
Abstract
Background:
Previous studies arguing that functional dysphagia could be explained by underlying neurobiological mechanisms are insufficient to explain brain regions that functionally interact in patients with functional dysphagia. Therefore, we investigated functional connectivity changes associated with functional dysphagia after applying facilitatory repetitive transcranial magnetic stimulation (rTMS) on the supplementary motor area (SMA).
Materials and Methods:
A patient with severe long-lasting functional dysphagia and 15 healthy controls participated in this study. A facilitatory 5 Hz rTMS protocol was applied to the patient's SMA. We performed functional magnetic resonance imaging (fMRI) using volitional swallowing tasks to investigate neural network changes before rTMS (pre-rTMS), immediately after rTMS, and 3 months later.
Results:
The pre-rTMS fMRI results of the patient showed extensive overactivation in the left-lateralized regions related to volitional swallowing compared with the healthy controls. Following rTMS, dysphagia symptoms partially improved. The patient showed positive connectivity with the bilateral cerebellum in the bilateral SMA seeds before rTMS treatment. Furthermore, left-lateralized overactivation was washed out immediately after completion of rTMS, and connectivity between the left SMA and left precentral gyrus recovered 3 months after rTMS treatment.
Conclusion:
Our findings confirm that functional dysphagia might be a neurobiological manifestation caused by maladaptive functional connectivity changes in brain structures related to swallowing. Furthermore, noninvasive brain modulation with rTMS over the SMA may facilitate functional connectivity changes between the cortical and subcortical regions. Accordingly, these changes will allow control of the movements related to swallowing and may lead to improved clinical symptoms.
Impact statement
In this study, the pre-repetitive transcranial magnetic stimulation (rTMS) functional magnetic resonance imaging results of the patient showed maladaptive brain activation and connectivity compared with those in healthy controls. Dysphagia symptoms partially improved after 5 Hz facilitatory rTMS on the supplementary motor area. Brain activation and functional connectivity changed immediately and 3 months after rTMS. Our findings confirm that functional dysphagia might be a neurobiological manifestation caused by maladaptive functional connectivity changes in brain structures related to swallowing. Furthermore, noninvasive brain modulation, such as rTMS, may facilitate functional connectivity changes between cortical and subcortical regions to control movements involved in swallowing disorders, and consequently, improve clinical symptoms.
Introduction
Functional dysphagia is a symptom of swallowing difficulty without organic diseases or structural damage to the brain. Most studies state that functional dysphagia is caused by psychological factors (Kim et al., 1996), and few studies have argued that functional dysphagia could be explained by abnormal sensorimotor processing involving peripheral or central neural pathways (Galmiche et al., 2006; Suntrup et al., 2014).
Many studies investigated brain regions related to swallowing such as the bilateral primary sensory and motor cortex (M1) (Hamdy et al., 1999a, 1999b; Kern et al., 2001; Martin et al., 2001; Fraser et al., 2002; Furlong et al., 2004; Harris et al., 2005; R. Martin et al., 2007; Sörös et al., 2009), and right inferior parietal lobule (IPL) and insula (Sörös et al., 2009) for reflexive swallowing, and the bilateral primary sensory and motor cortex, supplementary motor area (SMA), inferior frontal gyrus (IFG), and anterior cingulate cortex (ACC) (Kern et al., 2001; Martin et al., 2001, 2004, 2007; Suzuki et al., 2003; Sörös et al., 2009), basal ganglia (BG), thalamus, cerebellum (Suzuki et al., 2003), and parietal lobe (e.g., the cuneus and precuneus region) (Kern et al., 2001) for volitional swallowing. The bilateral SMA and precentral gyrus (PCG), in particular, are related to movement initiation and control in volitional swallowing (Sörös et al., 2009).
The SMA is a critical region related to the initiation of internally generated movements (Roland et al., 1980a, 1980b; Matsuzaka et al., 1992; Halsband et al., 1994). The SMA is structurally connected to the motor cortex, cingulate sulcus, and gyrus, including the cingulate motor area and ACC, which are related to cognitive control (Deecke and Kornhuber, 1978; Paus, 2001; Nachev et al., 2008). This is demonstrated by the slowly increasing negative potential in the SMA before movement onset. In addition, the readiness potential was greater when preceded by self-initiated movements compared with externally cued movements (Jahanshahi et al., 1995).
These findings indicate that the SMA plays a key role in voluntary actions, such as self-initiated movements, rather than in response to external events. Therefore, investigating the neural mechanisms of SMA is crucial to understand the therapeutic trigger for functional dysphagia.
Previous studies have reported that facilitatory conditioning of the SMA with 5 Hz repetitive transcranial magnetic stimulation (rTMS) increases the excitability of M1 (Matsunaga et al., 2005; Raux et al., 2010). Some studies have applied facilitatory rTMS treatment over the SMA of patients with neurological diseases such as Parkinson's disease (Koch et al., 2005; Brusa et al., 2006; Hamada et al., 2008; Grefkes et al., 2010; Shirota et al., 2013). However, no previous studies have investigated neural network changes after rTMS for functional dysphagia.
In this study, we investigated differences in brain activation between a patient with long-standing severe functional dysphagia and healthy controls during volitional swallowing. We applied facilitatory brain modulations using rTMS to the SMA to upregulate its initiating function. Furthermore, we investigated brain activation and connectivity changes during swallowing tasks using functional magnetic resonance imaging (fMRI) before rTMS (pre-rTMS), immediately after rTMS (post1-rTMS), and 3 months after rTMS (post2-rTMS) to examine the SMA and its connected regions of interest (ROIs) to key regions, associated with volitional swallowing such as subcortical regions (e.g., thalamus-BG) and the insula.
Materials and Methods
Case description
Patient S was a 42-year-old man who had persistent swallowing difficulty for more than 10 years. When the symptoms first developed, the patient visited the Department of Gastroenterology and Neurology, although no abnormality was found either through gastrofiberscopy or through brain magnetic resonance imaging (MRI). The patient was then transferred to the psychiatry department, diagnosed with a conversion disorder, and subsequently treated with clonazepam, baclofen, trihexyphenidyl, and aripiprazole. However, the symptoms did not improve.
The first neurological examination revealed normal motor and sensory functions in the limb and oro-bulbar areas and intact cranial nerves. However, when asked to drink a cup of water, he demonstrated hesitant hand movements while holding the cup and uncoordinated arm movements while moving it to his mouth. The initial video fluoroscopic swallowing study (VFSS) showed significant swallowing initiation and bolus transfer difficulties during the oral phase and prolonged pharyngeal delay time.
Experimental design
This study was conducted as single-case experimental design. We performed noninvasive brain modulation (NIBS) using a facilitatory rTMS protocol on the patient's SMA (Supplementary Fig. S1 and Supplementary Table S1). The patient underwent comprehensive dysphagia rehabilitation program immediately after completing the rTMS session for 30 min.
We investigated behavioral changes in the swallowing function and performed serial fMRIs (pre-rTMS, just after completing rTMS, and 3 months after rTMS) to determine different brain activation patterns and functional connectivity related to swallowing. The fMRI was only performed once before rTMS intervention, as did most single-subject fMRI studies in dementia (Dressel et al., 2010) or stroke (Hamilton and Martin, 2005; Rojo et al., 2011; Schuster-Amft et al., 2015; Radman et al., 2016). Fifteen neurologically healthy adults were enrolled as a control group (15 males; age range 19–45 years, mean [standard deviation] age = 33.53 [7.64]).
Informed consent was obtained from all participants. The study protocol was approved by the ethics committee of Korea University Anam Hospital (ED13158).
fMRI study
Volitional swallowing task
The patient and healthy controls performed a volitional saliva-swallowing task during the fMRI session (Fig. 1).
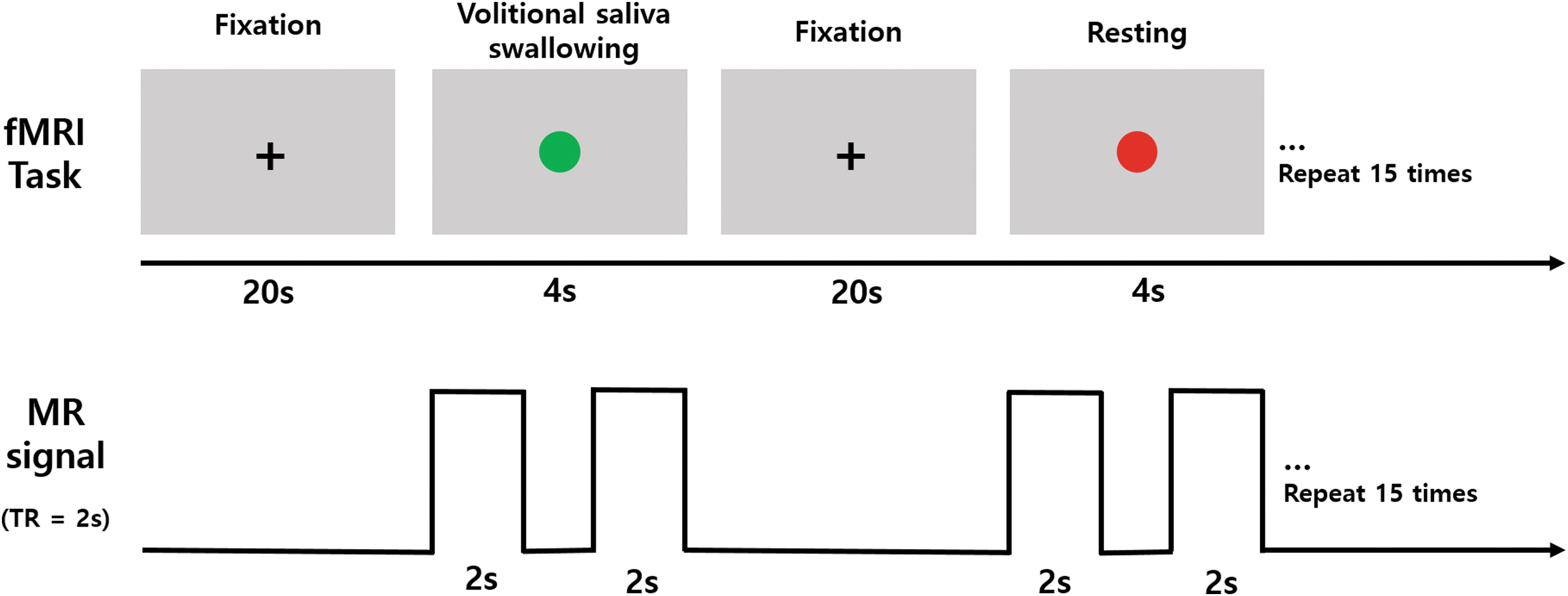
Volitional swallowing task. The swallowing task comprises two conditions: swallowing and non-swallowing. In every trial, a green dot or a red dot is shown for 4 sec. If the green dot is displayed, participants need to swallow their saliva once, although if the red dot is displayed, participants need to rest without any movement. A fixation cross “+” is first presented in every trial for 20 sec to remove the residual blood oxygen level-dependent signal due to swallowing. The swallowing trial and resting trial are repeated 15 times.
Image acquisition
Structural MRI of all participants was performed on a 3T Siemens Trio whole-body imaging system (Siemens Medical Systems, Erlangen, Germany) using T1-weighted sagittal high-resolution magnetization-prepared rapid gradient echo sequence with the following parameters: repetition time (TR) = 1,900 ms, echo time (TE) = 2.52 ms, flip angle (FA) = 9°, inversion time (TI) = 900 ms, voxel size = 1 × 1 × 1 mm. fMRI scans were acquired using an echo-planar imaging scan with the following parameters: 42 axial slices, voxel size = 3 × 3 × 3 mm, TR = 2,000 ms, TE = 20 ms, and FA = 90°.
fMRI data analysis
The pre-processing of the fMRI data included realignment, slice timing correction, co-registration to the structural scan, spatial normalization to the MNI space, and spatial smoothing (8 mm Gaussian kernel) using Statistical Parametric Mapping version 8 (SPM8; Wellcome Department of Neuroscience, London, UK) with default settings.
Individual contrast images were computed using a generalized linear model in SPM8. Individual T-contrast images were entered into a one-sample t-test for each experimental condition within the subject group, and two-sample t-tests with age as covariates between the subject groups, and between before and after rTMS conditions. A family-wise error (FWE) rate of 0.05 at the cluster level was used in both the one-sample t-test and two-sample t-test. The cluster size comprised more than 100 contiguous voxels. We performed small volume correction (SVC) with an FWE rate of 0.05, for the comparison between the single patient and healthy controls in predefined ROIs related to swallowing movements (see the Supplementary Data description for details).
Functional connectivity analysis
We created individual subject ROI-to-ROI connectivity maps using the CONN-fMRI Functional Connectivity toolbox version 13 to perform functional connectivity analysis. We used the predefined ROIs for volitional swallowing in SVC using anatomically defined masks from Wake Forest University PickAtlas (Maldjian et al., 2003) (Supplementary Table S3).
We performed “ROI-to-ROI” analysis in a statistical second-level analysis to create within-group functional connectivity maps (swallowing > non-swallowing) before completing the fixed-effect analysis with seed ROI as a “Seed-to-ROI” analysis. The threshold for each network had a corrected alpha level of 0.05, for multiple comparisons with false discovery rate (FDR). For each network, we presented threshold maps for positive connectivity in each group (see Supplementary Data description for details).
Results
Clinical symptom changes after rTMS
The patient reported subjective improvement in swallowing after completion of the rTMS protocol, and VFSS revealed a reduced pharyngeal transit time and decreased residue of the vallecular space and pyriform sinus. Three months after completion of rTMS, both the oral transit time and the pharyngeal transit time returned within the normal range (Supplementary Table S2).
Brain activation changes in fMRI
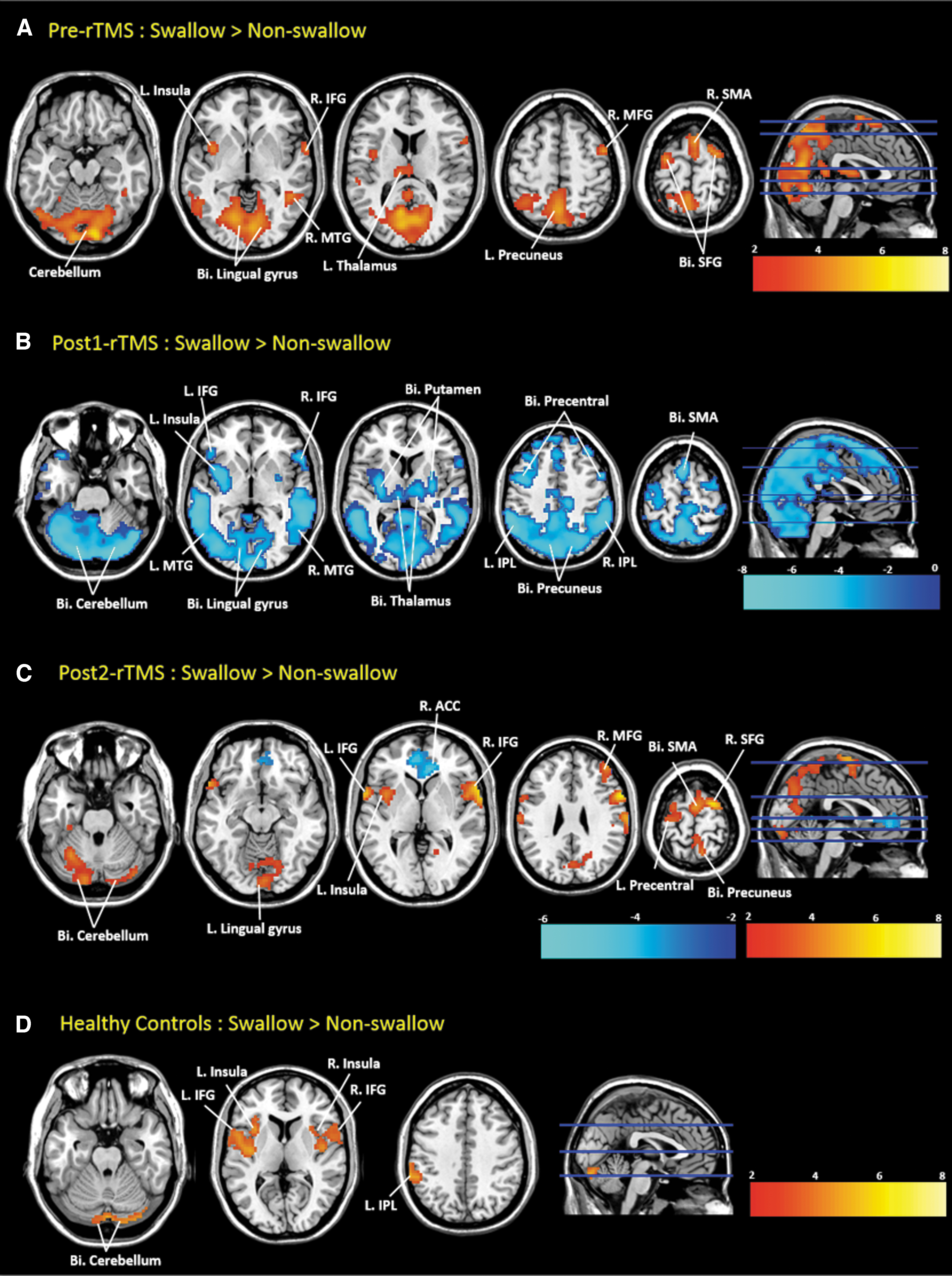
Healthy controls displayed neural activation in the insula, IFG, cerebellum on both sides, and IPL, supramarginal gyrus in the left hemisphere upon volitional swallowing (FWE-corrected p < 0.05, Table 1 and Fig. 2D). Neural activation in the patient's pre-rTMS fMRI was more extensive than that in healthy controls. However, neural activation in the patient changed to deactivation in post1-rTMS. In post2-rTMS, the patient showed neural activation in brain regions related to volitional swallowing, although there was also a neural deactivation in the right ACC while performing the swallowing task (FWE-corrected p < 0.05, Table 2 and Fig. 2C).
The fMRI results during volitional swallowing in a case with functional dysphagia and healthy controls.
Brain Regions Display Significant Activation in Healthy Controls During Voluntary Swallowing (Swallow > Non-Swallow: Family-Wise Error-Corrected p < 0.05, More Than 100 Voxel)
Brain regions contained within a single cluster are listed together. Regions containing peak voxels are printed in bold.
SMG, supramarginal gyrus.
Brain Regions Display Significant Activation or Deactivation in Patient S During Voluntary Swallowing (Swallow > Non-Swallow: Family-Wise Error-Corrected p < 0.05, More Than 100 Voxel)
Brain regions contained within a single cluster are listed. Regions containing peak voxels are printed in bold.
ACC, anterior cingulate cortex; IFG, inferior frontal gyrus; IPL, inferior parietal lobule; ITG, inferior temporal gyrus; MFG, middle frontal gyrus; MNI, montreal neurological institute; MTG, middle temporal gyrus; rTMS, repetitive transcranial magnetic stimulation; SFG, superior frontal gyrus; SMA, supplementary motor area; STG, superior temporal gyrus.
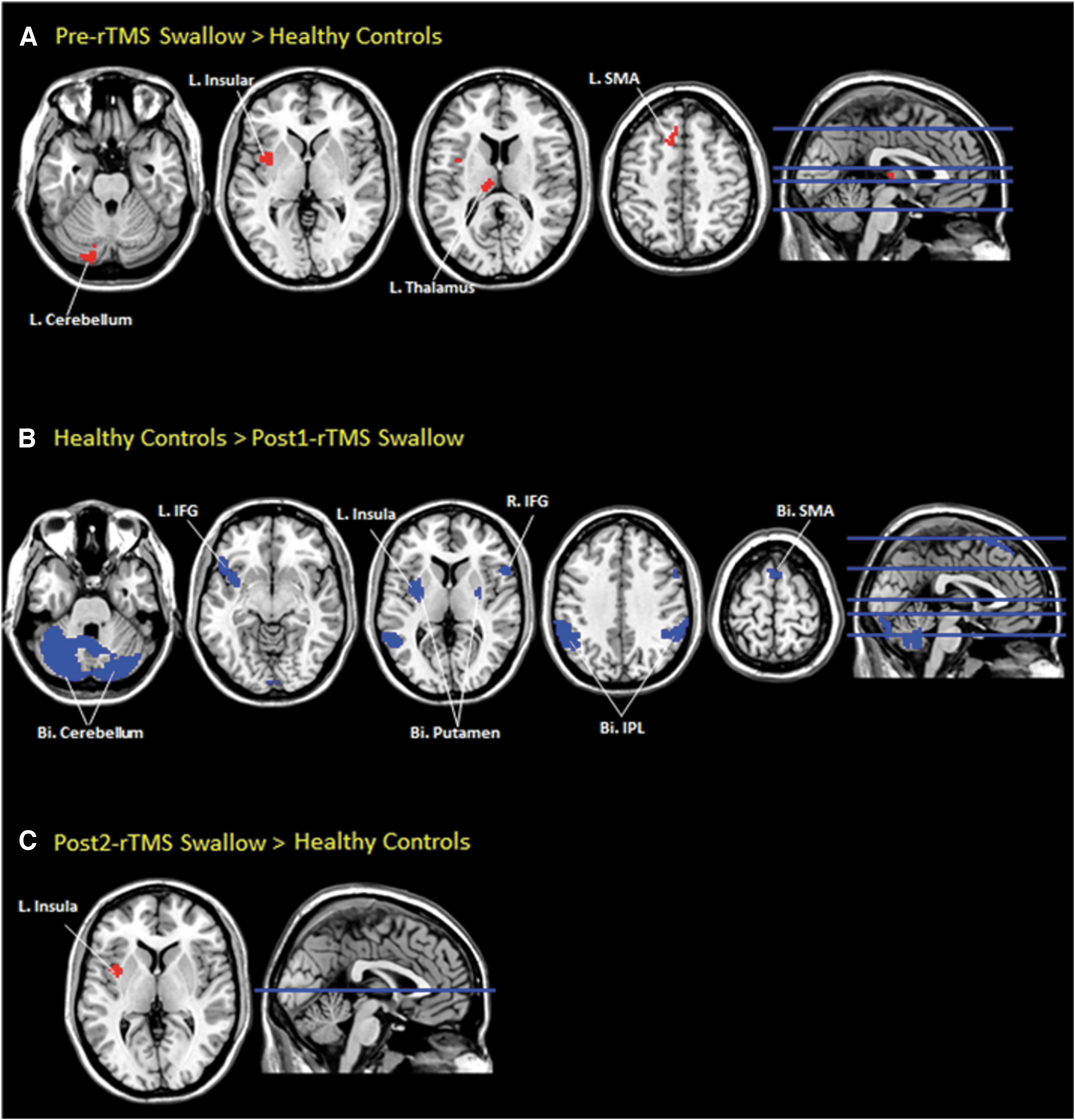
The patient's fMRI showed more neural activation at pre-rTMS in the bilateral lingual gyrus and cerebellum, and left SMA, IFG, and MTG than at post1-rTMS, and the patient at pre-rTMS showed more neural activation in the bilateral SFG, lingual gyrus, left thalamus, right ACC, fusiform gyrus, and putamen than at post2-rTMS. At post2-rTMS, the patient showed more activation in the bilateral cerebellum than at post1-rTMS (FWE-corrected p < 0.05, Table 3 and Fig. 3). The overactivation in the patient remained in the left insula alone 3 months after rTMS compared with that in healthy controls (SVC FWE-corrected p < 0.05, Table 3 and Fig. 4).

Comparison of fMRI findings in a patient with functional dysphagia.
Comparison of fMRI between the patient and healthy controls.
Brain Regions Display Significant Differences Between Pre- and Post-Repetitive Transcranial Magnetic Stimulation in Patient S, and Between Patient S and Healthy Controls During Swallowing (Swallow > Non-Swallow: Family-Wise Error-Corrected p < 0.05, More Than 100 Voxel)
Brain regions contained within a single cluster are listed. Regions containing peak voxels are printed in bold.
FFG, fusiform gyrus; HC, healthy controls.
Neural connectivity changes after rTMS
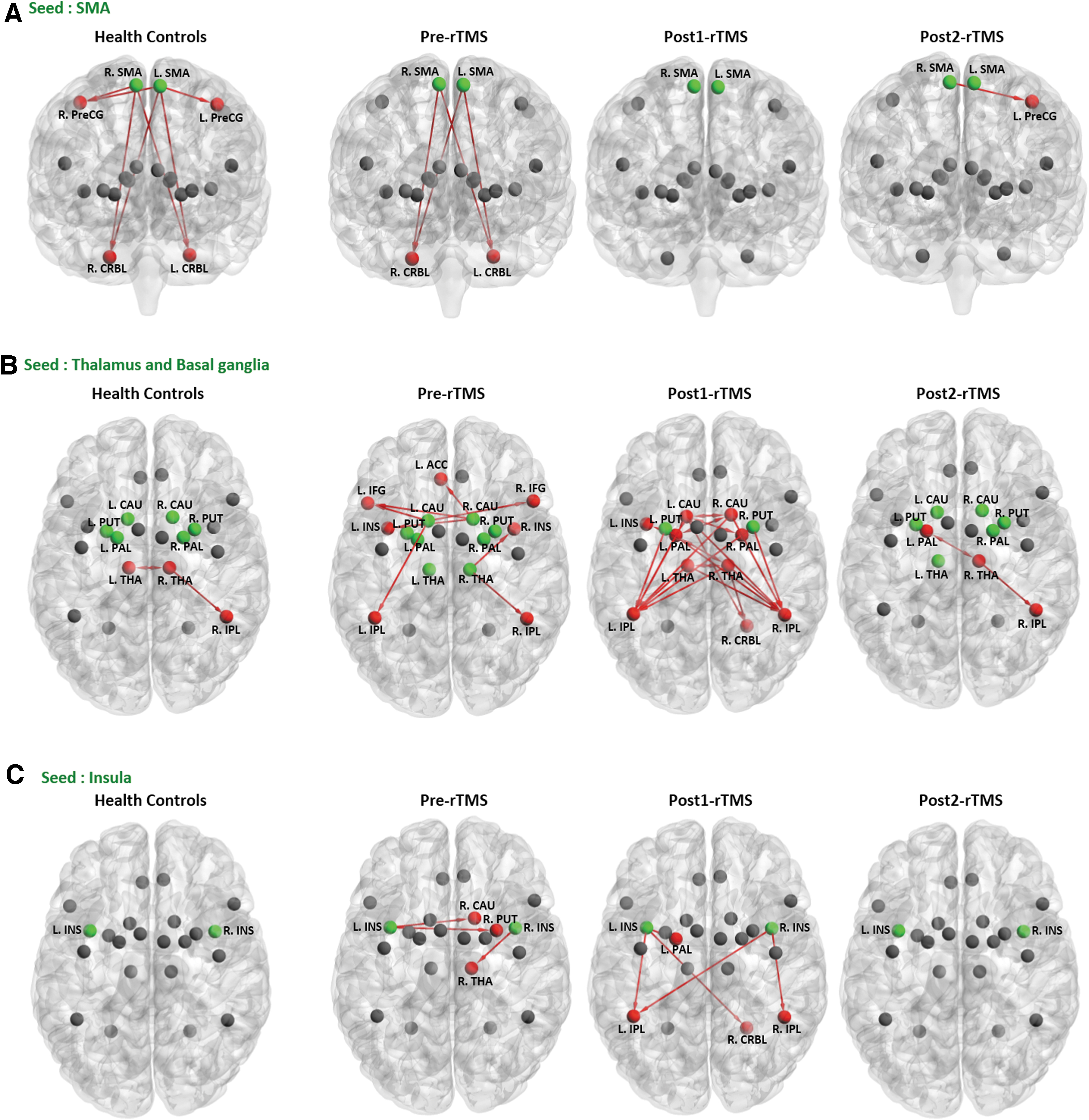
In the left SMA seed, healthy controls exhibited positive connectivity with the bilateral PCG and cerebellum; in the right SMA seed, healthy controls exhibited positive connectivity with the bilateral cerebellum and right PCG. However, the patient showed positive connectivity with the bilateral cerebellum in both SMA seeds before rTMS.
Immediately after the rTMS treatment, the patient did not show significant connectivity with ROIs in the bilateral SMA seeds; however, connectivity was recovered between the left SMA (seed area) and the left PCG (target area) in post2-rTMS. Significant positive connectivity with the ROIs in the bilateral BG seeds and bilateral thalamus was noted. The patient's neural connectivity with the insula seed differed in post2-rTMS, similar to the neural connectivity of healthy controls with insula seed (FDR-corrected p < 0.05, Table 4 and Fig. 5).
Connectivity analysis of the serial fMRI study in the patient and healthy controls using the different brain structures as seed areas (FDR-corrected p < 0.05).
Brain Regions Show Significant Connectivity Between Seed Areas and Region of Interests in Swallowing > Non-Swallowing Contrast (False Discovery Rate-Corrected p < 0.05)
Bilateral SMA, insula, BG (caudate, pallidum, putamen), and thalamus.
Bilateral precentral gyrus, SMA, IFG, insula, ACC, IPL, BG (caudate, pallidum, putamen), and cerebellum.
Among the brain regions, p < 0.05 is indicated in bold letters.
BG, basal ganglia.
Discussion
This study investigated the underlying neural mechanisms of functional dysphagia and whether NIBS could change behavioral symptoms and neural connectivity using fMRI. The pre-rTMS fMRI findings of the patient showed overactivation in the left-lateralized regions of the cerebellum, insula, SMA, and thalamus, suggesting maladaptive brain changes related to functional dysphagia. Applying rTMS on the SMA combined with behavioral intervention improved dysphagia symptoms, whereas brain activation and functional connectivity changed immediately in follow-up fMRI studies. These findings suggest that dysfunctional neural control, rather than a psychological problem, is the underlying pathomechanism of functional dysphagia and that NIBS may modulate and change brain connectivity in functional neurological disorders.
Volitional swallowing is reported to be mediated by two parallel loops: connections through the sensorimotor–cingulate module and connections through the cerebellum or insula (Mosier and Bereznaya, 2001). The IPL, known as a multimodal sensory association cortex, plays a role in controlling swallowing (Sirigu et al., 2004; Jaffard et al., 2008; Desmurget et al., 2009; Desmurget and Sirigu, 2012), as do the BG (Turner and Anderson, 2005; Turner and Desmurget, 2010).
In our results, before rTMS, the patient showed positive connectivity between the thalamus-BG circuit and widespread cortical regions such as the prefrontal, insula, and IPL. However, immediately after rTMS treatment, the widespread connectivity between the thalamus and BG converged on the bilateral IPL. Finally, after 3 months, the connectivity between the thalamus and BG in the patient resembled that in the healthy controls.
We could infer that the rTMS facilitated SMA-stimulated inhibition in the thalamus-BG circuit. Before rTMS treatment, the patient showed similar pattern of functional connectivity between the SMA and cerebellum, but no connectivity between the SMA and motor area. However, 3 months after rTMS treatment, all connectivity with the SMA disappeared, and only one positive connection between the SMA and left motor area appeared. These results implied that rTMS could produce more efficient paths to process swallowing by forming a new connection between the SMA and motor area, which was more beneficial 1–2 months after the intervention than immediately after (Yang et al., 2015).
The insula is an important brain structure for swallowing, and discrete lesions of the anterior insula cause disruption of the swallowing network and dysphagia (Daniels and Foundas, 1997). Given its role in the sequential aspects of control, the insula appeared to be related to synchronizing kinematic movement during swallowing (Mosier and Bereznaya, 2001).
In this study, 3 months after rTMS treatment, the deactivation pattern turned to overactivation compared with healthy controls, especially in the left insula. Our results suggest that the patient might need more resources from the insula compared with healthy controls to manage swallowing. Moreover, the patient's bilateral insula was connected with the thalamus-BG circuit before rTMS, but the connectivity with the insula disappeared 3 months after rTMS treatment, similar to the controls. This result indicated that the insula functions as an individual module to control swallowing (Mosier and Bereznaya, 2001), and the role of the insula was strengthened in the patient after rTMS.
The left hemisphere is known to be more specialized for movement organization and selection (Schluter et al., 1998; Rushworth et al., 2001; Serrien et al., 2006). In this study, the left-lateralized overactivation was washed out in fMRI of post1-rTMS, and the patient showed decreased neural activation in the bilateral SMA, IFG, IPL, putamen, cerebellum, and left insula compared with the healthy controls. Indeed, several studies have asserted that rTMS affects neural changes around the vicinity of the stimulated area, as well as in remote regions such as the subcortical areas (George et al., 1999; Bestmann et al., 2005; Gaudeau-Bosma et al., 2013).
Moreover, a study demonstrated that rTMS applied over the pre-SMA induced inhibitory control efficiency and increased regional cerebral blood flow in the prefrontal and parietal cortices (Obeso et al., 2013). This indicates that neural inhibition of the brain regions related to volitional swallowing was induced by 5 Hz facilitatory rTMS on the SMA.
This study has some limitations. First, patients with functional dysphagia who have persistent and severe symptoms are rare; thus, this study was conducted as a single-case follow-up study with control subjects. Therefore, to generalize our observations and hypotheses to other types of functional neurological disorders, more studies on different types of disorders are warranted. Second, we did not consider functional network metrics based on dynamic functional connectivity graphs, which were applied by a statistical and topological filtering scheme (Stavros et al., 2017; Antonakakis et al., 2020).
Conclusion
Our findings support that functional dysphagia might be a neurobiological manifestation caused by maladaptive changes in functional connectivity in swallowing-related brain structures. Furthermore, our results suggest that NIBS with rTMS over the SMA may facilitate functional connectivity changes between the cortical and subcortical regions. Accordingly, these changes will allow control of the movements associated with swallowing and may lead to improved clinical symptoms.
Footnotes
Authors' Contributions
S.-B.P. contributed to the original conceptualization and design of the rTMS protocol and diagnosed Patient S. S.C. contributed to the design of the fMRI protocol for volitional swallowing tasks, and the fMRI analysis and interpretation of research data. All the authors have written and reviewed the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Research Foundation of Korea (NRF) funded by the Korean government (no. 2019R1A2C2003020).
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.