
Abstract
Parkinson's disease (PD) is a neurodegenerative disorder that affects motor skills and cognition. As brain structure and function are compromised, functional magnetic resonance imaging (fMRI) can be a helpful tool to further investigate how intrinsic connectivity is impaired on the disease. The precuneus and medial prefrontal cortex (mPFC) are hub regions involved on the default mode network (DMN), a system that is active during rest and related to cognitive processes. We hypothesized that PD patients would present a decrease in functional connectivity among these two regions and the rest of the brain. Our goal was to identify regions in which functional connectivity to precuneus and mPFC was altered in PD. This study was based on resting-state fMRI data from 37 healthy subjects and 55 PD patients. Precuneus and mPFC were selected as seed regions in a whole brain functional connectivity mapping. As expected, we found abnormal connectivity from precuneus to motor system regions in PD patients, pointing toward a decreased connectivity in the disease. No significant group effects were found for the mPFC. Our findings suggest that internetwork connectivity from DMN to motor system is impaired in PD.
Introduction
P
As PD is related to alterations in brain structure and function, neuroimaging can be useful to further investigate its physiopathology (Ceballos-Baumann, 2003; Helmich et al., 2010; YorkWilliams and Poston, 2014). Resting-state functional magnetic resonance imaging (fMRI) protocols have been used to explore PD (van Eimeren and Monchi, 2009; YorkWilliams and Poston, 2014), mainly regarding changes in intrinsic connectivity of the motor system (Helmich et al., 2010). Previous neuroimaging studies have already demonstrated impaired corticostriatal connectivity from posterior putamen to bilateral primary and secondary somatosensory cortices and also from anterior putamen to secondary somatosensory cortex and supramarginal gyrus (Helmich et al., 2010). Substantia nigra compacta of PD patients showed decreased connectivity to corticostriatal and thalamocortical circuits, cortical motor areas, pons, cerebellum, and default mode network (DMN) when compared with healthy controls (Wu et al., 2012). Cognitive impairment, which includes decreased attention, visual–spatial dysfunction, and memory deficits, was shown to be associated with reduced cortical–subcortical connectivity (Baggio et al., 2015; YorkWilliams and Poston, 2014).
DMN is a system consisting of precuneus, posterior cingulate cortex (PCC), medial prefrontal cortex (mPFC), inferior temporoparietal cortex, and medial temporal lobes, which are highly metabolically active in resting-state protocols (Greicius et al., 2003; Gusnard et al., 2001; Raichle et al., 2001). DMN has decreased activation during goal-directed processes (Buckner, 2012). In PD patients, significant changes in DMN connectivity were found (van Eimeren and Monchi, 2009), this fact being possibly associated with a greater risk of cognitive impairment (Baggio et al., 2015) and dementia (Greicius et al., 2003). Likewise, visual hallucinations were found in patients in whom the DMN showed increased connectivity in the right middle frontal gyrus and bilateral precuneus/PCC (Yao et al., 2014).
The precuneus is located on the posterior and medial part of the parietal lobule and is considered as an associative cortex (Wenderoth et al., 2005). This area is not easily studied because it is rarely affected by tumors or by stroke, so fMRI has been of great importance for its understanding (Wenderoth et al., 2005). Many functions have been attributed to it, concerning motor and cognitive tasks. Studies have shown that in motor tasks involving both hands, precuneus is likely to be required in shifting attention between different locations in space (Wenderoth et al., 2005). Studies of precuneus connectivity in primates with the use of tracing techniques showed its connections to frontal lobes, dorsal premotor area, supplementary motor area, frontal eye fields, anterior and posterior cingulate cortices, and also to retrosplenial cortices bilaterally (Leichnetz, 2001). These connections are probably implicated in visual guidance of hand movements, like reaching for objects (Ferraina et al., 1997), elaboration of motor imagery (Cavanna and Trimble, 2006), and other spatially guided behaviors. An fMRI study carried out by Le et al. (1998) reported that shifting attention tasks activated the precuneus. It was also shown that it is activated during mnemonic tasks involving images (Buckner et al., 1995; Kircher et al., 2000).
Interestingly, precuneus consumes 35% more glucose than other areas of the resting brain (Gusnard and Raichle, 2001). Therefore, it has been postulated that it may also play a role in self-consciousness. The so-called hot spots of DMN, altogether, are apparently engaged in many cognitive tasks, such as memory consolidation and retrieval, mental imagery of motor tasks, and planning (Cavanna and Trimble, 2006). These findings are corroborated by other functional imaging studies that showed decreased activation of precuneus in mental altered states, such as persistent vegetative state or REM sleep (Laureys et al., 1999; Maquet et al., 1996).
In this study, we explored the functional connectivity between precuneus/PCC and mPFC to other regions of the brain during a resting-state fMRI acquisition. We reinforce that the focus of our study was the functional alterations instead of the structural alterations, as reported by Zhu et al. (2014). Results of PD patients were posteriorly compared with those of healthy volunteers. Since PCC and mPFC are hub regions, involved in countless processes and systems, we hypothesized that there would be a decrease in intrinsic connectivity of these areas with other brain regions in PD patients, once the dopaminergic pathway is compromised.
Materials and Methods
Subjects
This study was approved by the research ethics committee, and all patients signed a consent form. Owing to ethical reasons and to avoid motion artifacts, all patients were under medication in the day of scan.
The inclusion criteria for the PD group were (i) to meet the UK Parkinson's Disease Brain Bank Criteria and (ii) to be at stage I or II in the Hoehn and Yahr scale [HY; from Hoehn and Yahr (1967); mean = 1.9, standard deviation (SD) = 0.2]. To assess the severity of the PD symptoms, all patients were evaluated by a neurologist specialized in movement disorders, using the HY and Unified Parkinson Disease Rating Scale [from Goetz et al. (2007); total mean = 50.3, SD = 19.4; section III, mean = 31.3, 11.4].
Demographical information is given in Table 1. Clinical information is described in Table 2. Equivalent doses of levodopa were calculated for each patient as a measure of medication load as described by Tomlinson et al. (2010).
SD, standard deviation.
For the severity scales, the result of t-test was not significantly statistical.
UPDRS, Unified Parkinson Disease Rating Scale.
Image acquisition
All subjects were scanned in a 3.0 T MRI system (Siemens Trio scanner) and were subjected to clinical examination during a single visit at the Hospital Israelita Albert Einstein São Paulo–Brazil. The scanner was equipped with 32 channels head coil and 45 mT/m gradient. A multiband accelerated (factor of 5) echo-planar image sequence was used to acquire whole brain volume collections in a single time-of-repetition of 600 ms. The other acquisition parameters were 40 axial slices, 2.5 mm slice thickness, time-of-echo: 31 ms, number-of-excitations: 1, flip angle: 90°, bandwidth: 2290 Hz/px, field-of-view = 210, matrix 84 × 84 mm, voxel dimension 2.5 × 2.5 mm.
Image preprocessing
The images were preprocessed using the software FSL (
After preprocessing, functional connectivity maps based on the Pearson correlation coefficient (after Fisher transform) were extracted for each subject. In a second level analysis, a general linear model was fitted at each voxel for groups' comparison, considering the functional connectivity as the dependent variable, group as the main regressor, and age, gender, group, and head movement (relative displacement, in mm) as nuisance variables. The Type I Error was set at 5% adjusted to the cluster level (z-voxel >2.32) using permutation testing using FSL randomize. Correlation analyses between the average functional connectivity at the mapped ROIs and the clinical variables were also conducted.
Results
Figure 1 depicts a functional connectivity decrease in PD, when considering the PCC as seed region toward voxels at the basal ganglia, thalamus, premotor area, supplementary, and primary motor areas. No significant findings were found in PD when using mPFC as seed. Interestingly, most changes in connectivity of PCC to basal ganglia were at the right hemisphere. No significant correlation was found between the mean functional connectivity at these regions and the clinical variables, as shown in Table 2. The mean connectivity between PCC and the red voxels shown in Figure 1 was 0.42 ± 0.04 to control subjects and 0.37 ± 0.03 to PD. Also, no significant correlation was found between the functional connectivity and medication load (p = 0.553).
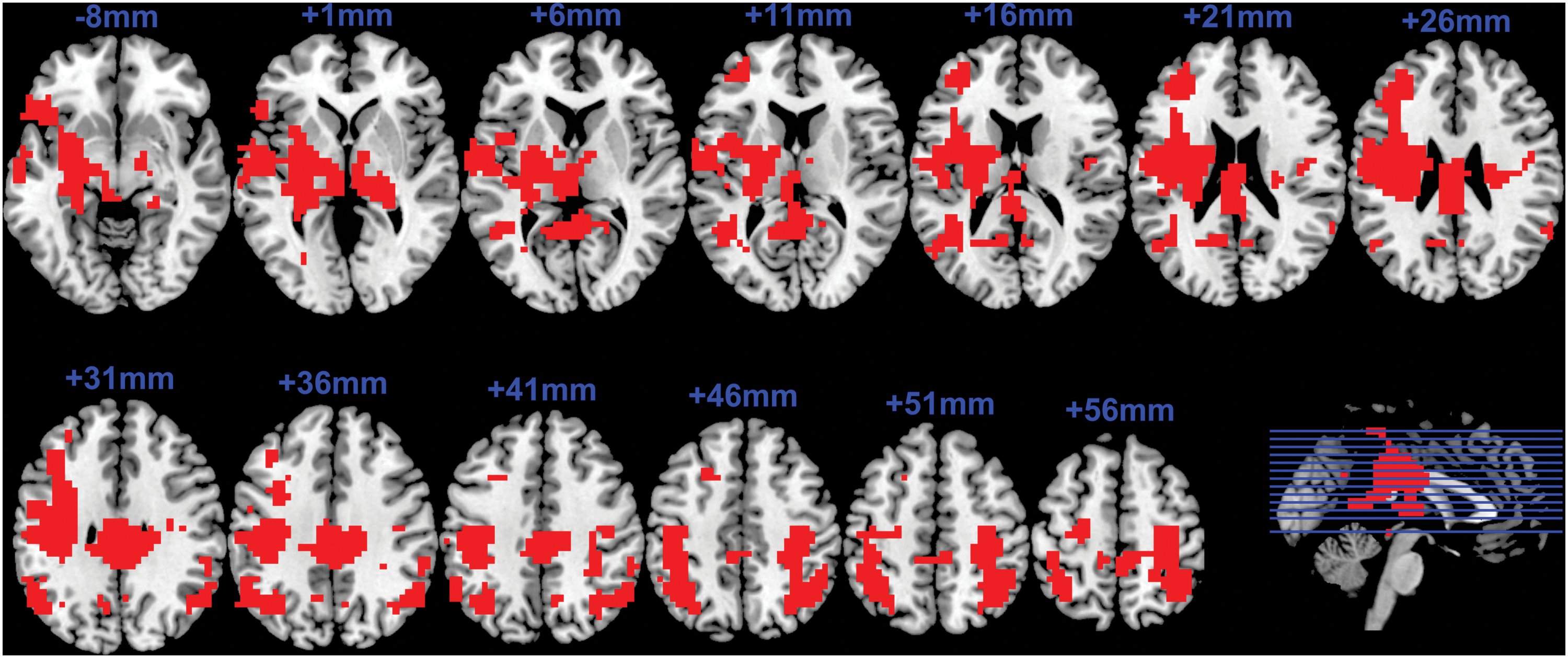
Brain map highlighting regions (red areas) with a decreased functional connectivity to PCC in PD. These maps were obtained based on voxelwise general linear models considering age, gender, and head movement as nuisance variables. The axial slices are in radiological notation, with z coordinates in blue. PCC, posterior cingulate cortex; PD, Parkinson's disease. Color images available online at
Discussion
The aim of this study was to compare brain functional connectivity of PCC and mPFC between healthy subjects and PD patients on resting state. As hypothesized by the dopamine depletion model in PD, our findings highlight that, indeed, PCC has a decreased functional connectivity to other regions of the motor system, such as basal ganglia, motor cortex, and thalamus.
Previous studies have demonstrated altered connectivity in PD patients, with diverse findings (Helmich et al., 2010; van Eimeren and Monchi, 2009; Wu et al., 2012). It was shown that in PD, posterior putamen had decreased connectivity to cingulate motor area and to primary and secondary somatosensory cortices, but not to PCC. In addition, a resting-state study (Tessitore et al., 2012) comparing PD and controls reported lower functional connectivity within some regions of DMN: right medial temporal lobe and inferior parietal cortex bilaterally, possibly correlated with cognitive impairment. Thus, our findings contribute to this knowledge by stressing out that disrupted internetwork connectivity may also play a role in explaining PD symptoms.
Since PCC is one of the functional hub regions of DMN, we expected that its most impaired connectivity would be within DMN. Moreover, by choosing PCC as the seed region for functional connectivity analyses, we proposed to go beyond motor regions. Surprisingly, our findings highlight that not only the motor system is abnormal in PD, but also the internetwork connectivity to DMN is impaired, even during a resting-state protocol.
Owing to methodological limitations (Woo et al., 2014), the precise location of alterations in the motor systems could not be determined, since we found only one big cluster comprising all these regions. We conjectured that impaired connection of PCC to motor areas might be associated with processes of motor mental imagery and planning, since DMN has the self as referential. In other words, DMN internal representation of motor components may also be disrupted in PD. In this line, a previous PET study of mental motor imagery task found that PD patients have lower activation of precuneus with dopaminergic stimulation then without it (Cunnington et al., 2001). In addition, Zhang et al. (2014) have demonstrated that motor imagery learning modulates the functional connectivity between sensory motor system and PCC. As a final point, since we found no significant correlation between the motor system/PCC's altered connectivity and the severity of PD symptoms, we believe that our findings are more related to a pathological state but not necessarily to its progression.
Toward conclusion, it is important to mention two limitations of this study, the first concerning the head motion artifacts, which are expected to be greater in PD. We handled this artifact by including the frame displacement of each subject as a nuisance variable in the general linear model group analyses, but residual nonlinear relations could still be affecting the results. Second, PD patients were studied under dopamine replacement therapy (DRT), for ethical reasons and also to avoid excessive head motion and discomfort during the examination due to axial rigidity and pain. Previous studies regarding fMRI on PD on DRT showed that we cannot fully separate the pathological condition per se from pharmacological effects (Cole et al., 2013; Dang et al., 2012). A systematic review was performed by Tahmasian et al. addressing studies in PD patients under DRT or not (Tahmasian et al., 2015). They concluded that it is possible to study patients on DRT, but it could have a significant influence on functional brain organization. Also, there are hypotheses that chronic use of DRT could still be present in the “OFF” state, which could also lead to changes in the resting state (Kurani et al., 2014). To check this possible bias, we have calculated the levodopa equivalent dosage and we found no correlation with the functional connectivity of the PD group.
Therefore, our results suggest that intrinsic connectivity changes in PD are not only present in motor system but possibly in other networks and, also, in the communication between different brain modules and internetwork connectivity.
Footnotes
Acknowledgments
R.B.T. is grateful to UFABC for the scholarship received. The authors thank the Brazil Parkinson Association (for helping to contact volunteers during the recruitment) and São Paulo Research Foundation (FAPESP) for the research grant (No. 2011/18747).
Author Disclosure Statement
No competing financial interests exist.