
Abstract
Background:
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is characterized by leukoencephalopathy leading to cognitive impairment. Subtle cognitive deficits can be observed early in the course of the disease, before the occurrence of the first stroke. Therefore, markers that can predict disease progression at this early stage, when interventions are likely to alter disease course, are needed. We aimed to examine the biological cascade of microstructural and macrostructural white matter (WM) abnormalities underlying cognitive deficits in CADASIL.
Methods:
We examined 20 nondemented CADASIL mutation carriers and 23 noncarriers who underwent neuropsychological evaluation and magnetic resonance imaging. Using probabilistic tractography of key WM tracts, we examined group differences in diffusivity measures and WM hyperintensity volume. Successive mediation models examined whether tract-specific WM abnormalities mediated subtle cognitive differences between CADASIL mutation carriers and noncarriers.
Results:
The largest effect size differentiating the two groups was observed for left superior longitudinal fasciculus–temporal (SLFt) diffusivity (Cohen's f = 0.49). No group differences were observed with a global diffusion measure. These specific microstructural differences in the SLFt were associated with higher WM hyperintensities burden, and subtle executive deficits in CADASIL mutation carriers.
Discussion:
Worse diffusivity in the left SLFt is related to greater severity of small vessel disease and worse executive functioning in the asymptomatic stage of the disease. Worse diffusivity of the left SLFt may potentially hold promise as an indicator of disease progression.
Impact statement
Diffusion tensor imaging outperforms conventional imaging of subcortical small vessel disease as a potential marker of future disease progression. Here we identified the left superior longitudinal temporal fasciculus as a critical white matter fiber bundle, of which worse diffusivity can link presence of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy mutations to greater severity of small vessel disease and worse executive functioning in asymptomatic stages of the disease. This tract may hold promise and deserves further examination as an early indicator of disease progression.
Introduction
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), the most frequent inherited nonamyloid type of cerebrovascular disease, is caused by mutations in the NOTCH3 gene (Chabriat et al., 2009, 2020; Dichgans et al., 1998; Joutel et al., 1996). It is characterized by leukoencephalopathy that is also often observed in older individuals with hypertension, but emerges at an earlier age (Chabriat et al., 1998, 2009; Herve and Chabriat, 2010). The natural course of CADASIL is variable but neurological symptoms can include migraine headaches and changes in behavior and personality (Chabriat et al., 2009). These symptoms can occur as early as age 30 years, and multiple consecutive transient ischemic attacks or strokes lead to insidious cognitive impairment progressing to dementia by age 65 years (Chabriat et al., 2009; Opherk et al., 2004). Subtle signs of cognitive decline, in particular in executive functions, can be observed before occurrence of the first stroke (Zuluaga-Castaño et al., 2018). In particular, the presence of lacunar infarcts is an important predictor of cognitive dysfunction and disability (Lee et al., 2011; Liem et al., 2007; Viswanathan et al., 2007).
Because of the lack of treatment options and the substantial impact on young families, there is a need to predict progression from its asymptomatic phase. Early detection is usually focused on measuring T2 lesion load, but this has low pathological specificity and low sensitivity to occult tissue damage in normal-appearing white matter (WM) (Schoemaker et al., 2019; Shi et al., 2018). Diffusion-weighted magnetic resonance imaging (MRI) is sensitive to WM abnormalities that cannot yet be detected with conventional MRI and has potential to provide information on microstructural changes linked to cognitive function or to precede small vessel disease pathology (Jacobs et al., 2012; Konieczny et al., 2020; Molko et al., 2002; O'Sullivan et al., 2004). Previous studies reported widespread abnormal diffusivity in WM lesions and normal appearing WM in symptomatic CADASIL patients (Ban et al., 2019; Holtmannspotter et al., 2005; Mascalchi et al., 2017), and more focal patterns of WM damage in asymptomatic individuals (O'Sullivan et al., 2004, 2005). Higher mean diffusivity (MD) in the cingulum bundle, but not in the thalamus, correlated with worse executive performance (O'Sullivan et al., 2004, 2005). Microstructural metrics obtained with diffusion tensor imaging (DTI) can be valuable for prognostic purposes given that they may signal impending macrostructural WM alterations. Although previous study indicated that worse diffusivity occurs in regions affected by small vessel disease (Chabriat et al., 1999; Mascalchi et al., 2017; Yin et al., 2018), so far no study has examined whether specific microstructural changes are associated with the initial small vessel disease lesions and consequently cognitive deficits in CADASIL.
In this study, we examined whether tract-specific WM abnormalities mediate CADASIL-related subtle cognitive differences between asymptomatic CADASIL mutation carriers and clinically normal noncarriers. In addition, we also examined the successive mediation of these tract measures and WM lesions on CADASIL-related cognitive performance.
Materials and Methods
Participants
Twenty individuals carrying R141C (n = 3), R1031C (n = 15), or C455R (n = 2) mutations and 23 noncarrier controls were recruited through families with confirmed CADASIL mutations on the Sistema de Informacion del Grupo de Neurociencias de Antioquia database, using a random sampling approach. Participants underwent comprehensive clinical (including medical history of cardiovascular risk factors) and neuropsychological testing and neuroimaging. Informed consent was approved by the ethical committee of the University of Antioquia. This study is in accordance with the Declaration of Helsinki. Exclusion criteria were prior neurological illness other than CADASIL, a history of psychiatric illness or noncontrolled systemic disease, or illiteracy, a mini-mental state examination score (MMSE) <23, and contraindications for MRI. All participants had a functional assessment staging (FAST) between 1 and 2, and no history of a cerebrovascular accident. DNA extraction determined the mutation type. Data collection was performed double blind, in which participants and investigators were not informed of the genetic status.
Neuropsychological assessment
All participants completed the MMSE, semantic and phonological fluency, the memory capacity test, the Institute of Cognitive Neurology (INECO) Frontal Screening, the Colombian-normed version of the Consortium to Establish a Registry for Alzheimer's Disease (CERAD) Neuropsychological Battery (including word list learning), Digit Symbol Substitution Test (DSST) from the Wechsler Adult Intelligence Scale, and the Stroop color word test (SCWT). In addition, we administered the geriatric anxiety inventory and geriatric depression scale to assess anxiety and depressive symptoms. We created two composites using the average of the z-transformed scores of subtests: (1) an executive functioning consisting of the INECO and the SCWT and (2) a memory composite consisting of the CERAD memory tests.
Magnetic resonance imaging
All MRI was performed at the Hospital Pablo Tobon Uribe in Medellin on a 3T Siemens system with a 12-channel phased-array head coil. The protocol included a T1-weighted magnetization–prepared rapid-acquisition gradient-echo sequence (repetition time [TR] = 2000 msec, echo time [TE] = 4.25 msec, flip angle = 9°; and 0.96 mm isotropic, field of view [FOV] = 245 × 245). Diffusion-weighted images were acquired with a single shot spin echo planar imaging sequence (TR = 9030 msec, TE = 93 msec, flip angle = 90°, FOV = 220 × 220, voxel size = 1.38 × 1.38 × 3.00 mm, 12 diffusion-sensitizing gradients with a b-value of 1000 sec/mm2 and 2 nondiffusion-weighted images (b = 0 sec/mm2). A T2-weighted fluid attenuated inversion recovery (FLAIR) was acquired to quantify white matter hyperintensities (WMHs; TR = 8000 msec, TE = 81 msec, TI = 2500 msec, flip angle = 150°, FOV = 192 × 220, voxel size = 0.69 × 0.69 × 5.20 mm). Susceptibility-weighted imaging was obtained to quantify microbleeds (TR = 27 ms, TE = 20 ms, voxel size = 0.76 × 0.76 × 1.80 mm).
Diffusion tensor analyses
Diffusion-weighted images were processed using TRActs Constrained by UnderLying Anatomy (TRACULA; Supplemental Methods), part of FreeSurfer 6.0 (Yendiki et al., 2011, 2014). This results in a probabilistic distribution of each tract in individual diffusion space (Yendiki et al., 2011) and the extraction of tensor-based measures from the average over the highest probability path (at center) (fractional anisotropy [FA], MD, axial diffusivity [DA], and radial diffusivity [RD]) using a standard least squares model. To reduce the number of decimals, diffusivity metrics were multiplied by 1000.
The major WM pathways include the forceps major, forceps minor, corticospinal tract, inferior longitudinal fasciculus, uncinate fasciculus, anterior thalamic radiation, cingulum–cingulate gyrus bundle, cingulum–angular bundle, superior longitudinal fasciculus–parietal bundle, and superior longitudinal fasciculus–temporal (SLFt) bundle.
Quantification of small vessel disease measures
Areas of WMH were automatically segmented on FLAIR images using a previously described algorithm (Schirmer et al., 2019). In brief, this algorithm relies on a deep learning u-net like architecture based on clinical grade input data to automatically identify and label WMH, while excluding imaging artifacts derived from acute ischemic lesions. All WMH masks were visually inspected and manually corrected. The extracted WMH volume was normalized to total WM
To enable voxel-wise analyses, FLAIR images were coregistered to the TRACULA MNI-template using FSL's (version 5.0.8) FLIRT and FNIRT with cost-function weighting of the lesions to avoid distortions. The resulting warps were applied to the WMH masks. Voxel-wise group differences in WMH were analyzed using a nonparametric permutation-based approach with the threshold-free cluster enhancement method. We used 5000 permutations for statistical inference (two-sample t-test) and applied a corrected FWE threshold of p < 0.05. WMH overlap probabilities per group were calculated starting from at least 20% overlap.
The number and location (deep, lobar, and infratentorial) of microbleeds were manually counted twice by the same trained expert. Count test–retest reliability was excellent (intraclass correlation coefficient = 0.96, p < 0.001). Lacunes of vascular origin were manually identified and segmented on the FLAIR images as ovaloid areas of signal hypointensity twice by an expert rater (intraclass correlation coefficient for volume = 0.92, p < 0.001). Volume of lacunes was quantified and normalized to total brain volume.
Statistical analyses
Statistical analyses were conducted in R version 3.4.2. Demographics are reported using mean and standard deviation and groups were compared using the Welsh two-sample t-test or chi-square.
To limit the number of models, we first identified tracts that differed between both groups, while remaining uninformed about their contribution to cognition. Group differences in diffusivity of all tracts were tested with robust linear regression (covarying for age, gender, and tract volume) using the Huber-M estimator. Robust regression is a more conservative test than least-square regression, as these models are stout against outliers. For tracts showing significant group differences in FA or MD after adjustment for multiple comparisons (false discovery rate [FDR] approach), we examined group differences in the other diffusion metrics, and examined FA of each voxel along the tract.
To obtain a global FA estimate—as control measure— we performed an exploratory factor analyses on the FA of all tracts using the covariance structure of the entire sample, maximum likelihood estimation, and a default oblimin rotation resulting in one factor.
To select specific DTI metrics for the mediation analyses, partial correlations (age adjusted and FDR adjusted for multiple comparisons) were performed between each of the DTI metrics and the two composite scores. In the first set of mediations, carrier status was the independent variable, diffusivity of selected tracts or global FA was the mediator and cognition the outcome. In the second set, diffusivity was mediator and WMH volume the outcome. All analyses were adjusted for age, gender, and education. The mediated (indirect) effect, direct effect, and proportion mediated were estimated with the quasi-Bayesian Monte Carlo method with bootstrap simulation (n = 5000). As the mediation analyses were derived from the stringent robust regressions and correlations, we performed no adjustment for multiple comparisons for the mediation analyses.
Results
We included 20 individuals carrying a CADASIL mutation and 23 noncarrier controls, all asymptomatic as determined by the MMSE and FAST. Groups did not differ in cardiovascular risk factors, microbleed count, or lacunar volume (Table 1).
Characteristics of Both Groups
Median and interquartile range are provided for the continuous data and proportions for dichotomous data. Groups were compared using the Welsh t-test or the chi-square test. * p < 0.001.
FAST scores of 1 and 2 indicate that the subject is cognitively unimpaired.
The fully observed range for lacunes for the CADASIL carriers was 0–5 (one person with two lacunes and one person with five lacunes).
CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; FAST, functional assessment staging; GAI, geriatric anxiety inventory; GDS, geriatric depression scale; WM, white matter; WMH, white matter hyperintensity.
Carriers were younger [t(39.07) = 4.07, p < 0.001], had higher WMH load [t(19.42) = −5.55, p < 0.001; Fig. 2], and performed at trend-level worse on the DSST compared with controls [t(33.51) = −1.98, p = 0.056; Table 2].
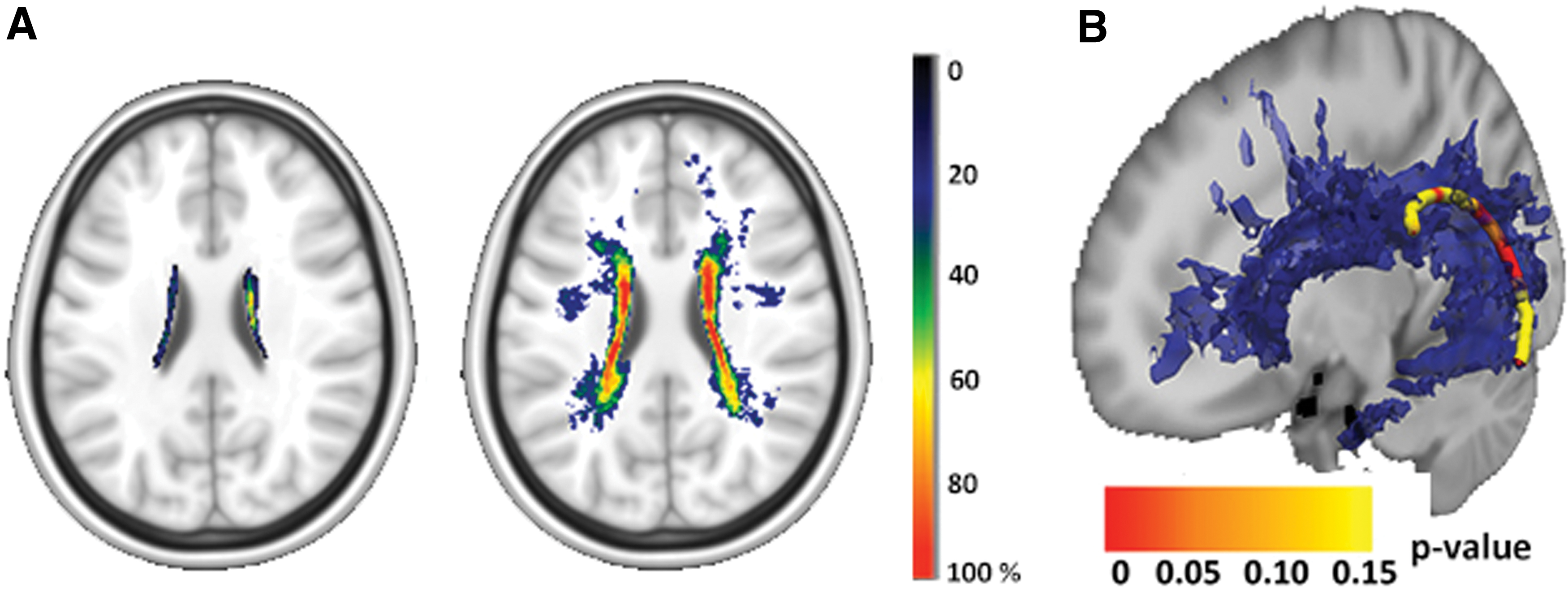
Group differences in WMH and DA of the left SLFt along the tract.
Cognitive Performance of Both Groups
Median and interquartile range are provided. Groups were compared using the Welsh t-test. $ p < 0.06.
CERAD, Consortium to Establish a Registry for Alzheimer's Disease; FAS, F-A-S phonemic fluency test; INECO, Institute of Cognitive Neurology; MCT, memory capacity test; MMSE, mini-mental state examination score; WLT, world learning test.
Of all FA measures, only the left—not the right—SLFt showed higher FA values in controls than carriers after multiple comparison adjustment [β = −0.03, t(38) = −3.38, p = 0.002; Supplementary Table S1]. No group differences were observed for MD of the SLFt [β = −0.07, t(38) = −1.03, p = 0.31; Fig. 1]. We then examined the other diffusion metrics of the SLFt and observed group differences in DA and RD [β = −0.04, t(38) = −2.65, p = 0.011; β = 0.02, t(38) = 3.15, p = 0.003]. No group differences were observed for global FA [β = −0.07, t(38) = −0.59, p = 0.56]. These results did not change when restricting the inclusion range to MMSE >25 (one CADASIL carrier scored <25) and/or when removing the consistent outlier across the diffusivity metrics (Supplementary Tables S2 and S3).
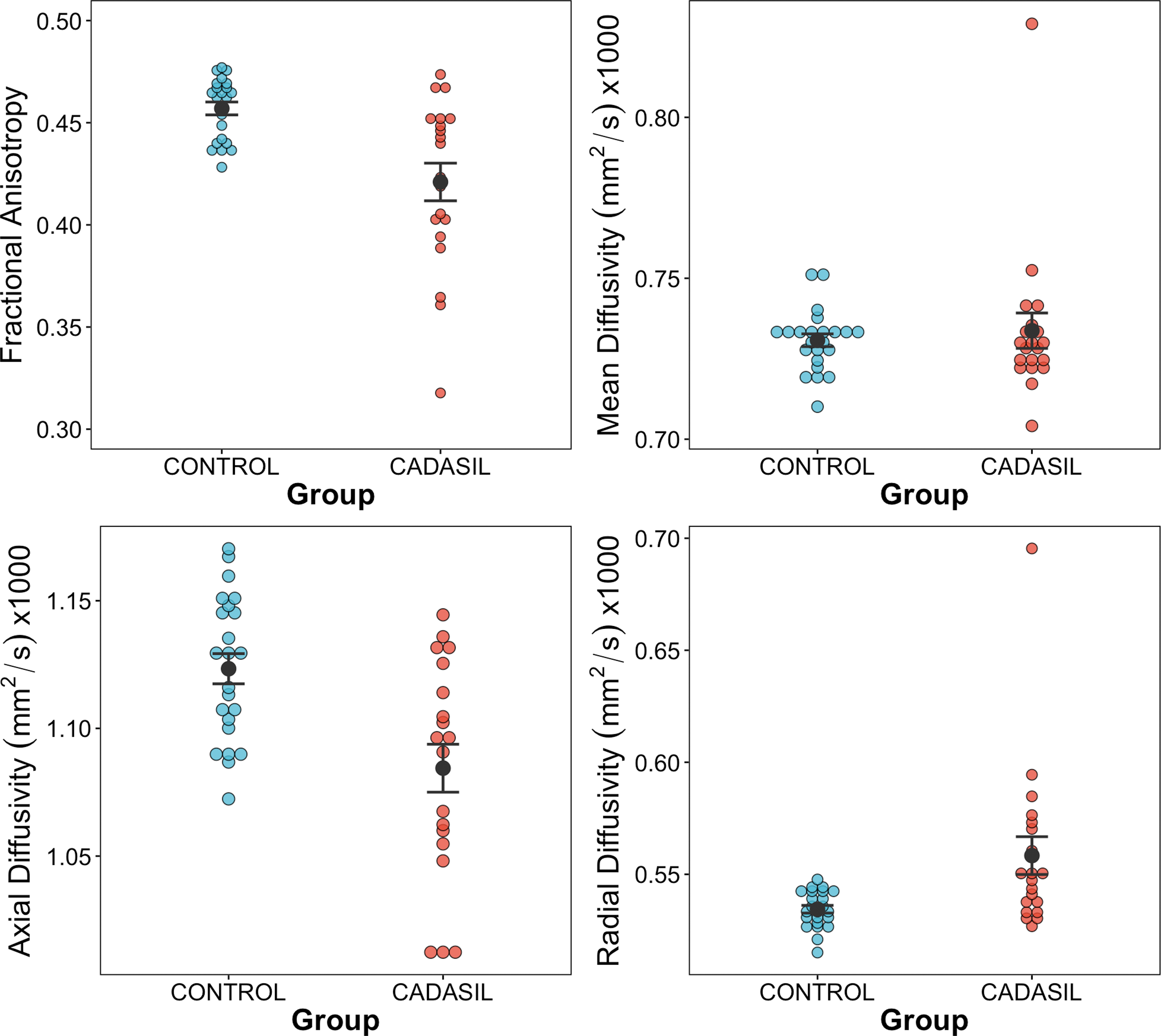
Group differences in diffusivity of the SLFt. Left: Group differences between controls and CADASIL patients in FA, MD, DA, and RD in the left SLFt. CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; DA, axial diffusivity; FA, fractional anisotropy; MD, mean diffusivity; RD, radial diffusivity; SLFt, superior longitudinal temporal fasciculus. Color images are available online.
Group differences in each voxel across the length of the left SLFt are predominantly localized in the middle, which overlaps with the location where carriers exhibited greater WMH than controls (Fig. 2B; FWE p < 0.05).
Diffusivity abnormalities and lesion load as mechanisms underlying CADASIL-related cognitive deficits
Scores on the executive composite correlated with the FA and DA of the left SLFt. The memory composite scores correlated with FA of the left SLFt (Table 3, FDR corrected). WMH load correlated with the DA metric of the left SLFt.
Partial Correlations Between Cognition, White Matter Hyperintensity, and Diffusion Metrics of the Left Superior Longitudinal Temporal Fasciculus and Global Fractional Anisotropy Across Both Groups
Partial Pearson correlation coefficients (adjusted for age) and their p-value between parentheses. Bold numbers are significant at alpha <0.05; *correlation was significant after multiple comparison correction using the FDR approach.
DA, axial diffusivity; FA, fractional anisotropy; MD, mean diffusivity; SLFt, superior longitudinal temporal fasciculus; RD, radial diffusivity.
The left SLFt FA did not mediate the relationship between carrier status and memory (mediation effect: β = −0.23, p = 0.304, 95% CI [−0.69 to 0.11]). However, there was a significant mediation between group and executive performance (mediation effect: β = −0.38, p = 0.002, 95% CI [−0.76 to −0.09], proportion mediated: β = 0.58, p = 0.016, 95% CI [0.12–1.69]). When adding WMH as covariate, mediation by the left SLFt FA on the association between group and executive performance remained significant (mediation: β = −0.38, p = 0.048, 95% CI [−0.87 to −0.01]).
Similar effects were observed for the left SLFt DA, which mediated the relationship between carrier status and executive performance (mediation effect: β = −0.31, p = 0.014, 95% CI [−0.65 to −0.05], proportion mediated: β = 0.48, p = 0.028, 95% CI [0.07–1.65]; Fig. 3A). No mediation was observed for the memory composite scores [mediation: β = −0.13, p = 0.56, 95%CI [−0.59 to 0.17]). Adding WMH as covariate removed the mediation by the left SLFt DA on the association between group and executive performance (mediation: β = −0.10, p = 0.28, 95% CI [−0.41 to 0.05]).
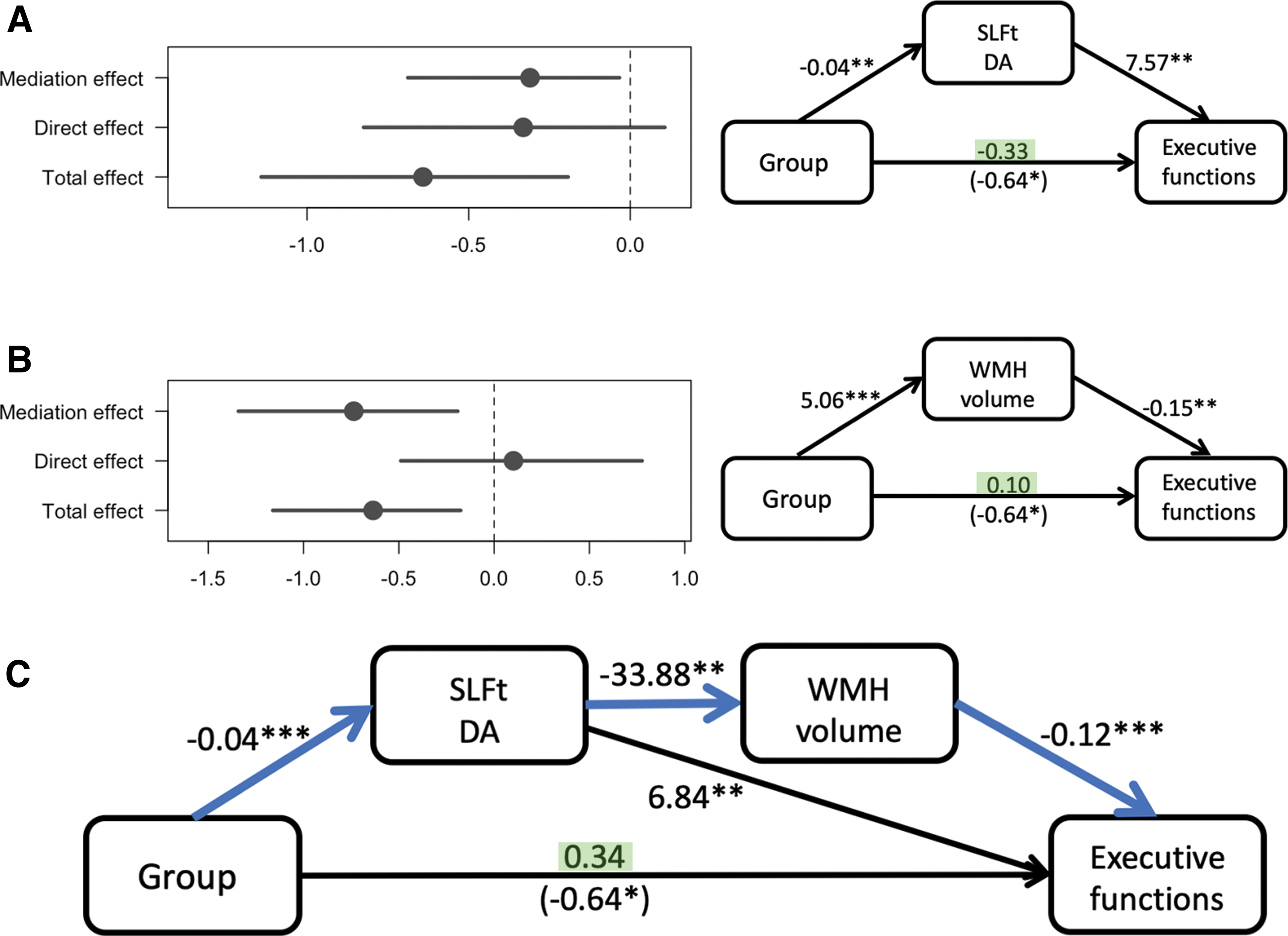
Sequential mediation by the left SLFt and WMH of the relationship between carrier status and executive composite scores.
None of the diffusivity metrics of the left SLFt mediated the relationship between group and WMH (mediation FA: β = 0.04, p = 0.94, 95% CI [−0.88 to 1.21]; mediation DA: β = 0.64, p = 0.11, 95% CI [−0.10 to 1.66]). However, WMH mediated the relationship between group and executive scores (mediation: β = −0.74, p = 0.012, 95%CI [−1.33 to −0.20], proportion mediated: β = 1.16, p = 0.018, 95% CI [0.26–3.72]; Fig. 3B), even when additionally covarying for the left SLFt FA (mediation: β = −0.73, p = 0.004, 95% CI [−1.22 to −0.23]) or DA (mediation: β = −0.52, p = 0.034, 95%CI [−1.07 to −0.05]). WMH volume did not mediate the relationship between group and memory (mediation: β = 0.41, p = 0.17, 95%CI [−0.17 to 1.18]).
As these results suggest a sequential mediation, we post hoc carried out a double mediation model in which the relationship between group and executive performance would be mediated sequentially by the left SLFt and WMH volume. The double mediation effect was significant for DA (β = −0.15, p = 0.039, 95%CI [−0.30 to −0.01]; Fig. 3C), but not for FA (β = −0.14, p = 0.075, 95%CI [−0.29 to 0.01]).
Discussion
We aimed to examine the anatomy and potential sequence of WM microstructural and macrostructural abnormalities that would underlie subtle cognitive deficits in asymptomatic CADASIL participants. Even though CADASIL mutation carriers did not differ from noncarriers on cognitive measures, specific WM microstructural differences were detected in the left SLFt. No group differences were observed with a more global measure. These specific microstructural differences were associated with higher WMH load and, in turn, mediated successively subtle executive deficits in CADASIL mutation carriers. Thus, the SLFt may be a critical nexus, carrying unique information linking NOTCH-3 mutations to small vessel disease and providing information on cognitive progression. Such a model is consistent with the established biological cascade underlying CADASIL (Chabriat et al., 2020), but can also be extended to more common diseases, such as sporadic forms of subcortical vascular disease.
The SLFt as a critical WM hub in asymptomatic CADASIL has so far only been reported in symptomatic patients (Mascalchi et al., 2017). The SLFt fibers run from the posterior superior temporal gyrus to superior parietal lobule and angular gyrus WM. The SLFt is adjacent to the arcuate fasciculus and ascends into other parts of the SLF that both run into the prefrontal cortex (Kamali et al., 2014). As such, the SLFt connects several distal brain regions and, as we showed, traverses regions of evolving WMH burden. This makes sense, as anatomically, there is a higher probability that anterior–posterior association fibers cross through WMH regions compared with callosal or projection fibers.
The biological processes underlying this affected tract remain unclear. Diffusion metrics may signal various biological processes that may not primarily be driven by ischemia, but, for example, by hypoperfusion or microcirculation failure (Muta et al., 2015). Even though caution is warranted when conferring biological interpretations, the combination of greater RD, lower FA, and DA may suggest presence of local fiber loss associated with glial infiltration that can lead to diaschisis and downstream changes (Madden et al., 2012). Consistent with our observations, Tatsch and colleagues (2003) observed marked asymmetry in glucose metabolism in CADASIL patients. Interestingly, these hypometabolic patterns were distal from T2 lesions, suggesting reduced blood flow or neuronal loss due to ischemia, or functional deactivation related to remote disconnection (Tatsch et al., 2003). Our associations are less likely to be confounded by atrophy, as all analyses were adjusted for tract volume.
Our sequential mediation suggested a chain of events from worse SLFt diffusivity to greater WMH burden and finally subtle executive deficits in CADASIL. The clinical phenotype captured in this model may be specific to early stages of the disease. Although the asymptomatic phase of CADASIL is heterogeneous, cognitive deficits are dominated by subtle executive impairments that can be detected with neuropsychological testing and also previously correlated with DTI measures (O'Sullivan et al., 2004). Executive functions comprise many cognitive functions and, hence, large-scale networks consisting of frontal and parietal regions connected by long association fibers, including the SLF, are believed to support the multifaceted nature of executive functions (Dixon et al., 2018). This multifaceted nature of executive functions can also include contributions of language expression and comprehension, given that many of the tests in our composite are verbal in nature or can involve verbalization strategies, and the SLFt, in particular the left side, plays an important role in language (Kamali et al., 2014). As patients age, cognitive impairments include attention and memory retrieval (Buffon et al., 2006). Thus, our results suggest that SLFt disruption reflects an early indicator of executive dysfunction in CADASIL.
Our findings have important implications. A diagnosis can be made by genetic testing, however, given that prognosis may depend upon the specific mutation, markers of disease monitoring are needed. Because of the greater sensitivity of SLFt diffusivity, its topographical relationships with WMH, and correlations to early subtle executive deficits, focusing on this specific tract may hold promise as an early indicator of increasing disease severity, where therapeutic interventions are more likely to attenuate hypertension and prevent stroke or delay cognitive decline.
Whether these findings are applicable to all CADASIL mutations warrants further investigation. It has been estimated that there are 500 families with CADASIL worldwide, representing >200 different mutations (Rutten et al., 2016), and individual differences in cognitive profiles exist across different mutations. Genotype–phenotype correlations revealed that patients with the Colombian C455R mutation have an earlier age of onset of strokes but slower and less aggressive cognitive decline compared with the R1031C mutation (Arboleda-Velasquez et al., 2002). The R141C mutation is rare (Coupland et al., 2018; Peters et al., 2005), but these individuals may have greater executive deficits than other mutations (Zuluaga-Castaño et al., 2018).
There are limitations. First, no causal inferences can be drawn given the cross-sectional nature of our data. Nonetheless, our mediation analyses provide a biologically plausible model that can be tested in large-scale longitudinal studies. Such studies will also have the opportunity to investigate spatiotemporal relationships between changes in WMH versus changes in diffusivity in tracts. Second, correction for age may be too stringent as age is the main risk factor for disease progression (Holtmannspotter et al., 2005; Mascalchi et al., 2017; O'Sullivan et al., 2004). In our models, age did not contribute to the explained variance, but gender often did. For consistency and to adjust for the age difference between both groups, we adjusted all models for both age and gender. Although the available evidence suggests that CADASIL affects men and women equally, we were unable to evaluate gender-specific phenotype differences (Gunda et al., 2012) as the majority of our participants were women. Third, despite the relatively small sample size, our results remained robust when using more conservative statistical methods, such as robust regression and bootstrapping, and when further restricting the sample to carriers with MMSE scores >25. Finally, the voxel size of our DTI images was not isotropic, as imaging was part of a clinical protocol. Thus, any tractography tool will be forced to interpolate voxels, making it harder to find smaller tracts or deal with crossing fibers. Therefore, we used probabilistic tractography in which FLIRT resampling was applied to approach isotropic voxels, and we focused on 10 larger tracts from which we extracted the tensor-based measures at the highest probability of the tract.
Conclusions
We identified the left SLFt as a critical WM fiber bundle, of which worse diffusivity can link presence of CADASIL mutations to greater severity of small vessel disease and worse executive functioning in asymptomatic stages of the disease.
Footnotes
Authors' Contributions
Conception or design of the study was carried out by H.I.L.J. and Y.T.Q.; data acquisition was done by H.T.-T., Y.Z., L.V.-J., C.O.-V., and F.L.; data analyses were carried out by H.I.L.J., D.S., and H.T.-T.; interpretation of the data was by H.I.L.J., F.L., J.F.A.-V., and Y.T.Q.; drafting the study was done by H.I.L.J., D.S., and Y.T.Q.; revising it critically and final approval were done by H.I.L.J., D.S., H.T.-T., Y.Z., L.V.-J., C.O.-V., F.L., J.F.A.-V., and Y.T.Q.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. Jacobs was supported by funding from the European Union's Horizon 2020 Research and Innovation Program under the Marie Sklodowska-Curie Grant agreement [IF-2015-GF, 706714]. Dr. Lopera was supported by COLCIENCIAS-Colombia. Dr. Arboleda-Velasquez received funding from the U.S. National Institute on Aging and the U.S. National Institute of Neurological Disorders and Stroke (3RF1NS110048-01S1). Dr. Quiroz received funding from the National Institutes of Health (RO1AG054671, DP5OD019833) and Massachusetts General Hospital ECOR. These funding sources had no role in study design, data collection, and interpretation, or the decision to submit the study for publication.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.