
Abstract
Although altered resting-state functional connectivity (FC) is a characteristic of many chronic pain conditions, it has not yet been evaluated in patients with chronic fatigue. Our objective was to investigate the association between fatigue and altered resting-state FC in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Thirty-six female subjects, 19 ME/CFS and 17 healthy controls, completed a fatigue inventory before undergoing functional magnetic resonance imaging. Two methods, (1) data driven and (2) model based, were used to estimate and compare the intraregional FC between both groups during the resting state (RS). The first approach using independent component analysis was applied to investigate five RS networks: the default mode network, salience network (SN), left frontoparietal networks (LFPN) and right frontoparietal networks, and the sensory motor network (SMN). The second approach used a priori selected seed regions demonstrating abnormal regional cerebral blood flow (rCBF) in ME/CFS patients at rest. In ME/CFS patients, Method-1 identified decreased intrinsic connectivity among regions within the LFPN. Furthermore, the FC of the left anterior midcingulate with the SMN and the connectivity of the left posterior cingulate cortex with the SN were significantly decreased. For Method-2, five distinct clusters within the right parahippocampus and occipital lobes, demonstrating significant rCBF reductions in ME/CFS patients, were used as seeds. The parahippocampal seed and three occipital lobe seeds showed altered FC with other brain regions. The degree of abnormal connectivity correlated with the level of self-reported fatigue. Our results confirm altered RS FC in patients with ME/CFS, which was significantly correlated with the severity of their chronic fatigue.
Introduction
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) affects over 1.3 million individuals in the United States and reduces the quality of life to levels comparable to people with congestive heart failure (Komaroff et al., 1996). Treatments for ME/CFS remain largely ineffective at reducing illness-related symptoms. To improve the care of these individuals, a greater understanding of the pathophysiology of ME/CFS is needed. Recent work in this area has examined the role of abnormal immunity as a pathway leading to ME/CFS (Hornig et al., 2015), while less attention has focused on the central mechanisms of persistent fatigue.
Fatigue is a common symptom in the general population, but usually resolves with sleep (Akerstedt et al., 2014). ME/CFS, however, is a condition characterized by disabling fatigue and cognitive abnormalities that seem to be unresponsive to rest. Similar but often less severe fatigue has been reported in other chronic conditions, such as depression, arthritis, and chronic pain, where symptoms persist for long periods of time (Katz et al., 2015; Kroenke et al., 2011; Maes et al., 2012).
With advances in neuroimaging, the brain's role in persistent conditions, like ME/CFS, has become an important focus of research. Previous investigations of brain abnormalities in ME/CFS were mostly inconclusive (Lange et al., 1998). There is conflicting evidence for altered brain structure in this illness, with some studies reporting either globally decreased gray matter or local abnormalities in several brain regions (Puri et al., 2012 and Okada et al., 2004), while others report no such findings (Perrin et al., 2010).
Global or regional reductions in cerebral blood flow (CBF) at rest have been reported in ME/CFS (Biswal et al., 2011; Cope and David, 1996; Tirelli et al., 1998; Yoshiuchi et al., 2006), but some investigators found no group differences in CBF compared to normal controls (Perrin et al., 2010). However, functional MRI (fMRI) has shown altered cortical activation during cognitive challenges in ME/CFS (De Lange et al., 2004; Tanaka et al., 2006).
Resting-state functional connectivity (FC) is often disrupted in chronic conditions, such as fibromyalgia, back pain, and temporomandibular joint disorder, and may contribute to prolonged symptoms (Baliki et al., 2011; Ichesco et al., 2014; Schmidt-Wilcke et al., 2014; Tagliazucchi et al., 2010). However, FC is yet to be investigated in patients with ME/CFS. Examining FC between brain areas in the absence of a task (i.e., resting state [RS]) may offer some insights as to why such patients have considerable difficulty in performing challenging tasks, such as the Psychomotor Vigilance Test (Lim et al., 2010).
Two general approaches can be used to evaluate the FC among brain regions. One requires prior knowledge of seed regions (i.e., model based), while the other is driven by the acquired data (i.e., data driven). The results of these approaches are complementary and, when combined, may provide powerful insights about the neural underpinnings of clinical disorders, like ME/CFS.
In this study, we used both approaches to assess FC in patients with ME/CFS. Our data-driven approach was similar to the one used in patients diagnosed with fibromyalgia (Napadow et al., 2010). We investigated FC among brain regions in ME/CFS patients and normal nonfatigued healthy controls (HC) in five resting-state networks (RSN): the default mode network (DMN), salience network (SN), sensory motor network (SMN), and the left and right frontoparietal networks (LFPN, RFPN). We hypothesized that self-reported fatigue would be associated with altered FC within these networks. Moreover, compared to HC, we expected the RS among ME/CFS patients to connect to additional brain regions such as the insula, parietal, and frontal lobes.
For the second set of analyses, we used the model-based approach to test FC among brain regions, using seed regions that had demonstrated decreased resting regional cerebral blood flow (rCBF) in ME/CFS patients through arterial spin labeling (ASL). Those regions were located in the parahippocampal and occipital lobes. Given the reductions in rCBF within these brain clusters, we expected the FC with other brain regions to be disrupted and associated with reports of fatigue in patients with ME/CFS.
Methods and Procedures
Participants
Individuals with chronic fatigue who fulfilled the 1994 Case Definition (Fukuda et al., 1994) as well as the 2003 Canadian Criteria for ME/CFS were recruited from outpatient clinics at the University of Florida. Only female subjects were enrolled because of the preponderance of women in ME/CFS. Following the recruitment of clinical subjects, nonfatigued healthy individuals were invited to participate through local advertising to serve as age- and sex-matched controls. Subjects with a history of heart disease, COPD, malignancy, or other systemic disorders were excluded, including those with psychiatric illnesses that would be exclusionary for a diagnosis of ME/CFS (Reeves et al., 2003). The work described in this article was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. All participants provided informed consent before participation. The University of Florida Institutional Review Board approved all study procedures before the start of study enrollment.
Multidimensional fatigue inventory
The multidimensional fatigue inventory (MFI) is a self-reported instrument that contains 20 statements covering different aspects of fatigue (Smets et al., 1995). The 20 items are organized into 5 scales: general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue. Higher scores on the questionnaire indicate more fatigue.
Neuroimaging
Acquisition
All neuroimaging data were acquired with a research-dedicated Philips Achieva 3T whole body MRI scanner using a 32-channel head coil. Three types of data were obtained during a single scanning session: (A) A high-resolution 3D anatomic structural scan; (B) a resting-state ASL scan; and (C) a blood oxygen level-dependent (BOLD) resting-state scan. The parameters for the anatomical T1-weighted MPRAGE structural scan were as follows: 176 slices in sagittal orientation, TR = 7 msec, TE = 3.2 msec, acquisition matrix = 240 mm × 240 mm, and voxel size =1 mm3. The ASL sequence used a pseudocontinuous ASL design with the following parameters: 20 slices in transverse orientation, slice gap = 1 mm, TR = 4000 msec, TE = 11 msec, label duration = 1500 msec, postlabel delay = 1800 msec, acquisition matrix = 72 mm × 72 mm, voxel size = 3.19 mm ×3.19 mm × 6 mm, and number of dynamic scans (pairs) = 45. Finally, the resting-state BOLD scans were acquired using an echo planar acquisition protocol with the following parameters: 42 slices in transverse orientation, slice gap =0 mm, TR = 2250 msec, TE = 30 msec, acquisition matrix =80 mm × 80 mm, and 3 mm isotropic voxels. The RS ASL scans were obtained to identify brain areas demonstrating rCBF differences between ME/CFS subjects and NC to be subsequently used as seeds in our model-based approach.
Resting-state CBF
Statistical Parametric Mapping 8 (SPM8) (Wellcome Department of Imaging Neuroscience, London, United Kingdom;
SPM12 was used to perform independent sample t-tests to compare CBF between the ME/CFS and HC groups. Contrasts were created to identify cortical regions where CBF was increased or decreased in clinical subjects compared to controls. These contrasts produce maps with a t-statistic for every voxel in the brain. The resulting t maps were thresholded at a t-statistic of p < 0.001 and a cluster size of 120 mm3 to control for the large number of multiple comparisons associated with voxelwise analyses.
BOLD data preprocessing
Functional imaging data were preprocessed in SPM12 (Wellcome Department of Imaging Neuroscience;
Data-based approach to RS network analysis
For the data driven analyses, an additional preprocessing step included smoothing the fMRI data with a 6 mm FWHM Gaussian kernel. The next step in the data-driven approach was done with the Group independent component analysis (ICA) of fMRI Toolbox (GIFT v3.0a;
Model-based approach to RS network analysis
For the model-based approach, additional preprocessing steps included spike correction to reduce the impact of artifacts using the postprocessing artifact detection tool (ART) toolbox for fMRI data (
Selection of a priori seed regions is a critical step in the model-based approach. For this study, we used brain regions where there was a significant reduction in CBF identified by ASL scanning, as our seeds, see Table 2. Binary masks of clusters (identified by ASL) were created and used as our seed region of interest (ROI) and overlaid with a gray matter mask to include only gray matter voxels. The time course was then estimated by the spatial average of the BOLD signal over all voxels at each time point within each ROI. Zero-order Cross Correlation coefficients (CC) (i.e., bivariate correlation) for each ROI's time course between the ROI time course and the rest of the brain were estimated using the Conn_v14 toolbox.
Group-level differences between seed and voxel-based FC
Contrasts for each of the previously identified seed regions were created to distinguish brain regions of ME/CFS subjects showing differential connectivity from those of controls. Each contrast produced a map with a t-statistic for every voxel in the brain. These contrasts were used to identify brains regions, where the strength of FC (CC) differed between groups. The strength of FC estimates the extent to which fluctuations in BOLD signal (interpreted as brain activity) between two regions are coupled. Typically, values range from −1 to 1. Values closer to 1 (or −1) suggest greater coupling, while values closer to 0 suggest less coupling. Negative values suggest anticoupling. To keep the familywise error rate at 5%, a permutation-based extent and cluster thresholding method was used, see Correction for Multiple Comparisons section.
Correction for multiple comparisons
The statistical result of each method (i.e., data driven and seed based) was corrected for multiple comparisons using AlphaSim (see the AlphaSim command description at
Correlations between clinical fatigue and FC
The Pearson's CC was used to characterize the relationship between fatigue and the strength of connectivity between seed regions and clusters of voxels that showed significant group differences. To extrapolate each subjects' mean strength of connectivity within a significant cluster, we used the response exploration software (REX, alpha 0.5) (available at
Results
Subject characteristics
Thirty-six females (19 ME/CFS, 17 HC) with a mean age of 48.75 years (SD = 11.75 years) volunteered for this study. Table 1 provides descriptive data on the sample, including the five domains of fatigue identified by the MFI: general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue. Significant group differences were found for all fatigue measures (Table 1).
Descriptive Statistics of Participants
All participants were female; variables are presented as mean and standard deviation.
Item of the multidimensional fatigue inventory (MFI).
HC, healthy controls; ME/CFS, myalgic encephalomyelitis/chronic fatigue syndrome.
Resting-state CBF
Using ASL, subjects with ME/CFS demonstrated reduced rCBF at rest when compared to control subjects in several clusters located within the occipital (right cuneus, inferior occipital gyrus, and left lingual gyrus) and temporal lobes (right parahippocampal gyrus) (Table 2). No cortical regions had increased rCBF in subjects with ME/CFS compared to control subjects. There was, however, no significant difference in global CBF between groups.
Brain Regions Used as Seeds for Functional Connectivity Analysis (Model-Based Approach)
Threshold t-statistic p < 0.001 and a cluster size (k) of 120 mm3.
x, y, and z coordinates are in Montreal Neurologic Institute (MNI) space.
RH, right hemisphere; LH, left hemisphere.
Data-based FC
A group-level ICA was used for the evaluation of each of the five RSNs (Fig. 1). Compared to HC, ME/CFS was associated with disrupted intrinsic connectivity within the left frontoparietal network. More specifically, a region in the left superior frontal gyrus, which is a major node of this network, showed reduced coupling of activity with the rest of the network. ME/CFS was also associated with decreased connectivity between the SN and the left PCC; similarly, the SMN demonstrated decreased connectivity with the left anterior midcingulate cortex (aMCC) compared to HC (Fig. 1). No differences in FC were found within the DMN or RFPN (Table 3).
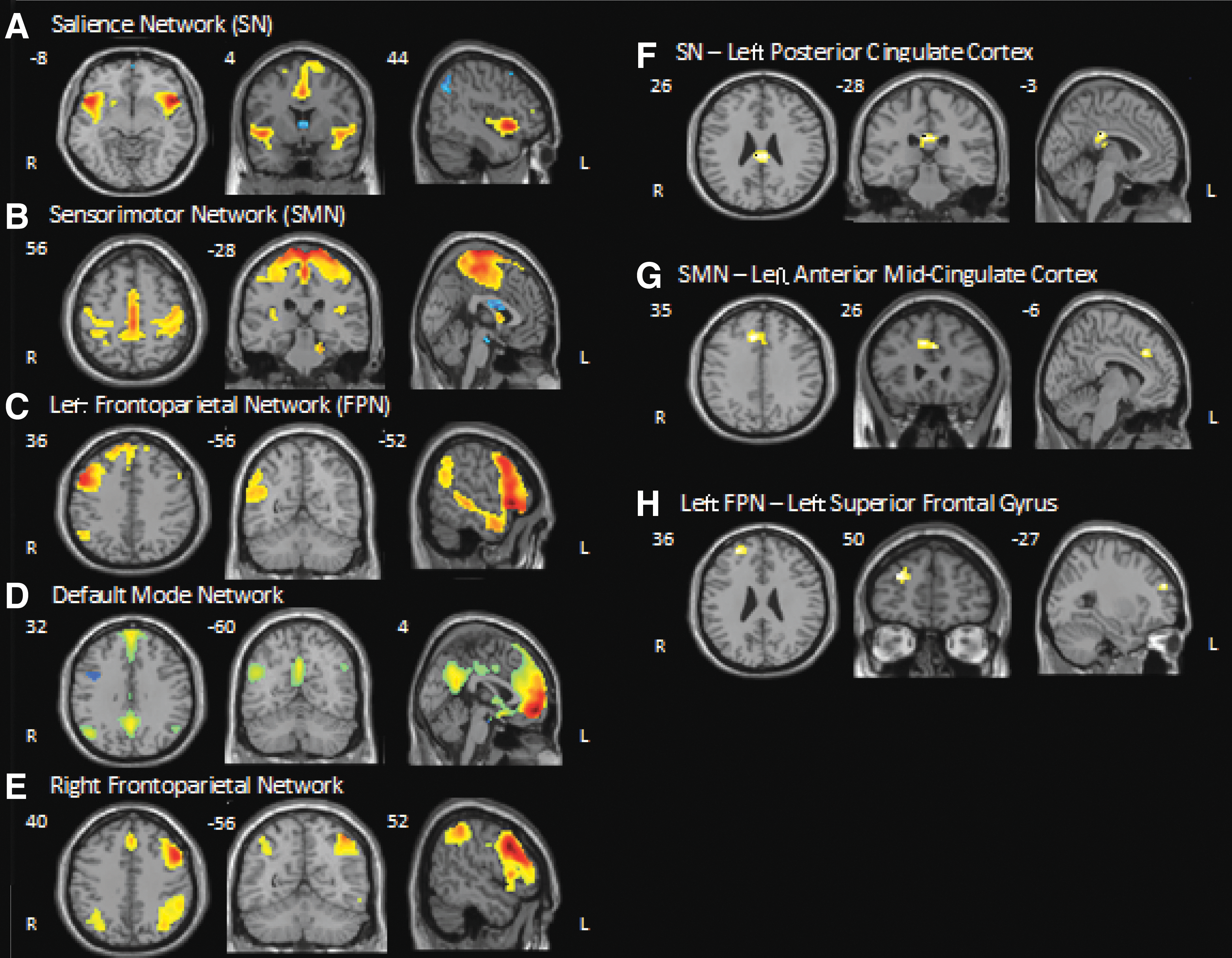
Spatial maps of resting-state networks and regional group differences in functional connectivity threshold t > 4.0; k > 15. R = Right, L = Left, x, y, and z coordinates are in Montreal Neurologic Institute space.
Brain Regions Showing Reduced Functional Connectivity (Data-Based Approach) in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Subjects
Threshold t-statistic of 4.0 and a cluster size (k) of 60 mm3.
x, y, and z coordinates are in MNI space.
FPN, frontoparietal network; RSN, resting-state network; SMN, sensory motor network; SN, salience network.
Data-based FC as predictor of fatigue
As all data met normalcy criteria (see Correlations Between Clinical Fatigue and FC section), Pearson's product moment correlations were used. The strength of connectivity between each of the disrupted regions was significantly correlated with self-reported fatigue ratings of the MFI, including general fatigue, physical fatigue, motivation, and mental fatigue (Table 4). The direction of all three relationships was negative, suggesting stronger FC is associated with less severe symptoms of fatigue.
Correlations Between Degree of Functional Connectivity and Self-Reported Fatigue in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Subjects
Item of the MFI.
p < 0.01.
p < 0.05.
aMCC, anterior midcingulate cortex; L, left; FPN, frontoparietal network; PCC, posterior cingulate cortex.
Model-based FC
Brain areas demonstrating rCBF abnormalities in ME/CFS subjects during RS ASL were used as a priori seeds for this analysis. Of the five seed regions, all but the right inferior occipital seed (seed 4) showed altered FC with other regions of the brain (Fig. 1). ME/CFS was associated with decreased FC between the right cuneus (seed 1) and a region in the right superior temporal gyrus; the left lingual gyrus (seed3) and regions located in the left occipital lobe and right precuneus; and the second right cuneus seed (seed 5) and regions within the right superior midfrontal gyrus and left midfrontal gyrus. Increased FC was found between the right parahippocampus (seed 2) and the right inferior parietal lobe (Table 5).
Brain Clusters Demonstrating Altered Functional Connectivity with Seed Regions in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Subjects
Threshold uncorrected p < 0.001; k > 15.
x, y, and z coordinates are in MNI space.
BA, Brodman area; k, cluster size; t, t-value; ME/CFS, myalgic encephalomyelitis/chronic fatigue syndrome.
Model-based connectivity as predictor of fatigue
As all data met normalcy criteria (see Correlations Between Clinical Fatigue and FC section), Pearson's product moment correlations were used. A significant relationship was found between the strength of connectivity and self-reports of fatigue obtained with the MFI for all disrupted seed-to-brain region pairs (Table 6). For the majority of seed-to-brain region pairs, ME/CFS subjects showed negative correlations with FC. Only for the seed-to-brain region pair (right parahippocampus to right inferior parietal lobe) a positive relationship with fatigue was observed in ME/CFS subjects.
Correlation Between Degree of Functional Connectivity and Self-Reported Fatigue in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Subjects
Item of the MFI.
p < 0.01.
p < 0.05.
Seed 1: cluster 1, RH cuneus—RH superior temporal gyrus; Seed 2: cluster 1, RH parahippocampus—RH inferior parietal lobe; Seed 3: cluster 1, LH lingual gyrus—LH occipital lobe; Seed 3: cluster 2, LH lingual gyrus—RH precuneus; Seed 5: cluster 1, RH cuneus—RH superior midfrontal gyrus; Seed 5: cluster 2, RH cuneus—LH middle frontal gyrus.
Discussion
To identify neural correlates of self-reported fatigue, we compared patterns of resting-state FC of ME/CFS patients with age–sex-matched normal control subjects. To obtain complementary information on FC of multiple brain networks in ME/CFS, two different methods of analysis were used: (1) ICA depends on statistical associations of neural activity between brain areas and (2) a seed-based approach exploring the associations of brain activity with a priori determined brain areas. Our results demonstrate that ME/CFS is associated with altered resting-state FC of several brain networks, and the degree of altered connectivity is significantly related to self-reported fatigue. Both approaches showed ME/CFS to be associated with decreased intrinsic connectivity in the LFPN and with decreased connectivity between regions in the cingulate cortex and the SMN and SN.
Neural networks encompassing multiple brain regions show synchronized activity at rest (Beckmann et al., 2005; Damoiseaux et al., 2006; De Luca et al., 2006; Salvador et al., 2005; van den Heuvel and Hulshoff Pol, 2010). The FPN is one of these networks that is composed of lateral prefrontal regions and inferior parietal cortices and often shows lateralization into right and left components (Beckmann et al., 2005; Damoiseaux et al., 2006; Di and Biswal, 2015; Smith et al., 2009). This RSN is implicated in cognitive control, attention, language processing, and working memory (Lois et al., 2014) and links the bilateral insular regions and anterior cingulate cortex (Dosenbach et al., 2007). Coherent activation between the FPN and the DMN has been suggested to play an important role in salience processes of human cognition (Fox and Raichle, 2007; Gusnard et al., 2001), including mind wandering (Mason et al., 2007), goal-directed behavior (Dosenbach et al., 2007), and relating oneself to the outside world (Gusnard et al., 2001). Considerable evidence suggests that the FPN, in particular the left FPN, plays a pivotal gate-keeping role in goal-directed cognition, mediating the dynamic balance between DMN and dorsal attention networks (Spreng et al., 2013; Vallesi et al., 2015; Vincent et al., 2008). Less FC within the left FPN, which was seen in ME/CFS patients, may be an important feature of the condition that needs more research to fully understand its role.
The SN mainly consists of the insular cortex and anterior cingulate cortex. This RSN is involved in a wide range of functions such as detection of salient stimuli, interoception, audition, pain, deception, music, and classical conditioning (Borsook et al., 2013; Kucyi and Davis, 2015). Because of the heterogeneous range of functions, the SN has been considered a transitional network linking cognition and emotion/interoception (Lois et al., 2014; Smith et al., 2009). The SN causally influences the DMN and FPN. It also mediates the “switching” between activation of the DMN and of the FPN and executive control networks to guide appropriate responses to salient stimuli (Uddin, 2015). In our study, there was decreased FC of ME/CFS patients between the SN and PCC, which is a key node of the DMN. Less effective connectivity between these regions was strongly associated with more fatigue. Therefore, it appears that decreased FC between these regions may be indicative of decreased drive to guide thoughts away from self-referential experience of fatigue toward externally directed cognition.
The SMN includes primary sensory motor cortices and is associated with action and somesthesis (Lois et al., 2014). ME/CFS participants showed reduced connectivity between this RSN and the aMCC. The aMCC has a key role for cognitive aspects of movement generation, that is, intentional motor control (Hoffstaedter et al., 2014). We found that fatigue strongly predicted an inverse relationship of FC between this RSN and the aMCC. Further research is required to better understand the altered relationship of the SMN and aMCC with ME/CFS. Taking into account ME/CFS patients' impaired physical, affective, and cognitive functions and the decreased connectivity between the spatial maps of these RSNs, it can be argued that patterns of FC within or between these networks may be impaired in ME/CFS (Laird et al., 2011). We believe that our findings shed new light on the understanding of chronic fatigue across individuals and how the intrinsic connectivity of the brain is influenced by ME/CFS patients' symptoms.
Our seed-based approach was predicated on brain regions that had demonstrated altered function during ASL imaging, as evidenced by reduced rCBF. It demonstrated that the parahippocampus and occipital lobes of ME/CFS patients have altered FC. Although we are the first to report abnormal resting-state FC in patients with ME/CFS, others have described altered structure and task-related dysfunction within some of the same regions using other imaging modalities (Cook et al., 2007; De Lange et al., 2005; Okada et al., 2004). In addition, utilizing diffusion tensor imaging researchers found disrupted white matter connectivity along the right inferior fronto-occipital fasciculus in veterans with gulf war syndrome, which was marked by severe levels of fatigue and malaise (Rayhan et al., 2013). The right inferior fronto-occipital fasciculus connects posterior brain structures such as the parahippocampus and occipital lobe with anterior brain structures. Our results would support such disrupted tracts because the relationship of brain activity between posterior brain structures and intermediate structures is decreased in ME/CFS patients. Similarly, a previous study reported that multiple sclerosis patients who reported significant levels of fatigue had decreased cortical activity within the precuneus, cuneus, and middle frontal gyrus compared to MS patients without fatigue (Filippi et al., 2002).
The DMN, the most commonly studied RSN, comprises the precuneus/PCC, the medial frontal cortex, and bilateral inferior parietal regions (Fox and Raichle, 2007; Greicius et al., 2009; Gusnard et al., 2001). Activity and connectivity of the DMN have been linked to central processes of human cognition, including integration of cognitive as well as emotional brain activity (Greicius et al., 2009), monitoring of the environment (Gusnard et al., 2001), and mind wandering (Mason et al., 2007). Abnormalities of DMN connectivity have been reported in attention deficit disorder, multiple sclerosis, and Alzheimer's disease, all of which demonstrate overlapping clinical features with ME/CFS, including attention and memory difficulties. Surprisingly, we did not find fatigue-related DMN abnormalities. The DMN can be represented as a single IC or it can split into two or three components. Such a decomposition is frequently observed with separation into anterior and posterior networks (Uddin et al., 2009 and Laird et al., 2009). In our study, we choose the components that best fit the spatial template of a typical DMN. Retrospective examination of all components, however, showed three that resembled aspects of the DMN. The ability of networks to split into more than one component is a limitation of our applied methods and may explain why the DMN did not show altered connectivity between ME/CFS and HC groups.
Limitations
Some caution needs to be exercised when interpreting our results, as our sample only included female participants. Although ME/CFS affects more women than men, our results may not be applicable to males. Second, our model-based results are dependent on our seed selection method. While other researchers may use alternative seed regions for connectivity analyses, we empirically chose our seeds according to a priori detected rCBF abnormalities in ME/CFS. This approach of seed selection allowed us to focus on brain regions clearly associated with ME/CFS. Group-dependent rCBF findings provide a rationale to explore FC between those regions and the rest of the brain.
Conclusions
ME/CFS appears to be a chronic illness that affects several different brain areas and is associated with abnormal neuronal connectivity. Using two different methods of analysis, significant differences in resting-state FC were detected between ME/CFS and HC. Furthermore, these changes were significantly correlated with self-reported levels of fatigue. Additional neuroimaging studies will be necessary to better understand the contributions of these brain regions to ME/CFS.
Footnotes
Acknowledgments
The expert assistance of Ricky Madhavan and Yesenia M. Lucas is gratefully acknowledged.
This study was supported by NIH grant R01 NR014049-01 and NIH/NCATS Clinical and Translational Science grants UL1 TR000064. CWG was supported by NIH training grant F32AT007729.
Author Disclosure Statement
None of the authors have any financial or other relationships that might result in a conflict of interest.