
Abstract
Background:
White matter hyperintensities (WMHs) indicate active small vessel disease. Emerging evidence suggests that confluent WMH (C-WMH) results in greater cognitive impairment compared with nonconfluent WMH (NC-WMH) visualized as punctate lesions. However, the mechanism linking C-WMH and early cognitive impairment is not clearly understood.
Aims:
To investigate the effects of C-WMH and NC-WMH on whole-brain functional connectivity (FC) across 138 regions of interest (ROIs) and cognition in 63 subjects with mild cognitive impairment (MCI).
Methods:
MCI subjects were classified as C-WMH or NC-WMH using the Staals criteria on the Fazekas WMH scale. Group-level ROI-to-ROI FC trends and differences based on WMH subtypes were computed using standard resting-state functional magnetic resonance imaging analysis. Global cognitive performance was measured with mini-mental state examination (MMSE).
Results:
Subjects with C-WMH exhibited increased inter-regional FC in the fronto-parietal, fronto-occipital, parieto-occipital, and temporo-parietal regions of the salience, dorsal-attention, default-mode, and visual networks compared with NC-WMH. Increased intra-regional FC was also observed within the frontal and parietal lobes in C-WMH. In addition to widespread increased FC in C-WMH, a few regions in the fronto-temporal and intra-frontal areas demonstrated reduced FC in C-WMH compared with NC-WMH. Analyses of cognitive correlates demonstrated increased parieto-occipital FC to be negatively associated with MMSE in the C-WMH. The increased parieto-occipital FC may be related to loss of higher order inhibitory control in the parieto-occipital regions induced by C-WMH or alternatively a compensatory mechanism to FC alterations induced by C-WMH.
Conclusion:
C-WMH in subjects with MCI is associated with widespread increase in intra- and inter-regional FC. These findings provide novel insights into divergent FC related to confluence of WMH in MCI.
Impact statement
White matter hyperintensities (WMHs) have been demonstrated to be a major risk factor for progressive cognitive decline. However, the relationship between structural and functional brain changes related to different types of WMH lesions as well as different stages of WMH progression remains unclear. In this study, we demonstrate that confluent WMH is significantly associated with divergent functional connectivity changes in patients with mild cognitive impairment (MCI). This finding may allow identification of MCI subjects who are adversely affected by WMH and thus provides a window of opportunity to introduce pharmacological and nonpharmacological interventional measures.
Introduction
Presence of white matter hyperintensity (WMH) is believed to be a manifestation of small vessel cerebrovascular disease (CeVD) (Gouw et al., 2011; Pantoni and Garcia, 1997; Wardlaw et al., 2015). WMH is classified as confluent (C-WMH) when there is progressive coalescence of punctate or nonconfluent (NC-WMH) lesions (Fazekas et al., 1987; Staals et al., 2014). Importantly, WMH often coexists with Alzheimer's disease (AD) pathology, and has been reported to accelerate cognitive decline and increase the rate of progression to dementia (Mortamais et al., 2014; Prins et al., 2013; Tosto et al., 2014; Van Straaten et al., 2008; Vemuri and Knopman, 2016). However, in patients with mild cognitive impairment (MCI), the effect of the subtypes of WMH on disease progression remains unclear. C-WMH has been shown to correlate to lacune count, and suggested to represent active ongoing occlusion of arterioles with greater clinical and cognitive consequences compared with NC-WMH (Ghaznawi et al., 2019; Silbert et al., 2012; Staals et al., 2014; Van Dijk et al., 2008). However, the mechanism by which C-WMH results in cognitive decline remains unclear.
Emerging functional magnetic resonance imaging (fMRI) studies related to CeVD pathology have mainly investigated the effects of high WMH burden on functional connectivity (FC), and have largely used seed-based approaches to assess FC alterations in key regions of executive control and the default mode network (DMN) (Benson et al., 2018; Chong et al., 2017; De Marco et al., 2017; Sheline and Raichle, 2013; Vipin et al., 2018; Ye et al., 2019). In this regard, intra-regional FC abnormalities suggest disruption to local neural function network, while inter-regional FC abnormalities suggest widespread disruption to neural networks (Wang et al., 2015). However, effects of subtypes of WMH, namely C-WMH versus NC-WMH, on whole-brain ROI-to-ROI FC alterations in MCI remain to be elucidated. Therefore, we evaluated intra- and inter-regional network-level FC alterations related to subtypes of WMH in individuals with MCI using a whole-brain seed-based ROI-to-ROI FC approach. We hypothesized that C-WMH would show greater intra- and inter-regional FC alterations compared with NC-WMH. In addition, we hypothesized that these FC alterations would be associated with cognitive performance.
Methods
Participants
Subjects included in this study were recruited from the memory clinic of the National Neuroscience Institute, Singapore between August 2013 and January 2018. The subjects were part of the Singapore Young Onset Dementia Cohort (SYNC) Study. Diagnosis of MCI was made by cognitive neurologists based on the NIA-AA and Petersen criteria (Albert et al., 2011; Petersen, 2004). MCI subjects presented with cognitive symptoms, and had deficits on their neuropsychological evaluation and had a clinical dementia rating score of 0.5. Only MCI subjects demonstrating the presence of C-WMH or NC-WMH on their fluid-attenuated inversion recovery (FLAIR) magnetic resonance imaging (MRI) were included in this study. All subjects were administered the standard mini-mental state examination (MMSE) battery by trained assessors to measure their global cognitive performance (Folstein et al., 1983). The institutional review board (IRB) named SingHealth Centralized Review Board approved this study. Informed consent was obtained according to the Declaration of Helsinki from subjects or their next of kin if they were incapable of giving consent, as deemed appropriate by the neurologists and clinical psychologists.
MRI protocols
The T2-weighted FLAIR, 3D T1-weighted magnetization-prepared rapid gradient echo (MPRAGE), and 5 min resting-state blood-oxygen-level-dependent (BOLD) fMRI sequences were acquired on a 3T Tim Trio system (Siemens Erlangen, Germany) scanner. The FLAIR MRI sequence was acquired with repetition time of 5000 ms, echo time 387 ms, inversion time 1800 ms, flip angle 120, 1 mm slice thickness, 192 slices, 1 × 1 × 1 mm voxel size. The 3D T1 MPRAGE structural sequence was acquired with repetition time of 2300 ms, echo time 2.28 ms, inversion time 900 ms, flip angle 8, 1 mm slice thickness, 192 number of slices, 1 × 1 × 1 mm voxel size. Finally, the fMRI scan was acquired with repetition time of 2000 ms, echo time 30 ms, flip angle 90, 3 mm slice thickness, 36 slices in continuous acquisition order, with 3 × 3 × 3 mm voxel size, and total 240 volumes.
Classification of C-WMH and NC-WMH
The FLAIR scans were visually rated by two trained raters on WMH severity based on the modified Fazekas scale (Fazekas et al., 1987), where periventricular WMH (PVH) and deep subcortical WMH (DWMH) are separately rated on a 0- to 3-point scale for both hemispheres. The scoring criteria were as follows: For PVH, absence of any WMH = 0; presence of caps or pencil-thin lining = 1; a smooth halo along the edges of the lateral ventricle = 2; irregular hyperintensities extending into deep white matter = 3. For DWMH, absence of any WMH = 0; presence of nonconfluent foci of WMH in the deep subcortical region = 1; beginning confluence of WMH foci = 2; presence of large confluent areas = 3. Any discrepant MRI visual-rating score was resolved by consensus. Subjects were classified as having C-WMH and NC-WMH based on the Staals criteria (Staals et al., 2014): Subjects with WMH rating of 3 in either periventricular and/or a rating of 2 or 3 in deep white matter (WM) regions on either hemisphere were assigned to the C-WMH group (n = 33) and the rest to the NC-WMH group (n = 30).
Quantification of C-WMH and NC-WMH
We used Lesion Segmentation Toolbox (LST version 2.0.15), a statistical parametric mapping package (SPM12 version 7487 from the Wellcome Trust Centre for Neuroimaging, Institute of Neurology, UCL, London, United Kingdom) based tool for WMH detection, to extract binary WMH lesion belief maps (Paul et al., 2012; Penny et al., 2007). We employed the automated lesion growth algorithm from LST on T1 anatomical and FLAIR images to quantify WMH as reported previously (Benson et al., 2018; De Marco et al., 2017; Ye et al., 2019). The algorithm first coregisters the T2 FLAIR to T1, and subsequently segments T1 images into gray matter (GM), WM, and cerebrospinal fluid (CSF) tissue maps. The information is then combined with the coregistered T2 FLAIR images to estimate the WMH lesion belief maps. By thresholding these maps with a predetermined initial kappa threshold (κ), an initial binary lesion map is obtained and is subsequently grown along voxels that appear hyperintense on the T2 FLAIR image. To define the optimal threshold, T1 and FLAIR images of 10 randomly chosen subjects with mild-to-severe WMH burden were segmented at κ = 0.3, κ = 0.2, and κ = 0.10. After further visual inspection of segmentation results at these threshold levels, the WMH visual raters determined κ = 0.10 as the optimal threshold.
To obtain the mean WMH mask image for C-WMH and NC-WMH groups in the standard Montreal Neurological Institute (MNI) space for FC overlay, the binary WMH probability maps extracted at κ = 0.10 were used to first fill hypointense WMH regions in T1 anatomical images using LSTs lesion filling technique (Paul et al., 2012). The WMH lesion filling in T1 structural MRI was also necessary for accurate FC analysis as not doing so would have resulted in WMH lesion volumes being misclassified as GM during fMRI preprocessing as has been previously reported (Levy-Cooperman et al., 2008). The lesion-filled T1 images were further segmented to obtain the deformation fields that were subsequently applied to the binary WMH lesion images to normalize them to the MNI using SPM. Finally, using SPMs image calculator (ImCalc) utility, mean C-WMH and NC-WMH masks were generated to give approximate location and size of WMH lesions for FC overlay.
To extract total and regional WMH volumes in MNI space, we generated frontal, parietal occipital, and temporal lobe masks in MNI space using SPM-based Wake Forest University's (WFU) Pickatlas toolbox (Maldjian, 1994). Subsequently, total and regional WMH volumes were computed using SPM.
fMRI image preprocessing
Resting-state FC analysis was performed using the connectivity analysis toolbox (CONN version 18b) (Whitfield-Gabrieli and Nieto-Castanon, 2012). Using CONNs default preprocessing pipeline with minor modification, fMRI data were realigned for motion estimation, coregistered to patient's lesion-filled T1 anatomical image, segmented into GM, WM, and CSF tissue classification, normalized to the MNI space and spatially smoothed with an 8 mm full-width-half-maximum Gausian kernel. The BOLD signal from the first four volumes of fMRI (initial 8 sec of scan) was discarded to account for the hemodynamic response pulse stabilization during the early scan. Subsequently, default FC analysis pipeline steps were performed as follows: the resting-state BOLD signal was band-pass filtered (0.008–0.09 Hz) and processed through the anatomical component correction algorithm (aCompCor) for physiological noise filtering in CONN (Behzadi et al., 2007). The Artifact Detection Tool algorithm implemented in CONN was used to identify and regress out outlier scans exceeding three standard deviations in mean global intensity and frame-to-frame differences exceeding 0.5 mm. The time series from WM and CSF, motion parameters, and artifact-outlier scans were used as regressors in the first-level FC analysis to reduce the influence of motion and physiological noise. We used CONNs predefined 138 GM seeds as regions of interest (ROIs) for whole-brain connectivity analysis. These CONN ROIs are based on cortical and subcortical brain parcellations from the FSL Harvard-Oxford atlas and an atlas of commonly used functional network nodes by CONN. The CONN functional network atlas comprised of DMN, sensorimotor, visual, salience, dorsal attention, frontoparietal, language, and cerebellar network seeds (e.g., medial prefrontal cortex, bilateral intraparietal sulcus, and posterior cingulate cortex nodes for the DMN). The ROI seeds as implemented in CONN have no specific size or shape, but take MNI coordinates from the center of the mass of each atlas ROI and use mean BOLD signal times series from all voxels of the parcellated region to compute bivariate correlation coefficients using the weighted-general linear model approach, and obtain subject-level ROI-to-ROI FC.
Statistical analyses
We performed a chi-square test on sample sex and two-sample t-tests on age, education, MMSE score, total Fazekas WMH visual rating score, regional and total WMH volumes to ascertain between-group differences. In the second-level seed-based FC analysis, we created an analysis of covariance (ANCOVA) model in CONN where groups were modeled as separate covariates and sample age, sex, total WMH, and GM volumes were included as covariates to control for intersubject variability. Here, the subject-level FC maps from subject-level analysis were entered to compute significant NC-WMH and C-WMH group-level ROI-to-ROI FC trends and between-group connectivity differences. The FC values (Fisher z-transformed correlation coefficients) were extracted from statistically significant ROI-to-ROI pairs at false discovery rate (FDR) correction p < 0.05. The z-scores from each ROI pair of C-WMH and NC-WMH groups illustrating significant FC differences were used to assess their relationship with MMSE in Pearson's correlation analysis.
Results
Sample characteristics
Table 1 summarizes the group-level sample characteristics. Of 63 subjects included in this study, 33 were classified as C-WMH and the remaining 30 as NC-WMH. The mean age and mean education of the C-WMH group were 63.39 ± 9.05 and 12.21 ± 4.04, respectively. Similarly, for the NC-WMH, the mean age and education were 61.22 ± 7.53 and 12.57 ± 4.14, respectively. There were no significant differences in age and education level between C-WMH and NC-WMH groups (p > 0.05). The mean MMSE score for C-WMH was 27.56 ± 1.48 (score range 25–30) and for NC-WMH it was 27.79 ± 1.73 (score range 26–30). The MMSE scores were not significantly different between the C-WMH and NC-WMH groups suggesting comparable cognition levels. The total Fazekas WMH visual rating scores were significantly different between the groups, with the C-WMH group showing a higher overall WMH visual rating score than the NC-WMH. Likewise, compared with NC-WMH, subjects with C-WMH also had significantly higher number of lesions, total and lobe-wise WMH volumes (p < 0.05).
Sample Demographic and Characteristics
Bold values in p-Value column indicate significant differences between C-WMH and NC-WMH groups at p < 0.05.
The values represent mean ± standard deviation (range) unless otherwise indicated. The total and regional WMH volumes are measured in milliliters.
Two-sample t-test was performed on all sample characteristics to estimate between group differences.
Chi-square test was carried out on sex.
Indicates subset of subjects (n = 27) with missing or outliers cognition data removed from C-WMH.
Indicates subset of subjects (n = 28) with missing or outlier cognition data removed from NC-WMH.
C-WMH, confluent white matter hyperintensity; F, female; l, left; M, male; MMSE, mini-mental state examination; NC-WMH, nonconfluent white matter hyperintensity; r, right; WMH, white matter hyperintensity.
Differential resting-state FC alterations related to C-WMH and NC-WMH
Figure 1 summarizes the whole-brain group-level ROI-to-ROI FC differences between C-WMH (Fig. 1a) and NC-WMH (Fig. 1b). Subjects with C-WMH exhibited widespread inter-regional FC increases in the frontoparietal, fronto-occipital, parieto-occipital, and temporoparietal regions (FDR-corrected p < 0.05, Fig. 1a, FC pairs in red) compared with NC-WMH (FDR-corrected p < 0.05, Fig. 1b, FC pairs in blue). When considering the frontoparietal inter-regional FC differences, the right frontal orbital region (r-FOrb) showed increased connectivity with dorsal-attention network seeds, namely the bilateral intraparietal sulcus (l-DorsalAttention IPS and r-DorsalAttention IPS), right superior parietal lobule (r-SPL), and right anterior supramarginal gyrus (r-aSMG) in subjects with C-WMH. At the fronto-occipital level, the left supracalcarine cortex (l-SCC) showed increased connectivity with salience network seed left anterior insula (l-Salience AInsula), indicating increased salience-visual network FC. At the parieto-occipital level, increased FC was observed between left supramarginal gyrus seeds l-Salience SMG, l-aSMG, l-pSMG and occipital lobe seeds bilateral intracalcarine cortex (l-ICC, r-ICC), bilateral supracalcarine cortex (l-SCC, r-SCC), Visual Medial, r-Cuneal, and the right lingual gyrus (r-LG) in subjects with C-WMH. Likewise, the l-aSMG showed increased FC with left temporal occipital fusiform cortex (r-TOFusC) and left occipital fusiform gyrus (l-OFusG). At the temporoparietal level, the right temporo-occipital inferior temporal gyrus (r-toITG) displayed increased FC with DMN seeds posterior cingulate, precuneus and l-aSMG showed increased FC with right posterior superior temporal gyrus (r-pSTG). The C-WMH group also showed increased intra-regional FC within the frontal and parietal regions. Within the frontal lobe, r-FOrb showed increased FC with salience network seed anterior cingulate cortex (Salience ACC), dorsal-attention network seed left frontal eye field (l-DorsalAttention FEF), and left juxtapositional lobule cortex formerly known as supplementary motor cortex (l-SMA). Similarly, within the parietal lobe, r-PostCG showed increased FC with left supramarginal gyrus seeds l-Salience SMG, l-aSMG, l-pSMG, and l-aSMG showed increased FC with right superior lateral occipital cortex (r-sLOC). While most regions showed an increase in FC in subjects with C-WMH, a reduction in FC was also observed within the frontal and between the frontotemporal regions (FDR-corrected p < 0.05, Fig. 1a, FC pairs in blue) compared with NC-WMH (FDR-corrected p < 0.05, Fig. 1b, FC pairs in red). Within the frontal lobe, r-FOrb showed reduced FC with the language network seed, namely the left inferior frontal gyrus (l-Language IFG). The r-FOrb further showed reduced FC with temporal regions, namely the right temporal pole (r-TP), right anterior middle temporal gyrus (r-aMTG), left posterior middle temporal gyrus (l-pMTG), and left anterior and posterior inferior temporal gyrus (l-aITG, l-pITG). The predominant widespread increase in intra- and inter-regional FC in the C-WMH remained significant even after correcting for WMH and GM volumes in the ANCOVA model.
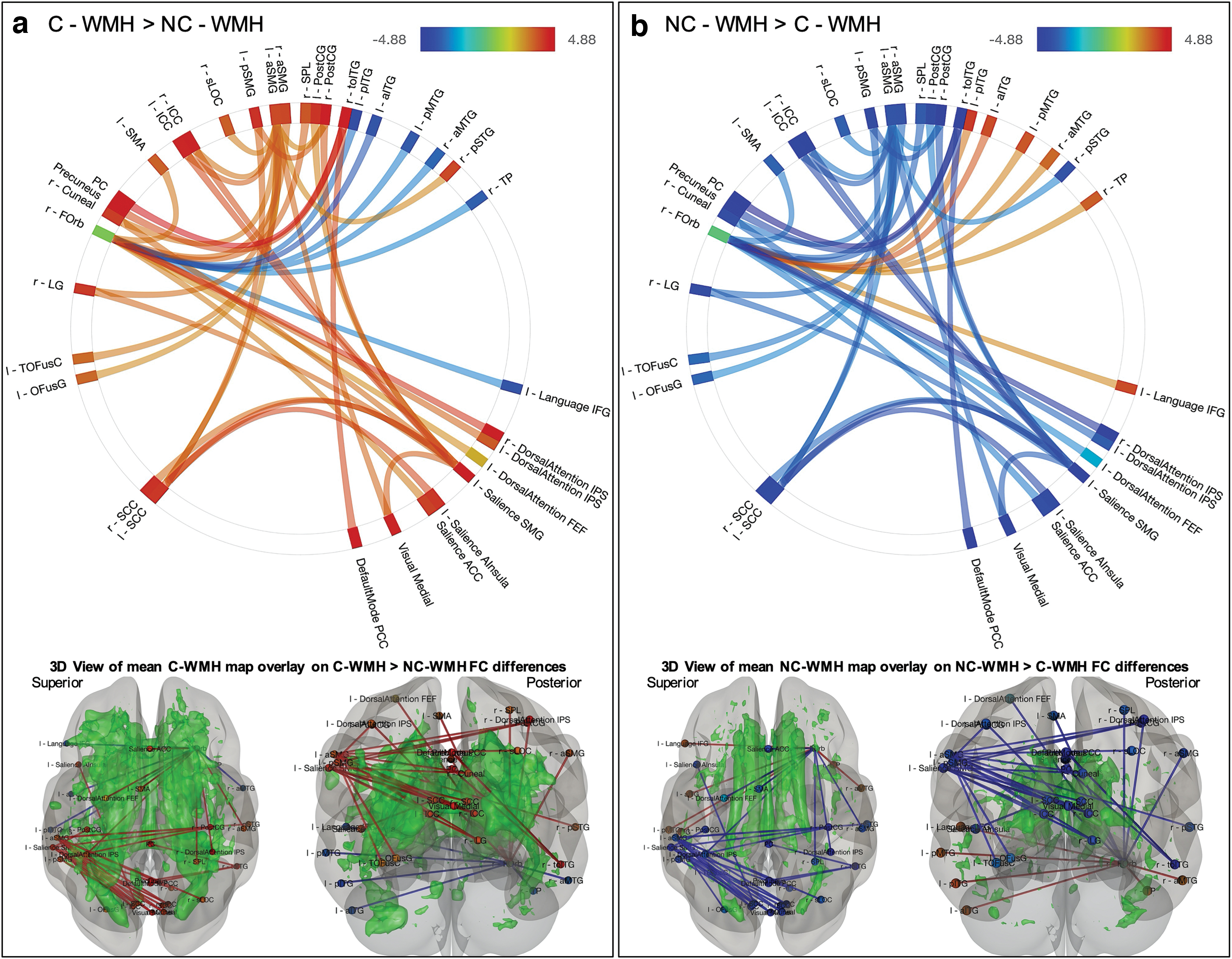
Group-level FC differences in C-WMH and NC-WMH (p < 0.05 FDR corrected). The FC increases between ROI pairs are illustrated in red, and FC reductions are illustrated in blue.
Association of cognition with WMH and FC
Performance on the MMSE was not significantly different between the C-WMH and NC-WMH groups; however, Pearson's correlation revealed a negative correlation between MMSE score and increased parieto-occipital FC only in the C-WMH (p < 0.05 uncorrected). Specifically, the FC of l-Salience SMG with r-SCC (R = −0.441, p = 0.021), r-ICC (R = −0.399, p = 0.039), Visual Medial (R = −0.496, p = 0.009), r-Cuneal (R = −0.484, p = 0.01), and r-LG (R = −0.382, p = 0.049) showed correlations with MMSE.
Discussion
This study evaluated the differential effects of C-WMH versus NC-WMH burden on whole-brain ROI-to-ROI FC in MCI. Subjects with C-WMH predominantly exhibited widespread increased inter-regional FC in the frontoparietal, fronto-occipital, parieto-occipital, frontotemporal, and parietotemporal regions compared with NC-WMH. Likewise, the C-WMH also showed increased intra-regional FC within the frontal and parietal lobes. Besides the widespread increased FC in subjects with C-WMH, reduction in FC was observed within the frontal and between the frontotemporal regions. In addition, we demonstrated that increased parieto-occipital FC in the C-WMH was negatively associated with cognitive performance on the MMSE. The increased parieto-occipital FC may be related to loss of higher order inhibitory control in the parieto-occipital regions induced by C-WMH or alternatively a compensatory mechanism to FC disruptions induced by C-WMH.
C-WMH showed greater inter-regional FC alterations between frontoparietal, fronto-occipital, parieto-occipital, parietotemporal, and frontotemporal regions belonging to higher order functional networks, including the salience, dorsal attention, visual, and DMN. Furthermore, the C-WMH group displayed intra-regional FC alterations in the frontal and parietal regions. Studies have previously demonstrated increased intra- and inter-regional FC in healthy controls and MCI subjects with CeVD as compensatory functional mechanism related to WMH burden (Benson et al., 2018; De Marco et al., 2017; Lockhart et al., 2015; Shi et al., 2017; Ye et al., 2019). In summary, we demonstrate greater intra- and inter-regional connectivity in regions belonging to higher order functional networks, including the salience, dorsal attention, visual, and DMN. Our findings support an emerging framework whereby increases in FC, in MCI, may indicate a mitigatory response to compensate for C-WMH burden (Benson et al., 2018; De Marco et al., 2017; Lockhart et al., 2015; Ye et al., 2019).
Our findings demonstrate that the increased parieto-occipital inter-regional FC negatively correlated with MMSE scores only in the C-WMH group. In this regard, previous studies show that the preservation and maintenance of brain function rely on multiple brain regions that connect and interact with each other (Chand et al., 2017; He et al., 2007; Wee et al., 2012). However, uncertainty remains whether FC alterations arising from cerebrovascular pathology are all compensatory, or could these be consequences of damage to higher order inhibitory control centers. For instance, at the MCI stage, increased inter-regional FC alterations have been associated with preservation of better cognition in MCI subjects with high WMH burden (Benson et al., 2018; Ye et al., 2019). Other studies using only FC measures to investigate cognitive decline at prodromal AD stage have also consistently found similar mitigatory effects of increased intra- and inter-regional connectivity on cognition (Franzmeier et al., 2017a,b,c). To the contrary, literature also suggests that some FC alterations could be abnormal functional mechanism pertaining to disease severity, which may ultimately affect cognition (Chen et al., 2019; Ding et al., 2015). Such FC alterations may be related to the loss of higher order inhibitory control in affected brain regions (Celone et al., 2006; Drzezga et al., 2005). Indeed, our results provide further support to previous findings, which illustrate that the brain actuates a compensatory response to C-WMH burden through dissociable intra- and inter-regional FC alterations, specifically in the early stages of the disease to maintain the cognition levels. However, some parieto-occipital FC alterations could be related to dysfunctional inhibitory control in these regions reflecting disease severity. It is likely that further progression of WMH would result in disruption to WM tracts with consequent reduction in intra- and inter-regional FC (Brier et al., 2012; Reijmer et al., 2015; Taylor et al., 2017). At this stage, cognitive worsening and progression from MCI to dementia can be expected (Brier et al., 2012; Celone et al., 2006; Inaba et al., 2011; Sperling et al., 2010; Van Dijk et al., 2008; Van Straaten et al., 2008).
Strengths and limitations
The strengths of our study include the use of whole-brain ROI-to-ROI FC method to obtain FC alteration patterns in WMH subtypes in MCI. In addition, although the groups were not age matched, age differences were accounted for in all the FC analysis. Our study has some limitations as well. This was a cross-sectional study in a relatively small sample, and we did not follow these subjects to track their cognitive and functional brain differences in a longitudinal manner. Hence, these findings need to be validated using a larger cohort of MCI subjects with follow-up time points. Using only MMSE as a measure of cognition and correlation with FC is also a limitation, and more detailed cognitive measures need to be assessed in future studies to analyze this relationship. Finally, since no amyloid imaging was available for this cohort, we are unable to perform correlations between FC and disease pathology. Nonetheless, the observed effects of C-WMH and NC-WMH burden on FC in this study provide novel insights into the divergent relationship between WMH subtypes, FC, and cognition in MCI.
Conclusion
The results from this study highlight the important role of C-WMH and NC-WMH in whole-brain FC. Increased inter-regional FC in higher order functional networks in MCI subjects with C-WMH may be a compensatory mechanism to attenuate the detrimental effects of CeVD or a reflection of damage to higher order inhibitory control centers. Our findings provide novel insights into divergent nature of functional alterations related to the confluence of WMH in MCI.
Footnotes
Authors' Contributions
D.K. contributed to the study concept, design, MRI visual rating, imaging data processing, statistical analysis, interpretation, and drafting of the article. A.V. provided scientific input to data analysis and revised the article for intellectual content. B.W. performed data collection and MRI visual rating. K.P.N. performed data collection, and revised the article for the intellectual content. N.K. also contributed to study concept, design, data collection, interpretation, and revising of the article for the intellectual content.
Acknowledgments
The SingHealth Centralized Review Board approved this study (CIRB Reference No. 2015/2218). All participants provided written informed consent according to the Declaration of Helsinki. We are grateful to the participants who took part in this study, the team at the National Neuroscience Institute and Duke-NUS for their assistance with data collection and supporting this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was conducted at the National Neuroscience Institute and funded by National Medical Research Council of Singapore, grant number NMRC/CIRG/1416/2015.