
Abstract
Aim:
To evaluate the effects of a single session of non-invasive brain stimulation (NIBS) on postural balance.
Introduction:
The NIBS has been used widely in improving balance. However, the effect of a single session of NIBS on balance in healthy individuals has not been systemically reviewed.
Methods:
A systematic literature review and best evidence synthesis were conducted, according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines, to determine the effects of different NIBS techniques on balance function in healthy individuals. The methodological quality of included articles was assessed by the risk of bias, and the Downs and Black tool. Data were analyzed by using the best evidence synthesis. Thirty-five articles were included that used the following NIBS techniques: anodal transcranial direct current stimulation (a-tDCS), cathodal transcranial direct current stimulation (c-tDCS), continuous theta burst stimulation (cTBS), and repetitive transcranial magnetic stimulation (rTMS) on primary motor cortex (M1), supplementary motor area (SMA), dorsolateral prefrontal cortex (DLPFC), and cerebellum on balance.
Results:
Strong evidence showed that a-tDCS of M1, SMA improve balance in healthy participants, and the a-tDCS of DLPFC induces improvement only in dual task balance indices. Also, the findings indicate that cerebellar a-tDCS might significantly improve balance, if at least 10 min cerebellar a-tDCS with an intensity of ≥1 mA, over or maximum 1.5 cm below the inion, is used. Strong evidence showed that c-tDCS, cTBS, and rTMS are not effective on the balance.
Conclusion:
According to the results, the a-tDCS may be a useful technique to improve balance in healthy adults.
Impact statement
The strong evidence found in this review indicates that single-session, stand-alone application of anodal transcranial direct current stimulation on the cerebellum, primary motor cortex (M1), and supplementary motor area can improve balance in healthy individuals. Moreover, strong evidence suggests that cathodal transcranial direct current stimulation has an adverse effect on balance and must be avoided as a technique for the treatment of balance. These results can be used to improve balance in patients with neurological disorders, and healthy older adults with balance dysfunctions.
Introduction
Balance is defined as an ability to maintain the body's center of gravity within the base of support with minimal postural sway (Muir et al., 2008), and it is an essential element of locomotion and is crucial for a higher quality of life (Duarte and Freitas, 2010). Balance is an adaptive sensorimotor process relying on the integration of sensorimotor inputs and adjustments through the cerebellum and other parts of the central nervous system (CNS) (Craig and Doumas, 2017; Horak, 2006; Peterka, 2002). Correct postural balance is the result of co-activation of different parts of the CNS such as the cerebellum, primary motor cortex (M1), dorsolateral prefrontal cortex (DLPFC), and supplementary motor area (SMA).
Each brain area has a specific role in the processing of the sensorimotor inputs, assisting in integrating and assessing the incoming sensory signals to obtain the accurate perception of body orientation in space, and providing outputs to the musculoskeletal system to act in a way to maintain balance (Bolton et al., 2012; Calautti et al., 2010; Kaminski et al., 2016; Morris, 2000; Yosephi et al., 2018). The cerebellum contributes to sensorimotor inputs processing (Rossi et al., 2009; Woods et al., 2016), compares the intended motor function with its execution, and provides corrective signals to the cerebral cortex, and muscles in case of any mismatch (Colnaghi et al., 2011; D'Angelo and De Zeeuw, 2009; Manzoni, 2007; Zenzeri et al., 2011). On the other hand, the DLPFC has a significant role in executive control and planning of the body movements during a balance task (Mihara et al., 2008, 2012; Wittenberg et al., 2017). These movement plans are compared with the movement memories stored in SMA (Mihara et al., 2008, 2012; Wittenberg et al., 2017) (Fig. 1).

Simplified connections of different brain regions in balance and movement control.
All of these brain areas are working together to produce the correlated pattern of muscle activity during motor activities along a continuum of motor control by either feedforward or feedback mechanisms (Shumway-Cook and Woollacott, 2017). The feedback control mechanism is postural control that occurs in response to sensory feedback (visual, vestibular, or somatosensory) from an external perturbation. However, the feedforward mechanism refers to anticipatory postural adjustments that are made in anticipation of a voluntary movement that is potentially destabilizing to maintain stability during the movement (Shumway-Cook and Woollacott, 2017). It has been shown that the cerebellum (Baillieux et al., 2008; Bastian, 2006; Diedrichsen et al., 2005; Fautrelle et al., 2011; Johnson et al., 2019; Mizelle et al., 2016; Peterburs et al., 2018), DLPFC (Allaert et al., 2020; Ishii et al., 2018; Macuga and Frey, 2014), SMA (Ishii et al., 2018; Macuga and Frey, 2014), and M1 contribute to both of these mechanisms based on situational demands (Bolton et al., 2012; Kaminski et al., 2016; Nonnekes et al., 2014; Saruco et al., 2017), to optimize the information processing, make purposeful and flexible reactions, and maintain balance. Thus, it is difficult to separate the activity of each of these areas in these two mechanisms.
In addition, sensory information helps individuals to adjust the postural control responses. The main sensory information is obtained from the visual, somatosensory, and vestibular systems (Grace Gaerlan et al., 2012; Shumway-Cook and Woollacott, 2017). Information acquired via vision is responsible for the spatial orientation, head's position and movement in relation to the surrounding objects. Thus, changes in the visual feedback (eyes open [EO] or eyes closed [EC]) may provoke different postural control strategies (Grace Gaerlan et al., 2012; Shumway-Cook and Woollacott, 2017).
It has been shown that any deficiency in the activation of these brain sites can lead to postural instability, which is usually evaluated by the time a person can keep the balance, known as “time in balance” (TIB), or the magnitude of center-of-pressure (COP) displacement in both EO and EC states (Di Nuzzo et al., 2018; Kang et al., 2016; Lee and Lee, 2015; Ludemann-Podubecka et al., 2014; Morris, 2000; O'Brien et al., 2018; van Dun and Manto, 2018; Wessel and Hummel, 2018; Woods et al., 2016; Yitayeh and Teshome, 2016; Zandvliet et al., 2018). Loss of balance is one of the main symptoms in several CNS disorders such as Parkinson, ataxia, stroke, or brain degenerative disorders (Di Nuzzo et al., 2018; Kang et al., 2016; Lee and Lee, 2015; Ludemann-Podubecka et al., 2014; Morris, 2000; O'Brien et al., 2018; van Dun and Manto, 2018; Wessel and Hummel, 2018; Woods et al., 2016; Yitayeh and Teshome, 2016; Zandvliet et al., 2018). Balance impairment often leads to an increased risk of falls if it remains untreated (Hernandez et al., 2012a; Jia et al., 2019; Muir et al., 2010; Pua et al., 2017). It also limits patients' ability to indulge in activities of daily living (Duarte and Freitas, 2010). Thus, the treatment of any balance deficiency is of clinical importance.
Typically, exercise therapy in the form of balance training has been widely used to treat balance disorders (Lord et al., 2003; McKeon et al., 2008; Sherrington et al., 2017; Silva et al., 2013). Although the evidence supports the use of exercise training for the treatment of balance disorders, this approach is quite challenging as it requires multiple weeks of training (8–24 weeks of training) (Barban et al., 2017; Gillespie et al., 2012; Hauer et al., 2006; Schoene et al., 2014; Sherrington et al., 2017; Yosephi et al., 2018; Zieschang et al., 2013), which makes it very time-consuming and cost-intensive. In addition, some of the literature on balance training only supports small to moderate effects of exercise, especially in older adults (Cohen's d: 0.21 to 0.75) (Finnegan et al., 2019; Gillespie et al., 2012; Lee and Kim, 2017). Therefore, the development of a novel therapeutic approach for the treatment of balance disordes is a timely step, which may lead to better management of balance impairment and reduces the burden of diseases associated with poor balance.
In recent years, non-invasive brain stimulation (NIBS) techniques overe M1, SMA, DLPFC, and cerebellum, whether as a stand-alone or a priming technique, have emerged as a promising tool for modulation of the cortical sites for improvement of the behavioral outcomes such as balance in different pathological conditions (Bueno et al., 2019; Harris et al., 2018; Kang et al., 2016, 2020) and even in healthy individuals (Colnaghi et al., 2011; Craig and Doumas, 2017; Dutta et al., 2014; Ehsani et al., 2017; Foerster et al., 2017; Grimaldi et al., 2014; Holdefer et al., 2000; Inukai et al., 2016; Ishigaki et al., 2016; Kaminski et al., 2013, 2016, 2017; Kincses et al., 2004; Naro et al., 2017; Poortvliet et al., 2018; van Dun et al., 2017; Yitayeh and Teshome, 2016; Yosephi et al., 2018; Zandvliet et al., 2018; Zhou et al., 2014).
Before the use of this technique in the management of balance dysfunction in pathological conditions, systemic analysis of the results from proof-of-concept studies on healthy participants is necessary. Although many studies have evaluated the effects of NIBS on balance in recent years (Baharlouei et al., 2020; Colnaghi et al., 2011; Craig and Doumas, 2017; Ehsani et al., 2017; Fernandez et al., 2017; Galea et al., 2009; Kaminski et al., 2016; Poortvliet et al., 2018; Richard et al., 2017; Saruco et al., 2018), there is a lack of a comprehensive systematic analysis in this area of research. This study is the first systematic review of the literature that investigates the available evidence on the effects of a single session of different NIBS techniques on balance in healthy individuals. Therefore, this systematic review aimed at investigating the effects of a single-session, stand-alone NIBS technique at different brain sites on balance-related outcome measures in healthy adults. Besides, this review aimed at determining the level of evidence for NIBS to improve balance.
Materials and Methods
This review followed the suggestions of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement (Maher et al., 2003). Our computerized literature searches focused on the effects of NIBS on balance in healthy adults. Seven online scientific databases were used for the available research (Web of Knowledge, Science Direct, PubMed, Medline, Scopus, Springer, and Wiley online library) to find potential studies for inclusion in this systematic review up to the first week of April 2020. The Keywords and search phrases were “cortex” or “cortical”; and/or “motor cortex” or “primary motor cortex” or “M1”; and/or “dorsolateral prefrontal cortex” or “DLPFC” or “prefrontal cortex”; and/or “supplementary motor area” or “SMA”; and/or “cerebell” or “cerebellum” or “cerebellar”; and “balance” or “posture” or “postural control”; and/or one of the NIBS stimulation techniques as listed later: transcranial direct current stimulation (tDCS), transcranial magnetic stimulation (TMS), repetitive transcranial magnetic stimulation (rTMS), transcranial alternative current stimulation (tACS), paired associative stimulation (PAS), and theta burst stimulation (TBS).
Eligibility criteria
Studies who met the following criteria were included in the review: (1) Participants aged older than 18 years; (2) administration of a single session of one of the NIBS stimulation techniques as listed: tDCS, rTMS, tACS, PAS, and TBS; (3) measured any balance-related parameters before and after the stimulations; (4) availability of the full text in English; and (5) study approved by a medical ethical committee or review board.
Study selection
The first author (S.B.) and another author (S.J.) individually initially screened the titles and abstracts of the articles recognized by the search strategy to identify potentially eligible studies. Two reviewers (S.B. and S.J.) evaluate the eligibility of the studies in detail via full texts independently. In cases where eligibility for inclusion was unclear or two reviewers disagreed, the third author (M.Z.) consulted to read the articles independently. The period of literature searches was March 2018 to the first week of April 2020.
Data collection process and data items
The first author (S.B.), in consultation with the other authors, performed data extraction. The authors regularly discussed the data collection process to resolve disagreements and to ensure consistency. A standardized form was used to extract information regarding authors, study objectives, sample characteristics, inclusion and exclusion criteria, study design, experimental processes, NIBS protocols, outcome variables, and data analysis strategy.
The following descriptive data were extracted from each included study when available: (1) Participant demographic data and sample size; (2) mean and standard deviation (SD) of the outcome measures before and after the stimulation; and (3) characteristics of the NIBS procedure (electrode montage and size, current intensity, and period of stimulation). The flowchart of the selection procedure is presented in Figure 2. When the numeric data were not available, mean and SD were calculated from the available figures by the free Web Plot Digitizer gms 3.10 software (2018). Further, if the required data were not available or could not be obtained from supplementary material, the corresponding authors were contacted, and relevant data were requested.
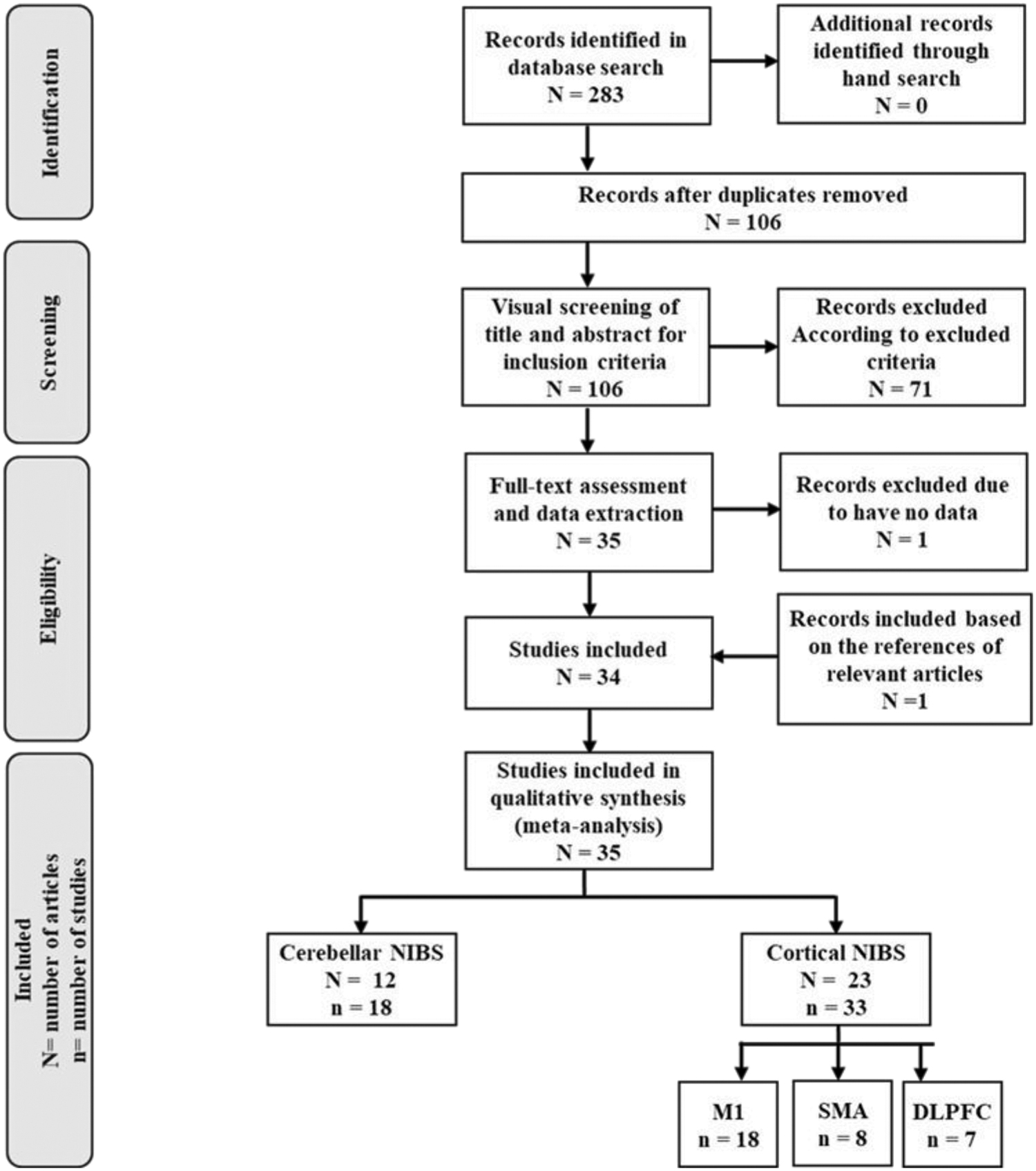
Flow diagram of study selection. cTBS, continuous theta burst stimulation; N, number of articles; n, number of studies; NIBS, non-invasive brain stimulation; tDCS, transcranial direct current stimulation.
The outcome measures of interest in the included studies were any outcome measure evaluating balance such as TIB (which is the mean of the time that specific balance position can be kept); COP displacement (which is the mean of mediolateral and anterior–posterior COP displacement in EO and/or EC situations in different balance tests).
Data analysis
Because the included studies were considered heterogeneous with regard to the study designs, NIBS technique and parameters, participants' characteristics, and outcome measures, performing a meta-analysis was not feasible. Therefore, in this review, “the best evidence synthesis” was performed. This review utilized the criterion that has been described in previous systematic reviews (de Visser et al., 2012; Maniar et al., 2016) to rank the level of evidence supporting a finding: Strong evidence: provided by two or more studies with high quality with generally consistent findings in all studies (≥75% of the studies reported consistent findings). Moderate evidence: provided by one high-quality study and two or more low-quality studies with generally consistent findings in all included studies (>75% of studies providing consistent findings). Limited evidence: provided by low-quality studies or in one high-quality study and by generally consistent findings (>75%). Conflicting evidence: provided by conflicting and inconsistent findings (<75% of studies showing consistent results). No evidence: provided when no studies or supportive findings could be found in the literature.
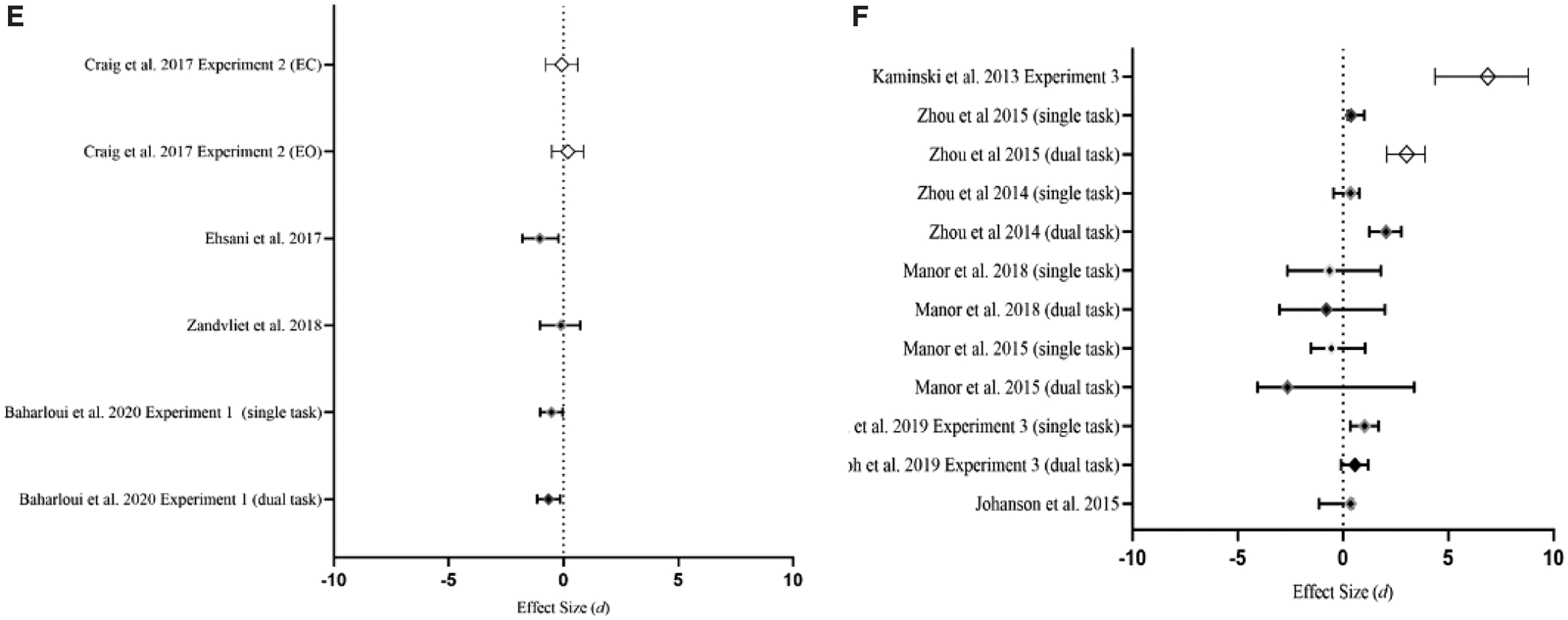
Based on the null hypothesis statistical test (significance tests and hypothesis tests), significant statistical testing is not enough to rely on, as it just provides information about the existence of the effects (Herbert, 2019). Therefore, Cohen's d effect size (Cohen, 1992; Greenfield et al., 1997; Hickey et al., 2018) was calculated to estimate the effect size of the included studies. According to the thresholds explained by Cohen, the effect size magnitude was interpreted as small (d = 0.20), moderate (d = 0.50), and large (d = 0.80) (Cohen, 1992). Also, the Cohen's d (Cohen, 1988) effect size and 95% confidence intervals were calculated and displayed in forest plots by using the Prism 8 for Windows (GraphPad Software, Inc., La Jolla, CA), for the purposes of visualizing key variables.
Risk-of-bias assessment
The methodological quality and risk of bias for each included study were assessed by using an adaptation of the criteria recommended in chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (Cumpston et al., 2019). The assessment areas were study design, selection bias, blinding, data collection method, data reporting, and withdrawals and dropouts. The quality of the included studies was assessed by the Downs and Black tool.50 Two authors (S.B. and S.J.) evaluated the quality of each study individually. The quality of the included studies was evaluated by the Downs and Black tool. Two researchers independently reviewed each article and gave a quality score by using the Downs and Black tool (Moher et al., 2009; Moseley et al., 2002). The Downs and Black tool contains 27 questions, of which 26 are graded on a 0 or 1 basis (“yes”/“no” or “not determined”); the remaining item is scored on a 0–2 scale. Thus, this scale ranges from 0 to 28, with a higher score indicating a higher methodologic quality (Downs and Black, 1998).
Results
Search result
Initially, the database search identified 283 articles, and 106 records remained after the removal of the duplicates. Based on the studies' titles and abstracts, only 35 articles were shortlisted. After screening of the full texts, 34 articles were included in the review. One more article was added after the hand screening of the references. The final sample comprised 35 published articles/articles included 51 studies. Some included articles included more than one study (Fig. 2).
Risk of bias and quality assessment
The risk of bias was different among studies for all assessment criteria. None of the 35 included articles was judged to have a high risk of bias across all criteria (Fig. 3).
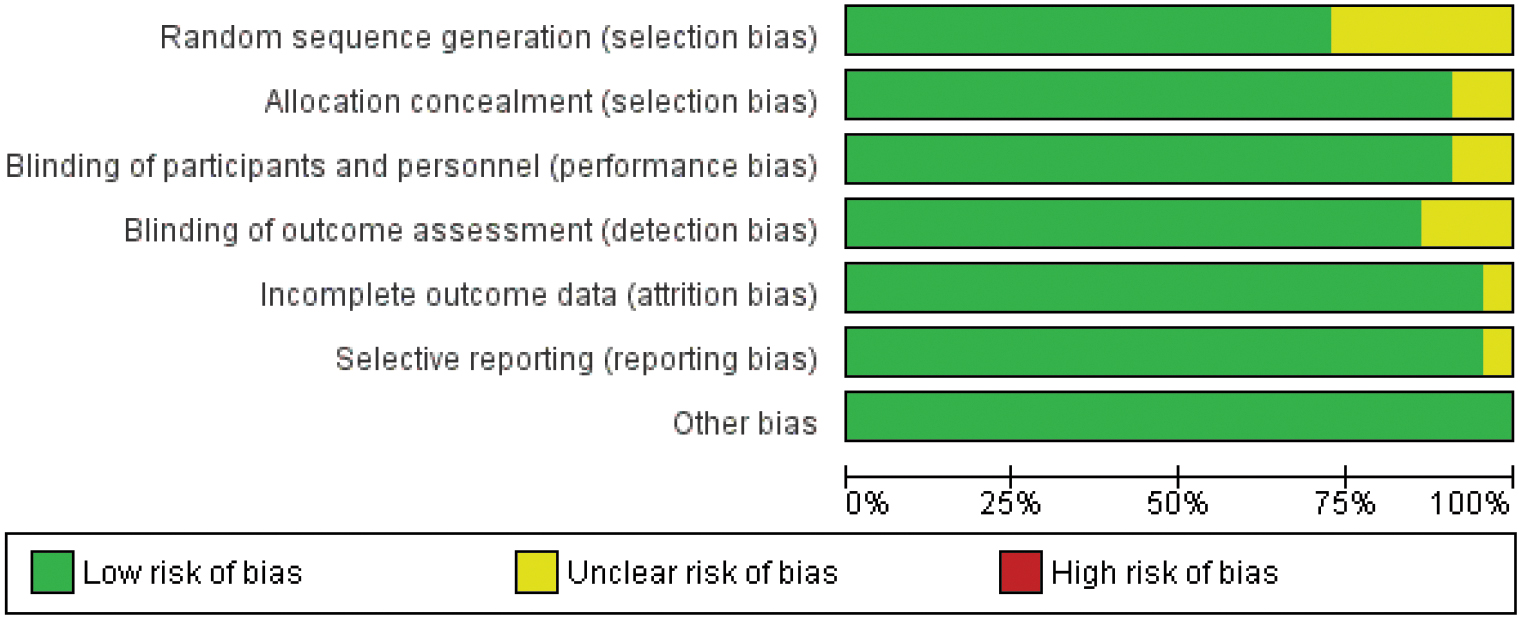
Risk-of-bias assessment of the included studies using the Cochrane Risk-of-Bias tool. Color images are available online.
From all included studies, six studies had unclear or inadequate information in random sequence generation, three studies had detection bias, two studies had allocation concealment bias, three had performance bias, and one study had reporting bias. The Downs and Black quality checklist provided high-quality scores for the included pre–post studies, ranging between 20 and 26 (22.83 ± 1.57) (Table 1).
Quality of Included Studies by Downs and Black Scale. Low-Quality Studies were Defined as Having a Risk-of-Bias Assessment Score of <70%, Whereas High-Quality Studies had a Score of ≥70%
Items 1–10 are for reporting criteria, items 11–13 for external validity, items 14–20 for internal validity (bias), items 21–26 internal validity (selection bias), item 27 for power.
Study characteristics
Most of the included articles had multiple studies evaluating the effects of different types of NIBS techniques on different stimulation sites over the brain. The included studies are divided and evaluated based on the location of the stimulation site: M1 (18 studies), SMA (8 studies), DLPFC (7 studies), and cerebellum (18 studies). All studies evaluated balance by using different outcome measures before and immediately after the NIBS techniques. Also, because the physiology of aging might have some effects on the results, the studies have been categorized into two main groups of participants: young and older participants.
Best evidence synthesis
Primary motor cortex
Eighteen studies were included (Baharlouei et al., 2020; Cioncoloni et al., 2016; Craig and Doumas, 2017; Dutta and Chugh, 2012; Dutta et al., 2014; Ehsani et al., 2017; Goh et al., 2019; Ishigaki et al., 2016; Kaminski et al., 2016, 2017; Lee, 2012; Nonnekes et al., 2014; Pohjola et al., 2017; Saruco et al., 2017, 2018; Zhou et al., 2018). Among all included studies, 14 studies evaluated the effects of anodal transcranial direct current stimulation (a-tDCS) (Baharlouei et al., 2020; Craig and Doumas, 2017; Dutta and Chugh, 2012; Dutta et al., 2014; Ehsani et al., 2017; Ishigaki et al., 2016; Kaminski et al., 2016, 2017; Lee, 2012; Nonnekes et al., 2014; Pohjola et al., 2017; Saruco et al., 2017, 2018; Zhou et al., 2018), 1 study evaluated the effects of cathodal transcranial direct current stimulation (c-tDCS) (Ishigaki et al., 2016), 1 study used continuous theta burst stimulation (cTBS) (Cioncoloni et al., 2016), and 1 study used rTMS (Goh et al., 2019).
a-tDCS of primary motor cortex in young participants
Fourteen studies with 268 participants evaluated the effects of a-tDCS on the M1 (Baharlouei et al., 2020; Craig and Doumas, 2017; Dutta and Chugh, 2012; Dutta et al., 2014; Ehsani et al., 2017; Ishigaki et al., 2016; Kaminski et al., 2016, 2017; Lee, 2012; Nonnekes et al., 2014; Pohjola et al., 2017; Saruco et al., 2017, 2018; Zhou et al., 2018), in young healthy adults (9 studies) (Craig and Doumas, 2017; Dutta and Chugh, 2012; Dutta et al., 2014; Kaminski et al., 2016; Lee, 2012; Nonnekes et al., 2014; Pohjola et al., 2017; Saruco et al., 2017, 2018) (Table 2) or older adults (5 studies) (Baharlouei et al., 2020; Craig and Doumas, 2017; Dutta et al., 2014; Kaminski et al., 2017; Zhou et al., 2018) (Table 3). In the nine studies that used a-tDCS in young adults (Craig and Doumas, 2017; Dutta and Chugh, 2012; Dutta et al., 2014; Kaminski et al., 2016; Lee, 2012; Nonnekes et al., 2014; Pohjola et al., 2017; Saruco et al., 2017, 2018), seven studies found significant balance improvement (Dutta and Chugh, 2012; Dutta et al., 2014; Kaminski et al., 2016; Lee, 2012; Nonnekes et al., 2014; Saruco et al., 2017, 2018), whereas the other two did not report any significant changes (Craig and Doumas, 2017; Pohjola et al., 2017) (Table 2). It is worth mentioning that two studies that showed significant improvement had large to very large effect sizes (Cohen's d: −1.9 to 2.11) (Kaminski et al., 2016; Nonnekes et al., 2014), and the other five studies had very small to moderate effect sizes (Cohen's d: −0.03 to −0.65) (Craig and Doumas, 2017; Dutta and Chugh, 2012; Dutta et al., 2014; Lee, 2012; Saruco et al., 2017, 2018), whereas two studies without any significant balance improvements had small to moderate effect sizes (Cohen's d: 0.18 to −0.59) (Fig. 4A).

Forest plot for effect size of studies stimulating
Studies Categorized Based on the Cortical Stimulation Site in Young Participants
NM, not mentioned; RCT, randomized control trial; ML, medio-lateral; AP, anterior-posterior; EO, eyes open; EC, eyes closed; tDCS, transcranial direct current stimulation; rTMS, repetitive transcranial magnetic stimulation; cTBS, continuous theta burst stimulation; MGOe, maximum energy density; COP, center of pressure, BS, Berg Balance Scale; TIB, time in balance; FRIGHT, functional reach task; TUG, timed up and go; FES, fall efficacy scale; EmNSA-LE, Erasmus modification of the Nottingham Sensory Assessment of the Lower Extremity; PFC, prefrontal cortex; DLPFC, dorsolateral prefrontal cortex; SMA, supplementary motor area; RMT, resting motor threshold; aMT, active motor threshold; MGOe, maximum energy density; EEG, electro-encephalography; EMG, electromyography; MMSE, mini-mental state examination; MoCA, montreal cognitive assessment. ↔, The outcome unchanged significantly; ↓, the outcome decreased significantly; ↑, the outcome increased significantly.
Studies Categorized Based on the Cortical Stimulation Site in Older Participants
↔, The outcome unchanged significantly; ↓, the outcome decreased significantly; ↑, the outcome increased significantly.
Overall, based on the included studies, more than 75% of high-quality studies showed significant effects with small to medium effects size in young adults. According to the large level of effect sizes and strong evidence in the best evidence synthesis, it can be concluded that a single-session a-tDCS on M1 has a positive effect on balance in both young adults.
a-tDCS of primary motor cortex in older participants
Moreover, five studies targeted the M1 of older adults with a-tDCS (Baharlouei et al., 2020; Craig and Doumas, 2017; Dutta et al., 2014; Kaminski et al., 2017; Zhou et al., 2018). Three studies found significant improvement, with small to moderate comparative effects (Cohen d: −0.14 to −1.63) (Baharlouei et al., 2020; Dutta et al., 2014; Zhou et al., 2018) whereas two studies only showed small to moderate effects, without any significant effects (Cohen's d: −0.39 to 0.71) (Craig and Doumas, 2017; Kaminski et al., 2013).
According to results of the included studies, more than 75% of high-quality studies had significant effects with small to medium effect sizes in older adults. In line with the large level of effect sizes and strong evidence in the best evidence synthesis, it can be concluded that a single-session a-tDCS on M1 has a positive effect on balance in older adults (Fig. 4B).
Other stimulation techniques on primary motor cortex
In addition, one study investigated the effects of c-tDCS on M1 on balance and showed no significant changes with very low effect sizes (Cohen's d: 0.25 to 0.03) (Ishigaki et al., 2016) (Tables 2 and 3). One study evaluated the effects of rTMS (Cohen's d dual task: 1.06, Cohen's d single task: −0.38) (Goh et al., 2019), and two studies investigated the effects of cTBS (Cohen's d: −0.14 to −0.15) (Cioncoloni et al., 2016). None of these studies found any significant effects on balance after M1 stimulation.
Supplementary motor area
Eight studies evaluated the effects of NIBS of the SMA on balance (Goel et al., 2019; Goh et al., 2019; Johannsen et al., 2015; Kaminski et al., 2013; Nomura and Kirimoto, 2018; Richard et al., 2017; Tsuru et al., 2020). Three studies used a-tDCS on the SMA and evaluated balance indices in healthy adults (Kaminski et al., 2013; Nomura and Kirimoto, 2018), two studies evaluated TIB in young adults (Kaminski et al., 2013), and one study evaluated the changes of the COP in older adults (Nomura and Kirimoto, 2018). These two studies on young participants found no significant changes (Kaminski et al., 2013) (Table 2 and Fig. 4C), but one study on older adults showed significant improvements in balance (Nomura and Kirimoto, 2018) (Table 3 and Fig. 4C). However, the large effect sizes in these three studies suggest that a-tDCS of SMA can improve TIB in healthy adults (Cohen's d: −1.75 to 4.70) (Kaminski et al., 2013; Nomura and Kirimoto, 2018). Given the strong evidence provided by best evidence synthesis, it seems that a-tDCS of the SMA can improve the balance of healthy adults as shown by the large comparative effect sizes (Cohen's d: −1.75 to 4.70) (Tables 2 and 3).
Moreover, two out of eight studies evaluated the effects of rTMS (Goh et al., 2019; Johannsen et al., 2015) and the results were inconsistent. One of these studies found a significant difference with large effect size (Cohen's d: 0.94) (Goh et al., 2019), whereas the other study did not find any effect (Cohen's d: 0.36) (Johannsen et al., 2015) (Table 2). Further, two studies evaluated the effects of the cTBS over the SMA on COP displacement and did not find any significant changes in balance with moderate effect size (Cohen's d: 0.57) (Goel et al., 2019; Richard et al., 2017). In addition, one study used Transcranial magnetic field stimulation on SMA and found significant improvement (Tsuru et al., 2020) (Tables 2 and 3).
Dorsolateral prefrontal cortex
Seven studies that evaluated the effects of NIBS of the DLPFC on balance were included (Goh et al., 2019; Johannsen et al., 2015; Kaminski et al., 2013, 2017; Manor et al., 2016, 2018; Zhou et al., 2014, 2015). Among these, five studies have investigated the effect of a-tDCS of the left DLPFC on balance (Kaminski et al., 2013; Manor et al., 2016, 2018; Zhou et al., 2014, 2015). Two out of these five studies evaluated balance in young participants (Kaminski et al., 2013; Zhou et al., 2014), whereas the other three recruited older adults (Manor et al., 2016, 2018; Zhou et al., 2015). In both young and older participants, none of the studies showed significant improvements in the single task balance (simple balance task without cognitive load) of healthy individuals (Manor et al., 2016, 2018; Zhou et al., 2014, 2015) (Tables 2 and 3 and Fig. 4F). Accordingly, best evidence synthesis shows strong evidence and consistent results with low to very large effect size (Cohen's d: −0.36 to −1.81), suggesting that a-tDCS of DLPFC might not have any effects on single balance tasks in healthy participants. The effect size of these studies showed that a-tDCS of the DLPFC is decreasing the center of gravity alignment sway velocity in single tasks (Cohen's d: 0.36 to −1.81), although the studies did not find any significance (Manor et al., 2016, 2018; Zhou et al., 2014). Also, one study found no significant effect on the single task performance after the a-tDCS of DLPFC (Cohen's d: 0.38) (Zhou et al., 2015). Moreover, best evidence synthesis suggests strong evidence, with a large effect size showing that a-tDCS of the DLPFC improves balance in dual tasks (Cohen's d: −2 to 6.88) (Kaminski et al., 2013; Manor et al., 2016, 2018; Zhou et al., 2014, 2015).
Moreover, two studies found that rTMS of the DLPFC had no significant effects on improving single balance (Cohn's d: −0.36 to −0.13) (Goh et al., 2019; Johannsen et al., 2015). However, very large effect sizes were observed after rTMS of the DLPFC during dual tasks, suggesting some improvements in dual task effects after this type of stimulation (Cohn's d: −3.38 to 1.17) (Goh et al., 2019; Johannsen et al., 2015).
Cerebellum
Eighteen studies have reported the effects of different cerebellar NIBS techniques on a range of outcome measures for assessment of balance (Baharlouei et al., 2020; Colnaghi et al., 2011; Craig and Doumas, 2017; Ehsani et al., 2017; Fernandez et al., 2017; Foerster et al., 2017; Inukai et al., 2016; Naro et al., 2017; Poortvliet et al., 2018; Richard et al., 2017; Steiner et al., 2016, 2020; Zandvliet et al., 2018). The effects of a-tDCS on balance were investigated in 10 studies (Baharlouei et al., 2020; Craig and Doumas, 2017; Ehsani et al., 2017; Foerster et al., 2017; Inukai et al., 2016; Poortvliet et al., 2018; Steiner et al., 2016, 2020; Yosephi et al., 2018; Zandvliet et al., 2018), with 6 studies on young adults (Craig and Doumas, 2017; Foerster et al., 2017; Inukai et al., 2016; Poortvliet et al., 2018; Steiner et al., 2016, 2020) and 4 studies on older adults (Baharlouei et al., 2020; Craig and Doumas, 2017; Ehsani et al., 2017; Zandvliet et al., 2018).
a-tDCS of cerebellum in young participants
Two out of six studies used a-tDCS in young participants and demonstrated a significant effect on improving balance in healthy adults (Cohen's d range 0.26 to −1.67) (Poortvliet et al., 2018; Steiner et al., 2020), whereas four other studies found some improvement, without significance, but demonstrated a small to large comparative effect (Cohen's d range 0.1 to 1.53) (Craig and Doumas, 2017; Foerster et al., 2017; Inukai et al., 2016; Steiner et al., 2016) (Table 4 and Fig. 4D). Best evidence synthesis demonstrated conflicting evidence for cerebellar a-tDCS to improve balance. However, given the large effect sizes of the individual studies, cerebellar a-tDCS seems to have a positive effect on balance.
Studies Categorized Based on the Cerebellar Stimulation Site in Young Participants
↔, The outcome unchanged significantly; ↓, the outcome decreased significantly; ↑, the outcome increased significantly.
tACS, transcranial direct current stimulation; VAS, visual analogue scale.
a-tDCS of cerebellum in older participants
In addition, two out of four studies that evaluated a-tDCS on older adults found significant improvement in balance (Cohen's d range −0.65 to −1.3) (Baharlouei et al., 2020; Ehsani et al., 2017). Also, two other studies did not find any significant effect on balance, with small effect sizes (Cohen's d: 0.1 to 0.2) (Craig and Doumas, 2017; Zandvliet et al., 2018) (Table 5 and Fig. 4E). Although the best evidence synthesis suggests some conflicting evidence regarding cerebellar a-tDCS effects on balance, however according to the large effect sizes of the two studies, cerebellar a-tDCS may have positive effects on balance.
Studies Categorized Based on the Cerebellar Stimulation Site in Older Participants
↔, The outcome unchanged significantly; ↓, the outcome decreased significantly; ↑, the outcome increased significantly.
BBS, Berg Balance Scale; FES, fall efficacy scale; FRIGHT, functional reach task.
Moreover, five studies investigated the effects of cerebellar c-tDCS on balance indices in young healthy individuals (Fernandez et al., 2017; Foerster et al., 2017; Inukai et al., 2016; Steiner et al., 2016, 2020). Two of these studies showed that c-tDCS could significantly deteriorate balance in healthy adults (Cohen's d: −0.12 to −1.67) (Foerster et al., 2017; Inukai et al., 2016), whereas the other three did not find any significant changes on balance (Cohen's d: 0.43 to −0.9) (Fernandez et al., 2017; Steiner et al., 2016, 2020). However, large effect size in one of these studies suggests deterioration of balance after cerebellar c-tDCS (Cohen's d: −0.9) (Fernandez et al., 2017). As a result, best evidence synthesis found that c-tDCS of the cerebellum impairs balance in healthy adults. Moreover, one study used tACS (Naro et al., 2017), two studies used cTBS (Colnaghi et al., 2011; Richard et al., 2017), and none of them found any significant effects on balance (Tables 4 and 5).
Discussion
Thirty-five articles with 51 studies were included in this systematic review. The main aim of this review was to summarize the literature on the effects of single-session, stand-alone NIBS techniques at different brain sites on postural balance. To the best of the authors' knowledge, this is the first systematic review providing a comprehensive evaluation of the effects of NIBS techniques, including a-tDCS, c-tDCS, tACS, and cTBS on the balance in healthy individuals. Overall, we had enough data to reach a meaningful conclusion on the effect of some NIBS techniques such as a-tDCS of M1 and cerebellum on improving balance in young healthy participants. On the other hand, for the effects of a-tDCS in older adults and the effects of other techniques such as c-tDCS, tACS and cTBS, the current evidence is not enough to reach any meaningful conclusion.
In this review, the included studies were categorized based on the site of stimulation. This included stimulation of M1, SMA, DLPFC, and cerebellum. The results showed that a-tDCS applied to the M1, and cerebellum could improve balance indices. Although a-tDCS of DLPFC and SMA did not produce any significant improvement on balance, the large effect sizes suggest that some improvement was seen in balance indices after a-tDCS of DLPFC and SMA, which seems, at a minimum, to be clinically important. The results also indicate that cTBS of the cerebellum significantly deteriorates balance in healthy participants.
The effects of M1 stimulation on balance in young participants
The results of this review suggest that a single session of a-tDCS on M1 might have positive effects on balance in healthy individuals. Fourteen studies assessed the effects of the stand-alone, single session a-tDCS over the bilateral lower limb M1 on the TIB and COP displacement (Baharlouei et al., 2020; Craig and Doumas, 2017; Dutta and Chugh, 2012; Dutta et al., 2014; Ehsani et al., 2017; Ishigaki et al., 2016; Kaminski et al., 2016, 2017; Lee, 2012; Nonnekes et al., 2014; Pohjola et al., 2017; Saruco et al., 2017, 2018; Zhou et al., 2018), and among all these studies just two studies failed to show any significant improvement (Craig and Doumas, 2017; Pohjola et al., 2017).
The main reason behind this discrepancy lies in the differences between the electrode stimulation site and the size of the active electrode in studies with higher effect size and significant results. For example, Pohjola et al. (2017) stimulated the C3, which is the M1 for the hand area, and found no significant improvement in balance indices. Although this study had a moderate effect size, no significant improvement was found. It is believed that the possible reason lay in the fact that there was no attempt to stimulate bilateral lower limb and trunk area in M1, which are the muscles responsible for the control of balance. In the other study, Craig and Doumas (2017) used a very big active electrode (50 cm2) over the Cz and reported no significant improvement in the balance indices. The issue with such a large pair of electrodes is a dramatic reduction of the current density and total charge compared with the smaller electrodes used in other studies. In addition, based on the small to large effect size found in the studies with significant balance improvement, it can be said that the a-tDCS with 1–2 mA, 15–20 min seems to be effective in the improvement of balance (Kaminski et al., 2016; Lee, 2012; Nonnekes et al., 2014; Zhou et al., 2018).
The effects of M1 stimulation on balance in older participants
Similar to the findings in younger adults, five studies investigated the effects of M1 a-tDCS on balance in older adults (Baharlouei et al., 2020; Craig and Doumas, 2017; Dutta et al., 2014; Kaminski et al., 2017; Zhou et al., 2018). Although only three studies reported statistically significant improvement (Baharlouei et al., 2020; Dutta et al., 2014; Zhou et al., 2018), all five studies found small to moderate effect sizes and improvement in balance indices. This discrepancy among studies that targeted older adults can first be explained by the difference in the stimulation density, which is dependent on the intensity and the size of the active electrodes. It has been shown that a density of less than 0.05 mA/cm2 is not able to make any significant changes in the balance of older adults (Craig and Doumas, 2017; Kaminski et al., 2017). Craig and Doumas (2017) used larger active and return electrodes (50, 25 cm2), with the 2 mA a-tDCS (density: 0.04 mA/cm2). Moreover, Kaminski et al. (2017) used 1 mA a-tDCS with a 25 cm2 active electrode, leading to a density of 0.04 mA/cm2 and did not find any significant changes in balance. Also, it has been suggested that differences in the brain processing between older and younger adults may be a reason for not having significant changes compared with younger participants (de Vries et al., 2014; Hernandez et al., 2012a, 2012b; Mouthon et al., 2016). Moreover, older adults have a slower and less accurate response to COP changes during movements in comparison with younger adults, which makes the sensitivity of balance outcome measure less in these populations (de Vries et al., 2014; Hernandez et al., 2012a, 2012b). Therefore, these conflicting results demonstrate the necessity of further well-controlled studies to reach a consensus about the stimulation intensity and duration, and electrode montages on balance-related outcomes.
The effects of SMA and DLPFC stimulation on balance
Within the eight studies that targeted SMA (Goel et al., 2019; Goh et al., 2019; Johannsen et al., 2015; Kaminski et al., 2013; Nomura and Kirimoto, 2018; Richard et al., 2017; Tsuru et al., 2020), three studies found significant improvement on the balance after a-tDCS of SMA regardless of the participants' age, with very large effect sizes (Cohen's d: −1.75 to 4.70) (Kaminski et al., 2013; Nomura and Kirimoto, 2018). Although the study of Kaminski et al. (2013) showed significant changes compared with the baseline of active stimulation with very large effect size, without significant changes compared with the sham stimulation,53 the large effect suggests that a-tDCS of the SMA is clinically meaningful to improve balance. One of the possible reasons is due to some difference in the baseline measures of both stimulation and sham groups. The other reason behind this discrepancy might be the homeostatic mechanisms and reversal of the a-tDCS effects in some studies (Karabanov et al., 2015; Muller-Dahlhaus and Ziemann, 2015). The effects of the a-tDCS have been introduced as non-linear, with complex behavior (Hassanzahraee et al., 2020; Monte-Silva et al., 2013; Nitsche and Paulus, 2000; Nitsche et al., 2003; Tremblay et al., 2016). These effects depend on many factors, mainly NMDA receptors and calcium channel activities (Hassanzahraee et al., 2020; Monte-Silva et al., 2013; Nitsche and Paulus, 2000; Nitsche et al., 2003; Tremblay et al., 2016). Recent studies have suggested that there is a specific duration and intensity, called duration or intensity window, for a-tDCS that can reverse the effect of a-tDCS (Hassanzahraee et al., 2020; Monte-Silva et al., 2013). It seems that in that specific duration or intensity window, neuronal counter-regulatory mechanisms are activated and they convert the direction of the effects of a-tDCS. Also, the other possible reason may be described by the stimulation intensity and electrode size. The study by Nomura and Kirimoto (2018) showed that using smaller active electrodes (9 cm2), and higher intensity and therefore higher current density and total charge are increasing the level of significance in COP displacement in older adults.
Moreover, five studies examined the effect of a-tDCS of the DLPFC on balance (Kaminski et al., 2013, 2017; Manor et al., 2016, 2018; Zhou et al., 2014, 2015). Regardless of the different outcome measures used, these studies failed to show any significant improvements in balance indices of single tasks (Kaminski et al., 2013, 2017; Manor et al., 2016, 2018; Zhou et al., 2014, 2015). However, some studies found that a-tDCS of the DLPFC may only improve the dual-task standing performance, not the single-task standing performance (Manor et al., 2016, 2018; Zhou et al., 2014, 2015). The main reason behind this finding is the fact that the DLPFC is mainly responsible for executive control of the more complex tasks (Mihara et al., 2008; Zhou et al., 2014, 2015) than the balance tasks, which are mainly controlled by reflexive control through the cerebellum and vestibular system (Solis-Escalante et al., 2019). This reasoning indicates that the type of tasks or outcome measures are the important factors that determine the effects of a-tDCS in studies targeting DLPFC.
The effects of cerebellar stimulation on balance
Eighteen studies have utilized cerebellar NIBS on a range of balance-related outcomes (Baharlouei et al., 2020; Colnaghi et al., 2011; Craig and Doumas, 2017; Ehsani et al., 2017; Fernandez et al., 2017; Foerster et al., 2017; Inukai et al., 2016; Naro et al., 2017; Poortvliet et al., 2018; Richard et al., 2017; Steiner et al., 2016, 2020; Zandvliet et al., 2018). The overall findings of the systematic review indicate conflicting evidence in both young and older adults. It seems that a-tDCS of the cerebellum may improve the indices of balance to some extent in both age groups, and it has the same effects in both young and older adults (Baharlouei et al., 2020; Ehsani et al., 2017; Poortvliet et al., 2018; Steiner et al., 2020), but this effect is not reported in all studies. The main reasons behind these inconsistencies might be because of different stimulation parameters and different electrode montages used in these studies. As can be seen, the electrode montage is one of the main factors leading to significant changes in postural balance. It seems that placement of the active electrode on the inion or maximum 1.5 cm below the inion increases the chance of significant balance improvement after cerebellar a-tDCS (Baharlouei et al., 2020; Ehsani et al., 2017; Steiner et al., 2020). Another important factor is the stimulation parameters. The overall results suggest that some significant improvement may occur, after using at least 10 min a-tDCS with an intensity of ≥1 mA, by applying the active electrode over the inion or maximum 1.5 cm below the inion (Baharlouei et al., 2020; Ehsani et al., 2017). Although there is no explicit explanation for these findings, it can be explained based on the cerebellar physiology and the amount of total charge that is stimulating the cerebellar cells. It is suggested that the cerebellar parts that are close to the inion, the posterior and inferior parts of the cerebellum (i.e., lobules VI–VIII), are particularly susceptible to be modulated by cerebellar a-tDCS. Hence, the montage that can stimulate these parts is more successful (Allen et al., 2005; Baillieux et al., 2008; E et al., 2014; Grimaldi et al., 2016; Mauk et al., 2000). Moreover, it has been proposed that the proper stimulation parameter of cerebellar a-tDCS can polarize Purkinje cells and change the levels or pattern of activity in the deep cerebellar nuclei output and affect the cerebellar activity (Baillieux et al., 2008; Bastian, 2006; Bellebaum and Daum, 2007; Galea et al., 2009; Grimaldi et al., 2016).
The effects of cerebellar c-tDCS (Fernandez et al., 2017; Foerster et al., 2017; Inukai et al., 2016; Steiner et al., 2016) on balance showed some consistent results. Two studies showed a significant decrease in balance ability (Foerster et al., 2017; Inukai et al., 2016), whereas the other studies did not find any significant changes (Fernandez et al., 2017; Steiner et al., 2016, 2020). One of the main differences between these two groups of studies lies in the electrode montages used in these studies. Fernandez et al. (2017) used unilateral cerebellar stimulation, whereas the other two studies, Inukai et al. (2016) and Foerster et al. (2017), used bilateral cerebellar stimulation. Overall, these findings suggest that the c-tDCS deteriorates balance ability, and it is better not to use it for treatment of balance. This finding is in line with current research studies that showed that the c-tDCS blocks and depresses the stimulated brain region and creates temporary cortical dysfunctions known as virtual lesions (Nitsche and Paulus, 2000, 2001; Schlaug et al., 2008).
Limitations of the study
The findings of this review should be considered in light of some limitations. First, the paucity of research in some NIBS techniques (such as c-tDCS, cTBS, or rTMS) limits the interpretation of the results. Second, the heterogeneity of the outcomes and stimulation parameters in the included studies prevented the meta-analysis. Finally, the low sample size in some of the included studies may have underpowered the significant results in some studies, and hence the small effects may not have been detected in these studies.
Suggestions for future research
This systematic review concluded that single-session a-tDCS of M1 and cerebellum might be effective in the improvement of postural balance. Although the single-session a-tDCS had statistically significant therapeutic effects, the lasting effects of a single session were not long enough to clinically improve the postural balance. Therefore, the importance of examining the effects of multiple-session NIBS on balance is highlighted. Also, given the complexities and multidimensional nature of brain activities, more sensitive outcome measures are needed (e.g., TMS, reaction time, and error rate) in parallel to balance-related outcome measures. These sensitive outcomes help to structurally investigate the mechanism of effects of the NIBS on balance. Also, these sensitive outcome measures may increase the information about physiological reasons behind findings and the ability in translating findings to clinical applications. Besides, future research should also seek to address the methodological limitations identified in the review, primarily regarding proper blinding, carefully planned randomized control trials, and larger sample size to reach more valid and reliable results. More studies are needed to explore the effects of NIBS on the balance of patients with different pathologies, and these would be extremely useful and can be used as a therapeutic approach.
Clinical implications
The findings in this review indicate that single-session, stand-alone application of a-tDCS on the cerebellum, M1, and SMA can improve balance in a healthy individual. Moreover, this review showed that c-tDCS has a deteriorating effect on balance and must be avoided as a technique for the treatment of balance. The results of this study can be used to improve balance in patients with neurological disorders, and healthy older adults with balance problems.
Conclusion
This systematic review indicates that a-tDCS of M1 is effective in the improvement of balance indices in healthy younger and older adults. Also, the a-tDCS of the cerebellum can be effective on the balance if the montage and stimulation parameters are selected accurately. Likewise, large effect sizes in the studies evaluating the effects of a-tDCS of the SMA are suggesting improvement of balance after a-tDCS of SMA, although some studies failed to show any significant improvement in indices of balance. In addition, it has been found that a-tDCS of DLPFC can only improve the balance of dual tasks, but not single tasks. Moreover, the finding in the current study indicates that c-tDCS of the cerebellum has significantly deteriorated the balance in healthy participants.
Footnotes
Authors' Contributions
Conceived and designed the study: S.B., M.Z., D.K., and S.J.; performed data collection: S.B.; conducted the analysis: S.B.; interpreted the findings: S.B., S.J.; wrote the article: S.B.; and writing and editing of drafts: S.B., M.Z., D.K., and S.J.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.