
Abstract
Cross-sectional and longitudinal studies in active duty and veteran cohorts have both demonstrated that deployment-acquired traumatic brain injury (TBI) is an independent risk factor for developing post-traumatic stress disorder (PTSD), beyond confounds such as combat exposure, physical injury, predeployment TBI, and pre-deployment psychiatric symptoms. This study investigated how resting-state brain networks differ between individuals who developed PTSD and those who did not following deployment-acquired TBI. Participants included postdeployment veterans with deployment-acquired TBI history both with and without current PTSD diagnosis. Graph metrics, including small-worldness, clustering coefficient, and modularity, were calculated from individually constructed whole-brain networks based on 5-min eyes-open resting-state magnetoencephalography (MEG) recordings. Analyses were adjusted for age and premorbid IQ. Results demonstrated that participants with current PTSD displayed higher levels of small-worldness, F(1,12) = 5.364, p < 0.039, partial eta squared = 0.309, and Cohen's d = 0.972, and clustering coefficient, F(1, 12) = 12.204, p < 0.004, partial eta squared = 0.504, and Cohen's d = 0.905, than participants without current PTSD. There were no between-group differences in modularity or the number of modules present. These findings are consistent with a hyperconnectivity hypothesis of the effect of TBI history on functional networks rather than a disconnection hypothesis, demonstrating increased levels of clustering coefficient rather than a decrease as might be expected; however, these results do not account for potential changes in brain structure. These results demonstrate the potential pathological sequelae of changes in functional brain networks following deployment-acquired TBI and represent potential neurobiological changes associated with deployment-acquired TBI that may increase the risk of subsequently developing PTSD.
Introduction
O
Synthesis across several types of neuroimaging methods has suggested that chronic phase TBI may be a disorder of disconnection, representing a potential mechanism through which TBI may increase the risk of developing PTSD (Hayes et al., 2016). As reviewed by Hayes et al. (2016), disconnection is related to injury effects on axons and may result from a variety of mechanisms, including axonal shearing or effects secondary to inflammation, and can occur subsequent to any injury mechanism. Network analyses allow quantification of network topology and communication throughout the brain, providing an ideal approach to understand the effect of TBI and potential disconnections on brain function (Bullmore and Sporns, 2009).
Two studies to date have utilized magnetoencephalography (MEG) to conduct whole-brain network analyses of individuals with TBI history. Alhourani et al. (2016) found reduced local efficiency in brain regions associated with the default mode network in civilian participants with mild TBI, a median of 8 months postinjury. Reductions in local efficiency occurred across several frequency ranges, most notably in the alpha and delta ranges. Rowland et al. (2017) found increases in small-worldness of whole-brain networks associated with TBI history, an average of 6.2 years postinjury and decreased levels of small-worldness associated with a diagnosis of PTSD in postdeployment Iraq and Afghanistan war veterans. Small-worldness is a network configuration characterized by short path lengths from any point in the network, while simultaneously maintaining high levels of clustering among nodes. Post-hoc analyses indicated the networks of participants with PTSD displayed decreases in clustering coefficient, but no differences in path length, while the networks of individuals with mild TBI history displayed increased levels of clustering coefficient without differences in path length. The findings of these two studies are not consistent; however, there was a significant difference in the time since injury and sample population that may explain these discrepancies.
Three studies have utilized functional magnetic resonance imaging (fMRI) to conduct whole-brain network analyses of TBI with mixed results. Higher modularity and a significant reduction in between module connectivity were associated with TBI history in a sample of active duty military personnel examined within 90 days of blast exposure (Han et al., 2014). Conversely, a reduction in modularity was observed in a civilian sample with TBI history and current postconcussive symptoms at 6 months postinjury (Messe et al., 2013). Finally, Spielberg et al. (2015) examined postdeployment veterans from the conflicts in Iraq and Afghanistan, finding no effect of PTSD or TBI on whole-network metrics, instead TBI moderated the relationship between graph metrics of specific brain regions and reexperiencing symptoms.
Overall, findings of studies utilizing network analyses to study TBI have produced mixed results that vary by the sample examined (e.g., civilian, veteran, and mixed severities), the time since injury, and the technology employed (Alhourani et al., 2016; Han et al., 2014; Messe et al., 2013; Rowland et al., 2017; Spielberg et al., 2015). However, differences in connectivity and network structure have been consistently reported, observed as soon as 24 h and as late as a decade following the injury. Alterations in brain networks offer insights into potential mechanisms through which TBI may increase the likelihood of developing PTSD. However, the changes in brain networks related to mild TBI are not yet fully characterized, and the circumstances under which these changes occur are not yet fully understood.
This study will determine differences in whole-brain resting-state functional networks associated with the development of PTSD following deployment-acquired mild TBI. Based on previous findings, it is hypothesized that higher levels of small-worldness, clustering coefficient, and modularity will be associated with the development of PTSD following deployment-acquired mild TBI.
Materials and Methods
This project was reviewed and approved by the Institutional Review Board at the W.G. “Bill” Hefner VA Medical Center in Salisbury, North Carolina. The welfare and privacy of human subjects were protected. Each participant voluntarily provided verbal and written informed consent before any study activity.
Participants
Participants were identified from a larger ongoing study (Blast Study) funded by the Chronic Effects of Neurotrauma Consortium. Inclusion criterion for the larger study was combat exposure during an Iraq or Afghanistan war deployment. Exclusion criteria for the larger study were as follows: TBI history outside of deployment involving loss of consciousness (LOC), neurological disorder, severe mental illness (schizophrenia or bipolar disorder), current substance use disorder, current psychotic symptoms, or presence of any contraindication for neuroimaging. Sixteen participants were identified from the larger study with a history of deployment-acquired mild TBI and included in this analysis. Seven participants met criteria for current PTSD. No participant met diagnostic criteria for PTSD before experience of deployment-acquired mild TBI. There was no requirement that the participants be experiencing current postconcussive symptoms.
Characterization
The Structured Clinical Interview for DSM-IV Diagnosis (SCID; First et al., 1996) was used to determine the presence or absence of any Axis I psychiatric diagnosis with the exception of PTSD. The SCID is a structured clinician-administered interview considered the gold standard for psychiatric diagnosis. The Clinician-Administered PTSD Scale–5 (CAPS-5; Weathers et al., 2017) was used to determine the presence or absence of current and lifetime PTSD using the past month and worst month versions. The CAPS-5 represents the gold standard assessment of PTSD. Participants were considered to have a current diagnosis of PTSD if they met at least one Criterion B symptom, one Criterion C symptom, two Criterion D symptoms, two Criterion E symptoms, as well as Criterion F and G. A structured clinician-administered interview was used to determine the presence or absence of mild TBI history across the lifespan according to the American Congress of Rehabilitation Medicine criteria (Menon et al., 2010). Specifically, participants were considered positive for TBI if they experienced a force acting on the central nervous system that resulted in LOC, alteration of consciousness (AOC), or post-traumatic amnesia (PTA) of any duration. Severity was based on VA/DoD consensus criteria, with mild TBI displaying LOC less than 30 min, AOC less than 24 h, and/or PTA less than 24 h (Management of Concussion/mTBI Working Group, 2009).
Demographically adjusted premorbid IQ was estimated using the Test of Premorbid Function (Wechsler, 2009). Self-report questionnaires were used for further characterization of participants. Postconcussive symptoms were measured using the neurobehavioral symptoms inventory (Cicerone and Kalmer, 1995), a 22-item self-report inventory asking about the severity of common postconcussive symptoms over the past 2 weeks. PTSD symptoms were measured using the PTSD Checklist–5 (PCL-5; Blevins et al., 2015), a 20-item self-report inventory asking about the severity of PTSD symptoms over the past month. Severity of combat exposure was measured using the Deployment Risk and Resilience Inventory–2 Combat Experiences questionnaire (Vogt et al., 2012), a 17-item self-report inventory asking about the frequency of combat experiences during deployment.
MEG recordings
Data were acquired using a whole-head CTF Systems Inc. MEG 2005 neuromagnetometer system equipped with 275 first-order axial gradiometer coils. Head localization was achieved using a conventional three-point fiducial system (nasion and preauricular points). Resting-state recording was conducted with the participant seated upright, sitting quietly, and with eyes open for 5 min. Data were sampled at 2400 Hz over a DC-150 Hz bandwidth. MEG data were preprocessed using synthetic third-order gradient balancing, whole trial DC offset, and band pass filtered from 0.5 to 80 Hz with a 60 Hz notch filter. Data were visually inspected for obvious muscle artifact, and such epochs were discarded from further analyses. Following MEG recording, a T1-weighted MRI scan was obtained for each participant for the purpose of coregistration and localization of MEG signals.
Network analysis
The network analysis applied as part of this study is identical to that used by Rowland et al. (2017). Rowland et al. (2017) analyzed networks within the alpha bandwidth as well as a wide-band network (1–70 Hz). Based on results from that study, this analysis examined wide-band connectivity only. Network analysis proceeds in a stereotypical manner, first identifying nodes of the network (node identification section) and then quantifying communication among those nodes (estimating functional connectivity between nodes section). The resulting matrices are conducive to the application of graph theory for calculating metrics describing the topology of the network (calculation of network metrics section).
Node identification
A well-validated beamformer (synthetic aperture magnetometry; SAM) (Hillebrand et al., 2005; Robinson and Vrba, 1998) was applied (voxel size of 5 mm3, lead fields for equivalent current dipoles, maximizing noise-normalized power) using a three-spherical shell, multiple local spheres head model based on the participant's MRI (Huang et al., 1999) to construct noise-normalized statistical parametric maps, identifying areas of significant brain activity for each participant individually. SAM was applied in the following frequency ranges: delta (0.5–4 Hz), theta (4–8 Hz), alpha (8–13 Hz), beta (13–30 Hz), gamma (30–80 Hz), as well as 0.5–80 Hz. Source series representing the unique weighted sum of the output across all MEG sensors for a specific location in the brain were calculated for each identified peak across all frequency ranges (Hillebrand et al., 2005; Robinson and Vrba, 1998).
Estimating functional connectivity between nodes
The weighted phase lag index (wPLI; Vinck et al., 2011) was calculated between all pairs of source series to measure functional connectivity between nodes. Each source series was divided into 6-sec epochs for this calculation. Connectivity was operationalized at the frequency with the highest wPLI value.
Thresholding
Data were first thresholded using 10,000 unique pairs of phase randomized surrogate time series calculated for each participant individually (Prichard and Theiler, 1994). Connectivity between node pairs was retained if at least two standard deviations higher than the surrogate data at the identical frequency bin (i.e., 10.25 Hz or 8.75 Hz). The resulting networks were then thresholded by satisfying the equation S = log(N)/log(K) where N represents the number of nodes in the network and K the average degree (Hayasaka and Laurienti, 2010). We selected S = 2.5 as prior research has demonstrated equivalence of S values between 2 and 4 (Hayasaka and Laurienti, 2010).
Calculation of network metrics
Network metrics calculated are listed in Table 2. Clustering Coefficient was calculated as defined in Stam and Reijneveld (2007). The clustering coefficient is a measure of grouping within the network, indicating how likely the neighbors of a node are to also be connected with one another. Small World was calculated as defined in Watts and Strogatz (1998). The average of the clustering coefficient and path length of 500 independently generated random networks with the same number of nodes and degree distribution as the original network were used for the calculation of Small World. Small-worldness is a network configuration with the benefits of both lattice-like and random networks, in that it simultaneously possesses high clustering coefficient and short path length. It is calculated by comparing the clustering coefficient and path length within a network, both normalized by the same coefficients in a random network. Modularity was calculated using the Louvain method of community detection as defined in Blondel et al. (2008). Following the recommendations of the Brain Connectivity Toolbox (Rubinov and Sporns, 2010), the analysis was run 500 times, using the average Q and average number of modules (Number Modules) as outcome variables. Modularity indicates how many subnetworks can be identified within the larger network by iteratively breaking the network into cohesive subnetworks.
The number of nodes within each participant's network varied, ranging from 69 to 128, but were not significantly different between groups (p > 0.45). To control for possible effects of network size, each network metric was normalized by the number of nodes in the network from which it was calculated.
Materials
Beamforming and source series construction were completed using software provided by CTF MEG International Services LP (Coquitlam, BC, Canada). Further analyses of source series data and network creation were conducted using Matlab 2016a. Network metrics were calculated using the Brain Connectivity Toolbox (Rubinov and Sporns, 2010), as well as functions created by members of the study team. Statistical analyses were conducted using IBM SPSS Statistics Version 21.
Analyses
Between-group differences in continuous demographic and self-report variables were examined using t-tests. Differences in categorical variables were examined with chi-square analyses. Between-group differences in normalized network metrics were examined using univariate ANCOVAs controlling for age and estimated premorbid IQ. Results are presented using an uncorrected alpha level of 0.05 along with effect sizes (partial eta squared and Cohen's d) to aid interpretation.
Results
Characterization
Table 1 for means and standard deviations of demographic variables. Seven participants met diagnostic criteria for current PTSD according to the CAPS-5 and 9 did not. Participants diagnosed with PTSD were significantly younger, F(1,14) = 6.63, p = 0.022, and scored significantly higher on the PCL-5, F(1, 14) = 15.83, p < 0.001. There were no other significant between-group differences. All participants were in the chronic stage of TBI (e.g., at least 1 year postinjury) at the time of participation. All participants met criteria for history of mild TBI (e.g., <30 min LOC, <24 h AOC, and <24 h PTA), none had history of TBI greater than mild. All TBIs occurred during deployment. Six of seven participants with PTSD developed the condition as a result of deployment-related traumatic events. For one, the traumatic event occurred after deployment. No participant diagnosed with PTSD had onset of the disorder before deployment.
Total sample size = 16.
Significant group difference, p < 0.05.
TBI, traumatic brain injury; TOPF, test of premorbid function; DRRI, deployment risk and resiliency inventory; PTSD, post-traumatic stress disorder; NSI, neurobehavioral symptom inventory; PCL-5, PTSD checklist–5.
Network outcomes
Mean and standard deviation of network metrics can be seen in Table 2. Participants with deployment-acquired TBI who developed PTSD displayed higher levels of small-worldness, F(1,12) = 5.364, p < 0.039, partial eta squared = 0.309, Cohen's d = 0.972, and clustering coefficient, F(1, 12) = 12.204, p < 0.004, partial eta squared = 0.504, Cohen's d = 0.905, than participants who did not develop PTSD. This is visually displayed in Figure 1. Modularity (Q) and the number of modules present were not different between groups. All participants except one had Small World greater than 1. In other words, PTSD diagnosis was associated with increases in the small world nature of the networks, and relatedly clustering within the networks. The group separation is not perfect, but clearly present in Figure 1. The increased clustering did not alter the modularity of the networks or the number of modules present.
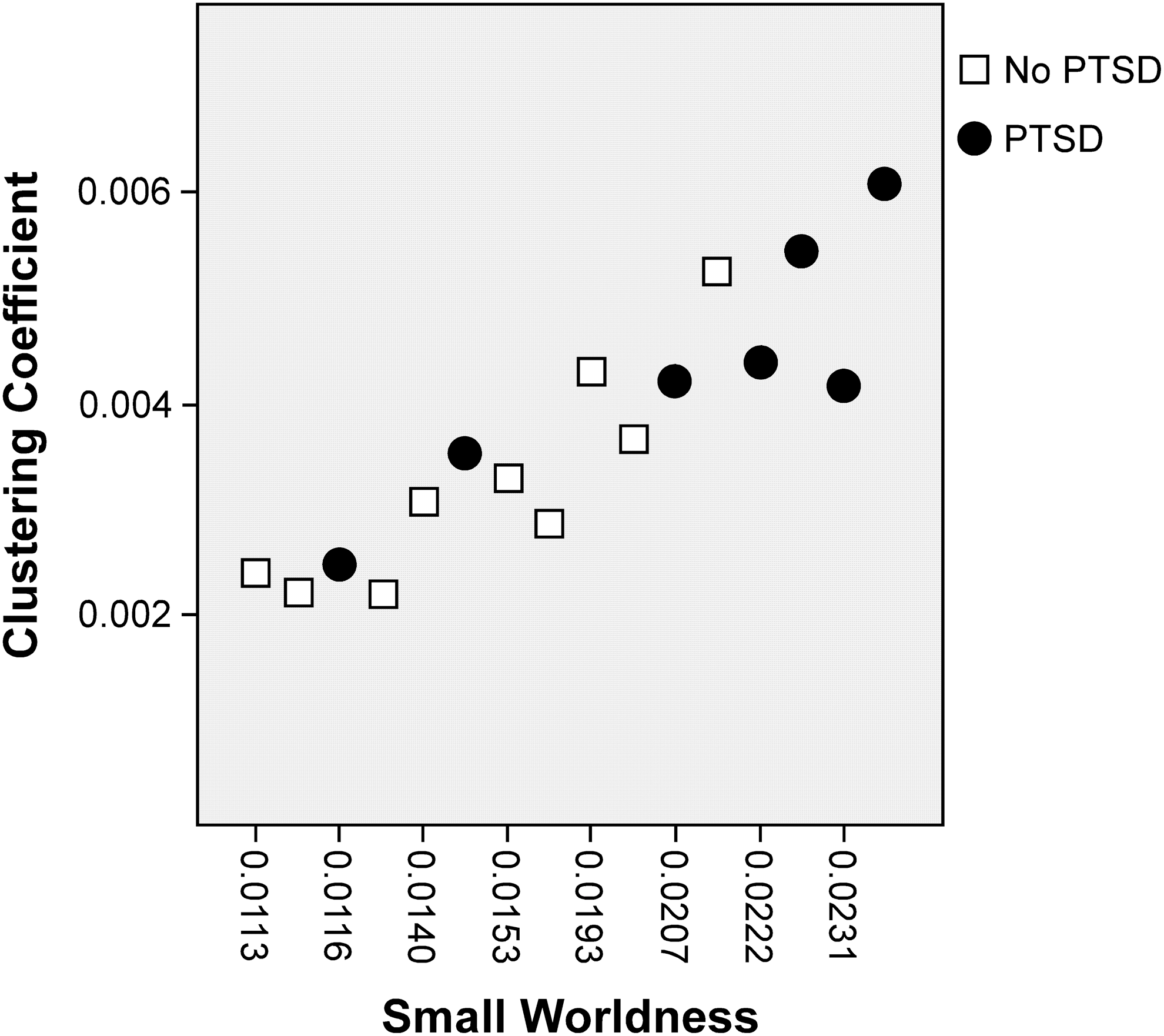
Scatter plot comparing normalized clustering coefficient and small-worldness by PTSD. PTSD, post-traumatic stress disorder.
All variables have been normalized by the number of nodes in a network and are presented × 102 for ease of reading. Total sample size = 16.
Significant group difference, p < 0.05.
Discussion
This study adds to the small, but growing literature combining resting-state MEG and network analyses to better understand TBI and PTSD. Previous work has clearly demonstrated that deployment-acquired TBI is a risk factor for the development of PTSD, beyond confounds such as combat exposure, physical injury, predeployment TBI, and predeployment psychiatric symptoms. This study demonstrates significant differences in whole-brain resting-state network topology between individuals who did and did not develop PTSD following deployment-acquired TBI. These differences represent one possible neurobiological mechanism through which deployment-acquired TBI may increase the risk of subsequently developing PTSD.
Two previous studies have identified potential mechanisms through which TBI may increase the risk of developing PTSD. Morissette et al. (2011) reported a potentially mediating role of postconcussive symptoms in the development of PTSD following deployment-acquired TBI. However, postconcussive symptoms are nonspecific and can result from many conditions and experiences, including PTSD itself. Postconcussive symptoms were not significantly different between individuals with and without PTSD in this study. Glenn et al. (2017) examined fear learning and extinction processes as potential mediators between deployment-acquired TBI and the development of PTSD. The study demonstrated that fear processes were altered as a result of deployment-acquired TBI. However, altered fear processes mediated the relationship between deployment-acquired TBI and PTSD only in cases where the participant had sustained a nondeployment TBI within the 2 years before deployment. Neither of these prior studies included neurobiological outcomes. Comparisons between changes in resting-state network topology, postconcussive symptoms, and fear processes may help better characterize the circumstances under which TBI increases the risk of developing PTSD and identify potential relationships across these modalities of inquiry. Future studies are encouraged to gather data across various modalities, including imaging, behavioral, and symptom report.
Two studies have utilized MEG to conduct whole-brain network analyses of individuals with TBI history. Alhourani et al. (2016) found reduced local efficiency in brain regions associated with the default mode network in civilian participants with mild TBI, a median of 8-months postinjury. Reductions in local efficiency occurred across several frequency ranges, most notably in the alpha and delta ranges. Rowland et al. (2017) found increases in small-worldness of whole-brain networks associated with TBI an average of 6.2 years after the injury and decreased levels of small-worldness associated with a diagnosis of PTSD in postdeployment Iraq and Afghanistan war veterans.
These findings extend those of Rowland et al. (2017) demonstrating the potential pathological implications of differences in network topology. While this entire sample was diagnosed with deployment-acquired mild TBI, the subsample who developed PTSD displayed higher levels of small-worldness and clustering coefficient than individuals who did not develop PTSD. Changes in clustering coefficient did not result in alterations in modularity, suggesting that the increase in clustering is not occurring specifically within modules, but is balanced by increases in intramodule clustering as well.
These findings do not clearly support the view of TBI as a disorder of disconnection (Hayes et al., 2016). The observed changes demonstrate that an increasing number of nodes are connecting to neighbors of nodes with which they are already connected, suggesting an increased level of order in the network, similar to the findings of James et al. (2013). The nature of this analysis maintains a particular ratio between the number of nodes and the number of connections (Hayasaka and Laurienti, 2010) If network changes were seen as a result of disconnection, the additional connections being maintained would be expected to occur randomly, decreasing clustering coefficient and small-worldness of the networks. While not directly evaluated as part of this analysis, these findings are consistent with the hyperconnectivity hypothesis (Hillary et al., 2014), suggesting the brain responds to TBI with increased connectivity in particular pathways as a potential coping or repair mechanism. It is possible these alterations also create a neurological milieu conducive to the development of PTSD, potentially within specific subnetworks. Future studies could investigate the anatomic consistency of network changes across individuals and how those changes affect particular subnetworks.
Limitations of this study include a small sample size. These findings should be considered preliminary until replicated in a larger sample. However, calculations suggest that the observed differences represent a moderate effect size. The findings are also consistent with those of Rowland et al. (2017), a study applying identical methods to an independent sample, suggesting the findings are robust and replicable. Another limitation is the cross-sectional nature of the study. It is possible that the observed differences in resting-state networks were present before the TBI event rather than a consequence of it. Alternatively, the TBI event may have created transient neurobiological alterations that resolved before study participation.
An additional limitation relates to the continuous nature of psychopathology. This study divided participants by PTSD diagnosis; however, many participants who did not meet full criteria for PTSD diagnosis nevertheless displayed subthreshold levels of symptoms. Future studies using larger sample sizes should consider alternative analytic approaches that could incorporate and potentially explain this variance across symptom presentations and its relationship to alterations in network metrics. It is also possible the observed group differences are the result of a cascade of changes initiated by the TBI event, but not yet present when PTSD initially developed. Future studies applying longitudinal designs or nonhuman models may help clarify temporal relationship between TBI, PTSD, and functional network differences. Finally, the methods applied to create networks generate a partial network solution, identifying areas of the brain active at rest and quantifying communication among them. This approach by definition does not identify when expected regions are not part of the network, potentially as a sequelae of TBI. Future studies may consider combining this approach with a standardized region of interest or voxel-based approach to allow an understanding of differences in the brain regions present in the networks or their role in the network.
Conclusion
Deployment-acquired TBI has been demonstrated to be an independent risk factor for the subsequent development of PTSD, beyond other known risk factors. This study demonstrates differences in small-worldness and clustering coefficient of resting-state brain networks between individuals who did and did not develop PTSD following a deployment-acquired TBI. These findings suggest the possibility that neurobiological mechanisms contribute to the increased risk for developing PTSD and highlight the need for further study in this area.
Footnotes
Acknowledgments
This material is based upon work supported by the U.S. Army Medical Research and Material Command and from the U.S. Department of Veterans Affairs [Chronic Effects of Neurotrauma Consortium] under Award Nos. W81XWH-13-2-0095 and 1 I01 RX002172-01, R01AA016852 (to DWG), AA026117 (to DWG and JAR), as well as the resources of the W.G. “Bill” Hefner Veterans Affairs Medical Center, the Mid-Atlantic Mental Illness Research Education and Clinical Center (MIRECC), and the Wake Forest School of Medicine Department of Neurology.
Disclaimers
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs, the Department of Defense, or the U.S. government.
Author Disclosure Statement
All authors declare that no competing financial interests exist.