
Abstract
Background:
Patients with age-related sensorineural hearing loss (HL) may benefit from auditory input amplification by using hearing aids (HAs). However, the impact of both HL- and HA-based rehabilitation on central auditory functional connectivity (FC) is not clear.
Methodology:
Sixty-two HL (22 females, aged 64.4 ± 7.6 years, pure-tone average 50.9 ± 14.7 dB right ear, 50.7 ± 12.9 dB left ear) and 32 normal hearing (NH) subjects (22 females, aged 59.3 ± 7.3 years) were examined in a 3T magnetic resonance imaging (MRI) study. HL patients were analyzed cross-sectionally at baseline (vs. NH subjects) and longitudinally at 6-month follow-up. Between the 2 scans, 31/62 patients used the HA 9.5 ± 3.8 h a day. Arterial spin labeling and blood oxygen level-dependent resting-state functional MRI were performed to measure regional perfusion in the primary auditory cortex and, from here to the whole brain, seed-based FC was performed. Before each scan, HL patients underwent audiological and neurological assessments.
Results:
At baseline, the HL condition was associated with regional hypoperfusion in right Heschl's gyrus (seed) and negative seed-based FC (anticorrelation) in posterior brain regions. Long-range FC in the precuneus correlated negatively with pure-tone and speech reception average thresholds. At 6-month follow-up, HA usage was associated with seed-based FC increase in the right superior frontal gyrus (SFG) and seed-based FC reduction in the right middle temporal gyrus. Long-range FC changes in the SFG correlated positively with executive function improvements.
Conclusions:
These findings suggest that HA-based rehabilitation may not reverse HL-related neural effects and yet carry neurological benefits by retuning long-range FC of the auditory system.
Impact statement
Age-related sensorineural hearing loss (HL) affects 40% to 60% of the worldwide population and a common, viable rehabilitation strategy is to provide auditory input amplification through hearing aids (HAs).
By targeting metabolically depressed, auditory cortical centers, our work reveals a possible neural link between peripheral and central vulnerability in HL patients in the form of aberrant, long-range, functional connectivity effects. Similarly, we unveil how wearing HAs for 6 months may induce neuroplastic changes that positively correlate with improved neuropsychological performances.
Introduction
Age-related sensorineural hearing loss (HL) is one of the most common disorders affecting older adults and a major cause of chronic disability in the elderly (Michels and Duffy, 2019). HL symptoms are typically ascribed to impairment of the peripheral auditory system (i.e., outer, middle, and inner ear and cranial nerves) with reduced collection, amplification, and transduction of sound waves causing reduced input into the central nervous system. However, more recently, HL has also been linked to morphological (Eckert et al., 2019; Lin et al., 2014), functional (Wolak et al., 2019; Xu et al., 2019a), and metabolic (Ponticorvo et al., 2019; Verger et al., 2017) changes in the central auditory pathway (i.e., subcortical nuclei and auditory cortex), resulting in reduced perception and integration of acoustic information streams (Golub, 2017).
HL patients may benefit from rehabilitation with cochlear implant and acoustic hearing aid (HA) devices. Although patients must adapt to their use (Chang et al., 2016; Dawes and Munro, 2017), these devices allow to experience significant auditory input amplification during work-related and social activities, and an improvement in general hearing (Barbosa et al., 2015; Pichora-Fuller and Singh, 2006) and cognitive abilities (Amieva et al., 2015) has been previously observed in HA users. Particularly, the use of HAs may improve not only speech perception, listening abilities, and quality of life (Sarant et al., 2020) but also working memory, executive functions, attention, and visual learning (Anderson, 2019).
Consequently, it has become crucial to address if, and eventually understand how, the prolonged exposure to HA-mediated auditory input amplification would also trigger functional changes in the brain, both locally, within the primary auditory cortex (i.e., the cortical entry point of sensorineural signals), and globally, within the whole-brain pattern of neural communications between primary auditory and higher order brain regions. To tackle the first part of this issue (i.e., HA-mediated local functional changes), a longitudinal magnetic resonance imaging (MRI) study has recently examined HL patients undergoing HA-based auditory rehabilitation (Pereira-Jorge et al., 2018). In this work, locally increased blood oxygen level-dependent (BOLD) functional MRI (fMRI) responses to naturalistic acoustic stimuli (alternating blocks of narrative listening and silence) were observed within auditory, language, and multisensory integration regions after 1 year of HA usage. However, this study did not investigate the long-range auditory functional connectivity (FC), that is, the functional coupling between primary auditory regions and anatomically distant brain areas throughout the whole brain.
Local functional alterations in the primary auditory cortex have been recently shown in cognitively intact HL patients (Ponticorvo et al., 2019). More specifically, using three-dimensional pseudocontinuous arterial spin labeling (3D-PCASL) MRI, a compact region in the right Heschl's gyrus (HG) was highlighted, where HL patients exhibited reduced absolute levels of cerebral blood flow (CBF) in comparison with age- and sex-matched normal hearing (NH) healthy controls. As these effects were largely confined to the primary auditory cortex, we hypothesized that a possible brain involvement in the pathophysiology of HL, as well as subsequent HA-mediated adaptive changes, at the larger scale of whole-brain functional networks might eventually originate from, or at least be closely linked to, this local perfusion deficit at the cortical entry point of auditory signals.
To test this hypothesis, we acquired both 3D-PCASL and BOLD resting-state fMRI (rs-fMRI) data from a larger sample of 62 HL patients across 2 successive time points (at baseline and after 6 months). During the follow-up period, about half of the HL patients used an HA device during normal daily life activities. We anticipated that (i) long-range, whole-brain FC changes from a seed region of reduced perfusion in the primary auditory cortex could be associated with the general HL condition and/or its HA-mediated peripheral correction and (ii) altered brain FC could be related to audiological and neurological features of patients and eventually to speech recognition and cognitive abilities.
Materials and Methods
Subjects
Eighty-seven HL patients (29 females) aged 64.4 ± 7.7 years (mean ± standard deviation) were consecutively enrolled for the study. All patients had a recent clinical diagnosis of HL (less than a month) and all of them were complaining about hearing problems for a few months or less. None of them used HAs before taking part in the study. Before MRI, all patients underwent audiological and neurological assessments (for details, see Audiological Assessment and Neuropsychological Assessment sections).
After completion of the first (baseline, t0) audiological assessment, upon HL diagnosis confirmation, the otorhinolaryngologist suggested that each patient consider the use of an HA device, although the patient was left free to decide about whether to use it or not, which center to refer to, and which type or model to take. Thirty-nine HL patients initially accepted to wear the HA device. During the first weeks after enrollment, these patients had several meetings with an audioprosthetist to adapt the device to their specific needs. These patients were instructed to wear the HA daily during normal activities (e.g., work-related activities, free time, and social activities). Among nonusers, commonly reported reasons supporting their choice included not only personal, social, and economic issues but also some prejudiced disappointment in HA effectiveness, which probably masked little perceived need of, or fear of social stigma associated with, this type of prosthetics. After completion of the first neurological assessment, four patients were excluded due to neurological issues (two patients were excluded for head trauma, one patient reported symptoms of epilepsy, and one patient was excluded because of right maxillary malignant neoplasm).
At follow-up (t1), 21 patients did not return to the planned visit and were therefore excluded from the study. In total, 62 HL patients (22 females) aged 64.4 ± 7.6 years completed the study with a second audiological and neurological assessment and a second MRI examination. Within the final sample, a subgroup of 31 HL patients (aged 63.4 ± 7.5 years) had been effectively using an HA device daily (mean HA usage 9.5 ± 3.8 h/day, range 1–17 h/day) (yHA group), whereas the remaining 31 patients (aged 65.3 ± 7.7 years) did not use the device (nHA group). Both patient subgroups came to the follow-up visit (t1) after a period of ∼6 months (198 ± 24.3 days). Patient characteristics (age, sex, and educational level) were statistically compared between the two groups (yHA vs. nHA) with the two-sample t-test (age and education) and chi-square test (sex). Neuropsychological (33 independent scores in total) and audiological (4 independent scores in total) clinical scores were compared at each time point (two-sample t-test) and longitudinally (t0 vs. t1, paired t-test).
Thirty-two NH controls (22 females) aged 59.3 ± 7.3 years with no medical history of HL (or complaint about their hearing) were included in the study.
None of the subjects enrolled had any history of neurological and/or psychiatric disorders, surgical interventions in the ear, or MR-specific contraindications. HL patients (20/62) and NH controls (29/32) had been also included in the sample of our previous metabolic study (Ponticorvo et al., 2019).
The study was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans, and the local ethics committee approved the study. Written informed consent was signed by each participant before MRI acquisition.
Audiological assessment
In both visits, HL was evaluated with pure-tone audiometry and speech audiometry. All the audiometric measurements (tonal/speech) presented here were performed in unaided conditions, that is, without HAs. The audiometric thresholds for air conduction in pure-tone audiometry were obtained at frequencies of 0.25, 0.5, 1, 2, 4, and 8 kHz in a soundproof chamber with headphones using a clinical audiometer. The pure-tone average (PTA) was calculated, as recommended by the Bureau Internacional d'Audiophonologie, as average loss at 0.5, 1, 2, and 4 kHz. Patients' ability to recognize speech sounds was evaluated in 57/62 HL patients and the speech reception threshold (SRT) for disyllables was calculated. Speech audiometry was performed in a soundproof chamber with the patient wearing headphones to receive the stimuli. The standard routine entails the examinator delivering blocks of 10 disyllabic words that the patient needs to repeat aloud. The intensity level is increased across blocks with increments of 10 dB from 10 to 100 dB, and the number of correct words at each intensity level is recorded. The SRT is determined as the level at which the patient is able to correctly repeat at least 50% of the words delivered (Bronkhorst and Plomp, 1989).
Neuropsychological assessment
All subjects underwent the Montreal Cognitive Assessment (MOCA) (Nasreddine et al., 2005) for screening of cognitive performances. HL patients (56/62) also performed a more accurate neuropsychological battery, including the attentional matrices and the Trail Making Test to investigate the attentional domain; Rey's auditory 15-word learning test to assess verbal memory (immediate recall and delayed recall; 15-RAWLT); the Stroop Color and Word Test; the Rey–Osterrieth Complex Figure Test memory (ROCF memory) to investigate visuospatial memory; the ROCF copy, Raven's Progressive Matrices (RPM), and the Clock Drawing Test to test frontal/executive functions; and the Short Form 36 (SF-36), Hearing Handicap Inventory (HHI), Beck Depression Inventory-II (BDI II), and Dimensional Apathy Scale (DAS) to assess the quality of life and levels of depression and apathy.
Image acquisition and preprocessing
Brain MRI was performed with a 3T scanner (MAGNETOM Skyra; Siemens Healthcare, Erlangen, Germany) equipped with a 20-channel radiofrequency head and neck coil.
The imaging protocol included a 3D T1-weighted anatomical sequence, a 3D-PCASL sequence (Dai et al., 2008, 2012; Detre et al., 2012; Wu et al., 2007), and a resting-state BOLD (T2*-weighted) multiband accelerated echo-planar (MB-EPI) fMRI sequence (rs-fMRI) (Feinberg et al., 2010; Moeller et al., 2010; Xu et al., 2013). During the 3D-PCASL and MB-EPI series, subjects were instructed to stay still with eyes open. The detailed imaging protocol and data preprocessing are provided in Supplementary Data Sections S1.1, S1.2, and S1.3.
CBF image analysis
CBF analysis was conducted at the regional level according to previous results (Ponticorvo et al., 2019) of local hypoperfusion in the right lateral HG. Mean CBF values in right HG were extracted at t0 for HL and NH subjects and corrected (with linear regression) for age, sex, and global CBF calculated as the mean value across all voxels in the brain (gray and white matter). Experimental groups were compared using a one-way analysis of variance (ANOVA).
For the longitudinal analysis, regional CBF values were extracted in the HL group at t0 and t1; corrected for age, sex, and global CBF; and then statistically compared in a two-way ANOVA with one within-subject factor (t1 vs. t0) and one between-subject factor (yHA vs. nHA).
Rs-fMRI data analyses
The ROI in the right HG was used to analyze whole-brain FC in a seed-based voxel-wise analysis. The Pearson r coefficient of correlation was calculated between the mean time series in the seed region and each voxel time course in the brain at t0 for HL and NH subjects and, for the follow-up analysis, at t0 and t1 for both yHA and nHA subjects. The r values were transformed to z scores by Fisher's r-to-z transformation (Fisher, 1915).
At baseline, FC z-maps were compared between HL and NH subjects in a one-way analysis of covariance (ANCOVA), as implemented in BrainVoyager (Brain Innovation, Maastricht, The Netherlands). Group membership (HL and NH) was specified as a between-subject factor and age as a continuous covariate. In the follow-up analysis, FC z-maps of HL subjects were compared in a two-way ANCOVA, with group membership (yHA and nHA) as the between-subject factor, time (t0 and t1) as the within-subject factor, and age as a continuous covariate.
To protect against false positives and correct for multiple comparisons, only statistically significant regional effects were displayed for compact clusters surviving the joint application of a voxel- and a cluster-level threshold to the ANCOVA t/F statistics maps. These were chosen using a nonparametric randomization approach based on Monte Carlo simulations (Forman et al., 1995), as implemented in BrainVoyager (Goebel et al., 2006). Namely, an uncorrected threshold (p < 0.001) was applied to all voxels (Eklund et al., 2016), then the minimum cluster size was set in such a way that an average of 5% false positive clusters were counted in 10,000 randomly generated images with smoothness matching the original maps (Forman et al., 1995).
Pearson correlation coefficients were also calculated to relate the observed neural effects (regional CBF and FC) to audiological characteristics. Spearman's rank correlation coefficients (ρ) were calculated between the variation in regional FC z-scores between time points and the corresponding variation in neuropsychological scores, separately for yHA and nHA subgroups. For these analyses, statistical significance (p-values) was reported without and with Bonferroni correction (for all correlation tests performed).
Results
Clinical and CBF evaluation
Audiological and neuropsychological characteristics of HL patients in the two subgroups at the two time points are summarized in Table 1 and Figure 1. There were no significant differences in sex, age, education, PTA, and SRT between yHA and nHA subgroups (p > 0.05) in both visits, and no audiological changes were detected over time in each group between the two time points (p > 0.05).
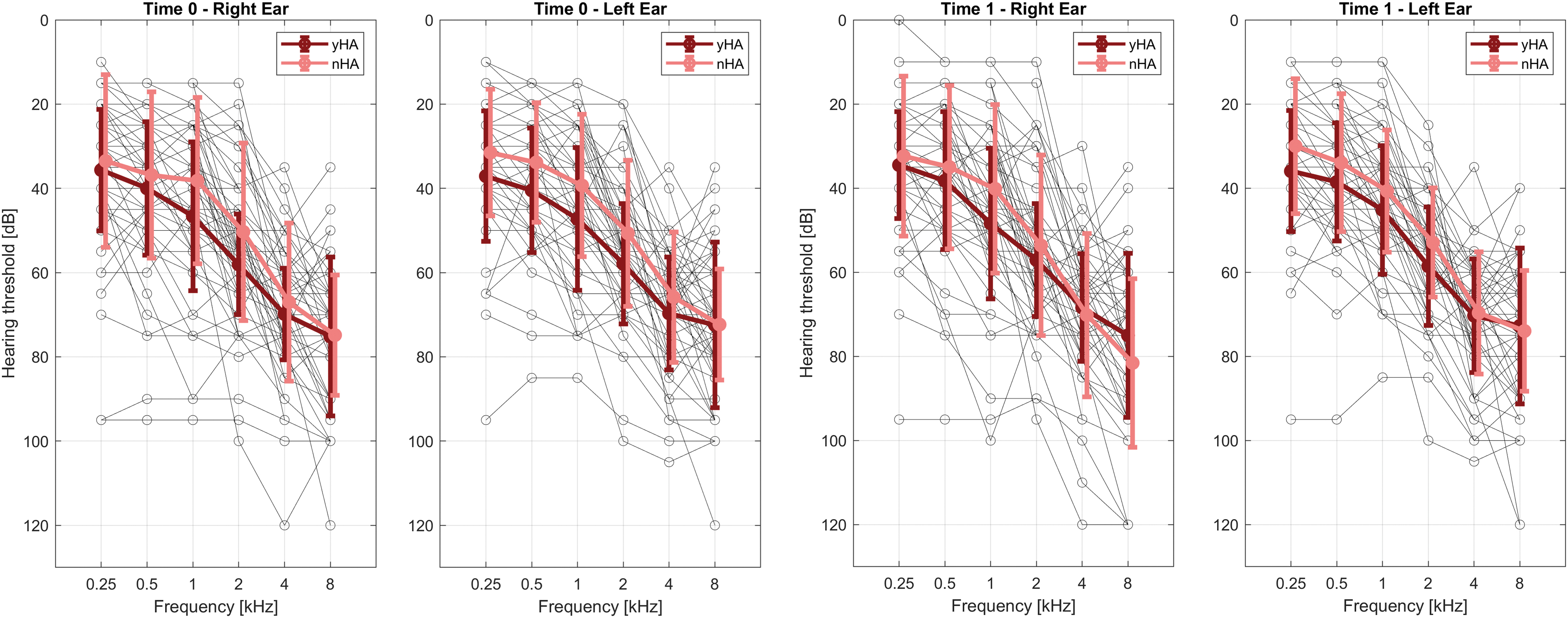
HL characterization of each patient (black line) in right and left ears, respectively, at the baseline visit (t0) and at the follow-up visit (t1). Overlayed in bold are the mean lines and standard deviation bars of the hearing loss of the yHA group (dark red line) and nHA group (pink line) at each visit (t0 and t1). To avoid bars, overlapping pink lines were shifted by 0.1 on the x-axis. nHA, patients not using hearing aids; yHA, hearing aid users. HL, hearing loss. Color images are available online.
Clinical and Neuropsychological Characteristics of Hearing Loss Groups
Audiological and neuropsychological characteristics of each of the two HL subgroups (yHA and nHA) at baseline (t0) and at 6-month follow-up (t1).
15-RAWLT, Rey's auditory 15-word learning test; ATT, attentional matrices; BDI II, Beck Depression Inventory-II; CDT, Clock Drawing Test; DAS, Dimensional Apathy Scale; HHI, Hearing Handicap Inventory; HL, hearing loss; MOCA, Montreal Cognitive Assessment; NA, not available; nHA, patients not using a hearing aid; PTA, pure-tone average on four frequencies (0.5, 1, 2, and 4 kHz); ROCF, Rey–Osterrieth Complex Figure Test; RPM, Raven's Progressive Matrices Test; SD, standard deviation; SCWT, Stroop Color and Word Test; SF-36, Short Form 36; SRT, speech reception threshold; TMT, Trail Making Test; yHA, hearing aid users.
All patients were cognitively intact (total MOCA score ≥15.5, according to the normative data of the Italian version of the MOCA) (Santangelo et al., 2015) and no significant differences were detected in total MOCA score (after correction for age and education) between yHA and nHA (p > 0.05) groups in both visits or in each group between time points (p > 0.05). No significant differences were detected between yHA and nHA groups both at t0 and t1 (p > 0.05) in any neuropsychological test. Significant differences between time points (t0 vs. t1) were detected, with an increase for the nHA group in 15-RAWLT immediate recall (p = 0.018) and RPM (p = 0.0013) test scores, an increase for the yHA group in 15-RAWLT delayed recall (p = 0.0087) and SF-36 subscore of physical pain (p = 0.017), and a decrease for the yHA group in HHI (p = 0.035). However, none of these differences remained significant after Bonferroni correction for all 66 comparisons (Supplementary Table S1).
The results of the CBF analysis are shown in Supplementary Figure S1. At baseline (t0), the mean regional CBF level in the right HG was significantly reduced in HL patients, compared with NH controls, after correction for age, sex, and global mean CBF level (t-value = −2.64, df = 92, p = 0.009). The mean ± standard deviation CBF levels as well as variations between time points (t1 − t0) in the right HG are reported in Table 2, respectively, for HL and NH groups. The regional follow-up CBF analysis in the right HG did not reveal any significant differences between time points (t1 vs. t0, yHA: t = 1.26, df = 30; nHA: t = −0.44, df = 30; p > 0.05) and between subgroups (yHA vs. nHA, t0: t = −0.23, df = 60; t1: t = −0.43, df = 60; p > 0.05).
Regional Cerebral Blood Flow Values
First two rows show absolute mean ± SD CBF levels (mL/100 g/min) in the seed region in right Heschl's gyrus for the three groups and the two time points. The third row shows the mean ± SD CBF variation over time (t1 − t0) for the two HL subgroups.
CBF, cerebral blood flow; NH, normal hearing.
Seed-based FC
Before FC group analysis, 10 HL patients and 2 NH subjects were excluded due to either excessive rigid head motion (2 HL subjects) or excessive local motion (8 HL and 2 NH subjects) in at least 1 session, therefore whole-brain FC group analyses were performed on 52 HL (25 yHA and 27 nHA) patients and 30 NH subjects.
At baseline, the whole-brain ANCOVA of FC z-maps (with seed region in the right HG) revealed a significant negative connectivity (anticorrelation) in HL patients, compared with NH controls (see Table 3 for details), with peaks in the right precuneus and right cerebellum crus I (Fig. 2). Within the whole HL group, the mean regional FC in the precuneus was found to negatively correlate with the mean PTA (Pearson r = −0.28, p = 0.04) and the mean SRT (Pearson r = −0.32, p = 0.027) from the right ear (Supplementary Fig. S2). In addition, the right HG-precuneus FC was negatively correlated with the BDI II score (Spearman ρ = −0.33, p = 0.032) and with the performance at the executive subtest of the DAS (Spearman ρ = −0.31, p = 0.049), although none of these correlations remained significant after correction for multiple comparisons.
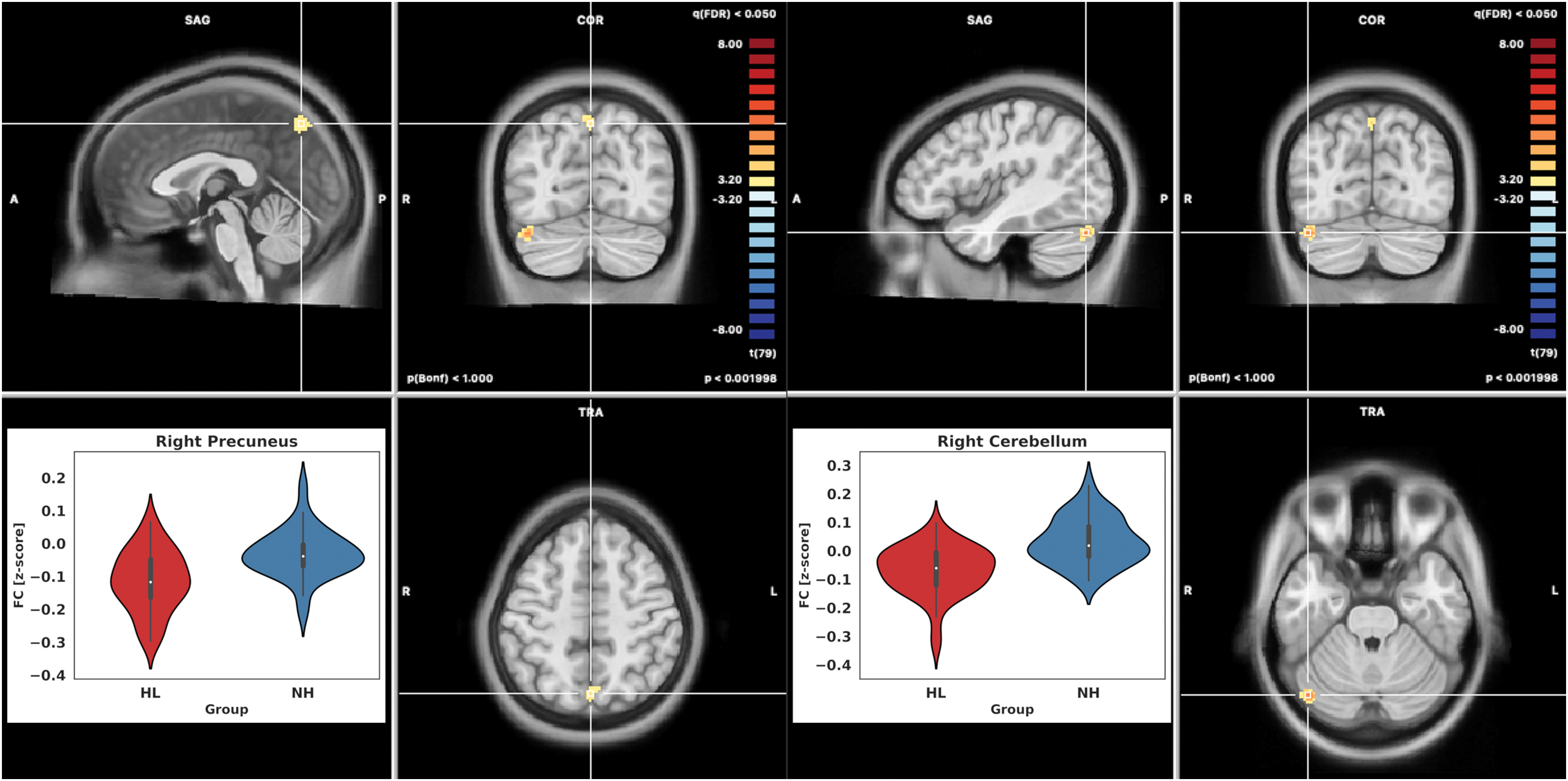
T-maps of the statistical comparison at baseline between HL and NH and violin plots with median (white circle) and relative frequency distribution of the functional connectivity in the two detected clusters for the two groups (HL, red; NH, blue). NH, normal hearing. Color images are available online.
Results of the Functional Connectivity Analysis
Results of the functional connectivity analysis. First column: peak location region label; second column: spatial coordinate (TAL) of the peak location; third column: p-value of the statistical comparison, respectively, between groups (HL vs. NH) for the baseline analysis and in the interaction group (yHA vs. nHA) by time (t0 vs. t1) for the follow-up analysis; and fourth column: details of the statistics in the peak with, respectively, the t-value and degree of freedom in the baseline analysis and the F-value and degree of freedom in the follow-up analysis for the interaction contrast.
df, degree of freedom.
At follow-up, the FC analysis revealed two clusters with significant time by HA use interaction effects (Fig. 3). These were located in the right superior frontal gyrus (SFG) and in the right middle temporal gyrus (MTG) (cluster-level corrected, minimum cluster size 96 mm3, see Table 3 for details).
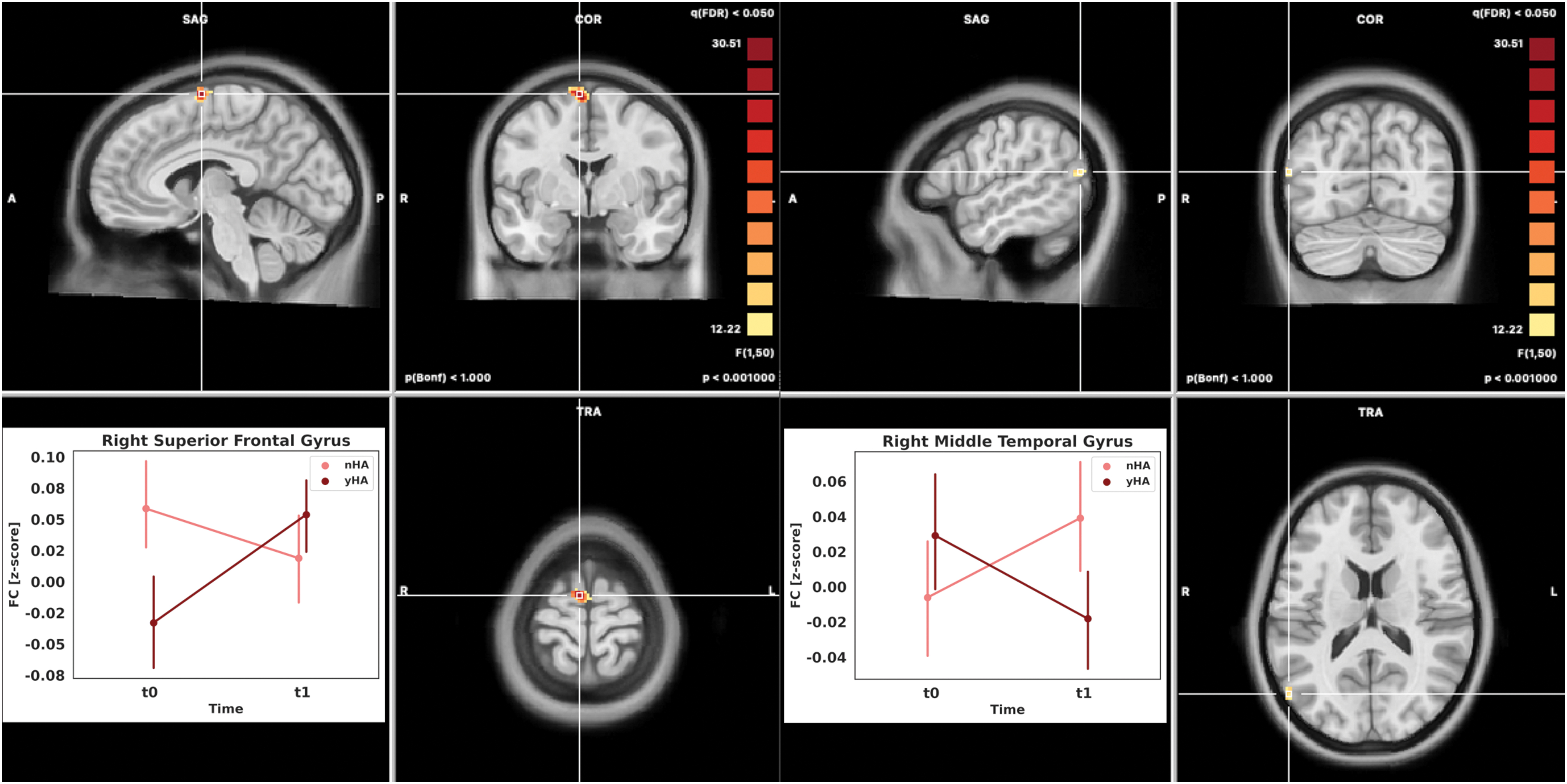
F-maps of the interaction contrast (time by HA) in the longitudinal two-way ANOVA, p < 0.05 after correction for multiple comparisons (cluster-forming threshold p < 0.001). Left panel: mean connectivity values (and confidence intervals at 95% of the value distribution bars) for the two groups (yHA, dark red line; and nHA, pink line) in the clusters of significant interaction at the two time points. ANOVA, analysis of variance. Color images are available online.
In the right SFG cluster, a significant positive difference in the regional FC z-score between t0 and t1 was observed in the comparison between yHA and nHA groups. This was due to a statistically significant increase in the yHA group (one-sample t-test on delta values, t1 − t0, p < 0.001) and a statistically significant decrease in the nHA group (one-sample t-test on delta values, t1 − t0, p < 0.001). For the yHA group, but not for the nHA group, a significant positive correlation was observed between the variation in the regional FC score (between time points) and variation in the MOCA score for the executive domain (Spearman ρ = 0.72, p = 0.00012, corrected for multiple comparisons on all 66 performed tests) (Supplementary Fig. S3).
A similar regional effect was observed, although with opposite polarity, in the right MTG. For this region, none of the correlation tests with audiological characteristics and neuropsychological performances were statistically significant for any of the two HL subgroups.
All r and ρ values (with corresponding p-values) from all the performed correlation analyses are reported in Supplementary Table S2. For both SFG and MFG, no significant correlations were found between the regional FC z-scores and the mean HA usage (h/day).
Discussion
This study builds on previous ASL-MRI findings showing that in the absence of cognitive impairment, HL is associated with neural tissue hypoperfusion (i.e., reduced CBF) within the primary auditory cortex (Ponticorvo et al., 2019). By seeding whole-brain FC analyses in the (hypoperfused and therefore potentially damaged) cortical entry point of the auditory system, in this study, we aimed at (i) exploring long-range auditory FC changes associated with HL and its peripheral correction through the usage of an HA device and (ii) relating such possible neural effects to audiological deficits and neuropsychological performances.
Regional CBF analysis
First of all, the CBF analysis at baseline (t0), extended to an enlarged sample of HL patients, confirms the previous observation of reduced neuronal metabolism in the right HG. Moreover, as no longitudinal CBF changes (t0 vs. t1) were found to be significant in the right HG, we also added that for at least 6 months, HL-related hypoperfusion in the right HG was neither reversed nor worsened regardless of hearing rehabilitation by means of HAs. This was in line with the audiological condition of HL patients as neither the PTA nor SRT significantly changed between time points in both yHA and nHA patients.
According to normative data (Clement et al., 2018), mean CBF levels across the whole gray matter are expected to decrease by normal aging at the rate of 0.31 mL/100 g/min per year. With this premise, we already expected that the pure age-related decrease in CBF levels would be negligible during the 6-month follow-up period at least when compared with any clinically meaningful physio-pathological effects. On the other hand, two previous studies reported an SRT improvement in HL patients using an HA device, respectively, after 12 and 18 months (Pereira-Jorge et al., 2018; Sarant et al., 2020). Thus, although none of these studies included a control cohort (i.e., HL patients not using an HA device) or CBF measurements, we cannot exclude that the 6-month follow-up period might have been just too short to disclose any significant changes in clinical conditions as well as in the local perfusion of the primary auditory cortex of HL patients. Notwithstanding these findings, it remains plausible that the plain, sensory input amplification provided by an HA device is simply not able to reverse the central metabolic damage, and future studies are needed to possibly address this aspect as well as the lack of systematic behavioral changes associated with the experience of HA fitting.
Seed-based FC analysis (baseline)
The seed-based whole-brain FC analysis at baseline (t0) revealed two regions with significantly negative (i.e., anticorrelation) effects in the comparison between HL and NH groups, which were located in the precuneus and in the cerebellum.
It is well established that the active human brain is intrinsically organized into task-positive and task-negative functional networks (Smith et al., 2009) and that in the resting state, signal fluctuations in task-positive regions are dynamically anticorrelated with signal fluctuations in task-negative regions (Fox et al., 2005). Particularly, signal changes within a sensory network are found to be anticorrelated with signal changes within a cognitive network (Zhu et al., 2016), reflecting the (average) amount of mutual inhibitory synchronization between remotely communicating neural populations (Deco et al., 2011).
Among task-negative regions, the precuneus is often targeted as the central hub of the default mode network (DMN) (Raichle et al., 2001). The DMN plays a pivotal role in the neural control of intrinsic cognitive processes, such as consciousness, autobiographical memory, and internal (self-directed) attention [see, e.g., Mak et al. (2017) for review]. Thus, the emerging anticorrelation between the right HG and precuneus may indicate that the chronic state of reduced cortical input from the auditory pathway, as induced by the HL condition, abnormally increases the level of mutual inhibitory influence between the auditory and DMN system, specifically through the (hypoactive) right HG. In this way, the intrinsic neural processes handled by the DMN would be directly impacted by the loss of sensory information along the auditory pathway.
An impact of the HL condition on the DMN has been already highlighted in previous works (Schmidt et al., 2013; Wang et al., 2014; Zhang et al., 2015), and an altered FC in the precuneus has been previously shown, either as a within-network effect, that is, secondary to disruption of the whole DMN (Chen et al., 2018; Husain et al., 2014; Schmidt et al., 2013), or as a between-network effect, that is, secondary to disruption of the coupling between the DMN and the dorsal attention network (DAN) (Rosemann and Thiel, 2019). Particularly, the latter study reported a significant correlation between DMN-DAN FC and listening effort in a sample of 19 HL patients. However, no previous FC study highlighted a direct neural link between the auditory function and (any nodes of) the DMN, in association with the HL condition. Therefore, seeding whole-brain FC analyses from such a specific region in the primary auditory cortex (possibly damaged according to the CBF analysis) might have been crucial to more directly probing into the long-range communication mechanism by which HL affects the brain. Indeed, this neural effect was found to significantly correlate with the audiological deficit, both at the pure-tone level (PTA) and at the speech reception level (SRT), implying that the more severe the clinical HL condition is, the more (aberrant) negative the coupling that occurs between the early auditory cortex and the DMN.
Although only explorative, we also observed that this negative FC effect was correlated with two neuropsychological measures: BDI II and DAS-es. These measures, respectively, reflect mood depression and apathy and may therefore indicate a modified mental state (Beck et al., 1961). Particularly, the DAS-es measure is associated with impaired planning, attention, or organization (Radakovic and Abrahams, 2014). Thus, the lack of complete information from the auditory environment, by chronically inducing an aberrant coupling between the primary auditory cortex and the DMN, may eventually lead to increased risk of depression and cognitive impairment in HL patients, as already postulated in the current literature (Rutherford et al., 2018).
An altered FC at baseline (t0) was also unveiled between the right HG and the right posterolateral portion (crus I) of the cerebellum. This was not surprising as (i) previous task-based fMRI studies had already shown that functional activity in the right cerebellum (crus I/II) is normally elicited during phonological processing and language comprehension (King et al., 2019; Lesage et al., 2017) and (ii) Xu and colleagues (2019b) had pointed out the role of HL in disruption of auditory cerebellar–cerebral communication. Thus, our results would confirm not only the presence of long-range FC changes in auditory cerebellar–cerebral communication but also add that this alteration may be vehicled by a damaged cortical center.
Seed-based FC analysis (follow-up)
In the longitudinal FC analysis (t0 vs. t1), two compact clusters were detected, in which a time by HA use interaction was statistically significant in the HL cohort. More specifically, the FC of the right HG was found to be increased in the right SFG and decreased in the right MTG in the yHA (vs. nHA) group at 6-month follow-up.
In the context of large-scale (task-positive) functional networks, the SFG plays an essential role in combining information from external inputs with the (intermediate) product of cognitive operations, thus enabling the necessary neural control on cognitive processing (Kamigaki, 2019). In this way, the SFG contributes to a number of executive functions, including working memory (du Boisgueheneuc et al., 2006; Owen, 2000; Owen et al., 1998; Petrides, 2000), and modulates external attention (Fox et al., 2006). In chronic HL patients, Xu and colleagues (2019a) reported reduced FC in the SFG (at baseline), although from a seed located in the anterior insula. However, no previous studies observed longitudinal changes in the whole-brain FC of the primary auditory cortex, before versus after a period of HA usage. In this study, we show that (i) using a seed in the right HG, the FC is not significantly altered at baseline, but can be longitudinally increased, in the SFG, of HL patients; (ii) this neural effect only occurs in HL patients employing an HA device for 6 months; and (iii) this FC change positively correlates with an improvement in the executive function, as indexed by the MOCA item, which specifically evaluates this cognitive performance. Altogether, these findings may suggest that auditory input amplification could help HL patients to more efficiently allocate neural resources for cognitive tasks (Anderson, 2019) by upregulating long-range FC between the right HG and SFG.
It is noteworthy that a different coupling of the auditory cortex with SFG between yHA and nHA HL patients existed before the intervention. While no prior hypotheses were formulated for comparison of whole-brain FC patterns at baseline between yHA and nHA groups, and none of the investigated parameters (both clinical and neuropsychological) explain this difference, it is possible that such pre-existing difference might be due to an unmatching of the two subgroups in the absence of randomization and that this aspect might have weakened the observed neural and behavioral changes after HA fitting.
The observed increase in the HG-SFG FC of yHA HL patients was mirrored by a parallel increase in the HG-MTG FC of nHA HL patients. The MTG is located at the junction between the temporal and occipital cortex and can be activated during audio–visual integration tasks (Naumer et al., 2009), including language perception (Nakamura et al., 2005). Notably, the MTG is significantly activated in deaf individuals engaged in interpreting sign language (Trumpp and Kiefer, 2018). Therefore, our data might suggest that the use of HAs and the consequential improved sensory input may lead to a decreased need, for yHA compared with nHA patients, of extra audio–visual integration of the auditory input to improve understanding and communication.
Finally, none of these FC changes correlated with the mean daily HA usage (in hours), suggesting that other variables, including the acoustic characteristics of the living environment or the content of auditory stimulations (e.g., music, speech, and noise), might eventually contribute to the full experience (and therefore the overall effectiveness) of HA amplification.
Study limitations
Even though this was the first fMRI study reporting long-range auditory FC changes in an HL population undergoing a period of HA-mediated rehabilitation, there were two limitations to consider. First, the longitudinal part of the study did not include an NH control arm, therefore the follow-up analysis lacks an external normative control on age-related neural effects. However, according to literature, possible within-subject (healthy) aging neural effects would be likely negligible within a time window of 6 months. Second, HL patients were left free to use (or not) an HA device and not (randomly) assigned to the yHA or nHA subgroup. Moreover, yHA patients were referred to the HA center of their convenience and not to a unique center (nor was this choice oriented toward a specific HA type or model), therefore we cannot exclude that taken together these choices might have introduced a bias between the resulting subgroups. Nonetheless, we observed no significant differences in all clinical scores between yHA and nHA subgroups at baseline, indicating that this subdivision did not result in bias with respect to any of the monitored variables. Thus, although additional (unknown) factors, other than the experience of HA fitting, might have also changed differently between yHA and nHA groups, the HA experience was the only known factor in this longitudinal study.
Conclusions
In conclusion, this study highlighted an impact of the HL condition (and its subsequent HA-mediated rehabilitation) on long-range neural communication between the primary auditory cortex and higher-order brain regions, suggesting that the hypoperfused early auditory cortex could be a seed place where different (maladaptive or protective) neuroplastic changes in whole-brain FC originate. These FC effects highlighted a mechanism of long-range neural communication, which could eventually explain the audiological and neurological course of HL.
Footnotes
Authors' Contributions
F.E. and F.D.S. designed the study. S.P., R.M., and F.E. acquired the MRI data. S.P. and F.E. performed the data analysis. J.P. developed the 3D-PCASL MRI sequence prototype. A.C., S.C., and M.T. performed the neuropsychological evaluation of patients and controls. D.T., E.C., and A.S. enrolled the patients and healthy subjects for the study and performed the audiological evaluation of patients. S.P. and F.E. drafted the article. All authors contributed to the critical discussion of results and reviewed and approved the final manuscript.
Acknowledgments
The authors would like to thank Amplifon SpA for supporting this research. The authors would also like to thank Domenico Zacà from Siemens Healthcare for facilitating and supporting the use of the 3D-PCASL prototype sequence.
Data Sharing Statement
Individual deidentified participant imaging data in the NIfTI format are available on Open Science Framework at the link: osf.io/pf943.
Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975 and the applicable revisions at the time of the investigation. Informed consent was obtained from all patients for being included in the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.