
Abstract
Age-related macular degeneration (AMD), the leading cause of blindness in developed nations, has been associated with poor performance on tests of phonemic fluency. This pilot study sought to (1) characterize the relationship between phonemic fluency and resting-state functional brain connectivity in AMD patients and (2) determine whether regional connections associated with phonemic fluency in AMD patients were similarly linked to phonemic fluency in healthy participants. Behavior-based connectivity analysis was applied to resting-state, functional magnetic resonance imaging data from seven patients (mean age=79.9±7.5 years) with bilateral AMD who completed fluency tasks prior to imaging. Phonemic fluency was inversely related to the strength of functional connectivity (FC) among six pairs of brain regions, representing eight nodes: left opercular portion of inferior frontal gyrus (which includes Broca's area), left superior temporal gyrus (which includes part of Wernicke's area), inferior parietal lobe (bilaterally), right superior parietal lobe, right supramarginal gyrus, right supplementary motor area, and right precentral gyrus. The FC of these reference links was not related to phonemic fluency among 32 healthy individuals (16 younger adults, mean age=23.5±4.6 years and 16 older adults, mean age=68.3±3.4 years). Compared with healthy individuals, AMD patients exhibited higher mean connectivity within the reference links and within the default mode network, possibly reflecting compensatory changes to support performance in the setting of reduced vision. These findings are consistent with the hypothesis that phonemic fluency deficits in AMD reflect underlying brain changes that develop in the context of AMD.
Introduction
Age-related macular degeneration (AMD) is a disease that affects people over 50 years of age and is characterized by gradual damage to the macula, which is the part of the retina that is responsible for sharp, central vision (Bressler et al., 1988; National Eye Institute, 2011). AMD does not cause complete blindness, but loss of central vision makes it difficult for affected persons to read, recognize faces, drive, or perform tasks that require detailed near-vision. About 30% of Americans over age 75 have AMD, although the rate of progression to significant vision loss varies (National Eye Institute, 2011). The annual incidence of AMD increases with age and, due to the increasing human lifespan, the prevalence of AMD is rising (Klein et al., 2002; Rein et al., 2009).
Studies with both animals (Darian-Smith and Gilbert, 1995; Giannikopoulos and Eysel, 2006; Kaas et al., 1990) and young humans (Liu et al., 2007; Pascual-Leone et al., 2005) have reported changes in brain function in response to decreased visual input, but the extent of brain changes associated with late-life maculopathy is unknown. Only a few functional magnetic resonance imaging (fMRI) studies on AMD have been reported, and they have typically focused on visual cortex activity during visual stimulation or tasks. One study compared eight patients with bilateral AMD with age-matched controls who had normal, or corrected-to-normal, vision (Baseler et al., 2011). During fMRI sessions, participants viewed standard retinotopic mapping stimuli (projected images of an expanding ring and rotating wedge). Some control subjects participated in a second scanning session during which AMD lesions were “simulated” by obscuring the central portion of the expanding ring stimuli. During retinotopic mapping sessions, AMD patients and controls with simulated lesions exhibited similarly diminished signals within their occipital poles (the lesion projection zone) (Baseler et al., 2011). For the AMD patients, the magnitude of fMRI response in regions of primary visual cortex (V1) that typically respond to peripheral retina was predicted by the amount of intact peripheral retina (Baseler et al., 2011). Taken together, these results indicate that AMD leads to diminished V1 activation of occipital cortex but not to widespread remapping of this cortical region (Baseler et al., 2011). In other words, in persons with long-standing AMD, as in normally sighted individuals, it appears that V1 activation is related to the degree of stimulation of intact retina.
However, the overall decrease in V1 stimulation that results from AMD may alter brain activity in other ways, due to changes in feedback signals or task demand (Masuda et al., 2008; Wandell and Smirnakis, 2009). AMD patients, compared with sighted peers, exhibit increased activation in prefrontal and parietal cortex during word recognition and processing tasks, possibly reflecting greater top-down attentional involvement to compensate for decreased visual input (Szlyk and Little, 2009). AMD patients exhibit greater activation in prestriate cortex (V2), compared with age-matched controls, when presented with monocular stimulation, which may be due to diminished feedback from the understimulated occipital poles (Nguyen et al., 2004). A study of four AMD patients found that the quiet area in the occipital pole was smaller during tasks of active viewing, compared with passive viewing, which may reflect task-dependent differences in top-down feedback signaling to the occipital pole (Liu et al., 2010). The task-dependent difference in V1 activation was even more pronounced among individuals who acquired their macular lesions earlier in life due to juvenile macular degeneration, in keeping with the theory that macular lesions induce brain changes (Liu et al., 2010).
If macular lesions alter brain activity, whether the mechanism is adaptive or consequential, then these brain changes may affect regions or neuronal networks that support cognitive processes. Data from behavioral investigations suggest a link between AMD and late-life cognitive changes. In several study populations, AMD patients, compared with their peers, exhibited higher rates of cognitive impairment (Pham et al., 2006; Woo et al., 2012), lower scores on cognitive tests (Baker et al., 2009; Clemons et al., 2006; Wong et al., 2002), and a twofold higher risk of incident dementia (Klaver et al., 1999). Recent work by our group and others suggests that AMD patients, even in the absence of dementia, perform especially poorly on tests of phonemic verbal fluency (Clemons et al., 2006; Whitson et al., 2010; Wong et al., 2002), which are indicators of executive function (Salthouse et al., 2003). However, we are not aware of prior studies that have examined the relationship between neurocognitive ability and regional brain activity in persons with AMD.
In this pilot study we investigated potential changes, with AMD, in the relation between cognitive performance and one measure of brain activity. Specifically, we investigated AMD-related differences in resting-state (intrinsic) functional brain connectivity (De Luca et al., 2006; Greicius et al., 2003; Lee et al., 2013). Resting-state functional connectivity (rsFC), though obtained in the absence of a task, differentiates task-relevant networks and covaries with task performance (obtained either during scanning or as a separate measure), demonstrating a role in cognitive function (Fox et al., 2006a, 2006b, 2007; Parks and Madden, 2013). In healthy individuals, the magnitude of rsFC typically decreases with adult age (Andrews-Hanna et al., 2007; Damoiseaux et al., 2008). Moreover, the covariation between rsFC and behavior changes with age, often decreasing but also increasing in some networks depending on the behavioral measure (Chen et al., 2009; Chou et al., 2013; Ferreira and Busatto, 2013). In comparing connectivity patterns between persons with and without AMD, an advantage to rsFC is that it is obtained without the introduction of visual or other task demands that may vary between participant groups.
Although AMD-related changes in behavioral measures of cognition as well as brain activation have been reported previously, in separate investigations, it has not been determined how behavioral and brain measures may be related in AMD. The primary objective of this pilot study was to examine the relationship between fMRI measures of rsFC, across several preselected functional networks, and behavioral assessment of phonemic fluency (obtained prior to the scanning session) in individuals with AMD. To do so, we identified pairs of brain regions (i.e., reference links) for which connectivity was associated with phonemic fluency in people with AMD. Next, using available data from healthy participants, we tested whether phonemic fluency was similarly associated with rsFC among the same reference links in people with normal vision. Our hypothesis was that the high rate of phonemic fluency deficit in AMD is due, at least in part, to brain changes that occur in the context of AMD. We therefore postulated that poor phonemic fluency would be associated with a unique pattern of rsFC in persons with AMD, relative to healthy individuals without AMD.
Methods
Participants
The AMD patients were seven individuals with long-standing, bilateral AMD (mean age=79.9±7.5 years, range=69–91 years; one man) recruited from Duke Eye Center clinics. Exclusion criteria were as follows: contraindication to 3.0 Tesla (T) MRI, vision-limiting eye conditions other than AMD, dementia (based on existing diagnosis or five or more errors on the Short Portable Mental Status Questionnaire) (Pfeiffer, 1975), left-handedness, history of brain surgery or significant brain pathology, and hearing loss or language barriers that prohibited survey administration.
For comparison, we examined data from two groups of healthy, community-dwelling adults: 16 older adults (mean age=68.3±3.4 years, range=65–74 years; 8 men) and 16 younger adults (mean age=23.5±4.6 years, range=18–35 years; 8 men) from a separate study protocol in the Duke Brain Imaging and Analysis Center (BIAC). Because the older-healthy group was younger, on average, than the AMD group, the young-healthy group was included to establish the direction of age-related changes in healthy people, potentially providing insight about whether any differences observed in the AMD group were age related versus AMD related. All participants in the comparison groups were right-handed, native English speakers with normal or corrected-to-normal vision. None reported a history of neurological or psychological disorders or any major medical conditions (e.g., diabetes and heart disease).
Each participant provided informed consent and received a small stipend. All experimental procedures were approved by the Duke University Medical Center Institutional Review Board.
Phonemic fluency test
Participants were administered the Controlled Oral Word Association Test (COWAT) (Loonstra et al., 2001), a phonemic fluency test, by trained individuals under standardized conditions in private, quiet exam rooms. In this test, participants are instructed that they will have 60 sec to name as many unique words as they can that begin with a particular letter. Participants are told to refrain from using proper nouns “such as the names of people or places” and that they should not repeat the same word with a different ending “such as run, running, runner.” After a practice trial to ensure comprehension of the task, participants completed three 60-sec trials with letters F, A, and S. The total score reflects the number of unique, acceptable words generated, summed across the three trials. Healthy participants completed cognitive testing 1–3 weeks prior to the date of their scan; AMD patients were tested immediately prior to the scan.
MRI acquisition
The imaging studies were performed on 3.0-T scanners at the Duke/UNC BIAC. For each participant, imaging included a localizer scan, high-order shimming, high-resolution structural scans, and functional resting-state imaging. The scanner employed for the AMD patients used the GE MR750 platform and the scanner employed for healthy participants used the GE ExciteHD platform. Both scanners operate with 40 mT/m gradient system and a 150 T/(m·s−1) slew rate. An eight-channel head coil was used for radio frequency reception (General Electric, Milwaukee WI). Sagittal T1-weighted localizer images were used to define a volume for data collection and high-order shimming. The anterior and posterior commissures were identified for slice selection, and a semiautomated high-order shimming program was used to ensure global field homogeneity.
The T2*-weighted functional imaging runs acquired slices parallel to the anterior commissure–posterior commissure plane using T2*-weighted imaging sequences that are sensitive to the blood-oxygen-level-dependent (BOLD) contrast. The specific T2* imaging acquisition parameters for the two study populations (AMD patients and healthy older volunteers) are summarized in Table 1.
Comparison of Imaging Acquisition Parameters in Study Participants
AMD, age-related macular degeneration.
For AMD patients, we acquired all brain imaging in the resting state, with no assigned task. AMD patients were instructed to “think about nothing in particular” and keep their eyes closed, in order to account for differing visual abilities. The resting-state fMRI data for healthy participants were collected at the beginning of the scan session (before any task) in a 5-min run, during which participants were instructed to keep their eyes open and look at a fixation cross. All participants remained awake for the duration of their fMRI run (confirmed by verbal communication after each run).
Data analysis
Data preprocessing
We conducted preprocessing through the BIAC processing daemons based on the tools from the Oxford Centre for Functional MRI of the Brain's Software Library (FSL version 4.0,
Analysis of FC
The preprocessed data were segmented into 116 regions of interest (ROIs) (90 cerebral and 26 cerebellar) using automated anatomical labeling (AAL) (Tzourio-Mazoyer et al., 2002). Intrinsic FC analyses rely on the covariances of the BOLD signal time series data to identify distributed cortical regions that activate in concert. The AMD and healthy comparison groups had different data-acquisition parameters, so we did not combine data from these groups. Rather, our primary aim was to identify pairs of brain regions in the AMD cohort for which FC covaried significantly with phonemic fluency. In an exploratory analysis, we tested whether the FC of these reference links was similarly associated with phonemic fluency among healthy individuals in the comparison groups.
Resting-state data present an opportunity to study connections within and across functional networks simultaneously. Because prior evidence suggests that AMD involves brain changes beyond the visual system (Nguyen et al., 2004; Szlyk and Little, 2009), many regions could be implicated in AMD patients' low performance on tasks of phonemic fluency. However, to minimize Type I error, we focused on a preselected set of ROIs involved in networks that support executive function, language, and/or vision. We hypothesized that connections between these ROIs were potentially relevant to phonemic fluency in people with AMD. Based on the AAL template (Tzourio-Mazoyer et al., 2002), we selected 24 ROIs (Table 2). Our analyses included the left and right hemispheres for each of these regions, yielding a total of 48 ROIs.
Regions Preselected for Inclusion in the Behavior-Based Connectivity Analysis in Age-Related Macular Degeneration Patients
Automated Anatomical Labeling (Tzourio-Mazoyer et al., 2002).
Primary analysis
Using data from AMD patients, we conducted a behavior-based connectivity analysis (BBCA) (Chen et al., 2009; Chou et al., 2013), to identify pairs of functionally connected regions in which the degree of intrinsic FC correlated with phonemic fluency performance. First, each participant's BOLD time series was averaged within each brain region. We calculated the Pearson correlation coefficient between averaged BOLD signal time series data for each pair of the 48 ROIs in the AMD study population. This yielded 1128 [(48×47)/2] unique connections (r values) for each of the seven AMD participants. To improve normality, we transformed the correlation coefficients (r values) to Zr values using Fisher's r-to-z transformation (Fisher, 1921). Next, we thresholded the 1128 connections on the basis of the correlations between those Zr values and fluency scores. In other words, we correlated the FC (Zr) of each link to phonemic fluency test scores across the seven AMD patients, resulting in 1128 correlation calculations. Using a cluster-size thresholding approach (Forman et al., 1995), we identified links for which FC covaried significantly with fluency (alpha level=0.01 with a cluster-sized threshold of two yields false positive probability=0.0008, corrected).
Secondary analyses
After the primary analysis identified six links for which FC was significantly related to phonemic fluency in our sample of seven AMD patients, our secondary objective was to evaluate whether the fluency-associated links defined in the AMD patients (i.e., the six “reference” links) were also associated with phonemic fluency in the healthy participants. First, we performed a two-way analysis of variance (ANOVA) with group (AMD, older healthy adults, and younger healthy adults) as a between-subject variable and link (the six links identified by BBCA, as described previously) as a within-subject variable. Age and education were included as covariates. Connectivity strength (Zr) was the dependent variable. The purpose of this analysis was to test whether there were significant differences in connectivity strength across the reference links or across the study groups. When significant differences were found, post hoc analyses were pursued to further characterize the differences.
Next, using the BBCA-identified links as a reference, we averaged the regional FC values (r) across the six links for each participant. Our primary rationale for averaging the FC values was to reduce the number of comparisons and to produce simple, more easily interpretable results. This approach was supported by a multivariable analysis that demonstrated no interaction between group and link with respect to FC. Next, we derived the correlation between these mean FC values and fluency, for each group. Because the reference links were defined in the AMD cohort, we expected that mean FC would correlate with fluency in that group. The purpose of this analysis was to examine group differences in the fluency-connectivity correlation.
Finally, as a supplementary analysis, we examined group differences in the default mode network (DMN) (Greicius et al., 2003; Raichle et al., 2001; van den Heuvel et al., 2009). These are brain regions that appear to be involved in self-referential memory and planning, which are deactivated during task performance but significantly covary at rest. Here, we selected four regions (left/right averaged) corresponding to major components of the DMN: medial prefrontal cortex, posterior cingulate cortex, lateral parietal cortex, and parahippocampal cortex. rsFC within the DMN has been found to diminish with normal aging (Ferreira and Busatto, 2013), but is increased in some disease states (Sharp et al., 2011; Whitfield-Gabrieli and Ford, 2012). For each participant, we constructed a DMN FC composite score, by averaging all of the z-transformed correlations, for the resting-state BOLD data, among the four ROIs. Although a multivariate analysis of the DMN links indicated a significant interaction between group and link, we decided to utilize a composite FC score because the absolute group difference in FC was in the same direction across all links (but the comparison only rose to statistical significance for certain links).
This DMN analysis served to confirm that we could replicate findings of age-related trends in resting-state DMN connectivity among our healthy participants. Further, because our healthy older participants are younger than the AMD patients, we used the well-characterized DMN to evaluate whether differences in the BBCA-defined links across the three study groups might be strictly age related. Finally, because we have no reason to expect that DMN connectivity would be related to phonemic fluency performance, the DMN analysis was useful as a validity check of the fluency-related findings.
We performed an ANOVA with group (AMD, healthy older adults, and younger older adults) as a between-subject variable to test for a difference in DMN mean FC across the groups. When a significant group effect was revealed, we pursued post hoc analyses to compare the DMN mean FC between groups and assess for age-related effects. To assess the regional specificity of a relationship between FC and phonemic fluency, we evaluated whether any significant correlations existed between DMN mean FC and phonemic fluency performance.
Results
Participant characteristics
The characteristics of the study participants are summarized in Tables 3 and 4. Each group of healthy participants included four African-Americans and equal numbers of men and women. The AMD patients were all Caucasian and only one was male (Patient 3 from Table 3). All AMD patients had long-standing (>3 years), bilateral disease, but some had pronounced discrepancy in visual acuity between eyes. When such discrepancy existed, the right eye was always the better eye, a fact which we believe was due to chance. Considering that both retinas contribute fibers to visual streams in each hemisphere, we do not expect that the left-predominance of visual impairment impacted our analysis of cortical FC in these patients. The healthy comparison groups were significantly younger and better educated, on average, relative to the AMD patients. Fluency scores were highest among the younger healthy participants; AMD patients' mean score was considerably lower than either the older or younger healthy participants' mean score.
Characteristics of the Seven Patients with Age-Related Macular Degeneration
Dry, or atrophic-type, AMD is characterized by drusen (small deposits) beneath the macula. Wet, or neovascular-type, AMD is characterized by abnormal growth of blood vessels beneath the macula. Dry AMD is typically more slowly progressive, though either type can result in significantly decreased visual acuity. Approximately 10–15% of dry AMD cases convert to wet AMD with time.
Verbal (phonemic) fluency score=the number of words generated during three 60-second letter fluency trials (letters F, A, and S).
Characteristics of Participants by Study Group (Age-Related Macular Degeneration Patients, Older Healthy Participants, and Younger Healthy Participants)
The AMD group differs significantly from healthy older group (p<0.05).
The AMD group differs significantly from healthy younger group (p<0.05).
The healthy older group and healthy younger group differ significantly (p<0.05).
M, mean; SD, standard deviation.
Fluency-related links in AMD patients
From the preselected ROIs in Table 2, we used BBCA to identify those rsFC values (Zr) that covaried significantly with phonemic fluency, across the AMD patients. We identified six links for which FC was significantly correlated to fluency score with a false positive probability <0.0008, corrected (Forman et al., 1995). The six links, summarized in Table 5 and illustrated in Figure 1, connected eight regions: left opercular portion of the inferior frontal gyrus (L IFGoperc, which includes Broca's area), left superior temporal gyrus (L STG, which includes part of Wernicke's area), left inferior parietal lobe (L IPL), right inferior parietal lobe (R IPL), right superior parietal lobe (R SPL), right supramarginal gyrus (R SMG), right supplementary motor area (R SMA), and right precentral gyrus (RpreCG). Phonemic fluency was negatively related to the strength of connectivity from the R SMA to the L IFGoperc, L IPL, R IPL, and R SPL and from the RpreCG to the L STG and R SMG.
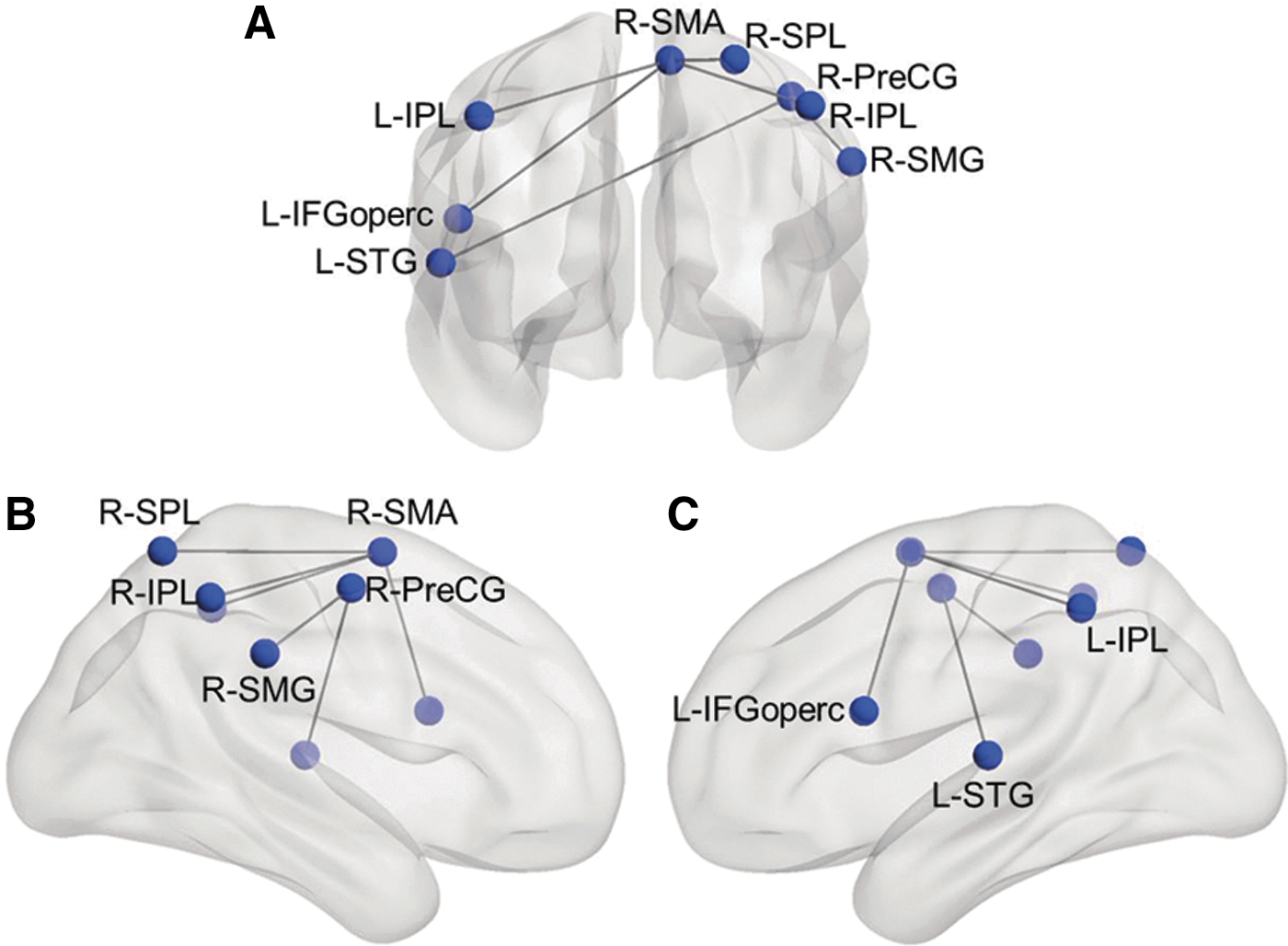
Behavior-based connectivity analysis identified six links (involving 8 regions) for which resting-state functional connectivity (rsFC) was correlated to phonemic fluency scores in patients with age-related macular degeneration (AMD). The figure displays the six links in frontal view
Links Identified by Behavior-Based Connectivity Analysis in Age-Related Macular Degeneration Patients
Abbreviations of brain regions are defined in Table 2.
Coefficient of correlation between phonemic fluency score and functional connectivity (Zr) of the referenced link.
p<0.05; ** p<0.01; *** p<0.001.
AMD patients with worse phonemic fluency scores exhibited higher levels of rsFC between these links (Fig. 2).
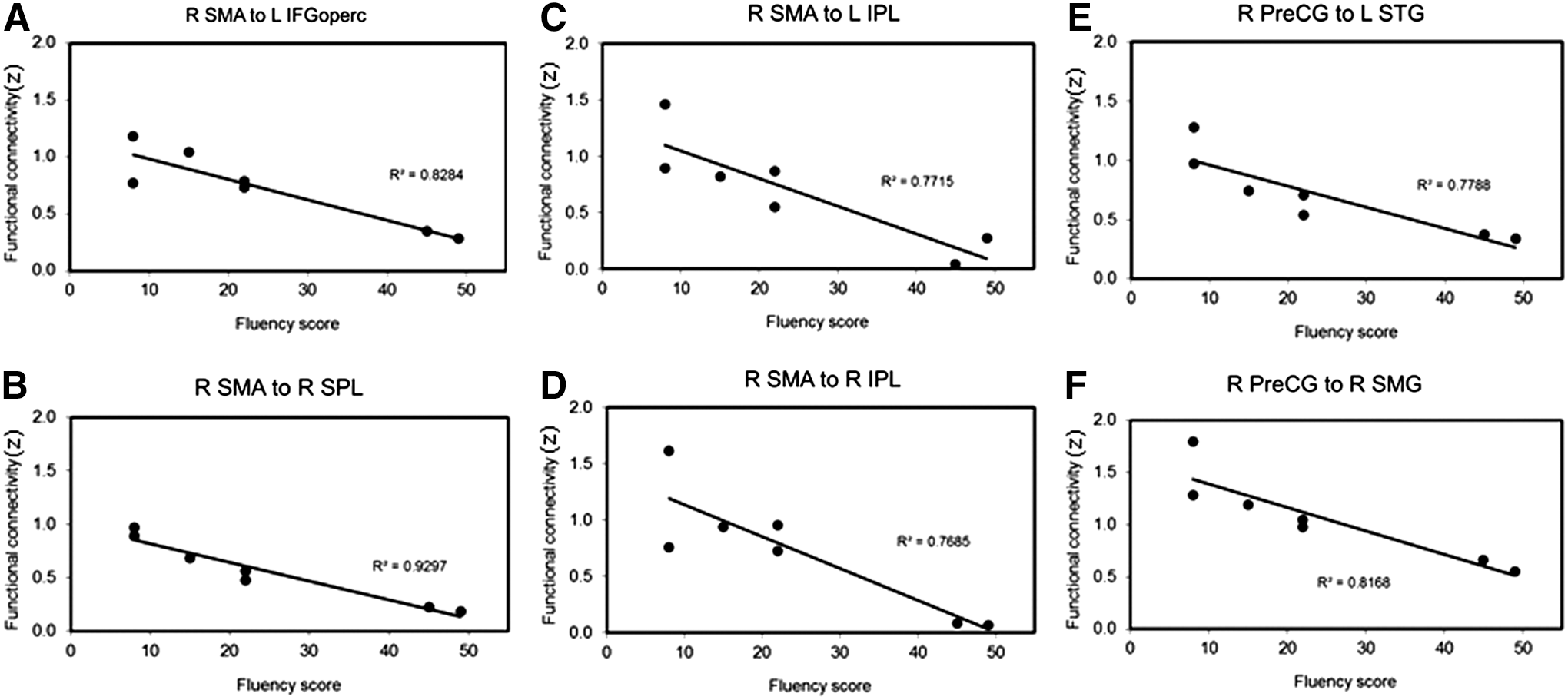
Linear relationships between phonemic fluency score and rsFC of six region pairs
Differences in connectivity strength of the six reference links
Two-way ANOVA with group (AMD, older healthy participants, and younger healthy participants) as a between-subject variable and link (six links identified in the primary analysis) as a within-subject variable, and age and education as covariates, revealed that the mean Zr values of the six BBCA-identified links varied by group (F[2, 180]=6.5, p<0.01) and by link (F[5, 180]=7.6, p<0.0001). The mean Zr values of these six links were significantly greater (p<0.01) in the AMD patients (mean Zr=0.75±0.41) compared with the younger healthy adult group (mean Zr=0.30±0.23) or the older healthy adult group (mean Zr=0.29±0.21). The group×link interaction was also significant (F[10,180]=1.9, p=0.05). The group effect was significant for R PreCG to R SMG and for R SMA to L IFGoperc (with Bonferroni correction), with the Zr of each of the six links greatest among the AMD patients (p<0.01). However, the link effect was only significant within the AMD group (F[5, 30]=8.75, p<0.0001). In the AMD group, the strongest FC was observed between the R preCG and R SMG (mean Zr=1.07±0.41). The FC of the other five links in AMD patients did not differ significantly from each other, with mean Zr ranging from 0.57±0.31 (R SMA to R SPL) to 0.73±0.33 (R SMA to L IFGoperc).
Relationship between FC and phonemic fluency in AMD patients and healthy participants
For each participant, we created a mean Zr value for the six BBCA-identified links. The AMD group exhibited a significant, negative correlation between connectivity (mean Zr) and fluency scores, r=−0.93, p=0.0021. The correlation was unchanged by controlling for the duration (years) of vision loss (r=−0.93, p=0.0069). The FC-fluency relationship was not significant for healthy younger adult participants (r=−0.08, p=0.77), the healthy older adults (r=0.22, p=0.41), or for both groups combined (r=0.06, p=0.40). We then compared the groups on the basis of their Fisher-transformed correlations between the mean Zr values and fluency scores. A z-test of the difference in the correlation coefficients (Cohen and Cohen, 1983) indicated that the FC-fluency correlation exhibited by the AMD group was significantly higher, relative to the older healthy adults (z=3.29, p<0.001) and the younger healthy adults (z=2.76, p<0.01).
DMN analysis
Finally, to assess whether our findings in the AMD population were specific to the BBCA-identified links (or whether phonemic fluency might be inversely associated with FC more globally in the AMD patients), we focused on the DMN. Among the healthy participants, our comparison of younger and older participant groups replicated previous findings of age-related decline in FC among DMN regions (F[1,30]=9.51, p=0.004). However, the AMD patients exhibited significantly stronger DMN connectivity (mean Zr=0.64±0.48) compared with the healthy younger adults (mean Zr=0.39±0.15) and healthy older adults (mean Zr=0.24±0.12). The difference in FC between AMD patients and healthy adults was greatest for these two DMN links: parahippocampal gyrus to lateral parietal cortex and parahippocampal gyrus to posterior cingulate cortex. Including age as a covariate did not alter the observed group effect. Correlations between DMN connectivity and fluency scores were not significant in any group.
Discussion
In this exploratory study of the relationship between phonemic fluency and rsFC in AMD patients, we identified a group of brain regions within which connectivity was strongly associated with AMD patients' fluency. Specifically, AMD patients with stronger connections among these brain regions exhibited worse fluency. The presence of stronger FC among persons with a cognitive-behavioral deficit may seem counter-intuitive, but others have reported increased functional activation and connectivity in aging (Biswal et al., 2010; Reuter-Lorenz, 2002; Tomasi and Volkow, 2012), neuropsychological disease (Greicius et al., 2007; Hawellek et al., 2011; Mensebach et al., 2009), and AMD (Szlyk and Little, 2009). Although the neurobiological foundation of this pattern is unknown, it may reflect increased cognitive effort required to support performance in the context of age-related changes or pathology. Here, the AMD patients exhibited stronger rsFC among the DMN links as well as the BBCA-identified links, compared with the healthy participants.
The rsFC of the links identified in our AMD sample was not correlated with phonemic fluency performance in healthy participants. These exploratory results suggest that the brain connectivity patterns observed in seven AMD patients were not present in healthy participants. However, we are mindful that the scan protocol for the healthy comparisons used for this post hoc analysis differed from the scan protocol used in our pilot study (Table 1). Previous studies have shown that resting-state brain connectivity patterns can be reliably observed with MRI systems of different magnetic field strengths (ranging from 1.5 to 7 T) using a variety of pulse sequences and scan parameters (Barkhof et al., 2014). Therefore, we believe that the between-group difference in brain connectivity patterns observed here was not solely attributable to the difference in acquisition parameters. Nonetheless, our findings need to be further validated.
This finding, although not conclusive with the present sample size and methodological limitations, is consistent with the hypothesis that fluency deficits in AMD patients are associated with a unique brain activity signature. If future work confirms this, then it would suggest that the higher-than-expected rates of cognitive impairment in AMD patients reflect underlying brain changes that are specific to AMD. There are a variety of mechanisms through which AMD could lead to brain changes that would manifest as alterations in FC as well as diminished cognitive ability. AMD-related brain changes could be brought about by loss of cognitively stimulating activities (which is a consequence of sensory impairment), or by adaptive reorganization of visual pathways, or by increased metabolic demand in regions related to effort and concentration, or by loss of positive or negative feedback signaling from visual cortex regions that receive less direct stimulation.
Because efforts to reduce cognitive impairment in AMD depend on a better understanding of its etiology, future research to confirm or refute our findings has important clinical implications. Importantly, more definitive studies that examine the relationship between brain biomarkers and cognitive performance may identify different regional patterns that distinguish AMD patients and their sighted peers. In this proof-of-concept study, we focused on phonemic verbal fluency because several previous studies had administered these tests in AMD populations, providing consistent evidence for deficits (Clemons et al., 2006; Whitson et al., 2010; Wong et al., 2002). Future work should evaluate cognition-connectivity relationships that may exist for AMD-related deficits in other cognitive processes, such as memory or semantic verbal fluency.
The six links identified in the present analysis include several regions known to support language or executive function, and which also may relate to visual processing. We identified two right-sided regions—the right preCG and the right SMA—which were each linked to several language-relevant regions, including Broca's area (in L IFG), Wernicke's area (in L STG), SMG, and the parietal lobes. The SMA and preCG contain primary and supplementary motor cortex, which could be implicated in visual tracking as well as language production. The SMA has been implicated in complex motor-based functions, such as postural stability as well as higher-order executive functions, such as temporal sequencing and planning actions that are internally generated or in response to sensory cues (Halsband et al., 1994; Penfield and Welch, 1951; Picard and Strick, 2003; Roland et al., 1980). More generally, from a recent hierarchical clustering analysis of the BrainMap database, Laird and colleagues (2011) proposed that the SMA, preCG, and SPL grouped together in a “motor/visuospatial” cluster of connectivity networks that support integration, coordination, and execution of visuospatial tasks.
Importantly, the BBCA methodology used in the current study identifies correlated regions that may represent connections either within or between networks (Chen et al., 2009; Chou et al., 2013). We found that AMD patients, but not healthy participants, who exhibited worse fluency had stronger resting-state connectivity between the right preCG and the right SMG (which is involved in language processing) as well as left STG (which likely includes parts of Wernicke's area). The rostral portion of the STG is also believed to play a role in visual input processing by synthesizing object- and space-related information from the dorsal and ventral visual streams (Karnath, 2001). Similarly, AMD patients with poor fluency exhibited stronger connections between the right SMA and the right SPL, both of which are implicated in Laird and coworker (2011) motor/visuospatial cluster, as well as the right SMA and three language-related regions: bilateral IPLs and the opercular portion of left IFG (Broca's area).
One potential interpretation of these findings is that, among AMD patients, poor phonemic fluency is associated with enhanced connectivity between motor/visuospatial networks and language networks. If so, stronger internetwork connectivity could be a cause or a consequence of the observed cognitive deficit. Hypothetically, AMD could result in altered connectivity patterns that, in turn, lead to cognitive changes in these ways; AMD could result in recruitment of new networks to support visually mediated tasks (adaptive plasticity) or stronger internetwork connections due to loss of inhibitory signals that normally result from visual stimulation. AMD-related changes in FC could then have maladaptive effects on cognitive performance, particularly if changes involve regions that play a dual role in visual and cognitive processes. Alternatively, AMD could directly impact cognitive task performance because patients with late-life vision impairment lose many cognitively stimulating activities. In affected patients, increased resting-state brain connectivity, such as we observed, may reflect increased cognitive effort. In the future, longitudinal studies may be helpful in distinguishing among the possible explanations. Ideally, such studies would involve patients with early AMD and examine changes in cognitive function and brain connectivity over time in order to tease out the temporal evolution of the relationship we observed.
Our study has several important limitations. First, these analyses are exploratory, involving a small AMD cohort of seven patients. However, several of the anatomic regions that surfaced in this analysis are clearly implicated in verbal fluency (e.g., Broca's area) and relate to visuospatial processing, which bolsters the face validity of the findings. Second, the AMD patients were heterogeneous with respect to severity, duration, and laterality of visual deficits. In future work, it will be important to consider the independent and interactive effects of these variables on brain connectivity patterns in AMD. Similarly, this small study was not able to consider the effects of potentially important confounders, such as depression or mild cognitive impairment. Third, the AMD group was significantly older than either comparison groups, raising the possibility that observed differences may have been age related rather than AMD related. However, within the DMN we observed the expected age-related decline in connectivity in the healthy participants (Ferreira and Busatto, 2013), whereas connectivity was increased among the AMD patients in the DMN as well as the BBCA-identified links. Fourth, in order to pursue secondary, comparative analyses in this pilot study of brain connectivity in AMD, we utilized existing data previously collected on healthy participants. It is possible that some of the observed cohort differences are influenced by different imaging parameters, study protocols (e.g., eyes closed versus eyes shut, and length of time between cognitive testing and MRI), or patient-level characteristics other than AMD status. Future research is needed to verify whether group-level differences persist when AMD patients are compared with prospectively matched control subjects.
Conclusions
Converging evidence indicates that AMD patients are at increased risk of cognitive decline and, in particular, phonemic fluency deficits. This pilot study is a first step in understanding how cognitive performance relates to brain connectivity patterns in persons with AMD. In seven older adults with AMD, we identified six links among eight brain regions, for which the degree of FC covaried with phonemic fluency. Specifically, greater FC among these regions was associated with worse fluency. We found no evidence that these same links were related to phonemic fluency performance among young or old healthy adults, suggesting that fluency deficits in AMD reflect disease-specific changes in brain connectivity patterns. Further, we found that AMD patients, compared with healthy participants, exhibited stronger FC in these fluency-related regions as well as in the DMN. Our results are consistent with previous reports of increased functional activation and connectivity in some disease states. Further, the results suggest that the AMD-related phonemic fluency deficit may be associated with enhanced connectivity between brain networks that support visual-motor and cognitive processes.
Footnotes
Acknowledgments
This research was supported by NIH research grants K23 AG032867 (H.E.W.), R01 AG043438 (H.E.W.), P30 AG028716 (H.E.W.), R24AG045050 (H.E.W.), R01 AG039684 (D.J.M.), R01 NS074045 (N.k.C.), and R01 AG034138 (M.T.D.). The authors are grateful to support from the Duke Brain Imaging and Analysis Center (BIAC), Allen Song, Director; the Durham VA Geriatric Research, Education, and Clinical Center (GRECC), Kenneth Schmader, Director; and Duke Aging Center, Harvey Cohen, Director.
Author Disclosure Statement
No competing financial interests exist.