
Abstract
Mild cognitive impairment (MCI) is considered to be the prodromal stage of Alzheimer's disease. The amygdala, which is considered to be a hub, has been shown to have widespread brain connections with many cortical regions. Longitudinal alterations in the functional connectivity of the amygdala remain unclear in MCI. We hypothesized that the impairment in the amygdala-cortical loop would be more severe in a follow-up MCI group than in a baseline MCI group and that these alterations would be related to the disease processes. To test this hypothesis, we used resting-state functional magnetic resonance imaging to investigate alterations in amygdalar connectivity patterns based on longitudinal data from 13 MCI subjects (8 males and 5 females). Compared to the baseline, decreases in functional connectivity were mainly found located between the amygdala and regions at the conjunction of the temporal-occipital system and the regions included in the default mode network in the follow-up MCI individuals. The alterations in the functional connectivity of the identified regions were validated in an independent dataset. Specifically, reduced amygdalar connectivity was significantly correlated with cognitive abilities. These findings indicate that impairments in the functional connectivity of the amygdala may be potential biomarkers of the progression of MCI.
Introduction
The term mild cognitive impairment (MCI) is used to describe people who have some memory complaints but do not meet the criteria for dementia (Petersen et al., 1999, 2001). In the past two decades, MCI has been considered to represent a state of cognitive function that is intermediate between normal healthy aging and fulfilling the criteria for Alzheimer's disease (AD) (Petersen, 2009; Petersen et al., 1999). Indeed, those with MCI have a significantly greater risk of converting to AD (Albert et al., 2011; Sperling et al., 2011). Considerable amounts of evidence have shown that 10∼15% of MCI patients, particularly amnestic MCI (aMCI) individuals, convert to AD each year (Landau et al., 2010; Petersen, 2009; Pozueta et al., 2011; Rami et al., 2007), and some studies suggest that the percentage is >20% (Fischer et al., 2007; Maioli et al., 2007). Although the definite pathogenesis of MCI is still vague, evidence regarding the pathologic basis of MCI has demonstrated that MCI subjects exhibit characteristics similar to those of AD patients, such as amyloid-β (Aβ) accumulation, neurofibrillary tangles, and neuronal injury (Markesbery et al., 2006; Petersen et al., 2006; Schneider et al., 2009; Sperling et al., 2011; Ward et al., 2012). Based on these similarities, MCI was often considered to be the earliest clinical sign of probable AD (Petersen et al., 2006; Sabbagh et al., 2006). Therefore, longitudinal studies are essential and may help us to understand the dynamic alterations in brain structure and function that occur in MCI (Amlien et al., 2013; Douaud et al., 2013; Li et al., 2011a; Stanga et al., 2012; Villemagne et al., 2013; Wang et al., 2012).
As a site of Aβ deposition in MCI and early AD, the medial temporal lobe is vulnerable to early involvement (Arnold et al., 1991; Braak and Braak, 1991; Furukawa et al., 2010). The amygdala is an important component of the medial temporal lobe and plays an important role in the relationship between emotion and cognition (Pessoa, 2008; Pessoa and Adolphs, 2010). Moreover, the amygdala exhibits widespread connectivity with cortical regions, such as the parietal lobe, orbitofrontal cortex, ventromedial prefrontal cortex, middle temporal gyrus (MTG), inferior temporal gyrus, cingulate, thalamus, insula, and hippocampus (Klavir et al., 2013; Pessoa, 2008; Pessoa and Adolphs, 2010; Roy et al., 2009; Xie et al., 2012; Yao et al., 2013). The amygdala is also thought to be an important connection hub in the brain network (Pessoa, 2008; Tomasi and Volkow, 2011). Previous longitudinal magnetic resonance imaging (MRI) studies have demonstrated that the amygdala atrophies at a rate of 3.79% per year in AD (Fjell et al., 2009) and that reductions in the volume of the amygdala are correlated with decreases in cognitive ability [as measured by the mini-mental state examination (MMSE)] in AD (Poulin et al., 2011; Roh et al., 2011). Impaired amygdalar functional connectivity has been associated with depressive symptoms and memory impairments in aMCI subjects (Xie et al., 2012), and altered functional connectivities between the amygdala and the bilateral posterior cingulate cortex, left dorsolateral prefrontal cortex, and MTG are related to the interactions between mood symptoms and memory performance (Xie et al., 2012). Importantly, decreases in the functional connectivities between the amygdala and the regions involved in the default mode, context conditioning, and extinction are correlated with reduced MMSE scores, which indicate that cognitive functional impairments are related to alterations in functional connectivity patterns in MCI/AD (Yao et al., 2013). However, it is currently unknown whether the functional connectivity patterns of the amygdala are impaired in follow-up MCI subjects.
The first aim of the current study was to test whether the amygdala-cortical circuit is impaired in follow-up MCI subjects. For this purpose, 13 MCI subjects (8 males and 5 females) were recruited, and resting state functional MRI (fMRI) data were acquired during an initial visit and a visit that occurred 1 year later (mean time 13.0±2.2 months). Alterations in the functional connectivity patterns of the amygdala were investigated using paired two-sample, two-sided t-tests. The second aim was to evaluate whether alterations in amygdalar connectivity were related to changes in cognitive ability in the follow-up MCI subjects. Pearson's correlation analyses were performed to assess the relationships between changes in the functional connectivity strengths of the identified regions with the bilateral amygdala and clinical variables [i.e., MMSE, Montreal cognitive assessment (MoCA), auditory verbal learning test (AVLT)-immediate/delayed recall scores, and the activities of daily living (ADL) measure].
Materials and Methods
Data from some of the subjects examined in the present study have been reported in our previous studies of regional homogeneity (Zhang et al., 2012), amygdalar connectivity (Yao et al., 2013), thalamic connectivity (Zhou et al., 2013), and marginal division connectivity (Zhang et al., 2014) during resting states. All of the subjects met identical methodological stringency criteria, and comprehensive clinical details can be found in our prior work (Yao et al., 2013; Zhang et al., 2012, 2014; Zhou et al., 2013). Notably, all of the analyses attempted in this study are fully orthogonal to any previously published effects that are based on the AD and MCI replication samples and thus ensure the independence of the reported effects.
To maintain the scientific integrity of the present study, we will provide a short description of the data collection and data preprocessing steps.
Subjects and data acquisition
The PLA dataset
All of the participants were recruited by an advertizement (
Demographic, Clinical, and Neuropsychological Data of the MCI Group at Baseline and Follow-Up
Paired t-test between the first and second visits.
One MCI subject converted from MCI to AD during the 13-month period and was diagnosed with AD with a CDR=1.0 in the follow-up. The MCI subjects were aMCI subjects.
Only 12 subjects underwent the MMSE evaluation twice.
AD, Alzheimer's disease; ADL, activity of daily living; ADNI, Alzheimer's Disease Neuroimaging Initiative; aMCI, amnestic-type mild cognitive impairment; AVLT, auditory verbal learning test; MMSE, mini-mental state examination; MoCA, Montreal cognitive assessment.
The data scans were performed at the Chinese PLA General Hospital, Beijing, China, with a 3.0-T GE MR system using a standard head coil. Resting-state fMRI data were acquired using an echo planar imaging sequence with a repetition time (TR)=2000 ms, echo time (TE)=30 ms, flip angle=90°, matrix=64×64, field of view=220×220 mm2, slice thickness=3 mm, and slice gap=1 mm. Each brain volume was comprised of 30 axial slices, and each functional run contained 200 volumes.
The validation dataset
The dataset used to validate the results of the current article were obtained from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). Because we only sought to validate the abnormal pattern of the amygdala within our own data and also to exclude the variance due to the use of different centers and MRI scanners, we selected data from only one center (S002 in ADNI); these data included 17 MCI subjects (7 early MCI and 10 late MCI), and 12 of these subjects exhibited similar MMSE scores after a mean follow-up time of 9.0±4.2 months. The demographic and neuropsychological details of the MCI subjects are shown in Table 1.
The included resting fMRI dataset was acquired on 3.0 T Philips scanners (varied models/systems) at one site (S002). The imaging in-plane resolution ranged from 2.29 to 3.31 mm, and the slice thickness was 3.31 mm. The TE for all subjects was 30 ms, and the TR ranged from 2250 to 3001 ms. At least 140 volumes were acquired from each subject.
Data preprocessing and definition of the amygdala
The data were preprocessed following the steps explicated in our previously published work using in-house software (
Functional connectivity and statistical analysis of the bilateral amygdala
As in our previous study (Yao et al., 2013), functional connectivity analyses were performed separately for the left and right amygdala. For each seed region, a voxel-wise functional connectivity analysis was performed separately for each ROI (Yao et al., 2013). The mean time series of all of the voxels within the ROI were used as the seed reference time series, and the Pearson's correlation coefficients between the average time series for each seed and each voxel in the brain were computed as indices of functional connectivity strength. For further statistical analysis, the correlation coefficients were transformed into z-values using the Fisher r-to-z transformation to improve the normality of the correlation coefficients. Thus, maps that represented the functional connectivity strengths of each seed region (in terms of the z-values for each subject) were obtained.
Within each group, the individual z-values were entered into a one-sample t-test in a voxel-wise manner to determine the brain regions that exhibited significant functional connectivity with the left amygdala. A combined threshold for the contrast maps was set using clusters with a minimum volume of 50 voxels with uncorrected individual voxel heights of p<0.05. We chose a relatively stringent threshold as the p-value due to the null hypothesis of a correlation coefficient of zero and the relatively large normal control sample size. We then obtained significant connectivity maps of the left amygdala for each group. These same steps were performed for the right amygdala.
A two-tailed paired t-test was performed between the follow-up and baseline data to identify and abnormality map using p<0.01 [T=2.39, df=(1, 24)] for each voxel and a cluster size of at least 100 voxels, which resulted in a corrected threshold of p alpha<0.01 as determined by a Monte Carlo simulation using the AlphaSim method (the parameters of this simulation were as follows: full width half maximum (FWHM)=6 mm, and the significant connectivity map of the amygdala within each group was used as a mask).
Subsequently, the regions that exhibited significant differences were extracted as regions of interest, and the mean z-values of the MCI subjects were used to evaluate the strengths of the functional connectivities. Statistical comparisons of the mean z-values between the two groups were performed using two-tailed paired t-tests at a threshold of p<0.05 (false discovery rate corrected by the number of identified regions). These same steps were performed for the right amygdala. The altered connectivity patterns of the identified regions in the cross-validation dataset were also examined.
Relationships between functional connectivity and the clinical variables
In the PLA dataset, correlation analyses of the alterations in functional connectivity strength (z-values) and the changes in the clinical variables (MMSE, ADL, MoCA, and AVLT-immediate/delayed recall scores) were performed to investigate whether alterations in functional connectivity varied with disease progression in MCI individuals at the statistical significance level of p<0.05 (uncorrected). This correlation analysis between the altered functional connectivity and the altered MMSE scores was also performed on the ADNI dataset.
Results
Demographic information and neuropsychological data
For the PLA dataset, the included 13 (5 females) MCI subjects (74.5±8.7 years of age) received neuropsychological tests and data scanning when they returned for their second examination 13.0±2.2 months after their baseline scans. The MoCA scores had significantly decreased over time (baseline 23.7±2.5 vs. follow-up 21.7±4.7, paired t-test T=2.36, p=0.04). Detailed demographic information and neuropsychological data are shown in Table 1. No significant differences were found in the MMSE (p=0.10), AVLT-immediate recall ability (p=0.24), delay recall (p=0.77) ability, or ADL (p=0.22) scores between the baseline and follow-up (Table 1). However, there was a tendency toward lower scores at the follow-up examination that was indicative of declining cognitive function at the follow-up among the MCI individuals.
For the selected ADNI validation dataset, 17 MCI subjects (9 females; 7 early MCI, 10 late MCI) were included, and 12 of these subjects had MMSE scores for both visits. These scores were not significantly different between the two test times (Table 1).
Alterations in the patterns at the follow-up MCI
First, a two-tailed paired t-test was used to determine the regions in which the functional connectivity was significantly different between the follow-up and baseline in the MCI individuals. Compared to the MCI subjects at baseline, the decreased functional connectivities with the left amygdala were found for several regions, including the bilateral MTG/middle occipital gyrus (MTG/MOG, BA 19/39), the left middle frontal gyrus/anterior cingulate cortex (MFG/ACC, BA 11/25), and the region of the conjunction of the left cuneus/posterior cingulate cortex/precuneus (Cun/PCC/Pcu, BA 23/31) (Figs. 1 and 2 and Table 2).
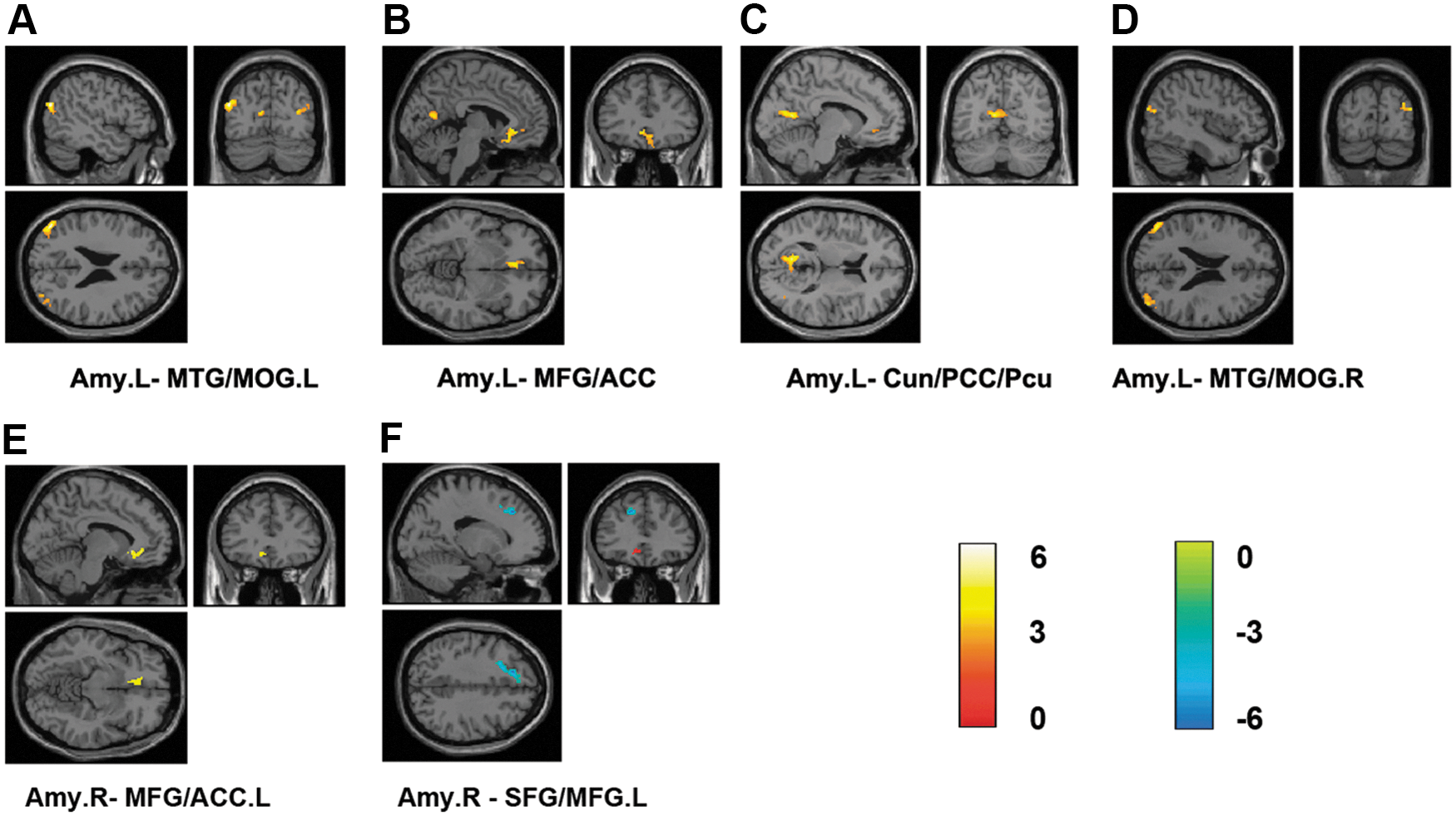
Brain areas exhibiting significant differences in the functional connectivity of the amygdala in the follow-up MCI group compared with the baseline MCI group (p<0.01, 100 voxels, AlphaSim corrected). The strength of the functional connectivity from high to low is indicated as red to blue.
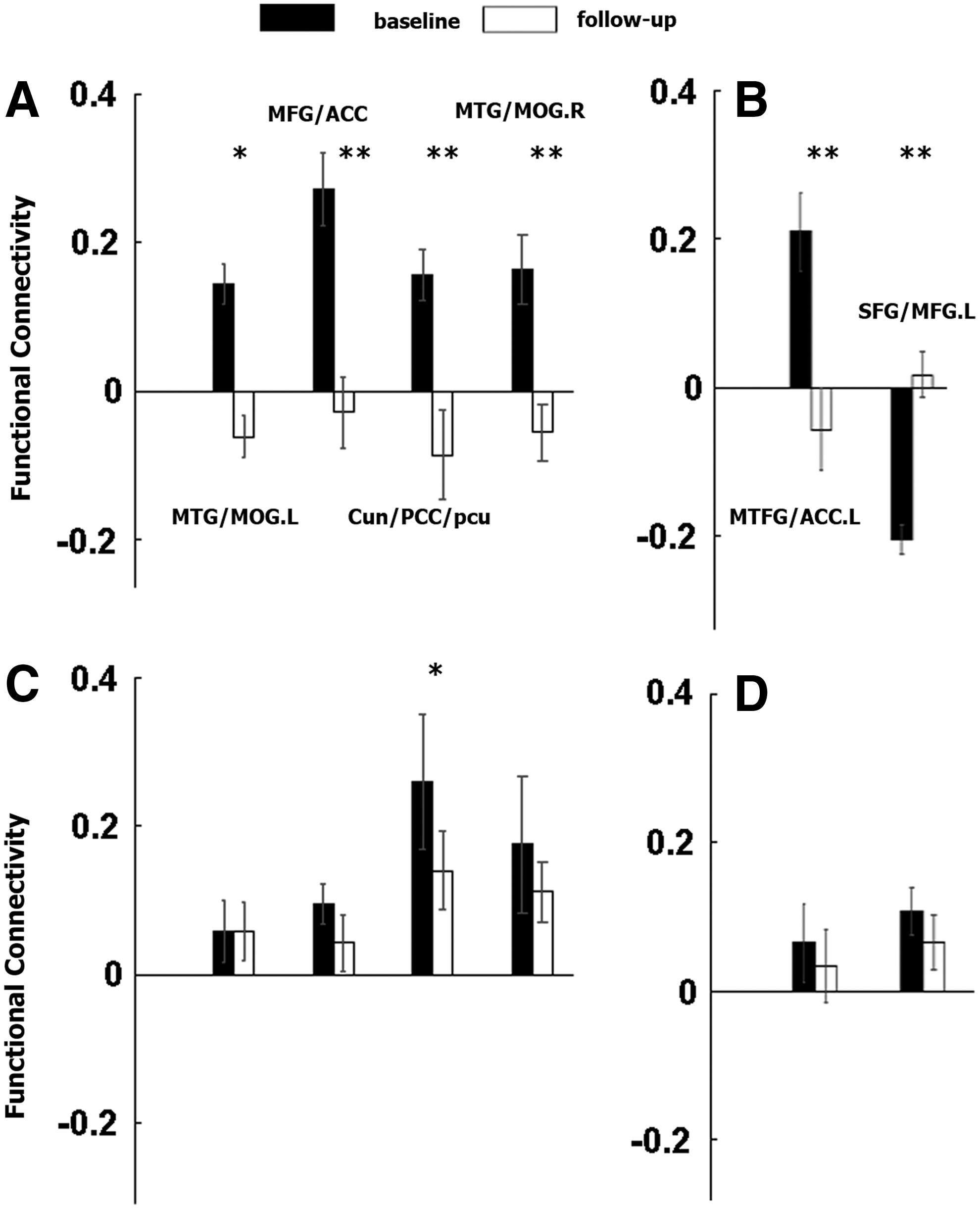
Mean functional connectivity strengths in the identified regions of the follow-up MCI group compared with those of the baseline MCI group (p<0.05, false discovery rate corrected).
Altered Functional Connectivity Using the Amygdala as ROI in the Follow-Up MCI Subjects Compared with Baseline (Cluster Size >100 Voxels p<0.01)
ACC, anterior cingulate cortex; L, left; MFG, middle frontal gyrus; MOG, middle occipital gyrus; MTG, middle temporal gyrus; PCC, posterior cingulate cortex; R, right; ROI, region of interest; SFG, superior frontal gyrus.
For the right amygdala, the follow-up of the MCI subjects revealed that compared to baseline, a decreased functional connectivity was found in the region of the conjunction of the left MFG/ACC (BA 11/25/32), and an increased functional connectivity was found in the region of the conjunction of the left superior frontal gyrus (SFG)/MFG (BA 6/32) as shown in Figures 1 and 2 and Table 2.
For the ADNI dataset, the follow-up MCI subjects also exhibited decreased functional connectivities in the identified brain regions (Fig. 2C, D).
Relationships between functional connectivity and the clinical variables
For the PLA dataset, the reductions in MMSE scores were significantly positively correlated with the strengths of the decreases in functional connectivity between the left amygdala and the MFC/ACC (R=0.753, p=0.003) (Fig. 3A). Changes in the MoCA scores were also significantly positively correlated with changes in the strength of the functional connectivity between the left amygdala and the left MTG/MOG (R=0.571, p=0.042) (Fig. 3B) and the left amygdala and the MFC/ACC (R=0.637, p=0.019) (Fig. 3C). Reduced AVLT-delay recall ability was significantly correlated with decreased functional connectivities between the left amygdala and the bilateral MTG/MOG (R=0.647, p=0.017; R=0.576, p=0.039) (Fig. 3D, F) and between the left amygdala and the MFC/ACC (R=0.572, p=0.041) (Fig. 3E). There were no significant correlations between changes in the other cognitive scores and impaired functional connectivity.
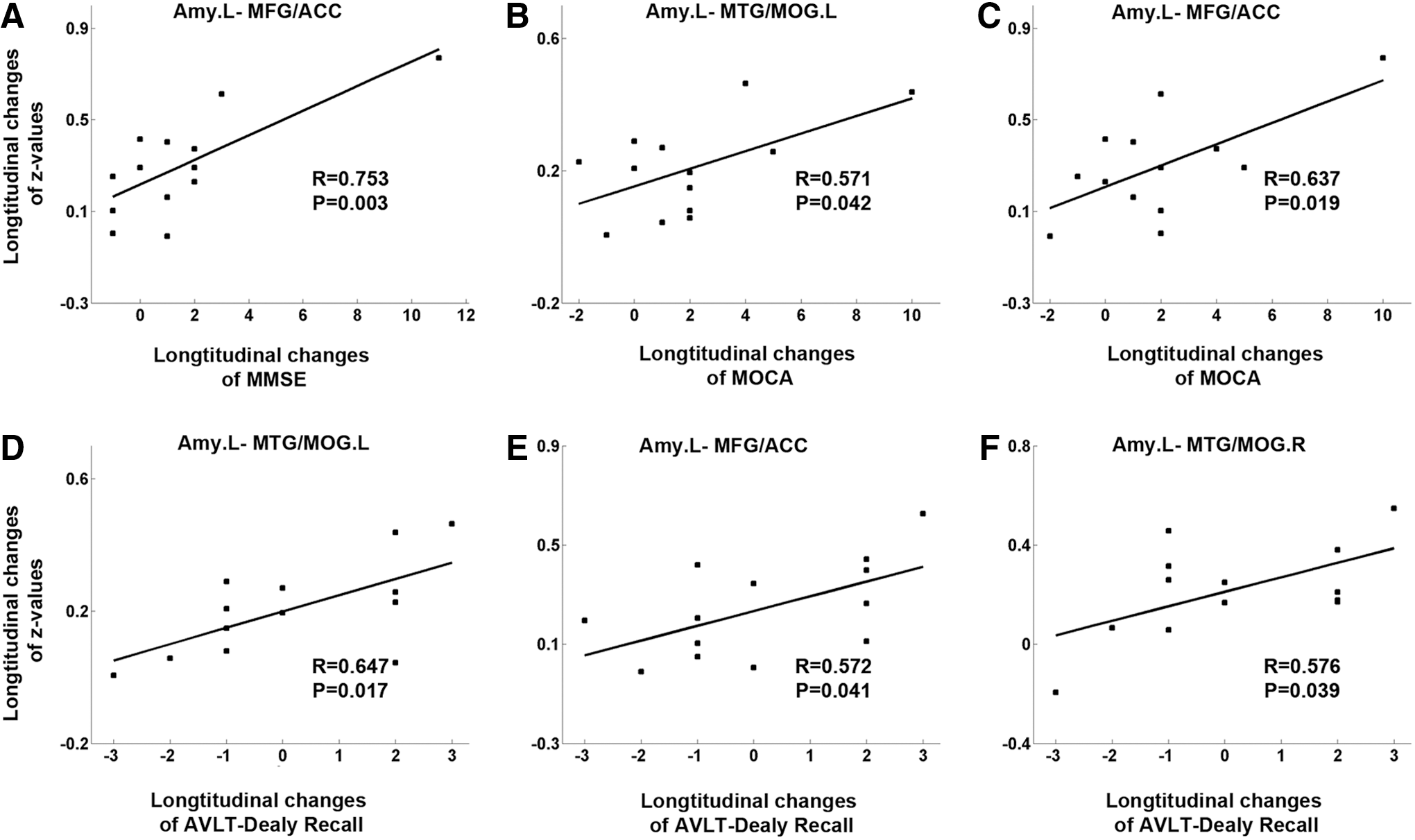
Relationships between the changes in cognitive scores and alterations in functional connectivity. Longitudinal changes in MMSE scores were positively correlated with longitudinal changes in the functional connectivity between the left amygdala and the MFG/ACC
We did not find any significant correlations between the changes in functional connectivities and changes in MMSE scores in the ADNI dataset, which may be due to the fact that the duration of the illness was relatively short (the mean duration was 9.0 months between the two test times) and that the sample was also small.
Discussion
In the current study, we investigated the altered functional connectivity patterns of the amygdala in follow-up MCI subjects for the first time. Specifically, decreases in the functional connectivities of the bilateral amygdala were found in the region of the conjunction of the temporal and occipital systems and the regions of the default mode network (Fig. 1). This pattern of results was also validated in an additional independent dataset.
Longitudinal functional connectivity patterns of the amygdala in MCI
Interestingly, decreased functional connectivity between the amygdala and the region of the conjunction of the MTG/MOG was found in the follow-up MCI subjects (Figs. 1 and 2 and Table 2). The MTG is known to be involved in several cognitive processes, such as language and semantic memory (Binder et al., 2009; Chao et al., 1999; Tranel et al., 1997), and it has been delineated as one of the core regions for the cross-modal integration of a variety of emotions (Pourtois et al., 2005). Many previous studies have demonstrated that the MTG exhibits significant functional connectivity with the amygdala (Jansma et al., 2013; Roy et al., 2009; Xie et al., 2012). Semantic memory impairments specifically occur in patients with amnesic MCI (Adlam et al., 2006), which can be considered as a biomarker of aMCI (Almkvist and Winblad, 1999; Gardini et al., 2013). Therefore, we speculate that the alteration of the functional connectivity between the MTG and the amygdala might be related to the reduced semantic memory and emotion processing abilities of MCI subjects. This speculation was confirmed by the observation that the decreased functional connectivity between the MTG/MOG and the left amygdala was significantly and positively correlated with decreases in cognitive ability [as measured with the MoCA, which is a neuropsychological test and a simple cognitive screening tool for detecting MCI with high specificity and sensitivity (Hoops et al., 2009; Nasreddine et al., 2005)] in follow-up MCI subjects (Fig. 3B). Additionally, our findings also demonstrated that the reductions in AVLT-delay recall scores were significantly correlated with decreases in the functional connectivity between the amygdala and the bilateral MTG/MOG (Fig. 3D, F), which indicates that the decreases in memory abilities were related to amygdala connectivity. As suggested by Xie et al. (2012), this amygdalar functional connectivity might reflect impairments of complex functions, such as emotion and cognition, in the MCI individuals. Therefore, disrupted functional connectivity of the amygdala might be useful as a predictive feature of MCI.
Not surprisingly, we also found significantly decreased functional connectivity between the left amygdala and the region of the conjunction of the MFG/ACC and Cun/PCC/PCu (Figs. 1 and 2). Interestingly, based on previous studies (Buckner, 2012; Buckner et al., 2008; Greicius et al., 2003, 2004; He et al., 2013; Liu et al., 2013; Song et al., 2013), the aforementioned regions are the key regions of the default mode network. The default mode network is engaged when individuals are not focused on the outside world, and it is involved in many neurophysiological processes of cognitive and emotional function, such as episodic memory and emotional regulation (Buckner et al., 2008; Greicius et al., 2004; Li et al., 2011b; Raichle et al., 2001). The PCC/Pcu is located in the posterior midline of brain and is a central hub that plays a significant role in the default mode network (Buckner et al., 2009). Furthermore, the regions of the default mode network are vulnerable to early Aβ deposition in MCI/AD (Buckner et al., 2008, 2009; Mormino et al., 2011; Sperling et al., 2009). A considerable number of studies have demonstrated that connectivity related to the default mode network is disrupted in AD/MCI, and the activity in the default mode network may ultimately prove to be a sensitive and specific biomarker of AD (Greicius et al., 2004; He et al., 2013; Koch et al., 2012; Liu et al., 2013; Qi et al., 2010; Song et al., 2013). More importantly, the observed reductions in cognitive abilities (e.g., reduced MMSE and MoCA scores) were significantly correlated with decreased functional connectivity between the left amygdala and the MFG/ACC (Fig. 3A, C), which indicates that progressive disruption of the functional connectivity between the amygdala and the default mode network might play a role in the progression of MCI.
Compared to the baseline results of the MCI sample, increased functional connectivity between the amygdala and the SFG/MFG (BA 6/32) was found in the follow-up MCI results. The SFG and MFG are involved in many high cognitive functions, such as motor tasks, execution within working memory, and attention (du Boisgueheneuc et al., 2006; Fox et al., 2006; Leung et al., 2002; Martino et al., 2011; Owen et al., 1998). Similar to many previous studies that have found increased functional connectivities between subcortical regions in MCI/AD (Bai et al., 2009; Wang et al., 2007, 2011, 2012; Zhou et al., 2013), the increased functional connectivity between the amygdala and the frontal cortical regions might reflect a compensatory mechanism for losses in cognitive functionality in other brain regions, particularly the loss of episodic memory in MCI subjects. This type of compensatory loop might be built in the early stages of MCI prior to the emergence of clinical symptoms; however, studies with large subject samples and long-term follow-ups are needed to confirm this speculation.
Methodological issues and further discussion
Our preliminary study is not without limitations. Our major finding was that changes in functional connectivity were correlated with reductions in cognitive measures (i.e., MMSE, MoCA, and AVLT-delay recall scores) among the MCI subjects. To validate the altered functional connectivity patterns of the amygdala in the MCI subjects, another independent dataset from the ADNI was included, and we found that the functional connectivity of the bilateral amygdala exhibited similar reductions in this independent dataset (Fig. 2C, D and Supplementary Fig. S1). These two datasets came from different population, had different durations of illness (13 months vs. 9 months) and were scanned with different imaging parameters (e.g., TR, time points, etc.). Moreover, the main purpose of the present study was to investigate the alteration in amygdalar connectivity in the follow-up MCI subjects; thus, there was no control group to support the findings. Following the idea of Li et al. (2002), to evaluate whether other regions also exhibited reduced connectivity patterns in the same group of subjects, we selected the bilateral primary visual cortex as an ROI and found that the follow-up subjects maintained the functional connectivity strengths between the amygdala and the primary visual cortex (two-tailed paired t-test, p=0.70 and 0.83 for the connectivities between the bilateral primary visual cortex and amygdala and p=0.29 and 0.40 for the right amygdala in the PLA dataset). These findings suggest that we should pay more attention to the role of amygdalar connectivity in the early stages of AD (Poulin et al., 2011).
Moreover, as discussed in our previous study (Yao et al., 2013), the specific individual subdivisions differentially contribute to the connections between the amygdala and cortical and subcortical brain regions (Gopal et al., 2013; Mishra et al., 2014; Roy et al., 2009; Saygin et al., 2011). In this study, the amygdala was considered as a singular structure, which likely masked the independent functions and patterns of connectivity of the individual subdivisions. The functional connectivity patterns of the subdivisions of the amygdala should be evaluated in the future. The gray matter volume has been found to be atrophied (Basso et al., 2006; Poulin et al., 2011; Whitwell et al., 2007), and the connectivity patterns have been found to be disrupted (Xie et al., 2012; Yao et al., 2013), in the amygdala of AD/MCI subjects. These impairments of the amygdala may be biomarkers for the diagnosis of MCI. However, it should be noted that we could not completely confirm this conjecture based on our longitudinal evaluation of this small sample over only a 1-year period; however, reductions in cognitive abilities were correlated with decreased functional connectivity. Future studies with larger samples and long-term longitudinal data are potentially important for MCI subjects.
Conclusion
In summary, using resting-state functional connectivity analysis, we were able to demonstrate an impaired amygdalar connectivity network in follow-up MCI subjects, and it is conceivable that the regions that exhibited impaired connectivity with the amygdala in follow-up MCI subjects are the same regions that have been reported to be involved in early AD neuropathology (Buckner et al., 2009; Jack et al., 2011, 2012; Liu et al., 2013; Sperling et al., 2011). Additionally, distinct areas of the amygdalar network were associated with cognitive abilities in the follow-up MCI subjects. To the best of our knowledge, this is the first demonstration that the amygdalar network is linked to cognitive dysfunction (as measured with the MMSE, MoCA, and AVLT-delay/immediate recall test) in follow-up MCI subjects. Similar reductions in amygdalar connectivity in the same identified brain regions were found in an independent dataset, which provides further evidence that amygdalar connectivity should be added to the list of potential markers of preclinical MCI. Our functional connectivity analyses provided new insights for the investigation of the complex factors that are associated with cognitive decline in MCI individuals.
Footnotes
Acknowledgments
This research was partially supported by the Natural Science Foundation of China (No. 60831004), the CASIA Innovation Fund for Young Scientists via the Lu-Jia-Xi Award, the Specific Healthcare Research Projects (13BJZ50), the Clinical Sciences Fund of the Chinese PLA General Hospital (2013FC-TSYS-1006), and the Science Technological Innovation Nursery Fund of the Chinese PLA General Hospital (13KMM19). We appreciate the generous assistance of Drs. Hengge Xie and Wei Wang with the data acquisition.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.