approach to trial recruitment has had success regarding a randomized clinical trial of hydroxychloroquine as post-exposure prophylaxis for COVID-19. The social media outreach resulted in the enrollment of more than 800 patients, half of whom were women, in less than two months, which was a phenomenal speed. Further, the PCORnet, Healthcare Worker Exposure Response and Outcomes, is enrolling healthcare workers in clinical trials related to COVID-19 and has recruited more than 16,000 health-care workers and connected a number to the current trials. 24 Also, the World Without COVID is recruiting people for a multitude of clinical trials online. 25
Secondly, the provision of remote consent: difficulties in getting the patients' consent can impede enrollment. The FDA employed innovative approaches to the consent process to address this issue, such as phone calls or video visits. 26 The participants orally acknowledge their intention to be part of the clinical trial and signs or has a witness sign the form and e-mail an image of it. Clinical trials which adopt these electronic mediums can obtain patient consent with fewer difficulties.
Thirdly, the adoption of telemedical monitoring and trial visits: due to the strict lockdown measures, onsite monitoring programmes and face-to-face visits have been changed to remote monitoring. Technologies such as Zoom are being utilised to increase efficiency and safety during patient consultations while ensuring quality monitoring. Home health-care visits can be executed with personal protective equipment where in-person visits are needed.
Remote event adjudication can be conducted in place of in-person ascertainment of clinical trial endpoints (which has conventionally been the gold standard for accurate recording outcomes for clinical trials). Ascertainment and adjudication of clinical endpoints can be performed remotely, akin to consent and monitoring. Phone calls, e-mails, and text messages will replace in-person visits to determine the occurrence of clinical events. Collectively, these steps are a lot cheaper and flexible compared to the previous in-person adjudication and can involve the safe presence of more medical teams and oversight during trial participant consultations.
Finally, novel, and efficient trial designs: a significant drawback of clinical trials is their great expense. However, the pandemic has led to the creation of creative novel trials. For example, the NIAID-sponsored Adaptive COVID-19 Treatment Trial (NCT04280705) 27 and the WHO-sponsored SOLIDARITY trial (ISRCTN83971151) 28 are leveraging adaptive clinical trial designs, in which several, prespecified, investigational treatments can be compared with placebo to identify subgroups of patients who respond best to them. In addition, pragmatic trial designs have also been recommended to evaluate treatments in the broader array of patients with the disease and increase the success of clinical trials.
Prompt ethics approvals are also crucial. 29 The necessity for clinical trial speed has prompted the need for quicker ethics approvals, not because there is less oversight but because ethics committee members are increasingly part and parcel of research meetings. In such settings, known as the integrated format, representatives from the ethics committee sit in the weekly research meetings to take any issues back to the ethics committee and figure out a solution. Moreover, this integrated format may assist the researchers in seeing the view of the ethics committee. As a result, a site-specific ethics clearance that previously took a minimum of two months can be finalised in weeks.
More research teams are planning studies using “adaptive design,” where a clinical trial is adjusted as it progresses based on new knowledge. This is especially important in novel diseases such as COVID-19, where the standard treatment, known as “background therapy,” can change as recent developments emerge. Teams can meet each week to explore the latest literature and trends and adjust background therapy accordingly. In addition, patients can influence how a study is conducted through patient and community input. What researchers and clinicians want to discover from a clinical trial is not necessarily what the society considers essential, and that issue is not limited to COVID-19-related studies.
It is clear that in order to improve clinical trials and continue to ensure the ethical treatment of participants, regulatory agencies, such as the FDA or Therapeutic Goods Association (TGA), along with the sponsors of clinical trials, should consider making remote consent, telemedical monitoring, and remote event ascertainment a feature of all clinical trials, whether they relate to COVID-19 or not. The progress of these trials using technology has further revealed that governments must provide or improve access to web-based technologies for participants in lower socioeconomic groups. Lastly, there should be prompt ethics approvals for clinical trials and the adoption of adaptive designs. COVID-19 has prompted us to consider more agility in the health system and how clinical trials are conducted.
5. Human Challenge Studies/Controlled Human Infection Studies
The present pandemic is unique and different from those previously encountered. Currently, numerous vaccine candidates are undergoing human safety testing all over the world. The duration of a vaccine's development could be reduced by adopting the “human challenge approach”, also known as controlled human infection studies (CHI). These challenge trials have been conducted to develop vaccines and treatments across several illnesses such as malaria, typhoid, norovirus, common cold, and influenza.
Human challenge studies (HCS) involve purposely infecting vaccinated participants with COVID-19. The vaccinated volunteers are given a dose of the virus so the scientist can determine whether the vaccine works. 30 While there are already vaccine rollouts, a challenge study can complement the data. In contrast, the conventional vaccine trials involve inoculating some volunteers with a vaccine and others with a placebo (consisting of salty water) to test if vaccinated people are less likely to be infected. In these conventional trials, the volunteers return to their regular under real-world conditions. As a result, there is a probability that only a small number of people would become infected. Thus, it could take a considerable amount of time to see the results.
The first COVID-19 HCS has just received approval in the United Kingdom. 31 Up to 90 healthy young volunteers (between 18 and 30) will be exposed to COVID-19 in a safe and controlled environment to increase knowledge of how the virus affects humans. The first-of-its-kind study for this type of virus will involve determining the least amount of virus needed to cause infection, which may give doctors a better understanding of COVID-19 and help support the pandemic response by aiding vaccine development.
Given the direction of these trials, the safety of these volunteers has been critical. During this trial, the virus characterisation research will use the version of the virus circulating in the U.K. since the pandemic began and has been demonstrated to be of negligible risk in young, healthy adults. Medical staff and scientists will closely monitor the effect of the virus on these volunteers and will be on hand to watch them 24 hours a day. As compensation for their time, the volunteers will receive £4,500, which includes follow-up tests.
However, there are serious concerns raised about HCS. Purposely infecting volunteers with a disease as dangerous as COVID-19 has been regarded as unethical by some scientific communities despite the clear evidence that accelerating the process of vaccine development could result in saving many lives.
It can be argued that HCS is justifiable, and it is also ethical to take certain risks. In many spheres of life, it is not unusual for society to allow people to pursue matters that would put them in danger, whether it is smoking, or riding a bike, or being a soldier or astronaut. 32
A critical question for this type of experiment is whether all risks are spelt out to the volunteers. Dr. Richards designed guidelines to guide researchers on an ethical path. 33 These guidelines are beneficial to regulators and ethics committees when considering HCS with COVID-19. In his study, Dr. Richards evaluates the standard arguments against HCS experiments, including the risk of harming participants, the risk of developing an ineffective vaccine and the lack of robustness of a volunteer's informed consent. He explains that these specific concerns can however be addressed and reminds researchers that the bar of ethical standards need not be lowered to allow these types of experiments. He argues that following his proposed guidelines will ensure that the research is carried out ethically.
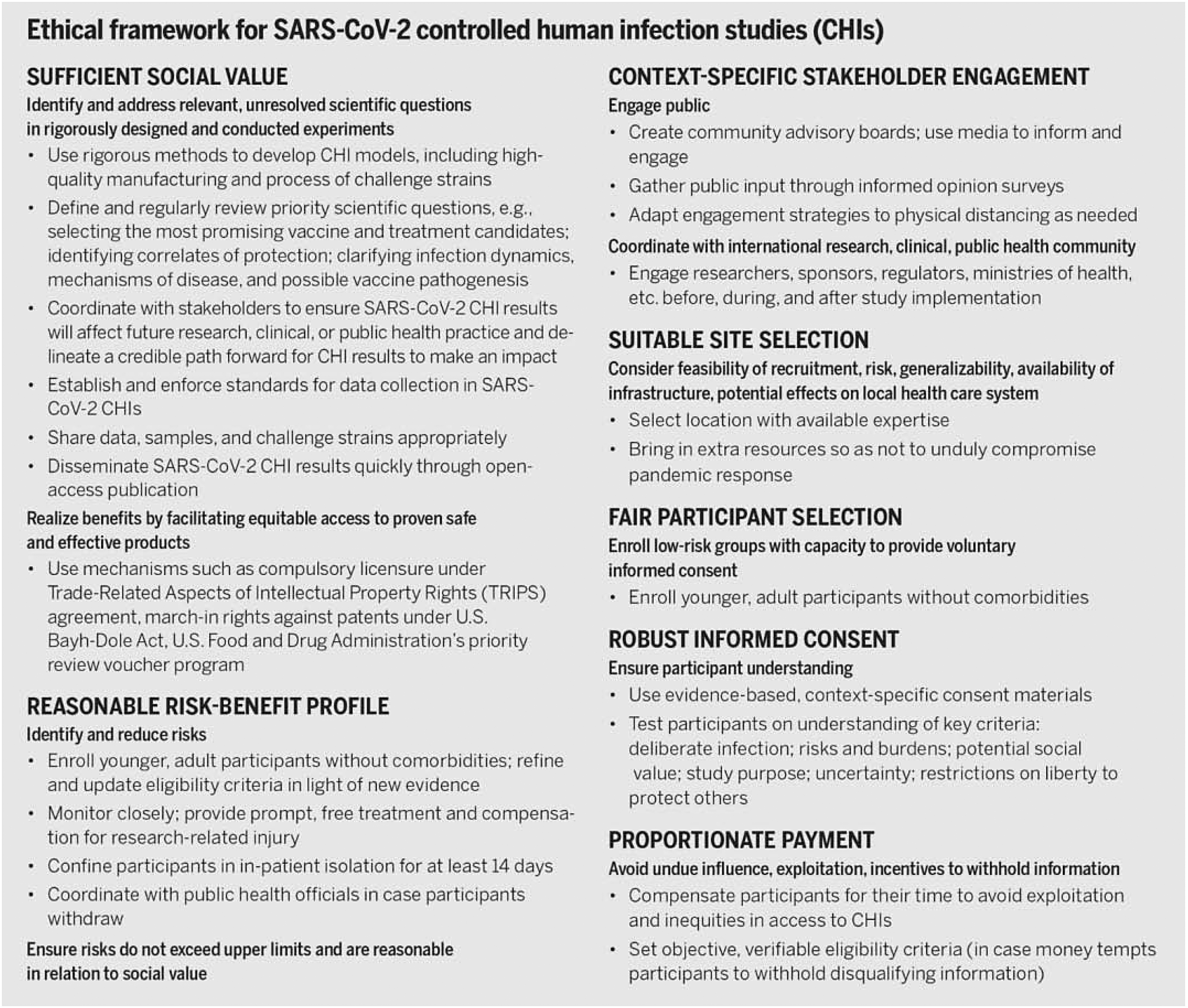
Ethical framework for SARS-CoV-2 controlled human infection studies (CHIs) (Shah, Miller, Darton, et al 2020, 7). 36
Dr. Richards poses crucial questions for researchers who have plans to conduct vaccine development research and reminds researchers to question whether reasonable care has been given to maximise the study's potential benefits and minimise the risks of harm to research subjects. This may include, in the case of a HCS COVID-19 trial, questions concerning the availability of ventilators for the participants if needed. He also suggested a pragmatic approach when interpreting the phrase ‘reasonable care’ to mean good enough care instead of ideal care.
The informed consent process must be rigorous to the extent that participants must comprehend the likely risks and benefits of participating and be provided with the most current data so that the consent can be ongoing as new data emerges. A psychological evaluation of the cognitive capacity of participants may further be needed. Dr. Richards stressed the importance of providing a reasonable reflection period to the potential participants, say three days before consenting and that at all times, they have a right to withdraw. If there is monetary payment, it should be a modest amount.
Currently in the UK HCS study, there is a desire to recruit younger human trial participants, as the current cohort are aged between 18 and 30 years of age. Younger participants, however, are not guaranteed less risk as these populations are receiving a dangerous virus and it could end in death with no cure. As a result, high-quality informed consent is crucial with an ongoing requirement to maximise participant comprehension of the experiment and its risks. This process may be facilitated by requiring the potential participants to pass a test on vital study information. 34 Continuous informed consent however is essential as new developments emerge, such as more knowledge of the virus and its modes of transmission. Long-term follow-up of the participants is also critical.
During some clinical trials, the sponsors may offer a sum of money to participants, as in the U.K. HCS, where each participant was offered £4,500 (more than A$8,000). Fairness calls for offering participants pay for their time and effort. However, it is stressed that the level of remuneration for participation in studies should be modest. During a pandemic, many people would have lost their jobs leading to financial desperation and the possible attraction of vulnerable participants. The serious concern is that the money offered to them may operate as an inducement/undue influence to participate in the experiment which may raise further ethical concerns.
In a paper by Shah et al., an ethical framework for COVID-19 HCS was formulated (see the diagram below). 35 It comprises the following conditions: demonstrating high social value, reasonable risk-benefit profile, context-specific stakeholder engagement, appropriate site selection, fair participant recruitment (e.g., young, and healthy adults), robust informed consent, and proportionate payment to participants. While some of these proposed conditions overlap with Dr. Adair's guidelines, additional factors in this ethical framework were needed to ensure the stakeholder engagement was undertaken, public opinion surveys were conducted, rigorous clinical trial site selection and quality care to participants to ensure risk is minimised.
The world is watching UK HCS closely and WHO has provided conditional approval to this extraordinarily contentious practice of HCS for COVID-19 vaccines. 37 However, the ethical issues surrounding COVID-19 HCS cannot be ignored and the continued need for a stringent regulatory framework is clear.
6. The Regulation of Human Research in Australia: Does it Ensure Ethical Protection to Participants in Research on COVID-19 Treatment?
This section of the article examines the current Australian regulation of human research. It provides a critical analysis of whether its regulatory framework ensures adequate safeguards afforded to all subjects in human research on COVID-19 treatment.
The foundational principles of medical research ethics originated from a blend of norms historically derived from the Hippocratic Oath (do no harm) and those that have emerged in the aftermath of the Nuremberg Nazi doctor trials. During World War II, atrocities that occurred during medical experiments conducted on concentration camp prisoners by the Nazis led to the development of a set of ten universal principles by the Nuremberg Military Tribunal in 1947 with which the conduct of research involving human participants must conform. This set of principles are known as ‘the Nuremberg Code’. 38 The Code requires that participation in research must be voluntary and that the research results must be valuable and unobtainable by other means; they must also be rationally based on knowledge of the disease or condition to be studied and avoid unnecessary suffering. The Code also requires that the research cannot include death or disabling injury as a foreseeable consequence; benefits of the research must outweigh its risks; proper facilities to protect participants must be used, and qualified individuals must conduct the research. Notably, the Code requires that participants should be able to withdraw from the study at any time if they wish and researchers must be prepared to stop the study should participants die or become disabled because of participation. Indeed, all research subjects must be able to trust the system.
Like the international codes and guidelines, the Australian regulatory framework and oversight are also comprehensive. Operating in conjunction with these laws are the governance structures and guidelines for the ethical conduct of health and medical research. The central government body in Australia relevant to human research is the National Health and Medical Research Council (NHMRC). It is responsible for various responsibilities, such as issuing guidelines and setting ethical standards for study and research funding. In addition, the Australian Research Council (ARC) advises the government on research and administers the National Competitive Grants Program (NCGP), a component of Australia's investment in research and development.
The National Statement was developed jointly by NHMRC, ARC, and Universities Australia. It accords with the Declaration of Helsinki, stating its main objective to “promote ethically good human research.” 39 It sets out various responsibilities intended to be in harmony with the global human rights instruments Australia has ratified. The National Statement underscores values that reflect research merit and integrity, justice, beneficence, and respect for human beings.
6.1 The crucial role of human research ethics committees
Under the National Statement, every proposal to perform research and clinical trials involving human participants in Australia require ethical review and approval by a Human Research Ethics Committee (HREC). HRECs must be known to the Australian Health Ethics Committee (AHEC) of the NHMRC. In addition, they must provide assurances they are operating following NHMRC National Statement and other guidelines.
The ethical approval and the extension of the approval for a research project by the HREC may only occur when the following conditions are met:
the research must be performed following the approved protocol/project description; there must be reports on the progress of the trial and any safety reports or monitoring requirements as indicated in the NHMRC guidance and accordance with the manner and form specified by the review body; any alterations to the project must be submitted for approval, including amendments that: a. are recommended to remove immediate risks to participants; b. may increase the risks to subjects; or, c. considerably affect the conduct of the study; and, the review body must be informed of new safety data that could affect the continued ethical acceptability of the project or may suggest the necessity for amendment of the research project and for clinical trials with implantable medical devices, set up processes that enable tracking of the research subjects, with their consent, for the device's lifetime.
40
The HREC should also be satisfied that there is a plan to ensure there are adequate resources to start and finish the project and that the skill, experience, and amenities are adequate and appropriately assigned for the project to be completed safely. 41 In addition, research participants must be sufficiently informed about research funding. 42
It is also essential that human research has robust safety monitoring and reporting mechanisms and that the HREC is informed of these: 43 for example, standard safety reporting and the use of a Data and Safety Monitoring Board (DSMB), a formalised committee tasked with evaluating a trial's accumulating results, or an identified expert or committee with the appropriate expertise to advise the institution and/or review body in fulfilling their monitoring duties. High-risk clinical trials will usually have in place a DSMB. However, there are no mandatory conditions that govern how these committees are to be organized or how they execute their tasks. 44
In Australia, researchers must refer to all relevant NHMRC documents addressing these issues. 45 In addition, at specific periods, reflecting the extent of risk, and at least yearly, and after the project is finished, researchers should submit various reports on the progress to date, or in the case of completed research, its result, maintenance and security records, compliance with the approved proposal, and compliance with conditions of approval, if any. 46
As some participants may suffer adverse effects due to the clinical trial, which entails various types of risks, institutions must ensure that the clinical trial sponsor has indemnity insurance and compensation schemes following relevant regulatory requirements. 47 Regarding monitoring ongoing clinical trials, it is noted with concern that some HRECs have limited time to carry out this function. 48
6.2 Critical aspects to ensure ethical safeguards for participants in clinical trials and studies: risk-benefit analysis, informed consent and adopting innovative technologies
In the following sections, there are discussions on various crucial aspects exploring whether and to what extent they ensure the ethical protection of participants in human research. The elements include the risk-benefit analysis, whether informed consent was provided by the participants, and the need to employ modern technologies in clinical trials to ensure the safety and convenience of the participants.
6.2.1 The risk-benefit calculus
The studies' potential benefits must outweigh the risks involved or else the research involving human participants is considered ethically unacceptable. 49 The benefits include gains in knowledge, insight, and understanding, improvement in the lives of family, friends, or others, and gains in expertise for researchers, their teams, or their institutions. 50 In attempting to determine whether the identified benefits outweigh the risks of a clinical research trial, it will be necessary for the researchers to identify, gauge, and minimise the risks to the greatest extent possible. Researchers and the HREC must, when designing and/or reviewing proposed research, consider the “profound tension between the obligation, on the one hand, to give maximum scope to participants' freedom to accept the risk and on the other to see that research is conducted in a way that is beneficent and minimises harm.” 51
6.2.2 Genuine informed consent by participants
Present approaches to informed consent in research often follow a regulatory regime which can be traced to The Nuremberg Code, which provides that a research subject “should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion.” 52 Thus, consent is fundamental to participation in a clinical research trial and is required under every international and national code of practice and guideline above-mentioned as well as under domestic and international law. However, informed consent has limitations, including but not limited to, age, cognitive function, and the financial incentivisation of participations. Moreover, there is complexity with obtaining authentic consent from participants in HCS. These challenges will be explored below.
As established by as The Nuremberg Code, each subject's decision to participate in research must be both voluntary and informed. Participants must be provided with complete information to comprehend the character of any proposed research and the implications for participation. 53 Complete information is taken to include the objectives, methodology, risks, and the potential benefits of the research. 54 Only then is the participant considered to be informed, and thereby able to partake in the research.
Detailed information must be communicated to participants to ensure comprehension of the following (among other information about the proposed research): any alternatives to participation; how the study will be monitored; provision of services to participants adversely affected by the research; the contact details of a person to receive complaints; contact information of the researchers; how privacy and confidentiality will be protected; the participant's right to withdraw from further participation at any phase, together with any implications of withdrawal, and whether it will be possible to withdraw data (more on this later); the amounts and sources of funding for the research; financial or other relevant declarations of interests of researchers, sponsors or institutions; any payments to participants; the likelihood and type of dissemination of the research results, including publications; any expected benefits to the broader community; any other relevant information, including research-specific details required under the different chapters of the National Statement. 55
In relation to the participant's right to withdraw from further participation at any phase, reference can be made to Martin Enserink, a participant in an efficacy trial of a candidate COVID-19 vaccine produced by CureVac. 56 Martin was in a dilemma as to whether he could or should withdraw his participation because while the clinical trial was still ongoing, he knew of a proven and available vaccine such as Pfizer and was seriously considering withdrawing from the trial to take the proven vaccine, a reasonable decision considering the seriousness of getting infected with Covid, especially with the emergence of the various variants. However, the written information provided to him did not discuss the options if a volunteer becomes eligible for a proven authorised vaccine, causing uncertainties and confusion for him. Having consulted two scientists who also experienced similar dilemmas earlier, Martin decided to withdraw his participation in the clinical trial. While he was allowed to leave, the lack of information caused him to suffer initial discomfort, inconvenience, and anxiety. Professor of Medicine and Chief Operating Officer of the Desmond Tutu HIV Foundation Dr. Linda-Gail Bekker asserts that participants become eligible for any authorised COVID-19 vaccine at any stage during the trial, they will be encouraged to withdraw from the trial. 57
Also, the participant's consent may need to be renegotiated periodically. For instance, some studies are lengthy, and if there are variations to the terms and conditions they originally agreed to, participants should be informed and be offered the chance to either continue their participation or withdraw from the research. 58
Once a research project has been approved by an ethics committee (which will consider how risks will be managed), the decision regarding whether a potential participant will participate in a trial is theirs alone. Here, the principles of consent, which uphold respect for a person's right to autonomy, self-determination, and bodily integrity, come into play.
However, the reality remains that there are limitations to informed consent. Special considerations must be had regarding the consent to participate in health or medical research by children and people who lack the mental capacity to give consent. In legal terms, they are considered incompetent to give valid consent. Yet, to completely debar their involvement in medical research will impede these groups from benefiting in totality from the achievements of modern medicine. As mentioned, there is no COVID-19 vaccine yet for children under age 16. 59 Studies involving younger children will start soon and multiple companies have started recruiting children as young as age 12 in these trials. In every case, relevant jurisdictional laws will need to be taken into consideration.
The legal concepts of capacity and substitute decision-making should be viewed within a broader context of ethical and respectful research. Older children should be regarded as capable of offering meaningful contributions. Where possible, people who cannot provide consent should be encouraged to express their wishes and opinions and have their views considered with due respect by researchers, legal guardians, and other decision-makers. 60
In relation to HCS, it can be challenging to establish authentic, informed consent. Amid a pandemic, there are concrete reasons to consider making compromises in medical research such as HCS. But it must also be borne in mind that these concessions must not come at the cost of exploitation or endangerment of the research subjects. 61 The question still arises; however, as to whether it is in fact even possible for the participants of a clinical trial to provide consent given the limited knowledge and multiple uncertainties regarding short- and long-term risks to participants from the infection and vaccines whose side effects are currently not wholly understood. The frank disclosure of all risks is essential and ideal. This practice is particularly challenging in an environment of a constantly changing understanding of the novel virus and the various types of risks. For example, there is an indirect risk associated with HCS due to the severe concern of secondary transmission from the participants to vulnerable cohorts, such as their own families and other people they may encounter later. 62
Despite the serious concerns, it can be argued that there is a vital function for HCS to proceed during a crisis such as a pandemic. In a paper, the authors explore the principle of risk parity. 63 The principle proposes the hypothetical that we allow some members of the population, such as health workers, to be exposed to a certain degree of risk to reduce overall harm from the virus. In this case, it is also permissible to expose fully informed volunteers to a similar level of risk in a holy grail study into the deadly novel virus. Suppose these individuals are able and want to help fight against a potent virus by participating in promising research; in this case, there would be solid moral and ethical grounds to receive their gracious help. To refuse participation on these grounds would subject the entire world's population to graver risks. As the authors noted, “There is too much that we do not know about COVID-19. The longer we take to find it out, the more lives will be lost.” 64
As mentioned, HCS has just begun in the U.K. and other countries may want to follow suit. To justify conducting this kind of risky research, the potential benefits must considerably exceed the risks. It is critical for there to be a thorough evaluation by an independent ethics committee, e.g., HREC. The burden will lie on the researchers to justify performing HCS and it is a heavy one. The design must optimise the prospects for the outcomes to have high utility (which is evident in this case), the findings from the study should be widely shared with many (including negative outcomes as well), and there must be a plan for the subjects to obtain long-term care for any adverse outcome that may be related to their participation in CHS. 65 Likewise, it is also an onerous burden for HREC to exercise their final judgment whether to grant ethical approval as this is such a complex matter.
Moreover, in some research, participants are paid for their participation. This is a contentious issue as payment in some situations could be perceived to operate as an inducement or even coercion to the potential participant to be involved in the research. 66 This point also illustrates the limitation of informed consent.
Payment for participation in clinical research trials includes giving participants financial or in-kind support, including remuneration, compensation, reimbursement, and/or incentive for involvement in research. 67 Providing monetary payments can be effective in increasing recruitment and decreasing attrition. 68 Moreover, such practice could increase research subject motivation and satisfaction with the research study. 69
Some see research participants' payments as highly contentious. 70 Not every participant in clinical research gets paid. When payment is made, its amount varies. It may include reimbursement for certain expenses, compensation for time and effort, minimum wage-like remuneration for a set period, or higher than minimum wage remuneration. This may seem like a negative in that it may influence who participates in the study. However, participants in clinical trials admit they do so for the money despite being known as volunteers. 71
The practice of payment for participation in clinical studies may be perceived as controversial. Some argue that offering to pay research participants is a form of coercion or may lead to undue influence, 72 contrary to the requirement for free, informed, and voluntary consent to participation found in all the leading ethical codes and guidelines. In the U.K. HCS, every participant was offered £4,500 (more than A$8,000), which is not modest. During the pandemic, several individuals have lost their jobs leading to dire straits for some. The worry is that the money offered to them may operate as an inducement/undue influence to participate in the research. Undue monetary or in-kind incentives should not be proffered where there is a likelihood or a perception that they may compromise the authentic voluntariness of the consent. Special care needs to be given to specific cohorts whose circumstances may affect their capacity to provide genuine consent—for instance, people in custodial settings or hierarchical organisations.
During such a public crisis, it is imperative to consider whether the recruitment of “cash strapped” participants, such as students, the unemployed, 73 and/or underemployed, are ethically acceptable. The pandemic has indeed aggravated the unemployment situation. While some are eligible for pandemic government relief (such as ‘Jobkeeper’ in Australia), many are financially challenged. Despite vaccine rollouts, the economic recovery is sluggish and uncertain during such unprecedented times.
Naturally, exploitation includes taking unfair advantage of an individual, for instance, an economically or socially vulnerable person. 74 The Tuskegee study offers a good example of this and few would deny it was exploitative. 75 Exploitation may involve coercion where a research subject might be inclined or even keenly consent to an exploitative offer if the unfair offer is superior to their other choices. 76 It is not surprising that economically disadvantaged populations would consider participating in highly paid clinical trials despite the various risks and discomfort. 77 Wertheimer refers to this paradigm as “mutually advantageous exploitation.” 78
Concerning specific segments of society who are vulnerable or perceived to be vulnerable, there is a need for special protection. The NHMRC provides that care should be taken when considering payments for participation in clinical research “to children (under 16 years of age) or their parents, or to adults who lack decision-making capacity or their legal representatives.” 79 In such cases, there is potential for the parent or his/ her legal guardian to unduly influence the young participant and enroll him/ her in the research to get monetary gain. 80 Therefore, the NHMRC provides that payment to these participants in clinical intervention research should be confined to mere reimbursements for only documented expenses; and proposals for payments in other research must be scrutinised. 81 The NHMRC also recommends that special consideration be given to clinical trials involving people affiliated with the body responsible for the research like students or employees, individuals obtaining government support or members of consumer advisory groups to reduce the likelihood of undue influence. 82
While it may seem of concern to make monetary payment to certain populations in clinical research, such as substance abusers, this concern is not considered by the NHMRC as being an unethical practice. The NHMRC provides that assumptions that payments should not be made to individuals with addictions are not substantiated by evidence. Such assumptions may include the worry that these participants will use monetary payments to buy drugs or alcohol. 83 The NHMRC notes that people who use addictive substances should be assumed to have self-determination and autonomy in relation to their participation in research, unless there is evidence to the contrary, and states that reviewers should not be insistent on the use of only vouchers or other non-cash payments for said potential participants. 84 Research suggests that high magnitude and financial remuneration can effectively increase recruitment and reduce attrition of substance abuse in clinical trials; with said participants using their r research payments responsibly. 85 In a similar vein, concerning prisoners, the NHMRC states that their incarceration does not negate their capacity to participate in research or obtain monetary payment for participating. 86
While special consideration needs to be had regarding financial payment for participation in research trials to specific categories of the vulnerable population, it is essential to recognize that payment is not considered unethical by the respective guidelines and codes. Nor does it necessarily negate free and autonomous decision making (i.e., informed consent). On the contrary, it is often considered a fair and reasonable way to recruit individuals into studies that would otherwise not participate. The NHMRC provides that offering payment for participation in cases where the research provides little or no benefit to individuals or where the study needs the participation of target populations that are hard to recruit, payment may be proffered as an incentive to participate, as long sufficient processes are in place to promote genuine consent. 87 This is especially relevant in pandemic studies. Thus, the researchers must present a full justification for, as well as details of, the payment when applying for HREC approval. The NHMRC has made some recommendation in their guidance statements. 88
6.2.3 Regulatory guidance on clinical trials
On 9 April 2020, the Australian Government released the “COVID-19: Guidance on clinical trials for institutions, HRECs, researchers and sponsors” document (Guidance Document), to provide regulatory guidance to industry stakeholders in the context of the COVID-19 pandemic. 89 The Guidance Document outlines fundamental principles including: that the well-being and safety of patients, participants and their families, health care employees, researchers, and other staff involved in patient care and research is of utmost importance. 90 Public health systems must respond to the community's needs, such as those affected by COVID-19. Conducting research related to COVID-19 is a priority; however, the initiation and continuation of ongoing and proposed research may be critical for the well-being of patients, participants, communities, and the research sector. Compliance with regulations, guidelines, codes, policies, and other standards is necessary. Finally, the interpretation of research responsibilities in the context of a pandemic should be informed by flexibility, consultation, and good sense that focuses on the safety and well-being of individuals most at risk in institutions and communities.
Researchers, sponsors, institutions, and HRECs should consult and follow existing safety monitoring and reporting published by NHMRC and the TGA (National Health and Medical Research Council 2016). 91 Any proposed changes to standard practice should be discussed among the relevant parties and authorised by the responsible party.
Any events associated with the attendance at a clinic of a volunteer known or later discovered to be symptomatic must be promptly reported as an adverse event or safety issue, following existing guidance. 92
If a planned amendment of a protocol is likely to impact participants' safety or increase risks, then a review by HREC is required. 93 Institutions should consider identifying an appropriate person, e.g., the HREC Chair, to decide whether a review is necessary before implementing the proposed amendment. Extensive amendments should be submitted and approved by the HREC.
Adopting methods to pre-approve specific categories of amendments is promoted and should be employed conditional on the directions of jurisdictional health departments. 94 Modifications that are eligible for pre-approval would be at the discretion of the institution and/or HREC and might include amendment of a clinical trial such as the following:
adopt virtual visits, telehealth, electronic consent, or conduct tele-trials
change the site to a location outside of a hospital or clinic or to allow a referral to another hospital or clinic
extend time frames for visits, procedures, trial medication delivery, or follow-up to accommodate isolation periods or other disruptions
ensure that returned investigational medical product is destroyed following standard protocols for the destruction of biohazards
any other changes that do not implicate participants' safety or well-being and are intended to safeguard participants' health, researchers and staff, or the community via infection control or reduce the burden of participation for the volunteers. 95
If time does not permit, changes to protocols intended to reduce participants' exposure to infectious agents or modify methodology, procedures, or project activity to lessen the burden on participants do not need to be approved by HRECs before being implemented. 96 For example, amendments that suspend recruitment of participants or modify research locations or staffing and other administrative matters can be implemented as necessary. However, if there is sufficient time for a modification of this type to be reviewed following amendment approval processes, that is desirable.
If changes are made, these should be reported to the sponsor according to standard processes and to the HREC, when that becomes possible, according to standard procedures and following the National Statement. For example, protocol deviations could be reported to HRECs in the usual method or collected and sent in bulk at the end of the crisis. 97 Although deviations must be reported to the trial sponsor, only a sub-set of deviations that significantly impact participants' continued safety or rights or the reliability and rigor of the data generated in the clinical trial must be reported to HREC.
The TGA provides support for monitoring several issues relating to therapeutic goods in response to COVID-19. 98 A clinical trial that aims toward a medical treatment or a vaccine for COVID-19 will be given priority by the TGA.
Finally, HREC members, ethics officers, research governance officers, and executive officers should have contingency planning related to their daily operations and adopt sensible approaches to fulfilling their responsibilities following the National Statement and institutional policy. 99 These approaches should not be excessively rigid or impose burdensome obligations on researchers and their sponsors. HREC members, ethics administrative officers, research governance officers, and executive officers must be cognisant of the guidance document, including updated guidance and the latest advice.
While the Guidance Document is a set of recommendations that is not legally enforceable, it stands for best practice at the government level. It will be reviewed and revised regularly to reflect policy changes, public health advice, and the needs of those managing and participating in clinical research in Australia. The NHMRC, TGA, Departments of Health and CTPRG support institutions, HRECs, researchers, and sponsors to lessen the burden of adhering to regulations and guidelines by adopting creative and streamlined strategies.
7. Conclusion
The COVID-19 pandemic continues; and the vaccines on which the world relies to transport them to safety and normality, do not have a 100% efficacy threshold. Variants to the virus continue to emerge and engage the scientific community in a high-stakes and expensive game of whack-a-mole. The need for urgent and comprehensive data regarding COVID-19 vaccines, specifically from clinical trials, persists. The scientific community has been clear that epidemic and pandemics will occur in the future. Today's research is poised to support the vaccines of tomorrow, as the DNA and RNA research of SARS and MERS support that of COVID-19 today. Such studies are critical not only for science, but also public policy. As Dr. Andrew Ward states: “Chances are, in the next 10 to 50 years, we may have another outbreak like SARS-CoV-2.” 100
It is critical for nations to adopt a robust regulatory framework that ensures adequate ethical protection for participants in studies and clinical trials for the present and could also be used and adapted for future epidemics/pandemics. Some scientists may compromise quality control and rigor in a frantic race to find a cure/ vaccine. However, crises and emergencies are not reasons for lowering the bar of ethical and scientific benchmarks. Ethicists have cautioned researchers not to succumb to bad science; fundamentally because “bad science” or “lazy science” is capable of destroying public trust.
All human research, including involving COVID-19 vaccines amid a pandemic, can commence if new approaches show sufficient scientific promise, research ethics committees are satisfied that the risks have been minimised, benefits outweigh risks, and the research subjects are capable of and provide voluntary informed consent based on being informed all they need to know. Concerning the highly controversial HCS, researchers have a high threshold to justify conducting such studies to the HREC. It is also challenging for HREC to make a final decision on whether to grant ethical approval.
While the analysis of the current Australian regulation on studies and clinical trials indicates that it is commendable, there is no specific reference to HCS. Thus, appropriate regulation of these challenging studies needs to be incorporated into the existing framework such as the Guidance Document. Nevertheless, the overall Australian regulatory framework on studies and clinical trials is a model for other nations to adopt, especially for some developing countries that may not currently have a detailed and stringent regulatory system on studies and clinical trials. All human participants and the public must trust the system, especially studies and clinical trials being conducted in the midst of a severe and profoundly concerning unprecedented crisis.