
Abstract
Resting-state functional magnetic resonance imaging has been playing an important role in the study of amyotrophic lateral sclerosis (ALS). Although functional connectivity is widely studied, the patterns of spontaneous neural activity of the resting brain are important mechanisms that have been used recently to study a variety of conditions but remain less explored in ALS. Here we have used fractional amplitude of low-frequency fluctuation (fALFF) and regional homogeneity (ReHo) to study the regional dynamics of the resting brain of nondemented ALS patients compared with healthy controls. As expected, we found the sensorimotor network with changes in fALFF and ReHo, and also found the default mode network (DMN), frontoparietal network (FPN), and salience network (SN) altered and the cerebellum, although no structural changes between ALS patients and controls were reported in the regions with fALFF and ReHo changes. We show an altered pattern in the spontaneous low-frequency oscillations that is not confined to the motor areas and reveal a more widespread involvement of nonmotor regions, including those responsible for cognition.
Introduction
Amyotrophic lateral sclerosis (ALS) is a devastating motor neuron disease characterized by upper and lower motor neuron dysfunction, with cognition and behavior being affected as well (Abrahams et al., 2005; Kiernan et al., 2011; Strong et al., 2017). Neuroimaging studies have been playing an important role to understand the pathophysiology of the disease and especially resting-state functional magnetic resonance imaging (rs-fMRI) studies offer a new perspective in ALS (Schulthess et al., 2016). Since patients are not required to perform any specific task, this magnetic resonance imaging (MRI) sequence, which can measure functional changes in the brain, becomes increasingly relevant considering the physical disability of ALS patients. Specifically, resting-state functional changes may be an early indicator of transactive response DNA binding protein with Mr 43 kDa (TDP-43) depositions, the main pathology found in ALS (Braak et al., 2013; Mackenzie and Rademakers, 2008).
Human brain activity is supported by oscillatory waves in different frequencies that are linked to different neural processes (Zuo et al., 2010). While functional connectivity analysis has been frequently used to investigate interregional interactions, spontaneous low-frequency fluctuations in local areas have been less explored in ALS. Different approaches to measure amplitudes of low frequencies in the resting brain have been proposed. One method is the fractional amplitude of low-frequency fluctuation (fALFF). The fALFF computes the total power of low-frequency range divided by the total power of the entire frequency range (Zou et al., 2008). This method is an improvement for the amplitude of low-frequency fluctuation (ALFF) measure, which is highly influenced by physiological noise induced by cardiac and respiratory artifacts (Zou et al., 2008).
Regional homogeneity (ReHo), which uses Kendall's coefficient of concordance (KCC), measures the similarity of the time series of each voxel and the time series of its neighboring voxels based on the hypothesis that brain activity occurs in clusters, thus providing an effective method of local brain activity (Zang et al., 2004).
Although fALFF and ReHo are established methods to analyze spontaneous brain activity (resting-state protocol), they extract different features from the BOLD signal. fALFF is a voxel-by-voxel analysis focusing on quantifying the percentage of contributions from 0.001 to 0.1 Hz oscillations to the blood oxygen level dependent (BOLD) signal variance. In other words, fALFF is a univariate spectral analysis of each voxel signal. In contrast, ReHo analysis focuses on measuring the signal similarity of a voxel with its neighboring voxels, and thus, the regional homogeneity. The neurophysiological underpinnings of both measures are still not established, but one possible explanation is that fALFF is related to the integration among many oscillating systems, resulting in low-frequency fluctuations. Complementary, ReHo could be explained by intraregional functional connectivity.
Amplitudes of low frequencies are proved to vary in different brain tissues and regions (Biswal et al., 1995; Zuo et al., 2010), according to age and gender (Lopez-Larson et al., 2011), and are found to be different among clinical populations (Wang et al., 2015; Zang et al., 2007; Zhang et al., 2012). Frequency-dependent changes of spontaneous neural activity have been used to study a wide range of diseases, including Parkinson's disease (Sheng et al., 2016; Yang et al., 2013), Alzheimer's disease (Cha et al., 2015; Peraza et al., 2016), and mild cognitive impairment (Li et al., 2017; Yuan et al., 2016), but have been poorly explored in ALS.
Resting-state functional connectivity is one of the most used MRI analyses studied in ALS; however, exploring the amplitudes of low frequencies can be particularly interesting and brings new insights to study the pathophysiology of the disease. Ma et al. (2016) have reported widespread fALFF changes at slow-4 and slow-5 bands, while Zhou et al. (2013) investigated ReHo in the sensorimotor network (SMN).
Motivated by the scarce work in the area, in the present study, we explored in a whole-brain analysis if both fALFF and ReHo would present low-frequency resting brain changes in nondemented ALS patients compared with healthy controls (HC). We hypothesized that fALFF would be altered in the whole brain as shown previously (Ma et al., 2016) and that not only the SMN but whole-brain ReHo alterations would be present as well. In addition, we also carried out a whole-brain voxel-based morphometry (VBM) analysis of structural images to explore potential associations between structural changes and spontaneous neural activity.
Materials and Methods
Participants
This is a retrospective and exploratory study performed on existing MRI data and the patients were included in another study (Bueno et al., 2018). Patients were diagnosed by an experienced neurologist and classified according to the El Escorial (Brooks et al., 2000) and Awaji diagnostic criteria (de Carvalho et al., 2008), as definite or probable ALS. Patients with diagnosis of dementia were not included. Respiratory function was above 70%, indicated by forced vital capacity, with no indication of nocturnal hypoventilation. Disease duration was calculated in years from symptom onset to MRI date. Controls were recruited from the community. All participants underwent the Addenbrooke's Cognitive Examination-Revised (ACE-R), which provides general indication of cognitive impairment. Years of education for the control group were not available when the present analyses were performed. Ethical approval was obtained from the Human Research Ethics Committee of South Eastern Sydney/Illawarra Area Health Service. Written consent was obtained from each participant or a close relative.
MRI acquisition
ALS patients (n = 20) and HCs (n = 11) underwent whole-brain MRI on a 3T Philips scanner. Due to technical issues with the scanner, rs-fMRI was available only for 11 participants in the control group. T1-weighted images were acquired with a multishot 256 turbo field echo factor (time of repetition/time of echo [TR/TE] 5.4/2.4 ms, 256 × 256 matrix, field of view (FOV) 256 × 256 × 180, flip angle 8°), slice thickness 1 mm, coronal orientation, and voxel size 1 × 1 × 1 mm3. The following protocol was used for resting-state fMRI acquisition: T2*-weighted images using single shot EPI (TR/TE 3000/30 ms, 120 × 120 matrix, field of view (FOV) 240 × 240 × 140, flip angle 80°), 127 scans, 40 transverse slices with 3.5 mm thickness and no gap, and voxel size 2 × 2 × 3.5 mm3.
MRI processing
Functional magnetic resonance analysis
fMRI data were preprocessed using the CONN toolbox version 17.a. The first four scans were dropped to achieve the steady-state condition. Preprocessing steps included a standard pipeline (slice-timing correction, realignment and unwarping, spatial normalization, and smoothing), resulting in both functional and structural images in the Montreal Neurological Institute (MNI) space. The preprocessed images were then analyzed using REST toolbox (
VBM analysis
VBM analysis was performed using Statistical Parametric Mapping 12 software (SPM12; Wellcome Department of Imaging Neuroscience, UCL, United Kingdom). The images were preprocessed following a standard VBM protocol (Ashburner, 2007). The anterior commissure of all images was set as the origin of the spatial coordinates. Then, segmentation algorithm bias corrected the raw T1-weighted images for inhomogeneities and generated rigid body aligned gray matter (GM) and white matter (WM) images of the subjects. Finally, we used the DARTEL algorithm to estimate the nonlinear deformations that best aligned all images together by iteratively registering the imported images with their average. The created mean template was registered to the International Consortium for Brain Mapping template in the MNI space. We obtained the normalized and modulated tissue probability map of GM image (with isotropic voxel size of 1.5 mm) that was smoothed with a 10-mm full-width at half-maximum smoothing kernel, considering significance level as 5%. After generating the maps of GM, we performed the randomized command in FSL platform version 5.0.9 with 10,000 permutations cluster-level corrected at p < 0.05, to investigate if changes in ReHo and fALFF would be accounted for structural changes. Statistical analyses were performed with SPSS and the processed data were fit to a GLM, considering brain structures as dependent variables, age and total intracranial volume (TIV; Computational Anatomy Toolbox 12 was used to calculate TIV—CAT12) as covariates, and gender as fixed factor, considering significance level as 5% and Bonferroni corrected for multiple comparisons.
Results
Demographical analyses and cognitive testing
ALS patients and HC did not statistically differ on age (t-test; p = 0.31), but there was a significant difference in gender (chi-square statistic = 5.18; p = 0.02), with a higher proportion of females in the control group. To minimize possible influence of gender in the results, statistical analyses were implemented considering gender as fixed factor. Mean education for the ALS group was 12.5 years (standard deviation [SD] = 3.56), and mean disease duration 2.61 years (SD = 2.17). Demographic data and ACE-R results are shown in Table 1. ALS patients and HC did not differ in the ACE-R subdomains, except for language.
Demographics
Statistical significance set as p < 0.05.
ACE-R, Addenbrooke's Cognitive Examination-Revised; ALS, amyotrophic lateral sclerosis; HC, health controls; SD, standard deviation.
Fractional amplitude of low-frequency fluctuations
We found decreased fALFF in ALS patients compared with HC in widespread cortical regions, including motor and sensory regions (bilateral precentral gyrus, p < 0.001; bilateral postcentral gyrus, p < 0.001; and bilateral supplementary motor cortex, p ≤ 0.03) as well as cingulate regions (bilateral anterior cingulate gyrus, p ≤ 0.02; bilateral posterior cingulate gyrus, p ≤ 0.04), occipital and parietal regions (left occipital pole, p = 0.02; bilateral lateral occipital cortex, p ≤ 0.04; right superior parietal lobule, p < 0.001; bilateral supramarginal gyrus, p ≤ 0.02; bilateral precuneus, p ≤ 0.02; and left fusiform gyrus, p = 0.002), and finally, temporal region (left middle temporal gyrus, p = 0.007). Figure 1 illustrates the areas found with decreased fALFF in ALS patients compared with HC. Decreased fALFF in the left precentral gyrus were negatively correlated with disease duration (Spearman's rho = −0.47; p = 0.04, two tailed). By contrast, increased fALFF was found in the right anterior parahippocampal gyrus (p = 0.005) and cerebellum (p ≤ 0.001). Figure 2 illustrates the areas found with increased fALFF in ALS patients compared with HC (Supplementary Tables S1, S2, S3, and S4 for MNI coordinates for Figs. 1 and 2 and statistics, including effect size).
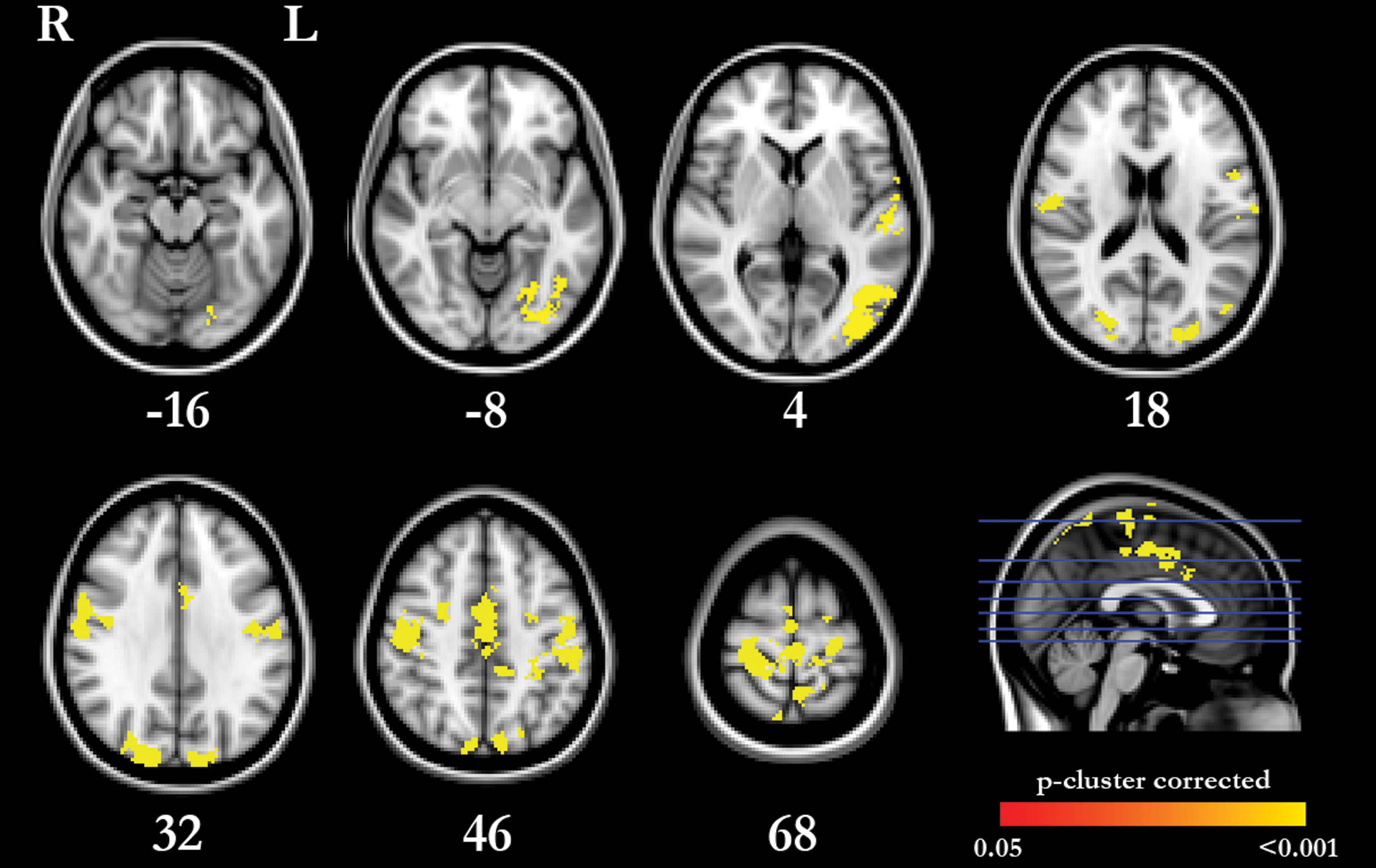
Areas with decreased fALFF in ALS patients compared with HC. Decreased fALFF (fewer fluctuations in the low frequencies) in bilateral precentral gyrus, bilateral postcentral gyrus, bilateral supplementary motor cortex, bilateral anterior and posterior cingulate gyrus, left occipital pole, bilateral lateral occipital cortex, right superior parietal lobule, bilateral supramarginal gyrus, bilateral precuneus, left fusiform gyrus, and left middle temporal gyrus. Blue horizontal lines indicate axial slices. ALS, amyotrophic lateral sclerosis; fALFF, fractional amplitude of low-frequency fluctuation; HC, health controls. Color images are available online.
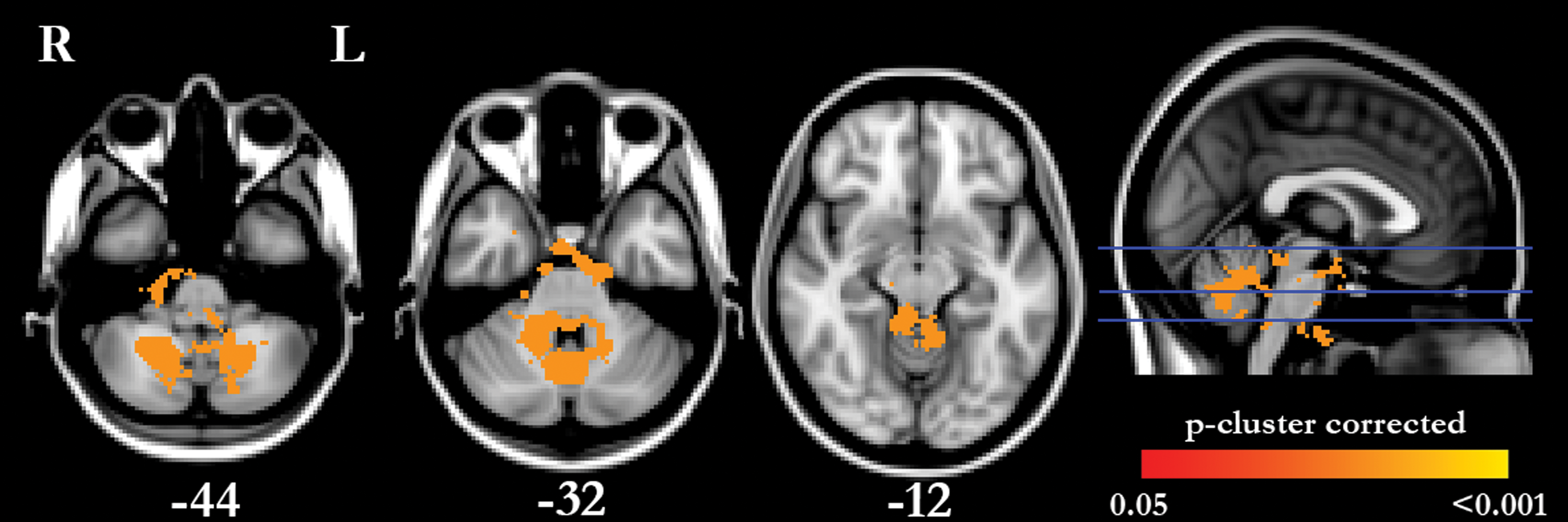
Areas with increased fALFF in ALS patients compared with HC. Increased fALFF (more fluctuations in the low frequencies) in right anterior parahippocampal gyrus and cerebellum. Blue horizontal lines indicate axial slices. Color images are available online.
Regional homogeneity
Decreased ReHo in ALS patients compared with HC was found in sensory motor regions (bilateral precentral gyrus, p < 0.001; bilateral postcentral gyrus, p ≤ 0.03; and bilateral supplementary motor cortex, p < 0.001), cingulate regions (bilateral anterior cingulate gyrus, p < 0.001; bilateral posterior cingulate gyrus, p < 0.001), frontal, occipital, and parietal regions (bilateral superior frontal gyrus, p = 0.003; bilateral occipital pole, p < 0.001; bilateral lateral occipital cortex, p < 0.001; right superior parietal lobule, p < 0.001; bilateral precuneus, p < 0.001; and bilateral fusiform gyrus, p < 0.001), and temporal regions (right middle temporal gyrus, p = 0.02; right inferior temporal gyrus, p < 0.001; and cerebellum, p < 0.001). Figure 3 illustrates the areas where decreased ReHo was found with significant difference between ALS patients and HC. There was a negative correlation between disease duration and decreased ReHo in the right supplementary motor cortex (Spearman's rho = −0.54; p = 0.01, two tailed). Increased ReHo was found in frontal regions (right frontal pole, p < 0.001; right middle frontal gyrus, p = 0.02; and bilateral orbitofrontal cortex, p = 0.03). Figure 4 illustrates the areas where increased ReHo was found with statistical significance between ALS patients and HC (Supplementary Tables S5, S6, S7, and S8 MNI coordinates for Figs. 3 and 4, and statistics, including effect size).
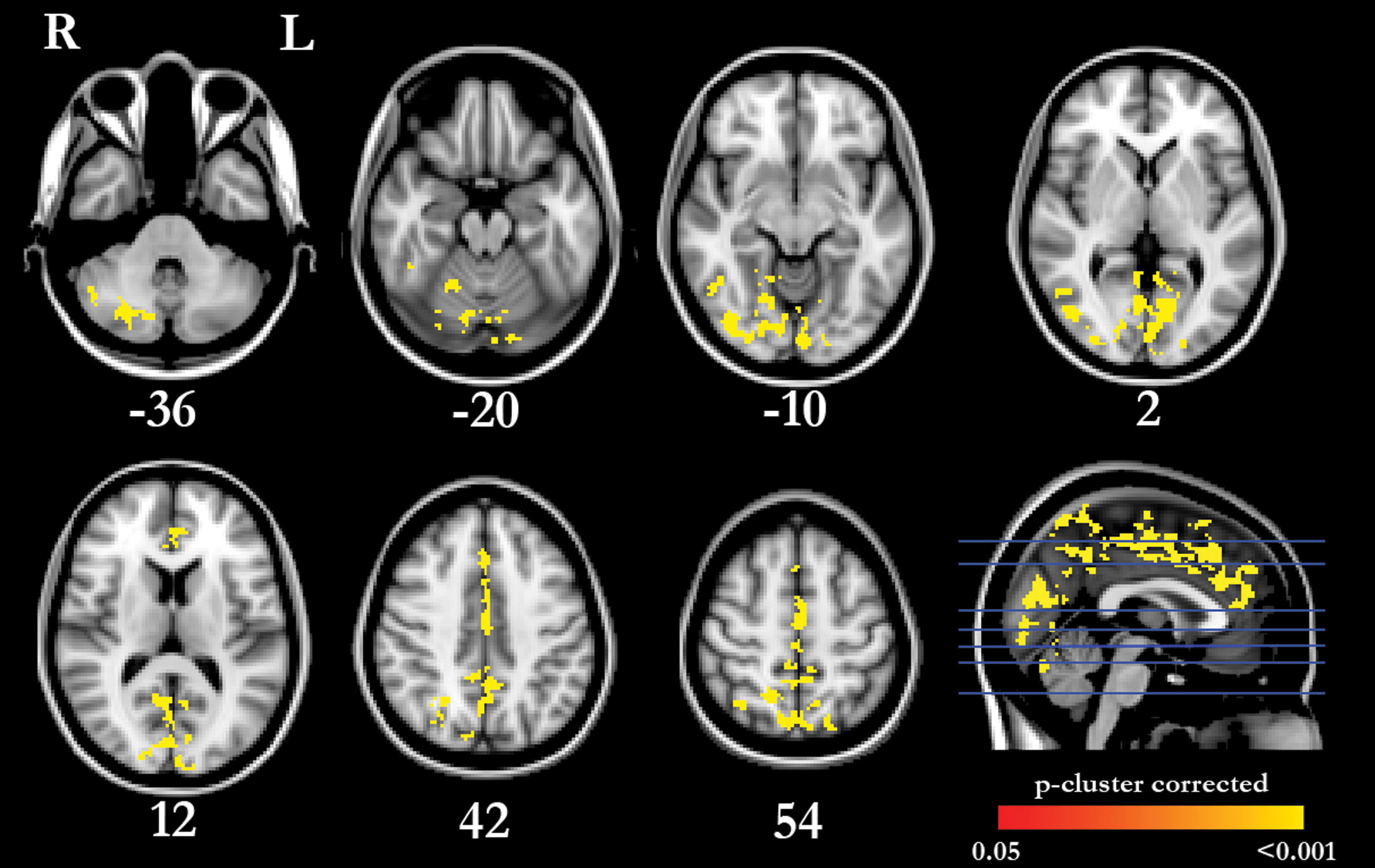
Areas with decreased ReHo in ALS patients compared with HC. Decreased ReHo (fewer fluctuations in the low frequencies) in bilateral precentral gyrus, bilateral postcentral gyrus, bilateral supplementary motor cortex, bilateral anterior and posterior cingulate gyrus, bilateral superior frontal gyrus, bilateral occipital pole, bilateral lateral occipital cortex, right superior parietal lobule, bilateral precuneus, bilateral fusiform gyrus, right middle temporal gyrus, right inferior temporal gyrus, and cerebellum. Blue horizontal lines indicate axial slices. ReHo, regional homogeneity. Color images are available online.
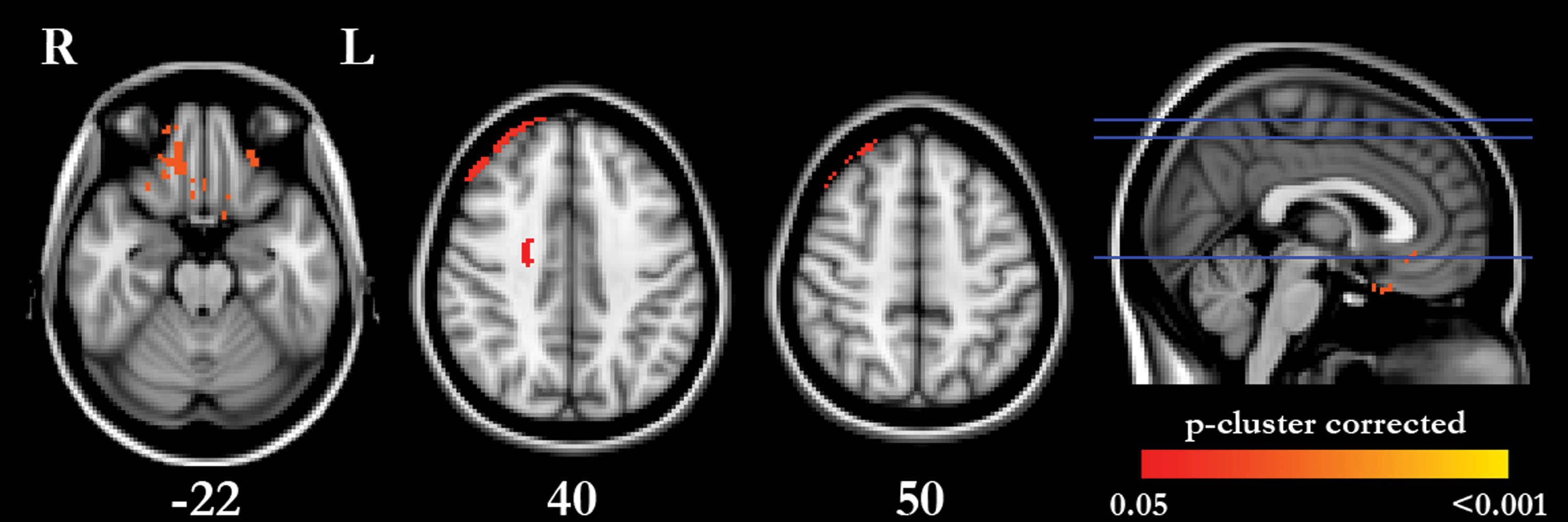
Areas with increased ReHo in ALS patients compared with HC. Increased ReHo (more fluctuations in the low frequencies) in right frontal pole, right middle frontal gyrus, and bilateral orbitofrontal cortex. Blue horizontal lines indicate axial slices. Color images are available online.
Voxel-based morphometry
Regions with significant fALFF and ReHo changes did not present significant differences on modulated GM in the VBM analysis (Supplementary Tables S9 and S10 for VBM results).
Discussion
Unlike most ALS studies investigating functional connectivity in rs-fMRI, in this study, we applied fALFF and ReHo methods to conduct a whole-brain analysis of ALS patients' cerebral low-frequency oscillations and compared with HCs. Our results revealed abnormal neural activity in key nodes of the SMN as well as in components of the default mode network (DMN), frontoparietal network (FPN), salience network (SN), and the cerebellum. Importantly, our results reached statistical significance corrected for multiple comparisons.
Motor symptoms are the hallmark of ALS and, as expected, motor areas were found with changes in both fALFF and ReHo. Decreased fALFF and ReHo in ALS patients were found bilaterally in precentral and postcentral gyrus, as well as the bilateral supplementary motor cortex, all regions considered part of the SMN.
Changes in the connectivity of the SMN are one of the most consistent findings in ALS (Schulthess et al., 2016; Tedeschi et al., 2012; Trojsi et al., 2015; Mohammadi et al., 2009; but see Chenji et al., 2016). In fact, previous studies reported changes in functional and effective connectivity in the SMN of ALS patients (Fang et al., 2016; Trojsi et al., 2015). Components of the SMN were previously indicated as involved in the planning, execution, and controlling of voluntary movements (Biswal et al., 1995). Alterations in this network can help to explain the motor features of the disease, which are corroborated by anatomical deterioration and correlated with disease duration and progression (Agosta et al., 2012; d'Ambrosio et al., 2014; Verstraete et al., 2010). The fALFF and ReHo changes found in our study may help to explain the difficulties ALS patients present in starting and controlling voluntary movements, even before structural damage is established or detectable at MRI.
Similar to Ma et al. (2016) who reported decreased fALFF in middle and inferior occipital gyrus, we report decreased fALFF and ReHo in bilateral occipital pole and bilateral lateral occipital cortex, areas comprising the primary visual cortex. Decreased fALFF were also found in the left fusiform gyrus, while ReHo decrease was found in bilateral fusiform gyrus. Interestingly, Luo et al. (2012) studied ALFF in ALS patients and found a decrease in the fusiform gyrus and inferior occipital lobe. These findings in fusiform and occipital areas together with the changes in postcentral gyrus are suggestive of possible deficits in the sensory system of ALS patients. In fact, changes in visual perception were previously reported in ALS, although not frequently (Strong et al., 1999).
We reported changes in fALFF and ReHo in the DMN, with bilateral posterior division of the cingulate gyrus and bilateral precuneus showing decreased fALFF and ReHo in ALS patients, as well as in bilateral frontal and temporal regions. The DMN is associated with internal processing, including manipulation of episodic memory, theory of mind, and future thinking, and deactivates when the subject engages in any goal-oriented task (Raichle et al., 2001).
Changes in functional connectivity of the DMN are often reported in ALS (Trojsi et al., 2015; Heimrath et al., 2014; Mohammadi et al., 2009; but see Chenji et al., 2016; Schulthess et al., 2016) as well as deficits in memory recall (Machts et al., 2014) and theory of mind (van der Hulst et al., 2015). In addition, attentional and verbal fluency impairments are reported in ALS (Abrahams et al., 2000; Goldstein and Abrahams, 2013) and correlated with changes in the DMN (Heimrath et al., 2014). Posterior cingulate and precuneus are important nodes of the DMN and were found with decreased fALFF and ReHo in the present study. Abnormal activity in the posterior cingulate is documented in rs-fMRI and PET-FDG studies in ALS (Bueno et al., 2018; Matías-Guiu et al., 2016; Mohammadi et al., 2009) as well as functional changes in the precuneus (Loewe et al., 2017; Palmieri et al., 2010).
Despite reports of episodic memory deficits in ALS (Machts et al., 2014), most cognitive impairments are attributed to executive/frontal dysfunctions (Abrahams et al., 2004; Hanagasi et al., 2002). Interestingly, our analyses revealed clusters of fALFF and ReHo changes in frontal areas. Ma et al. (2016) reported the frontal lobe with increased fALFF in middle and superior frontal gyrus. However, no frontal changes in functional connectivity were found in a different study (Heimrath et al., 2014), despite the alterations found in the posterior DMN. Unlike the latter study, Mohammadi et al. (2009) reported decreased activation in frontal regions, but no changes in activation in the temporal region of the DMN.
Despite the controversial results, increased fALFF in temporal regions and ReHo in frontal regions could be speculatively attributed to a compensatory mechanism as suggested elsewhere (Douaud et al., 2011), however, this could also be related to reduced inhibitory function (Zhou et al., 2014). These different results may be explained by the heterogeneous presentation of the disease or the different disease stages of the patients among studies. Interestingly, frontal areas are associated with working memory, which is extensively reported in ALS, and changes in these areas are well documented in the literature (Ellis et al., 2001; Hammer et al., 2011; Hanagasi et al., 2002; Volpato et al., 2010). In sum, these changes in the spontaneous low-frequency oscillations in the DMN could be predictive of cognitive changes in ALS, especially those related to episodic and working memory.
In addition, we report decreased fALFF and ReHo in the supramarginal gyrus and parietal lobule of ALS patients. These changes, in combination with the changes in superior and middle frontal areas reported, may be suggestive of alterations in the FPN, which can be relevant to cognition, including attention, executive processing, and working memory. Similarly, Tedeschi et al. (2010) found functional connectivity decreased in the FPN. Changes in this network could reflect executive dysfunctions often reported in ALS (Abrahams et al., 2005; Christidi et al., 2016).
The anterior cingulate was found with fALFF and ReHo decreased bilaterally in ALS patients compared with HC, despite preservation of the insular cortex. The anterior cingulate is an important node of the SN, which is involved in a variety of functions through the interaction between cognition, emotion, and action [for a review, see Menon (2015)]. Importantly, anterior cingulate is considered to have an important role in selecting voluntary action (Rushworth, 2008). Changes in fALFF and ReHo in this area, having strong direct connections with the spinal cord, can help to explain motor difficulties in ALS. Particularly, anterior cingulate functional changes are reported (Agosta et al., 2013; Mohammadi et al., 2009). However, our results in the anterior cingulate are not in accordance with a previous study reporting increased fALFF in ALS (Ma et al., 2016).
Particularly interesting is the finding of widespread increased fALFF and decreased ReHo (in less proportion) in the cerebellum, reported for the first time. This structure is proved to participate in motor as well as in cognitive and behavioral functions and plays an important role in neurodegenerative diseases, including ALS [Strick et al., 2009; for a review, see Gellersen et al. (2017)]. Functional abnormalities and hypometabolism in the cerebellum are well documented in ALS (Buhour et al., 2017; Ferrer et al., 2016) as well as GM and WM changes, and have proven to correlate with cognitive and behavioral symptoms (Christidi et al., 2017; Tan et al., 2014; Thivard et al., 2007). Clinical motor characteristics and possibly cognitive symptoms could be further explained by the involvement of these fALFF and ReHo changes found in the cerebellum. A detailed study on the fALFF and ReHo changes in the cerebellum areas would be then recommended to better evaluate cerebellar involvement in ALS.
As functional changes are often associated with structural damage, we performed a VBM analysis to control for any confounding influences of GM atrophy. However, no structural differences were found between ALS patients and HCs in the regions presenting fALFF and ReHo changes. This finding of preserved GM supports the idea that functional alterations may precede structural changes as previously suggested (Trojsi et al., 2015). Interestingly, ALS patients and controls did not differ in any cognitive domain measured by the ACE-R, except for language. The absence of atrophy might explain the relatively preserved cognition of our patients and also corroborates other studies showing that GM changes in ALS are less present than in conditions such as frontotemporal dementia (FTD) or ALS-FTD (Lillo et al., 2012). However, the functional changes detected might indicate that cognitive changes could be developing and be detected in later stages as well as structural damage.
Lower ReHo was previously associated with longer disease duration and higher disease severity (Zhou et al., 2014). Functional connectivity changes in ALS were reported as related to disease duration (Chenji et al., 2016). In our study, decreased fALFF and ReHo were negatively correlated with disease duration, corroborating previous findings suggesting that these measures could be used as biomarkers for disease progression and severity (Zhou et al., 2014).
Furthermore, Schulthess et al. (2016) report functional changes in a large cohort in different networks, and suggest that these changes may follow the distribution of TDP-43 pathology in stages (Brettschneider et al., 2013). This pathology distribution in stages has been recently discussed in a statistical meta-analyses of diffusion tensor imaging (DTI) studies (Gorges et al., 2018) supporting the hypothesis that ALS pathology is disseminated by axonal projections (Braak et al., 2013), an idea corroborated by recent DTI studies (Kassubek et al., 2014, 2017). Importantly, our results of widespread fALFF and ReHo changes are compatible with changes in functional connectivity demonstrated in other studies (Schulthess et al., 2016; Tedeschi et al., 2012; Trojsi et al., 2015) and may indicate that these resting-state changes may be potentially related to the spread and location of TDP-43 pathology, although in our study we show no evidence of the sequence the pathology follows.
However, some limitations should be addressed in this study. First, there is the small size of our sample that limits the generalization of the results. Further studies considering a larger sample or providing enough statistical power will be necessary to better investigate the prevalence of our findings. However, such a small sample is often found in the neurodegeneration literature, including studies evaluating the fMRI measures here studied (Luo et al., 2012; Wang et al., 2015, 2016). Another important limitation is the lack of clinical measures (e.g., ALSFRS-R) to better characterize the physical disability of our patients.
The lack of specific neuropsychological measures to indicate any potential correlation with changes in fALFF and ReHo limits the interpretation of our findings. However, regarding cognitive measures, although the ACE-R is not the most indicated battery for cognitive screening in ALS, our study excluded patients with diagnosis of dementia and included one neuropsychological measure, when the existing literature of fALFF and ReHo in ALS does not present any cognitive data (Luo et al., 2012; Ma et al., 2016; Zhou et al., 2014). The pattern of changes in spontaneous low-frequency oscillations in the resting brain of ALS patients and the relationship with cognitive performance and TDP-43 pathology should be explored in the future to better characterize the pathophysiology of ALS. In addition, the results reported as increased ReHo, as shown in Figure 4, may lead to misinterpretation in the prefrontal cortex since it is not possible to discriminate actual neural changes from template mismatching or edge artifacts.
A question remains if in presymptomatic patients or in early stages of the disease these alterations in fALFF and ReHo would be present and if they could potentially be used as biomarkers to indicate the spread of TDP-43 pathology. More studies are warranted to clarify the relationship between these functional changes and depositions of TDP-43, as well as with the presence of cognitive impairments.
Footnotes
Acknowledgments
The authors thank Dr. Donnie Cameron and Dr. David Willis from Norwich Medical School for their help with the Supplementary Data. Funding: A.P.A.B. is supported by the São Paulo Research Foundation (FAPESP) grant 2016/19376-9.
Ethical Approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee (Human Research Ethics Committee of South Eastern Sydney/Illawarra Area Health Service) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all individual participants included in the study or from a close relative.
Authors' Contribution
A.P.A.B. performed image preprocessing, data and statistical analyses, and drafted and wrote the final version of the article; W.H.L.P. participated in the VBM preprocessing; K.R. conceived the study; L.C.d.S. drafted the article; M.H. drafted the article; and J.R.S. conceived the study and participated in image preprocessing and statistical analyses. All authors have read and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.