
Abstract
The aim of this study is to determine whether regional homogeneity (ReHo) of resting-state blood oxygenation level-dependent (BOLD) functional magnetic resonance imaging (rsfMRI) data based on Kendall's coefficient of concordance (KCC-ReHo) and coherence (Cohe-ReHo) metrics may allow detection of brain tumor-induced neurovascular uncoupling (NVU) in the sensorimotor network similar to findings in standard motor task-based BOLD fMRI (tbfMRI) activation. Twelve de novo brain tumor patients undergoing clinical fMRI exams (tbfMRI and rsfMRI) were included in this Institutional Review Board (IRB)-approved study. Each patient displayed decreased/absent tbfMRI activation in the primary ipsilesional sensorimotor cortex in the absence of corresponding motor deficit or suboptimal task performance, consistent with NVU. Z-score maps for motor tasks were obtained from the general linear model (GLM) analysis (reflecting motor activation vs. rest). KCC-ReHo and Cohe-ReHo maps were calculated from rsfMRI data. Precentral and postcentral gyri in contralesional (CL) and ipsilesional (IL) hemispheres were parcellated using an automated anatomical labeling (AAL) template for each patient. Similar region of interest (ROI) analysis was performed on tbfMRI, KCC-ReHo, and Cohe-ReHo maps to allow direct comparison of results. Voxel values in CL and IL ROIs of each map were divided by the corresponding global mean of KCC-ReHo and Cohe-ReHo in bihemispheric cortical brain tissue. Group analysis revealed significantly decreased IL mean KCC-ReHo (p = 0.02) and Cohe-ReHo (p = 0.04) metrics compared with respective values in the CL ROIs, consistent with similar findings of significantly decreased ipsilesional BOLD signal for tbfMRI (p = 0.0005). Ipsilesional abnormalities in ReHo derived from rsfMRI may serve as potential indicators of NVU in patients with brain tumors and other resectable brain lesions; as such, ReHo findings may complement findings on tbfMRI used for presurgical planning.
Introduction
B
In recent years, there has been increasing interest in the application of rsfMRI for presurgical planning in patients with brain tumors. Studies have documented various advantages of rsfMRI over conventional task-based BOLD fMRI (tbfMRI) in presurgical planning (Fukunaga et al., 2006; Shimony et al., 2009). One important advantage is that it does not require patient cooperation for specific task performance; therefore, rsfMRI is particularly useful in patients who are not able to perform cognitive or other prescribed tasks during conventional tbfMRI scanning. In addition, rsfMRI can identify many networks such as the sensorimotor, visual, and default mode networks (DMNs) simultaneously during a single scan acquisition, therefore reducing overall scanning time when information from multiple networks is needed (Beckmann et al., 2005; Damoiseaux et al., 2006; Kiviniemi et al., 2003; Seeley et al., 2007; Smith et al., 2009).
However, in the setting of brain tumors, reliability of BOLD imaging, including task-based and resting-state BOLD fMRI, suffers because of impaired BOLD signal response. This impaired BOLD signal is due to the phenomenon known as neurovascular uncoupling (NVU) (Attwell et al., 2010; Holodny et al., 2000). NVU occurs due to the disruption of coupling between neuronal activity and adjacent neurovascular response in the vicinity of brain tumors or other focal brain lesions. NVU can produce false-negative or abnormally decreased BOLD signals, which in turn can lead to inaccurate presurgical planning and resultant possible inadvertent eloquent cortical resection. This phenomenon has been established in tbfMRI (Holodny et al., 2000; Ulmer et al., 2003; Zacà et al., 2014).
Very recently, a few publications (Agarwal et al., 2016a, 2016b; Mallela et al., 2016) have demonstrated similar impaired BOLD responses in rsfMRI due to brain tumor-induced NVU. Studies by Agarwal et al. (2016b) have demonstrated that tumor-related NVU can adversely affect the resting-state BOLD signal similar to its effect on task-based BOLD activation. They assessed brain tumor-related NVU quantitatively using two standard rsfMRI analysis methods—ICA (independent component analysis) and seed-based correlation analysis (SCA)—in a group of patients with perirolandic primary glial neoplasms.
Another study demonstrated that brain tumor-related NVU may also similarly affect rsfMRI at ultrahigh field (7 Tesla) despite the higher signal-to-noise ratio afforded by higher field strength (Agarwal et al., 2016a). Mallela et al. (2016) have examined the correlation of rsfMRI data with tumor characteristics and clinical information to characterize functional reorganization of resting-state networks (RSNs) and the limitations of this method in high-grade gliomas due to NVU. Thus, practical application of rsfMRI for presurgical planning should take into account the possibility of NVU to ensure mapping accuracy.
Analysis methods such as SCA and ICA focus on the similarities of inter-regional time series and therefore investigate temporal synchronization of low- frequency fluctuations, that is, functional connectivity between various regions. More recently, Zang et al. (2004) proposed regional homogeneity (ReHo) metrics of rsfMRI signals as a voxel-based measure of brain activity, which evaluates the synchronization between the time series of a given voxel and its nearest neighbors. This measure was based on the hypothesis that intrinsic brain activity is manifested by clusters of voxels rather than single voxels. They used Kendall's coefficient of concordance (KCC) (Kendall and Gibbons, 1990) as an index to evaluate the similarity of the time series within a cluster of a given voxel and its nearest neighbor voxels in healthy subjects.
Later, Liu et al. (2010) applied coherence to voxel-wise measurement of regional homogeneity of rsfMRI signals (Cohe-ReHo) in healthy participants as well as in patients with attention-deficit/hyperactivity disorder (ADHD). However, no study to date has examined the utility of these voxel-wise measurements of regional homogeneity of rsfMRI signals (KCC-ReHo and Cohe-ReHo) in the assessment of brain tumor-induced NVU.
In our current study, we aim to explore whether the regional homogeneity of rsfMRI data based on KCC-ReHo and Cohe-ReHo allows detection of brain tumor-induced NVU in the sensorimotor network, and compare the ReHo results with those of standard motor tbfMRI activation.
Materials and Methods
Patients
Twelve de novo (i.e., treatment naïve) brain tumor patients referred for routine clinical presurgical motor mapping with BOLD fMRI were included in this Institutional Review Board (IRB)-approved study. These patients demonstrated evidence of potential NVU based on results of their clinical task-based BOLD fMRI scans as described in previous publications (Zacà et al., 2014). In every patient, decreased/absent tbfMRI activation in the primary ipsilesional sensorimotor cortex without associated clinical deficits was highly suggestive of NVU. All these patients presented with primary perirolandic gliomas with NVU affecting the face or hand representation area of the primary sensorimotor cortex.
Table 1 presents clinical and demographic data for 12 patients recruited for the study.
F, female; M, male.
MRI acquisition
Scanning was performed using our standard clinical sequences for fMRI studies on a 3.0 Tesla Siemens Trio MRI system (Siemens Medical Solutions, Erlangen, Germany) equipped with a 12-channel head matrix coil. Imaging protocol included a three-dimensional, T1-weighted imaging sequence (repetition time [TR] = 2300 ms, inversion time [TI] = 900 ms, echo time [TE] = 3.5 ms, flip angle = 9°, field of view = 24 cm, acquisition matrix = 256 × 256 × 176, slice thickness = 1 mm) as well as an axial, two-dimensional, (2D) T2 fluid-attenuated inversion recovery (FLAIR) imaging sequence (TR = 9000 ms, TI = 2500 ms, TE = 116 ms, flip angle = 141°, field of view = 17.2 × 23 cm, acquisition matrix = 240 × 320 × 53, slice thickness = 3 mm with 3-mm gap between slices) for structural imaging and multiple 2D gradient-echo echo-planar imaging (GE-EPI) T2*-weighted BOLD sequences for functional imaging (TR = 2000 ms, TE = 30 ms, flip angle = 90°, field of view = 24 cm, acquisition matrix = 64 × 64 × 33, slice thickness = 4 mm with 1-mm gap between slices, interleaved acquisition) run while patients were performing a motor paradigm as described in more detail in the following subsection.
For resting-state fMRI, 180 volumes were acquired using the same functional imaging protocol. For the resting-state fMRI acquisition, each patient was instructed to remain still with eyes closed without falling asleep during the scanning period of 6 min.
Note that we coregistered (normalized) the anatomical data of each patient to the MNI-152 template. For simplicity, throughout the rest of the article, we refer to these normalized T1-weighted images as T1-weighted images.
Task-based motor activation maps (tbfMRI)
All patients performed one or more motor tasks for sensorimotor activation mapping during scanning. To map the face representation area of the primary motor cortex, a 3-min-long tongue movement task was used, consisting of three cycles of 30-sec blocks of rest alternating with 30-sec blocks of repetitive vertical tongue movement. The hand representation area was mapped using a 3-min duration finger-tapping task, consisting of three cycles of 30-sec blocks of rest alternating with 30-sec blocks of bilateral simultaneous sequential finger tapping.
Instructions for all tasks were visually cued. A comprehensive prescan training session outside the MRI scanner ensured full patient understanding of task instructions and confirmed each patient's ability to adequately perform each of the tasks. Patient task performance was monitored during the scan through the use of both an LCD monitor in the scan suite for observation of finger tapping and real-time fMRI for assessment of brain activation, head motion, and physiological noise.
SPM12 software was used for preprocessing and postprocessing of tbfMRI data. As preprocessing steps, fMRI raw data were slice-time corrected, spatially realigned to correct for head motion, normalized to MNI space at 2 mm voxel resolution, and spatially smoothed using a 6-mm isotropic full-width at half-maximum (FWHM) Gaussian filter. The maximum spatial displacement from the volume taken as reference during motion correction calculation was <1.0 mm and <1° of rotation was present in all cases (less than one voxel size in each direction) and therefore no data were discarded (Breiter et al., 2001).
Preprocessed tbfMRI data were then analyzed using the standard SPM canonical hemodynamic response function (HRF) (reflecting motor activation vs. rest). A voxel-wise general linear model (GLM) analysis was performed with the expected BOLD response modeled by convolving the stimulus corresponding to each paradigm with a canonical HRF. From results of the GLM analysis, standard activation maps, expressed as T-value maps for the motor tasks, were created. Z-scores were then calculated from the obtained T-value maps.
Resting-state ReHo analysis
SPM12 software was used for preprocessing of rsfMRI data. As preprocessing steps, rsfMRI raw data were slice-time corrected, spatially realigned to correct for head motion, and normalized to MNI space at 2 mm voxel resolution.
Preprocessed rsfMRI data were analyzed using the REST (version 1.8) (Song et al., 2011) toolkit. After detrending (for removal of systematic linear trend) and low-frequency (0.01–0.08 Hz) bandpass filtering of preprocessed rsfMRI data, KCC-ReHo and Cohe-ReHo maps were calculated for each patient. We used cluster size of 27 voxels to include all the neighboring voxels adjacent to a given voxel. Spatial smoothing was performed using a 6-mm isotropic FWHM Gaussian filter on KCC-ReHo and Cohe-ReHo maps. For region of interest (ROI) analysis, precentral and postcentral gyri were automatically parcellated using an automated anatomical labeling (AAL) template (Smith, 2002; Tzourio-Mazoyer et al., 2002). Contralesional (i.e., contralateral to tumor [CL]) ROIs and ipsilesional (i.e., ipsilateral to tumor [IL]) ROIs circumscribing the combination of precentral and postcentral gyri were obtained for each consecutive imaging slice along the z-axis in MNI space for each patient. The purpose of ROIs was to limit evaluation to the primary motor and somatosensory cortex. ROIs were then visually inspected to ensure that they encompassed the precentral and postcentral gyri even in the presence of tumor-induced regional mass effects and gyral expansion. Consecutive axial sections were evaluated along the z-axis along the full craniocaudal extent of the tumor as seen on T1-weighted images. Identical ROIs were used for analysis of tbfMRI, KCC-ReHo, and Cohe-ReHo maps to allow comparison of results from these three spatial maps.
Results
Example of analysis for three patients included in this study is provided in Figure 1. This figure displays results of thresholded task-based activation map, KCC-ReHo map, and Cohe-ReHo map, all overlaid on T1-weighted anatomic images in each case. The selected IL and CL ROIs are also shown. In all maps, there is abnormally decreased signal in the ipsilesional perirolandic ROIs (IL) compared with the normal contralesional perirolandic ROIs (CL). In the setting of preserved clinical motor function and excellent task performance, these findings are indicative of tumor-induced NVU. Figures for the remaining 9 cases are provided as Supplementary Figures S1–S9 (Supplementary Data are available online at
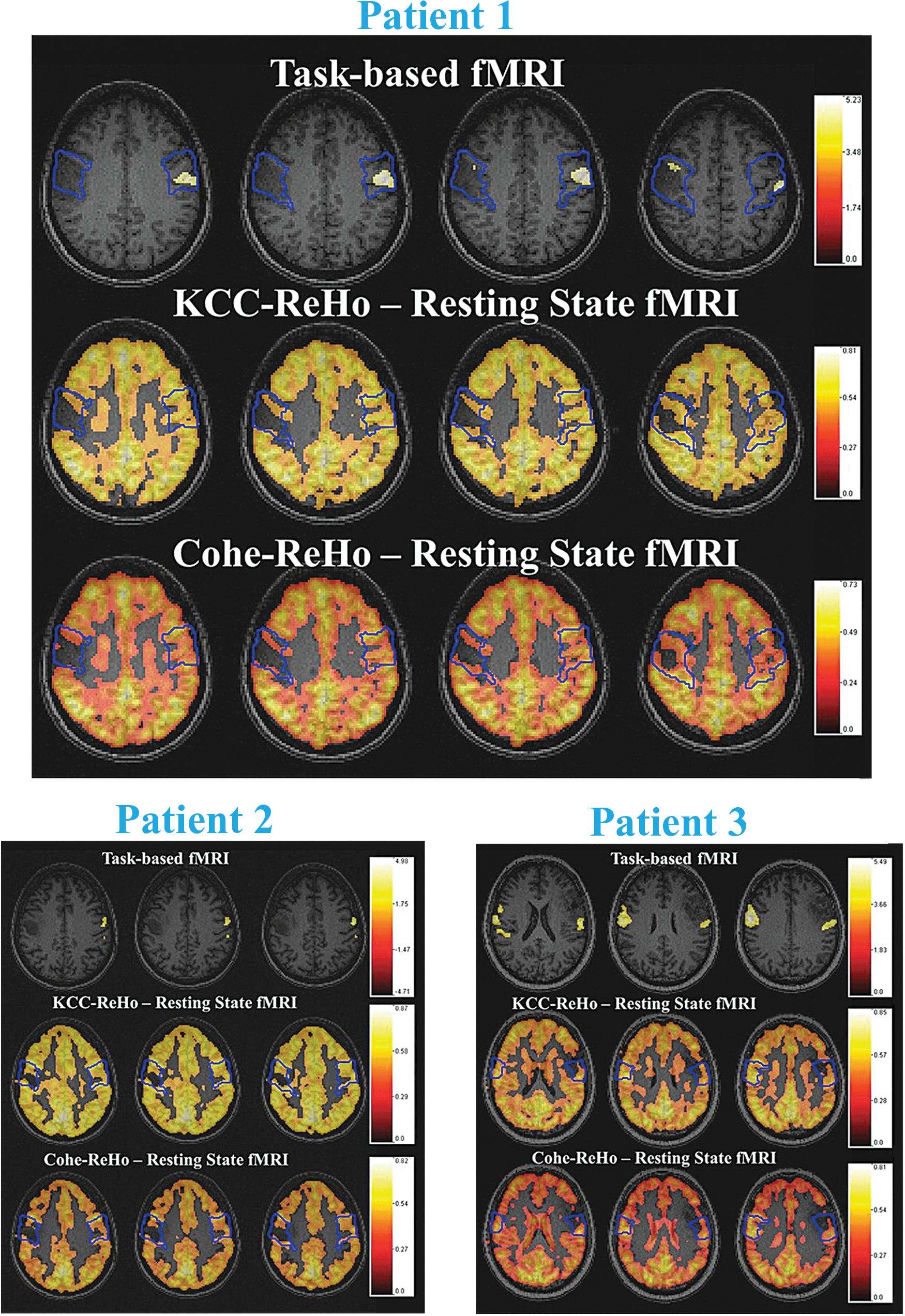
Three cases are presented with the task-based activation map, KCC-ReHo map, and Cohe-ReHo map overlaid on T1-weighted structural images in each case. Patient 1: Patient with grade II oligodendroglioma. First row shows the vertical tongue motor fMRI activation map (tbfMRI) (Z-score >4.0) overlaid on T1-weighted structural images. Second and third rows show ReHo—KCC-ReHo and Cohe-ReHo, respectively—maps (KCC >0.45 and Cohe >0.3) from rsfMRI. Patient 2: Patient with grade III anaplastic astrocytoma. First row shows the tongue motor fMRI activation map (tbfMRI) (Z-score >3.5) overlaid on T1-weighted structural images. Second and third rows show ReHo—KCC-ReHo and Cohe-ReHo, respectively—maps (KCC >0.5 and Cohe >0.4) from rsfMRI. Patient 3: Patient with grade II oligoastrocytoma. First row shows the tongue motor fMRI activation map (tbfMRI) (Z-score >3.5) overlaid on T1-weighted structural images. Second and third rows show ReHo—KCC-ReHo and Cohe-ReHo, respectively—maps (KCC >0.4 and Cohe >0.3) from rsfMRI. Blue contours display ROIs from automatically parcellated combined precentral and postcentral gyri. Notice in all maps that there is abnormally decreased signal in the ipsilesional perirolandic ROIs (IL) compared with the normal contralesional perirolandic ROIs (CL). In the setting of preserved clinical motor function and excellent task performance, these findings are indicative of tumor-induced NVU. NVU, neurovascular uncoupling; ReHo, regional homogeneity; ROIs, regions of interest; rsfMRI, resting-state functional magnetic resonance imaging; tbfMRI, task-based fMRI.
The mean Z-scores in IL and CL ROIs in task-based activation maps were obtained in each case and a paired t-test in the group of 12 patients was then performed. The mean Z-score, which was computed as mean of nonzero value voxels in each ROI, provides information about the mean amplitude of task-based sensorimotor activation. The p-values obtained comparing mean Z-score (1.72 ± 0.42) in IL ROIs with the mean voxel Z-score (2.14 ± 0.46) in the CL ROIs demonstrated significantly decreased amplitude of motor activation in IL ROIs compared with CL ROIs (p = 0.0005).
A similar approach was applied to resting-state ReHo maps. Voxel values in the CL and IL ROIs of KCC-ReHo and Cohe-ReHo maps were divided by the corresponding global mean of KCC-ReHo and Cohe-ReHo in the bihemispheric cortical brain tissue. The means of such normalized ReHo values in IL and CL ROIs were obtained in each case and a paired t-test in the group of 12 patients was then performed. Group analysis revealed significantly decreased mean ipsilesional voxel KCC-ReHo (0.96 ± 0.05, p = 0.02) and Cohe-ReHo (0.93 ± 0.08, p = 0.04) values (computed as mean of nonzero value voxels in each ROI in each slice that included the lesion) compared with the respective normal contralesional (CL) ROIs (1.02 ± 0.09 for KCC-ReHo and 1.03 ± 0.12 for Cohe-ReHo). These KCC-ReHo and Cohe-ReHo findings are similar to the findings of statistically significantly decreased ipsilesional task-based fMRI activation mentioned above. All results are listed in Table 2.
Voxel values in the CL and IL ROIs of KCC-ReHo and Cohe-ReHo maps were divided by the corresponding global mean of KCC-ReHo and Cohe-ReHo in the bihemispheric cortical brain tissue.
CL, contralesional; Cohe-ReHo, coherence regional homogeneity; IL, ipsilesional; KCC-ReHo, Kendall's coefficient of concordance ReHo; ROI, region of interest; rsfMRI, resting-state functional magnetic resonance imaging; tbfMRI, task-based functional magnetic resonance imaging.
Discussion
In this preliminary study, we have demonstrated that ipsilesional reduction in regional homogeneity of resting-state fMRI due to perirolandic tumors may be a similar indicator of tumor-induced NVU affecting the sensorimotor network as asymmetric ipsilesional reductions in tbfMRI activation. While abnormally reduced ipsilesional task-based activation in the absence of corresponding clinical sensorimotor deficits or suboptimal task performance constitutes evidence of NVU (Zaca et al., 2014), our current findings relating to regional homogeneity metrics suggest that these metrics may represent resting-state correlates of such NVU.
Previous imaging studies have demonstrated NVU in high-grade gliomas (Hou et al., 2006; Jiang et al., 2010) as well as in low-grade gliomas (Pillai and Zacà, 2011, 2012; Zacà et al., 2011, 2014). The mechanisms for such NVU have not been fully elucidated, but it is believed that in high-grade gliomas, tumor angiogenesis, which disrupts cerebral autoregulatory capacity, is the main factor, whereas in low-grade gliomas, infiltration of such tumors into the surrounding microvasculature and astrocytes (Chaitanya et al., 2014; Pelligrino et al., 2011; Watkins et al., 2014) is felt to be the main reason for reduced cerebrovascular reactivity (CVR) and associated NVU. CVR is a measure of change in cerebral blood flow in response to a vasodilatory or vasoconstrictive stimulus. Evaluating CVR has been shown to be useful for identifying cortical regions of NVU and can be performed using either breath-hold (BH) or exogenous gas administration methods (Pillai and Mikulis, 2015). In our current study, all of the patients underwent BH CVR mapping as part of their clinical presurgical mapping fMRI examinations, and the BH CVR maps did display concordant ipsilesional decreases in CVR that correspond to tumor-induced NVU. However, an alternative approach to CVR assessment involves the use of resting-state fMRI; resting-state fluctuation of amplitude (RSFA) has been described as an alternative approach to evaluate CVR (Kannurpatti and Biswal, 2008; Kannurpatti et al., 2011; Wise et al., 2004). These studies examined the correlation between end-tidal CO2 fluctuations and low-frequency BOLD fluctuations available from rsfMRI and established RSFA as a strong CVR correlate. A recent study (Liu et al., 2016) proposed a different resting-state CVR map, which exploits the natural variation in respiration to map CVR using resting-state BOLD data. However, CVR is an indirect measure of neurovascular coupling, and other resting-state fMRI approaches show promise in the evaluation of neurovascular coupling. For example, one study using healthy subjects (Yuan et al., 2013) used ReHo to investigate whether the similarities of one voxel with the surrounding voxels are properties of neurovascular coupling and found that there was reliable mean voxel-wise spatial correlation between ReHo and other neurovascular variables (such as BH responses).
In the resting-state literature, ReHo has been widely used to evaluate resting-state cortical activity. As proposed by Zang et al. (2004), ReHo signifies the temporal synchrony of BOLD signals from an individual voxel with those of its neighboring voxels that are involved in performance of a related function in a given region. Zang et al. (2004) applied the KCC (i.e., Kendall's coefficient of concordance) correlation method to calculate a summary index of temporal synchrony within an individual and neighboring voxels to provide an estimation of the efficiency of coordinated neuronal activity. Studies conducted on patient populations have demonstrated altered ReHo in multiple disease conditions, including Alzheimer's disease (Liu et al., 2008), ADHD (Cao et al., 2006), and schizophrenia (Liu et al., 2006). However, none of the studies performed thus far has explored ReHo resting-state metrics in patients with resectable focal brain lesions. To our knowledge, our current study is the first to explore whether ReHo of rsfMRI data based on KCC-ReHo and Cohe-ReHo metrics may allow detection of brain tumor-induced NVU in the sensorimotor network.
Although ReHo does not require a priori definition of ROIs and can provide information about the local/regional activity of regions throughout the brain, in this preliminary study, we were interested in evaluating the relatively nonlateralized primary sensorimotor network that serves as a simple model for the study of unilateral lesion-induced NVU. Thus, we only focused on KCC- and Cohe-ReHo parameters in ROIs that isolated the precentral and postcentral gyri. To avoid manual tracing of such ROIs, we adopted an operator-independent, atlas-based parcellation technique to define identical ROIs in the ipsilesional and contralesional sensorimotor cortex. This ROI approach, along with MNI normalization, enabled us to evaluate the group performance across the task-based and resting-state fMRI maps to evaluate the relative value of KCC-ReHo and Cohe-ReHo metrics in the assessment of NVU.
KCC was computed for every voxel in each subject and was based on the time series of each voxel, the number of time points within a time series, and the number of voxels within a cluster (Zang et al., 2004). Values of KCC range from 0 to 1, with higher values indicating greater similarity between the BOLD signal of a given voxel and that of its neighbors. Zang et al. (2004) found that more neighboring voxels and greater smoothing yield greater differences between conditions in a motor task. Liu et al. (2010) have shown that the two measurements, KCC-ReHo and Cohe-ReHo, differed mainly in some brain regions where physiological noise is dominant. Liu et al. found that coherence is not as susceptible to random noise induced by phase delay among the time courses to be measured. They compared the sensitivity of these methods in detecting the difference between resting-state conditions—eyes open (EO) versus eyes closed (EC)—and in detecting abnormal local synchronization between two groups—ADHD patients versus normal controls. They found that Cohe-ReHo is more sensitive than KCC-ReHo to the difference between two conditions (EO vs. EC) as well as between ADHD and normal controls and therefore suggested that Cohe-ReHo is superior to KCC-ReHo. To maximize reliability across subjects as well as to provide sufficient specificity to examine individual differences, we reported both measures in our current study.
Some limitations of our study include the following: although our study demonstrated ipsilesional regional decrease in regional homogeneity, this decrease may be indicative of an inherent property of the tumor tissue itself and may not be necessarily specific to NVU. However, similar ipsilesional abnormal activation reductions on tbfMRI of these patients who displayed no motor deficits suggest that the decrease in ReHo is sensitive to NVU. Although some of the asymmetry we observed on ReHo maps may be due to differences in handedness, our observed asymmetry is similar to the degree of asymmetry we obtained on task-based activation maps; as reported in previous publications, this degree of asymmetry is greater than what would be expected based on differences in handedness alone (Dassonville et al., 1997; Solodkin et al., 2001; Zacà et al., 2014). Furthermore, the relatively small sample size is a limitation of this study. However, such data are difficult to acquire given the highly homogeneous nature of the dataset and overall relatively low prevalence of such lesions, and we were, nevertheless, able to demonstrate statistically significant results.
The potential advantages of ReHo may be the scalability of this method for assessment of other brain networks beyond the sensorimotor network, and future studies will explore this possibility. This preliminary study may serve as a catalyst for future application of ReHo to the assessment of brain tumor-related NVU in more lateralized networks such as language and additional RSNs.
Conclusion
In conclusion, we have shown in this study that ipsilesional abnormalities in ReHo derived from rsfMRI may serve as potential indicators of NVU in patients with brain tumors and other resectable brain lesions; as such, ReHo findings may complement findings on tbfMRI used for presurgical planning. The possible advantages of ReHo may be the scalability of this method for assessment of other RSN beyond the sensorimotor network, and future studies will explore this possibility.
Footnotes
Acknowledgment
This work was partially supported by an NIH grant R42 CA173976-02 (NCI). (PI: Jay J. Pillai, MD)
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.