
Abstract
Although there are many studies of people with complete or partial hypogenesis of the corpus callosum (CC), little is understood about the hypoplastic CC in which all structures are present but thinned. Spina bifida myelomeningocele (SBM) is a model organism for such studies because many have either a hypogenetic or hypoplastic CC. We used diffusion tensor tractography (DTT) to evaluate the hypoplastic CC in SBM and its relation to interhemispheric functions and intelligence quotient (IQ). Participants were individuals with SBM and an intact or hypoplastic CC (n=28), who were compared to a typically developing comparison group (n=32). Total and regional DTT volume and integrity measures (fractional anisotropy, axial diffusivity, and radial diffusivity) of the CC were related to measures of intelligence (IQ), bimanual motor functioning, and dichotic auditory performance. As predicted, DTT showed variations in volume and integrity that were maximized in the entire CC and the posterior CC. IQ correlated with entire CC volume, anterior and posterior regional CC volumes, and also with measures of integrity. Bimanual motor functioning correlated with the anterior and posterior volumes of the CC but not with any integrity measures. Axial diffusivity in the posterior CC was negatively correlated with right ear dichotic listening performance. The hypoplastic CC is not macrostructurally or microstructurally intact in SBM, even when it appears radiologically intact. Both volume and integrity of the posterior regions were related to reductions in IQ and to interhemispheric processing. These findings may transfer to other disorders characterized by a hypoplastic CC.
Introduction
There are many studies of interhemispheric transfer in people with complete and partial development of the corpus callosum (CC), or hypogenesis. However, little is known about neurobehavioral development in people with a CC that is characterized primarily by thinning in which all the structures of the CC can be visualized, or hypoplasia. One disorder of development characterized by both hypogenesis and hypoplasia is spina bifida myelomeningocele (SBM), the most prevalent nonlethal birth defect affecting the central nervous system (Centers for Disease Control and Prevention, 2009). SBM is identified at birth by a posterior midline mass that often contains abnormal nerves and protruding spinal cord, along with meninges and cerebral spinal fluid (Reigel and Rotenstein, 1994).
Because SBM is a disruption of neuroembryogensis, regional maldevelopment of the brain affects the brainstem, cerebellum, and CC. The Chiari II malformation, virtually ubiquitous in SBM, is characterized by a herniation of the brainstem from the posterior fossa into the cervical spinal canal (Barkovich, 2005); the result is a mechanical blockage of the flow of cerebrospinal fluid (CSF) out of the skull that results in hydrocephalus in about 80% to 90% of children with SBM (Reigel and Rotenstein, 1994). CC anomalies of various forms occur in virtually all people with SBM (Hannay et al., 2009).
The CC and spina bifida
The prototype for understanding the effects of damage to the CC has generally been research on epilepsy patients who received a corpus callosotomy to treat intractable seizures (Jenssen et al., 2006; Lassonde and Sauerwein, 1997) and the small number of individuals born with congenital absence of the CC as a result of heterogeneous etiologies (Lassonde and Jeeves, 1994). Important sources of information about CC function, and one not confounded by a history of epilepsy or unknown etiology, are conditions in which a large number of individuals have congenital disorders of the CC that involve both congenital processes like agenesis/hypogenesis and secondary acquired destructive processes, like hypoplasia. Callosal hypogenesis and hypoplasia occur in more than half of children with SBM, while hypoplasia without hypogenesis occurs in 44% (Fletcher et al., 2005). In callosal hypogenesis, the rostrum, splenium, and/or posterior body are typically missing, indicating a primary neural insult originating from a disruption of neuroembryogenesis; in hypoplasia, the entire CC is thinned or earlier developed structures, like the body, are missing, presumptively as a result of hydrocephalus (Barkovich, 2005). In SBM, it is possible to differentiate between CC hypogenesis and CC hypoplasia.
Measurement of the structure of the CC in spina bifida
Despite its potential as a model of CC abnormalities, SBM has generated few studies specifically assessing the CC structure and function. Some studies have used morphometric MRI to obtain a cross-sectional area of the CC in SBM. For example, Fletcher and colleagues (1992, 1996) found that area measurements of the CC were significantly smaller in SBM compared with a typically developing (TD) group. In an application of diffusion tensor imaging (DTI), Hasan and colleagues (2008) found reduced fractional anisotropy (FA) in the CC in a group of 29 children with SBM relative to a TD comparison group. Herweh and colleagues (2009) reported that the overall area and FA of the CC was significantly reduced relative to controls, and, further, that CC cross-sectional area and CC FA were highly correlated. Since axonal membranes contribute the most to the measurement of FA (Beaulieu, 2002), Herweh concluded that reduced area and FA indicate a reduced number of axons traveling through the CCs of the people with SBM.
Castillo and colleagues (2009) used both DTI and magnetoencephalography to study structural integrity and neurophysiological patterns of the CC, finding an atypical pattern of brain oscillations in children with SBM as compared to controls, mainly in the posterior and temporal regions connected by the splenium. This atypical activity correlated with reduced CC area in SBM based on DTI assessment. These findings suggest that the structurally abnormal CC in SBM, including both hypogenetic and hypoplastic patients, may affect interhemispheric coordination and integration of information.
CC structure-function relations in spina bifida
A few studies have examined CC structure-function relations in SBM and early hydrocephalus. Fletcher and colleagues (1992, 1996) reported that an area measure of the CC was correlated with intelligence quotient (IQ), nonverbal spatial skills, and fine motor dexterity, but less correlated with measures of verbal skills and executive functions. Klaas and colleagues (1999) investigated interhemispheric transfer of visual, tactile, and auditory information in children with SBM and hydrocephalus with hypogenesis and/or hypoplasia of the CC, finding left visual field superiority for complex forms, which suggested disrupted transfer of right visual field information across the CC from the left hemisphere. Hannay and colleagues (2008) reported that TD children demonstrated the expected right ear advantage (REA) during dichotic stimulation, but that auditory interhemispheric transfer depended on handedness and the status of the splenium of the CC in SBM; right-handed children with hypogenesis of the splenium showed a nonsignificant left ear advantage while right-handed children with a hypoplastic CC had a significant REA that was not significantly different from the REA of the TD sample. In contrast, children with SBM who were nonright-handed and had hypogenesis of the splenium did not show REA.
Rationale for the present study
No studies have related quantitative CC measures to interhemispheric processing in individuals with SBM. Prior studies involving area measurements of the CC have shown only small reductions in the area of the CC; area measurements may be limited in their assessment of the integrity of the CC. In particular, area measurements in the SBM population have not addressed the specific regions of the CC that may be impaired, and do not provide regional subvolumes. There are no studies specifically addressing the hypolastic CC, which in radiological reviews is often viewed as “grossly intact” (Miller et al., 2008).
We used diffusion tensor tractography (DTT) to evaluate the volume and integrity of the hypoplastic CC in SBM and its relation to neurobehavioral functions, including intelligence (as a general marker of neurobehavioral outcomes), and interhemispheric transfer and integration. The first objective was to use DTT to assess the macrostructure, microstructure, integrity, and connectivity of the fiber tracts of the hypoplastic CC in SBM. For volume, we hypothesized that the entire CC volume of the patients with SBM would be significantly reduced when compared with a TD comparison group. Regionally, the posterior segments (i.e., posterior midbody, isthmus, and splenium) of the CC should be more altered due to SBM pathology than the anterior CC. For integrity, we hypothesized that the group with SBM would show reduced FA, mostly in the posterior CC, when compared with TD participants. In addition, we hypothesized that the group with SBM would have increased axial and radial diffusivity values compared with their TD peers in the entire CC and in the posterior segments of the CC.
The second objective was to relate structure and function. Following Fletcher and colleagues (1992, 1996), we expected that reductions in volume measurements of the CC would be significantly and inversely correlated with IQ scores. We had no specific hypotheses about correlations with integrity measures. Following Fletcher and colleagues (1996) and Johansen-Berg and colleagues (2007), we hypothesized that a bimanual task assessing fine motor dexterity would significantly correlate with the entire CC volume and with the body of the CC. The anterior body of the CC has projections to the motor cortex, so we hypothesized that performance on a bimanual dexterity task would significantly correlate with DTT assessments of the body of the CC. Previous research utilizing DTI found significant correlations between percentage of correct reports for the right ear (REA) and area measures of the entire CC, the isthmus, and the body of the CC (Westerhausen et al., 2006). Although the study by Westerhausen and colleagues (2006) utilized normal adults, we used their results as a guide and hypothesized that the performance on DL by the group with SBM would significantly and inversely correlate with the entire CC volume, specifically in the posterior CC, including the posterior body and isthmus of the CC. In addition, we hypothesized that integrity measures of the posterior CC, especially the body and isthmus of the CC, would significantly correlate with DL performance.
Materials and Methods
Participants
The study was approved by the Institutional Review Boards at the University of Houston and the University of Texas Health Science Center at Houston. All participants 13 years of age and older provided written informed consent. Children under 13, gave assent while their parents (or guardians) also provided written informed consent. The sample consisted of 28 children and adults with SBM and 32 TD participants between the ages of 8 and 36 years. Only participants with SBM and a fully intact CC, hypoplastic CC, or intact/hypoplastic CC with a missing rostrum were used for the study. Participants with SBM and evidence of callosal hypogenesis, especially of the posterior body or splenium, were excluded because the quantitative measurements used cannot be applied to a missing structure. A missing rostrum was not exclusionary provided the rest of the genu was intact; the rostrum is a small structure that is difficult to reliably visualize and measure (Barkovich, 2005), and segmentation schemes for the CC have often not attempted to separate the rostrum from the rest of the genu (e.g., Clarke and Zaidel, 1994; Hofer and Frahm, 2006).
Participants with SBM were recruited through two primary sites: The Spina Bifida Clinic at Texas Children's Hospital in Houston, Texas and the Shriner's Hospital for Children in Houston, Texas. Exclusion criteria for the participants of this study included the following: (1) a diagnosis of spina bifida other than SBM, (2) unrelated neurological disorder, (3) severe psychiatric disorder (e.g., autism, psychosis), (4) uncontrolled seizure disorder, (5) inability to control upper limbs, (6) serious hearing loss, (7) hypogenesis of a portion or all of the CC other than the rostrum, and (8) age range of 8 to 36 years. Participants with SBM had evidence of a Chiari II malformation and/or a myelomeningocele at birth. These determinations were made by review of medical records and clinical coding of MRI scans performed by board certified radiologists involved in the ongoing research study (Fletcher et al., 2005).
Of 116 available participants with SBM, 31 (27%) had CCs that could be fully tracked using DTT. Of these, three were outside the targeted age range, leaving a total of 28. A comparison group of TD individuals (n=32) comparable in age was recruited as part of the overall study largely through local advertising. The TD group had no evidence of neurodevelopmental disorder or brain injury, or other exclusionary criteria.
Demographic comparisons and clinical markers
Table 1 shows that SBM and TD groups were comparable in age, t (49.9)=0.96, p=0.34), gender [χ 2 (1, N=60)=0.35, p=0.55], and ethnicity. Ethnicity was grouped into Hispanic and non-Hispanic groups for a chi-square analysis due to the small number of African Americans, Asians, and other ethnicities. Results revealed no significant association of ethnicity and group, χ 2 (1, N=60)=1.07, p=0.30. The TD group had higher SES than the SBM group, t (58)=2.88, p=0.006. Handedness tended to be associated with group, χ 2 (1, N=60)=3.601, p=0.06, with more people with SBM showing evidence of nonright-handedness.
Demographic Information by Group
Significant difference between etiologies at p<0.05.
SBM, spina bifida myelomeningocele participants; TD, typically developing controls.
Table 2 describes clinical markers of SBM. Multiple shunt revision surgeries are common in this population (Reigel and Rotenstein, 1994); most in this sample had at least one shunt revision. Most participants were partially ambulatory; only 2 of 24 had normal ambulation. Based on clinical coding of MRI scans performed by board certified radiologists (Fletcher et al., 2005), three-quarters had an intact, but hypoplastic CC. Most participants with SBM had a Chiari II malformation and lower level lesions.
Clinical Markers
Missing information on 1 case.
Neurobehavioral measures
Three measures previously correlated with area measurements of the CC (Fletcher et al., 1996) were used for this study: Stanford-Binet Test of Intelligence (Thorndike et al., 1986), Purdue Pegboard (Tiffin, 1968), and dichotic listening (Hannay et al., 2008).
Stanford-Binet test of intelligence, 4th ed
The composite IQ score from the Stanford-Binet intelligence test (Thorndike et al., 1986) was utilized as a measure of general cognitive ability. Raw scores were four subtests (verbal reasoning, abstract/visual reasoning, quantitative reasoning, and short-term memory) converted to standard age scores, which then were converted to the composite IQ score. The composite IQ score demonstrates excellent reliability with internal consistency reliability ranging from 0.95 to 0.99 for 17 different age groups (Thorndike et al., 1986).
Purdue Pegboard
The Purdue Pegboard test assesses unimanual and bimanual fine motor dexterity (Tiffin, 1968) by requiring participants to place small pins into a perforated board as quickly as possible in 30 sec time intervals. Test-retest reliability estimates for single-trial scores range from r=0.63 to r=0.82 (Tiffin, 1968). The number of pegs placed in the board by both hands in 30 sec, the bimanual trial score, was used as the measure.
Dichotic listening
A verbal DL paradigm was administered using a TASCAM 202 MK III cassette deck with an Optimus SA-155 stereo amplifier (Hannay et al., 2008). Participants listened to auditory stimuli in both ears on Sony MDR-7506 professional quality stereo headphones calibrated at 81 dB audio output level. A monotic listening task was used as a screener to ensure that the participants could hear and discriminate between the auditory stimuli. For the DL paradigm, six consonant-vowel (CV) syllables acted as the auditory stimulus. The syllables were created from the six stop consonants,/b/,/d/,/g/,/k/,/p/, and/t/and the vowel/a/, resulting in the sounds/ba/,/da/,/ga/,/ka/,/pa/, and/ta/(Hugdahl, 2003). Pairs of CV syllables were presented simultaneously, a different syllable to each ear. The task was to report the strongest syllable heard first and then, if possible, to report the other syllable heard (Hiscock and Decter, 1988). With six CV syllables, 36 pairs of syllables were possible. A total of 72 trials were administered. All 36 pairs were presented and then the headphones were reversed and the pairs were presented again (Hannay et al., 2008). The number of correct first responses after stimuli presentation to the right and the left ears on each trial were used as the dependent measures, as in earlier studies of SBM and CC (Hannay et al., 2008). This allowed an examination of whether scores were increasing or decreasing with right or left ear presentation in the groups.
Procedures
All participants had the same imaging protocol and neuropsychological assessment in a quiet laboratory setting by trained examiners supervised by licensed neuropsychologists (Fletcher et al., 2005). A subset of the imaging sequences and the neuropsychological tests administered were used for the DTT and correlation analysis.
MRI and DTI acquisition and processing
Whole brains were scanned using a Philips 3.0T Intera system with a SENSE (Sensitivity Encoding) receive head coil. The MRI protocol included two conventional MRI scans and matching diffusion-encoded tensor MRI scans (DT-MRI). The conventional MRI scans included a 3D spoiled gradient-echo (FOV=240×240 mm2 and isotropic voxel size=0.9375 mm) and 2D dual fast spin-echo (echo times: TE1/TE2=10/90 ms; repetition time: TR=5000 ms; 44 axial slices of 3 mm thickness and 0 gap). The DT-MRI data were acquired axially (superior to inferior from the foramen magnum to the vertex) using a single-shot spin-echo diffusion sensitized echo-planar imaging (EPI) sequence with a balanced Icosa21 encoding scheme (Hasan and Narayana, 2006). In total, 44 contiguous 3 mm thick with 0 mm gap axial slices were acquired, thus matching the spatial coverage of the conventional MRI sequences described above and providing full coverage of the entire brain. Acquisition details of the EPI sequence include: diffusion sensitization of b-factor=1000 sec×mm−2, repetition time of TR=6100 msec, echo time of TE=84 msec, FOV=240×240 mm2, and square matrix of 256×256 pixels (Hasan, 2007). The encoding scheme used 21 uniformly distributed directions, which was consistent with scanner capabilities at the time of the study and the need to reduce overall time in the scanner for child participants. The number of nondiffusion weighted (b≈0) magnitude image averages=8 and each encoding was repeated twice and averaged to enhance the signal-to-noise ratio. Total DTI acquisition time was about 7 min. The DTI image processing and DTI quality control measures are described in Hasan (2007).
DTI metrics
The integrity of the fiber tracts of the CC was assessed using DTI-derived rotationally invariant metrics. Three integrity measures [FA, axial (parallel) diffusivity, and radial (perpendicular or transverse) diffusivity] were calculated from the average values of all the voxels that were contained in the fiber tracts of interest (Hasan and Narayana, 2006). FA is a measure of anisotropy or the orientation preference in a voxel (Chanraud et al., 2010); it expresses the proportion of the largest eigenvalue, λ 1 , to the two smaller eigenvalues, λ 2 and λ 3 , in an ellipsoid. Axial diffusivity is a measure of the largest eigenvalue, λ 1 , and radial diffusivity is a measure of the average of the two smaller eigenvalues, λ 2 and λ 3 . Higher axial and radial diffusivity values mean greater water diffusivity, which indicates reduced myelination, tissue organization, and possible axonal pathology.
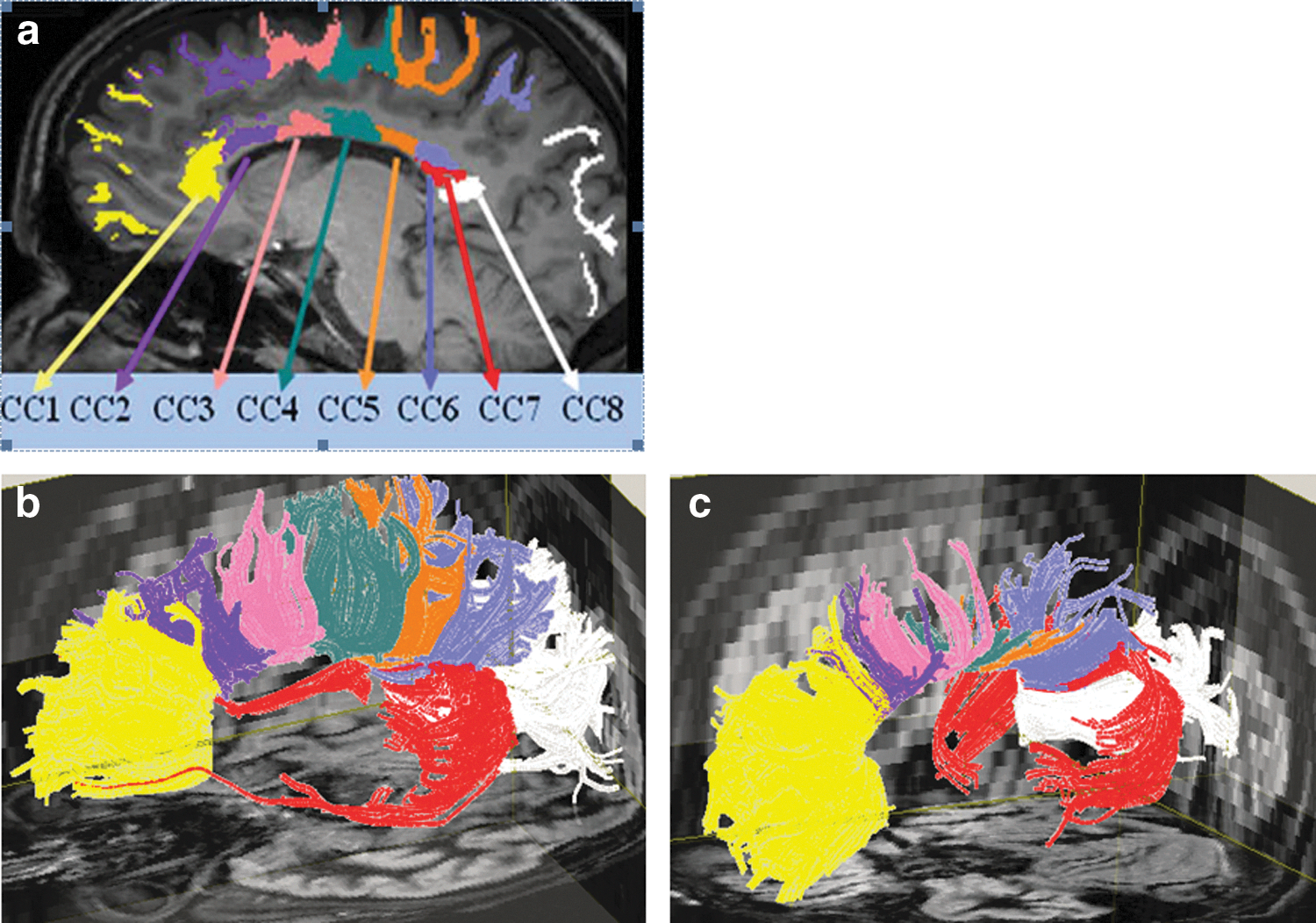
DTT of the CC
Fiber tracking of the CC was performed using DTIStudio software (
Statistical analyses
Age and gender were included as covariates in all ANCOVA models to potentially reduce unexplained variability in the error term. Ethnicity was not used as a covariate in subsequent analyses because it is closely linked with Hispanic ethnicity, which accounts for the lower SES in our participants with SBM, so SES was used as a covariate. These variables were removed from the final models if they did not contribute to a statistically significant interaction or main effect. All analyses involving CC structure, entire CC volumes and CC subvolumes, were normalized for differences in brain size by dividing volume measurements by entire white matter volume (WMV) of the brain and multiplying by 100%. Statistical tests were run using SAS 9.2 Software (
For hypotheses involving structure, separate analyses were completed for entire volume/integrity measures (ANCOVA) and for regional CC measuring a group (SBM vs. TD)×CC segment (CC1–CC8) using a multivariate approach to repeated measures ANCOVA. Due to multiple comparisons, a Bonferroni adjustment of the critical level of alpha (p=0.05/8=0.00625) was used to maintain the family wise error rate at 0.05. Hypotheses involving functioning of the CC were assessed by computing Spearman correlation coefficients among volume, integrity, and behavioral measures within the group with SBM. To avoid inflation of correlations because of the explicit group structure in the data, analyses were run only within the group with SBM. Effect sizes were assessed using eta-squared (η2); calculated by taking the sum of squares of the effect and dividing it by the total sum of squares. Cohen's interpretation of small, medium, and large effect sizes for eta-squared was utilized, where 0.01 constitutes a small effect size, 0.06 a medium effect size, and 0.14 a large effect size (Cohen, 1988).
Results
Neurobehavioral measures
Results are summarized in Table 3. IQ group differences were apparent, t (58)=5.90, p<0.0001, with TD participants performing about one standard deviation higher than the participants with SBM. Consistent with previous studies (Fletcher et al., 2005; Hannay et al., 2008), TD participants performed around one standard deviation higher than the participants with SBM, t (58)=5.90, p<0.0001, with Purdue Pegboard bimanual trial score group differences favoring the TD group, t (55)=3.50, p=0.0009. For dichotic listening, ANCOVA analysis, with presentation ear as the repeated factor, revealed a significant REA for the first reported CV syllables in the TD group, F (1, 19)=14.35, p=0.0012, partial η2=0.43, and in the group with SBM, F (1, 21)=9.35, p=0.006, partial η2=0.31.
Neurobehavioral Test Results (Means and Standard Deviations)
p<0.05.
CV, consonant-vowel; N/A, no statistical comparison was performed so no p-value was generated.
Objective 1: DTT volume and integrity measurements of the CC
No volume or integrity models exhibited significant interactions of age, gender, or SES with group, so all interactions were removed from the final models. Main effects involving age, gender, and SES were tested in each analysis and left in the model in some cases.
Macrostructure (volumetrics)
Only age showed a significant main effect and was included as a covariate in the final volume models. Table 4 shows the results of the group comparisons of mean entire CC normalized volume and CC segment (CC1–CC8) normalized subvolumes adjusted for age. For the entire CC volume, there was a significant effect of group, F (1, 59)=39.11, p<0.0001, η2=0.38, with the group with SBM having smaller CC volumes than the TD participants. For CC1–CC8, the group×CC region interaction was significant, F (7, 51)=11.96, p<0.0001. Table 4 shows that on follow-up of each region, the posterior parts of the CC (CC5-CC8) showed a significant volume difference between the group with SBM and the TD group, p<0.00625, and large effect sizes, all 0.39>η2>0.19. The SBM group had reduced WMV in the posterior CCs relative to the TD group.
Comparison of the Normalized Volumes (CC Volume/WMV×100%) of the Entire CC and CC Subvolumes (CC1–CC8) for the SBM and TD Groups
p<0.00625.
CC, corpus callosum; eCC, entire CC.
Microstructural integrity
For the FA models, only gender was included in the final models. A significant group effect for the entire CC was found, F (1, 59)=9.90, p=0.0026, η2=0.14 (Table 5), with the participants with SBM exhibiting decreased FA in the entire CC when compared to the TD group. In addition, the group×CC region interaction was significant, F (7, 51)=14.85, p<0.0001. In Table 5, the posterior parts of the body of the CC (CC3 and CC4), the isthmus (CC5), and the posterior splenium (CC7 and CC8) showed a significant reduction in FA for the participants with SBM versus the TD comparisons, p<0.00625, and large effect sizes, 0.43>η2>0.16.
Comparison of FA of the Entire CC and CC Subvolumes (CC1–CC8) for the SBM and TD Groups
p<0.00625.
FA, fractional anisotropy.
For the axial diffusivity models, only age was included as a covariate. Table 6 shows the results of the statistical analysis of mean entire CC axial diffusivity and CC segment (CC1–CC8) axial diffusivity. Contrary to hypothesis, the effect of group for entire CC did not meet the critical level of alpha, F (1, 59)=2.09, p=0.15. The group×CC region interaction was significant, F (7, 51)=10.96, p<0.0001. Table 6 shows that on follow-up of each region, the isthmus (CC5) and the most anterior portion of the splenium (CC6) showed a significant increase in axial diffusivity for the participants with SBM versus the TD comparisons, p<0.00625, and large effect sizes, 0.29>η2>0.27.
Comparison of Axial Diffusivity (mm2/s) of the Entire CC and CC Subvolumes (CC1–CC8) for the SBM and TD Groups
p<0.00625.
For the radial diffusivity models, only age was included in the final model. Table 7 shows the results for entire CC radial diffusivity and CC segment (CC1–CC8) radial diffusivity. The effect of group for the entire CC was significant, F (1, 59)=17.04, p=0.0001, η2=0.20, with the group with SBM demonstrating increased radial diffusivity in the entire CC when compared with the TD group. The group×CC region interaction was also significant, F (7, 51)=16.51, p<0.0001. For individual CC segments, the posterior body (CC3 and CC4), the isthmus (CC5), and the entire splenium (CC6, CC7, and CC8) showed a significant increase in radial diffusivity for the participants with SBM compared to the TD group, p<0.00625 (Table 7). Results for CC3 demonstrated a medium effect size, η2=0.13, and results for the more posterior regions of the CC (CC4–CC8) exhibited a large effect size, 0.37>η2>0.17.
Comparison of Radial Diffusivity (mm2/s) of the Entire CC and CC Subvolumes (CC1–CC8) for the SBM and TD Groups
p<0.00625.
Objective 2: Correlations between structure and function of the CC in SBM
IQ was significantly correlated with entire CC volume, rho=0.44, p=0.02. Regionally, IQ significantly correlated with CC1 volume (genu fibers), rho=0.38, p=0.048, and the posterior CC volume, CC7 and CC8 (splenium), rho>0.38, p<0.04. IQ did not significantly correlate (p<0.05) with entire CC FA, axial diffusivity, or radial diffusivity. Regionally, IQ significantly correlated with FA, rho=0.39, p=0.04, and radial diffusivity in the posterior CC, CC8, rho = −0.41, p=0.03. No significant correlations (critical level of p<0.05) were found between IQ and regional CC axial diffusivity.
Bimanual coordination did not significantly correlate (critical level of p<0.05) with entire CC volume. Regionally, bimanual coordination significantly correlated with CC1 volume (genu), rho=0.40, p=0.05, and CC7 volume (temporal lobe fibers), rho=0.40, p=0.04. Contrary to our hypothesis, bimanual coordination did not significantly correlate (critical level of p<0.05) with any integrity measure (FA, axial diffusivity, or radial diffusivity) of the entire CC or the regions of the CC (CC1–CC8).
Neither DL measures (number of first response CV syllables of each ear) correlated with entire CC volume or with individual regions of the CC (CC1–CC8; critical level of p<0.05). Furthermore, neither DL measure significantly correlated (critical level of p<0.05) with FA, axial diffusivity, or with radial diffusivity of the entire CC. Regionally, the number of first response CV syllables of the right ear correlated negatively with axial diffusivity in CC fibers traveling to the occipital lobe (CC8), rho = −0.58, p=0.005. No significant correlations were found with DL performance and regional FA or radial diffusivity.
Discussion
Questions about CC structure and function have been addressed with individuals or small groups with epilepsy and corpus callosotomy or with congenital CC agenesis/hypogenesis. In this article, we have studied individuals with SBM who exhibit an intact but hypoplastic CC and used this unique configuration of the CC to explore a set of questions about CC macrostructure and microstructure that are not accessible from studies of corpus callosotomy or hypogenesis. The principal finding was that the hypoplastic CC is not macrostructurally or microstructurally intact in SBM. We found both global and regional macrostructure and microstructure differences, and we were able to identify a set of structure-function relations. The data bear on a number of issues: the effect of posterior CC hypogenesis on CC volume reductions; the role of hydrocephalus in CC hypoplasia; the nature of global and regional CC microstructure; and differences in function between those with CC hypogenesis and those with CC hypoplasia.
DTT volume and integrity of the CC
This study provides the first analysis of entire CC volume and subvolumes in SBM. Previous research that quantified the structure of the SBM CC focused on region of interest (Hasan et al., 2008) or midsagittal area measurements of the CC (Fletcher et al., 1992, 1996; Herweh et al., 2009). The new information is that group reductions in entire CC volume occur in SBM, even when participants with posterior hypogenesis are excluded.
The results help clarify the role of hydrocephalus in CC hypoplasia. Hydrocephalus, a secondary neural factor due to mechanical CSF blockage, may be responsible for the thinning of the hypoplastic/intact CC in SBM. The primary developmental mechanisms leading to hypogenesis of the CC in SBM occurs early in gestation and are likely related to the overall disruption of brain development, especially because the most anterior and posterior portions of the CC are missing and may not develop (Barkovich, 2005). We found that the posterior regions of the CC (isthmus and the splenium) were most reduced in volume, consistent with the conclusion that the posterior CC is the most affected by SBM pathology. All participants had hydrocephalus, so these findings imply a continuum of impairment in relation to hypoplasia as opposed to qualitatively different events, given that hypogenesis affects posterior regions of the CC.
Most studies have relied on macrostructure assessments, like area or volume, to make conclusions about the status of the CC. Structural measurements of white matter alone, like volume and area, may not be sensitive to alterations of the CC, especially in this particular population of participants with SBM who have hypoplastic/intact CCs. Integrity measures, such as FA, have been demonstrated to be more sensitive to white matter changes than volume alone (Fjell et al., 2008).
The study adds new information about the microstructural integrity of the CC in SBM. Consistent with previous research by Hasan and colleagues (2008) and Herweh and colleagues (2009), we found that FA was reduced in SBM. We add two pieces of new data in a larger sample: FA reduction, global and regional, occurs even when the CC is not hypogenetic; and there are specific reductions in the posterior body, isthmus, and posterior splenium.
Higher axial and radial diffusivity values indicate greater water diffusivity, which may be related to demyelination, reduced tissue organization, and axonal pathology (Beaulieu, 2002). Significantly increased radial diffusivity—but not axial diffusivity—was found in the entire CC of the participants with SBM. Only the isthmus and the anterior splenium showed a significant difference in axial diffusivity between the two groups, with the SBM group displaying higher axial diffusivity in these regions. Increased radial diffusivity was observed in all parts of the posterior SBM CC, including the posterior body, the isthmus, and the entire splenium.
The results of this study were consistent with other studies that considered the effects of hydrocephalus in humans and animals (Assaf et al., 2006; Del Bigio et al., 2003). Assaf and colleagues (2006) used DTI to study the effects of hydrocephalus on periventricular white matter in patients with acute hydrocephalus and found that the CC had decreased FA and dramatically increased radial diffusivity, the same pattern of results found in this study. Furthermore, Assaf and colleagues (2006) noted greater alteration of the posterior CC than the anterior CC in hydrocephalus, also consistent with the results of this study. Ito and colleagues (1997) found that ventriculomegaly in children with SBM and hydrocephalus was most severe in the posterior horns of the lateral ventricles, and concluded that pathological changes might be more severe in areas surrounding the posterior horns, like the posterior CC. These effects of hydrocephalus also help explain why other commissural structures of the brain (e.g., the anterior capsule, which is not located near the posterior lateral ventricles) do not exhibit the same kind of pathological changes that the CC exhibits in SBM (Herweh et al., 2009).
Structure-function correlations of the CC in SBM
IQ correlated positively with the volume of the entire CC, and regionally with the anterior and posterior CC. IQ decreased with volume decreases in the genu and splenium fibers of the CC, a finding consistent with previous research where measures of IQ positively correlated with area measures of the entire CC in SBM (Fletcher et al., 1992, 1996).
Measures of integrity reflected a similar pattern. IQ positively correlated with FA in the posterior CC and negatively with radial diffusivity of the posterior CC. As FA decreases in the posterior CC (indicating less fiber density, axonal diameter, and myelination), IQ decreases. The negative correlation between IQ and radial diffusivity indicates that IQ decreases with increases in radial diffusivity in the posterior CC (indicating tissue disorganization and reduced myelination). Either the CC may be pivotal for normal intellectual functioning and both macrostructural (volume reduction) and microstructural (demyelination and reduced fiber density) changes in white matter affect cognitive functioning in SBM or it may simply be a marker for overall severity of changes to the white matter that may affect global intellectual functions.
Previous research has found a moderate relation between area measurements of the CC and fine motor dexterity in children with SBM, which included both hypoplastic and hypogenetic CC (Fletcher et al., 1992, 1996). We found no correlation between bimanual fine motor skills in SBM and entire CC volume in this group with hypoplastic CCs. We hypothesized that bimanual fine motor skills would significantly correlate with the volume of the body of the CC because the anterior body has projections to the motor cortex. Bimanual coordination did correlate positively with the volume of the genu (CC1) and the temporal lobe fibers (CC7), although not the body of the CC, such that bimanual fine motor skills decrease with volume decreases in the genu and temporal fibers of the CC. In a previous DTI study of healthy subjects, Johansen-Berg and colleagues (2007) found a high correlation between bimanual coordination and FA in the body of the CC. In the present study, no significant correlations were observed with bimanual coordination and any of the integrity measures. Though findings are contrary to hypothesis, there is evidence that the CC is important for interhemispheric transfer of lateralized information, such as visuospatial or verbal premotor information, and it may not be heavily involved in transfer of explicit motor commands from the motor cortex (Geffen et al., 1994). Bimanual coordination requires feedback from the senses, especially from vision and proprioception, and the CC seems to be the conduit for transfer of this information (Geffen et al., 1994). Along with sensory information, motor feedback mechanisms are important for bimanual coordination of the CC. Indeed, feed-forward mechanisms appear to be transmitted through the anterior CC and feedback mechanisms are likely transferred through the posterior CC (Geffen et al., 1994). Therefore, the correlations between bimanual fine motor skills and the anterior and posterior CC volumes, rather than the body of the CC, may actually reflect coordination of motor feedback in SBM. Since the correlation was positive, bimanual motor skills decrease as the volume of the anterior and posterior CC decreases in volume.
Neural anomalies other than the CC have significant impact on fine motor coordination in SBM. Because of the Chiari II malformation, the cerebellum and its connectivity to other brain regions is impaired in SBM (Juranek et al., 2010). Hand function also reflects the cerebellar influences on precision and timing of fine motor movements. Tasks that make lower demands on precision and timing, but require interhemispheric transfer (e.g., tactile naming) may be more sensitive to the alterations in hand connectivity.
Research on healthy participants has shown correlations between DL performance (specifically the size of the REA) and the midsagittal cross-sectional area of the typically developed CC (Yazgan et al., 1995; O'Kusky et al., 1988). In research utilizing DTI, significant correlations were found between DL measures and area measures of the entire CC, and the isthmus, body, and genu of the CC (Westerhausen et al., 2006). Research with partial callosotomy patients has indicated that the isthmus and splenium are important for normal DL performance (Springer and Gazzaniga, 1975). Although we had hypothesized that participants with SBM and hypoplastic/intact CCs would demonstrate relations between DL performance and entire CC volume and sspecifically with the posterior CC, no significant relations were found with DL performance measures and CC volume. This highlights the difference between CC hypogenesis and CC hypoplasia in individuals with SBM: The absence of a REA has been primarily associated with hypogenesis rather than hypoplasia of the CC in SBM (Hannay et al., 2008); and differences in CC hypogenesis and CC hypoplasia in SBM have been described for aspects of oral language comprehension (Huber-Okrainec et al., 2005).
Other studies have found relations of DL measures in samples that include people with SBM and hypogenetic CC, but not hypoplastic CC (Hannay et al., 2009). We hypothesized that DL scores would correlate with integrity measures of the posterior CC because previous research has found correlations between DL measures and DTI integrity measures (FA and mean diffusivity) in the posterior third of the CC in TD participants (Westerhausen et al., 2006). No significant correlations were found between DL scores and FA or radial diffusivity. However, one significant negative correlation was found between the right ear performance on DL and axial diffusivity of the fibers traveling through the posterior CC to the occipital lobe (CC8). This indicates as axial diffusivity increases (increased pathology) in the posterior CC, DL performance of the right ear decreases. Although this finding is consistent with the general hypothesis, a correlation with the occipital lobe fibers is not where the strongest correlation was expected. Previous studies found the strongest correlations with the isthmus (since fibers traveling from the isthmus travel to the auditory cortex). Furthermore, axial diffusivity in the occipital fibers (CC8) was not significantly different between the participants with SBM and the TD participants and we would not expect the TD participants to have a significant correlation between DL and CC8. This finding may be an artifact of the number of independent tests conducted for correlations, though a Bonferroni adjustment was utilized to maintain the family wise error rate at 0.05.
Limitations and future directions
Although an encoding scheme of only 21 directions can be justified (Lebel et al., 2012), especially in relation to the time required to acquire the entire imaging sequence on the scanner available when the study began, current DTI acquisition techniques using more directions, higher spatial resolutions, or multiple b-factors likely would have improved signal detection and more significant results may have been observed. Consequently, the DTI encoding scheme used may actually have underestimated the severity of callosal pathology in our sample of SBM patients.
Handedness and lesion level have been shown to affect ear advantage in DL tasks in SBM (Hannay et al., 2008). A much larger and heterogeneous sample would be needed to address these questions, especially if they relate to structural brain assessments. In this study, the few nonright-handers and upper level spine defects tended to show REAs. In addition, the age range was broad. Both WMV (Wozniak and Lim, 2006; Giedd, 2004) and FA (Cascio et al., 2007; Snook et al., 2007) increase in childhood and adolescence. For the CC, Hasan and colleagues (2008, 2009) showed that the CC FA and macrostructure (area and volume) followed an inverted U-shaped curve across the lifespan and CC axial and radial diffusivity followed a U-shaped curve across the lifespan. In other words, the CC changes across the lifespan, both in size and microstructure, and there may be differences in these measures between different age groups. Future studies with larger samples and longitudinal evaluations that permit assessment of growth and development would enhance understanding of the structure and function of the CC in SBM and other disorders characterized by callosal pathology.
Conclusion
The hypoplastic CC in SBM is not normal, but shows variations in volume and integrity that affect neurobehavioral function. The pattern of macrostructural and microstructural volume and integrity differences were largely focused in the posterior CC (posterior body, isthmus, and splenium). This was expected considering that posterior brain regions in SBM are generally more affected by the hydrocephalus (Fletcher et al., 1996). Although structural hypotheses were supported, relatively few significant correlations were found between functional outcomes and CC volume and integrity measures in this particular sample of participants with SBM and hypoplastic/intact CCs. Interhemispheric function appears intact in the hypoplastic CC and the relations that do emerge may reflect more general relations with the severity of white matter injury.
Footnotes
Acknowledgments
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development grants P01 HD35946 (Spina Bifida: Cognitive and Neurobiological Variability) and 5U01 HD068541-02, A Follow-Up of Children Enrolled in the Management of Myelomeningocele Study. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health and Human Development or the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.