
Abstract
Background/Introduction:
Transcranial direct current stimulation (tDCS) delivered over the dorsolateral prefrontal cortex (DLPFC) while patients are at rest can decrease craving in patients with substance-related and addictive disorders. Yet, the effects of tDCS on resting-state brain activity remain unknown in this population. This study examined the effects of tDCS on resting-state functional connectivity (rsFC) with concurrent stimulation and functional magnetic resonance imaging in patients with gambling disorder.
Methods:
This was a randomized, sham-controlled, double-blind, crossover study. The anodal and cathodal electrodes were applied over the right and left DLPFC, respectively. Patients received 30 min of active and sham stimulation on separate days. rsFC was assessed before and during stimulation with seed-based analyses.
Results:
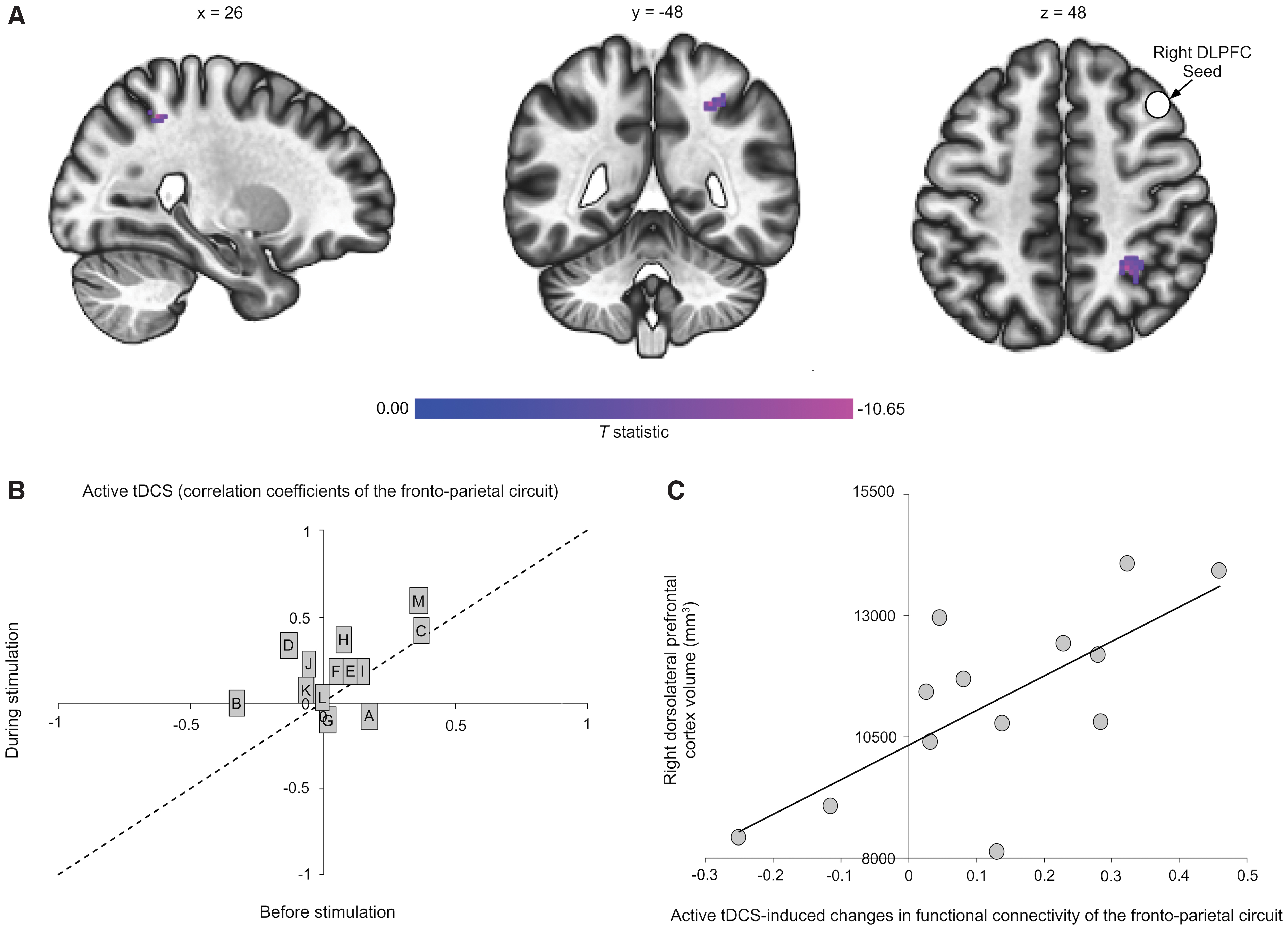
There was a significant increase of rsFC between the right DLPFC seed and the right superior parietal lobule during active stimulation as compared to during sham stimulation (p = 0.0059, corrected for multiple comparisons). There was also a positive correlation between rsFC change of this frontoparietal network and brain volume of the right DLPFC (p = 0.0042, corrected for multiple comparisons).
Discussion:
A single session of tDCS targeting the DLPFC strengthened functional connectivity in a frontoparietal circuit, known to be implicated in cognitive control, especially in patients with a greater volume of the region under the anode electrode.
Impact statement
Transcranial direct current stimulation increased the functional connectivity of a frontoparietal circuit in patients with gambling disorder. These changes were larger in patients with greater volume of the dorsolateral prefrontal cortex. Transcranial direct current stimulation strengthened the connectivity of a brain network known to be associated with cognitive control.
Introduction
Gambling disorder is a psychiatric disorder characterised by problematic gambling behavior leading to important impairment (Potenza et al., 2019). Craving is central to gambling disorder pathophysiology (Spagnolo et al., 2018) and strongly predicts relapse (Smith et al., 2015). Existing treatments do not effectively treat craving (Potenza et al., 2019). For example, only 23% of patients remain abstinent after 12 months of cognitive behavioral therapy (Hodgins et al., 2007), which is considered to be among the most effective treatments (Potenza et al., 2019). Other therapeutic strategies are needed to target craving.
Transcranial direct current stimulation (tDCS) applied over the dorsolateral prefrontal cortex (DLPFC) can decrease craving levels in patients with substance-related and addictive disorders (Jansen et al., 2013). tDCS holds the potential to reduce gambling craving as well (Hone-Blanchet et al., 2015). For instance, tDCS applied over the DLPFC decreased craving in one patient with gambling disorder (Martinotti et al., 2018) and in patients with substance-related and addictive disorders and gambling disorder (mainly polyusers) (Martinotti et al., 2019). Most of these studies applied tDCS while patients were at rest. However, it seems that no studies investigated tDCS-induced effects on resting-state functional connectivity (rsFC) during stimulation in gambling disorder. Thus, our goal was to identify the impact of tDCS applied over the DLPFC on rsFC during stimulation with concurrent tDCS and rsFC in patients with gambling disorder. We previously characterized tDCS-induced changes on rsFC in healthy individuals with concurrent tDCS and functional magnetic resonance imaging (fMRI). We found that tDCS over the DLPFC increased rsFC of a frontoparietal circuit (Mondino et al., 2020). It has also been shown that patients with gambling disorder display abnormally weak rsFC between the DLPFC seed and parietal cortex (Bae et al., 2017). Based on these studies, we hypothesized that tDCS will increase rsFC of a frontoparietal circuit. In addition, we previously observed positive correlations between tDCS-induced elevations of prefrontal gamma aminobutyric acid levels and volume and thickness of the DLPFC in patients with gambling disorder (Bouchard et al., 2020). Thus, our second goal was to examine whether brain morphometry influences tDCS-induced changes of rsFC strength. We predicted positive correlations between tDCS-increased rsFC of a frontoparietal network and volume and thickness of the DLPFC.
Materials and Methods
Design
This was a randomized, crossover, sham-controlled, double-blind study. Patients underwent two concurrent tDCS/fMRI sessions (active and sham tDCS), separated by 7 days. They were randomized with a 1:1 ratio (active or sham). We administered a standardized tDCS side effect form at each session. We assessed blinding integrity in patients and outcome assessors with a standardized form after each session.
Participants
We recruited 18 patients who met DSM-5 criteria for gambling disorder and were eligible to receive tDCS (Keel et al., 2001) and MRI. Thirteen participants (5 women; mean age ± SD: 37.4 ± 16.7 years; mean years of education: 13.0 ± 1.4 years; 5 left-handed as assessed by the Edinburgh Handedness Inventory) (Oldfield, 1971) were included in the analyses. They were free of substance-related and addictive disorders, except for tobacco use disorders, in the past year. Seven patients were taking medications, mainly for depression, and were stable on their medications for at least 3 months before their participation. We recruited patients at the Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale and obtained their written informed consent before their participation. This study received ethical approval (#374) from the Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale.
Intervention
tDCS was delivered with an MR-compatible battery-driven stimulator (NeuroConn GmbH, Germany) that was placed in the operator room and connected to two 7 × 5 cm2 rubber electrodes through an isolated optical cable with a filtering system. The question of whether tDCS should target the right and/or the left DLPFC remains open (e.g., Pettorruso et al., 2021). We chose to place the anode and cathode electrodes over the right and left DLPFC, respectively, using the international electroencephalography 10–20 system (F4, F3). The goal of this article was to identify the effects of tDCS on rsFC in gambling disorder, using the tDCS montage that seems to improve decision-making skills relevant for addictive behaviors (e.g., strengthening cognitive control and/or reducing risk taking and reward seeking; Fecteau et al., 2007; also supported by more recent work: Martinotti et al., 2018, 2019; Soyata et al., 2019). Active stimulation was delivered for 30 min at a current intensity of 1 mA (this device does not stimulate above 1 mA) with ramp-up and ramp-down periods of 30 sec. Sham stimulation was delivered for 30 min with no active current between the 30-sec ramp-up and ramp-down periods (Gandiga et al., 2006). We first acquired a 6-min T1 and a 5-min fMRI scan. We then started stimulation and acquired an fMRI scan during the last 5 min of the 30-min stimulation period. Patients were instructed to rest and keep their eyes open during scanning.
Measures
Morphometry assessment
We used CBrain (Sherif et al., 2014) to perform FreeSurfer's recon-all pipeline with default parameters (version 6.0.0). We labeled the DLPFC using the Desikan–Killiany–Tourville protocol (Klein and Tourville, 2012), where the DLPFC corresponded to the rostral middle frontal gyrus.
fMRI data acquisition
Whole-brain MRI scan acquisitions were performed with a Philips 3T Achieva scanner (Philips Healthcare, The Netherlands; standard 8-channel head coil). T1-weighted structural magnetic images were acquired with a magnetization-prepared rapid acquisition gradient-echo sequence repetition time (TR) = 8.2 ms, echo time (TE) = 3.7 ms, field of view (FoV) = 250 mm, flip angle = 8°, 256 × 256 matrix, 180 slices/volume, slice thickness = 1 mm, no gap. For the rsFC scans, EPI blood oxygen level dependent (BOLD) images were acquired with the following parameters: TR = 3000 ms, TE = 30 ms, FoV = 224 × 224 × 140 mm, flip angle = 70°, 64 × 64 matrix, dynamic scans 100, voxel size = 3.5 × 3.5 × 3.5 mm, slice thickness = 3.5 mm, no gap.
Analyses
fMRI preprocessing
We preprocessed structural and functional volumes using SPM 12 through CONN version 19.c (Whitfield-Gabrieli and Nieto-Castanon, 2012). Both CONN and SPM ran on MATLAB R2019a (Mathworks, Inc.). We used the Harvard–Oxford Atlas (Desikan et al., 2006) to label the cortical and subcortical areas and the AAL atlas to label the cerebellum (Tzourio-Mazoyer et al., 2002), as implemented in CONN. We performed CONN's default preprocessing pipeline with a functional smoothing of 7 mm full-width-at-half Gaussian kernel. We used CONN's default tissue probability maps and Artifact Detection tools to identify outliers. We used intermediate settings (97th percentile in normative sample) and defined functional outliers using a global signal z-value threshold of 5 and a subject-motion mm threshold of 0.9 mm. Patients with >15% outlier scans were rejected. From the 18 recruited patients, 17 completed the study as one dropped out at the first session because of MRI-related discomfort. Due to technical problems with the stimulation cables in the magnetic field, two patients were excluded. Two other patients were excluded due to MRI artifacts.
From the 18 recruited participants, 13 participants were entered into the analyses (effect size dz = 0.85, α = 0.05, and power = 80%, two-tailed paired-samples t-test using G*Power (Faul et al., 2007).
We used CONN's quality analysis reports to verify preprocessing steps. We performed denoising, using a component-based noise regression method to regress out physiological sources of noise (signals from white matter and cerebrospinal fluid, 20 confound dimensions including their first-order derivatives) (Behzadi et al., 2007). Furthermore, we regressed out movement-related covariates (scrubbing and realignment [with its first-order derivatives]) and session effects (before, during active and sham stimulation, each with their first-order derivatives). Lastly, we applied band pass filtering of 0.008–0.09 Hz (Hallquist et al., 2013) and linear detrending. We used CONN's quality analysis plots to verify denoising steps. Furthermore, we used Afni (
Seed-based functional connectivity
We performed seed-based functional connectivity analyses with the right and left DLPFC as seeds (± x = 36 y = 29 z = 38, with 5 mm radii) using CONN. Seed-based correlation analysis is defined as the Fisher-transformed bivariate correlation coefficients between the seed BOLD time series and an individual voxel BOLD time series (Lv et al., 2018) from the entire brain. We used a 2 × 2 (Stimulation × Time) repeated-measures analysis of variance (ANOVA) to examine whether there were significant tDCS-induced effects on rsFC. We used a voxel threshold of p-uncorrected <0.001 and cluster threshold cluster size p-false discovery rate (FDR) corrected <0.05 (Friston et al., 1994). If results were significant, we used REX to compute average connectivity values within our clusters from CONN's graphic user interface. Correlations were bootstrapped 1000 times using a 95% confidence interval to verify robustness and were controlled for age. If appropriate, we used the Bonferroni test to correct for multiple comparisons of the correlations with an α threshold of p = 0.05/4 for the morphometric measures (right DLPFC thickness, volume, left DLPFC thickness, volume = 0.0125). Post hoc and correlation analyses were performed using SPSS, version 26 (IBM Corp.).
Results
Effects of tDCS on rsFC
We first tested whether there were differences on rsFC between sham and active stimulation conditions at baseline. There were no differences between conditions for both seeds (right DLPFC, p-FDR >0.22; left DLPFC, p-FDR >0.26).
Seed-based functional connectivity analyses revealed a significant stimulation × time interaction on rsFC between the right DLPFC seed (under the anode electrode) and a cluster that encompassed the right superior parietal lobule (Fig. 1A, B and Table 1). Post hoc t-tests indicated that active compared with sham tDCS increased rsFC of this frontoparietal network during stimulation. In addition, rsFC increased from before to during active stimulation and decreased from baseline to during sham stimulation. Lastly, there was no significant Stimulation × Time interaction on rsFC using the left DLPFC seed (under the cathode electrode).
Significant Effect of Transcranial Direct Current Stimulation on Resting-State Functional Connectivity and Post hoc Comparisons
ANOVA, analysis of variance; DLPFC, dorsolateral prefrontal cortex; FDR, false discovery rate; L, left; MNI, Montreal Neurological Institute; R, right; SPL, superior parietal lobule.
Correlation between tDCS-induced changes on rsFC and brain morphometry
There was a positive correlation between active tDCS-induced changes in rsFC of the frontoparietal network and volume of the right DLPFC (r = 0.813, p = 0.0042; Fig. 1C). There were no correlations that survived Bonferroni corrections between rsFC for active and sham tDCS and the other brain morphometric measures (active: right DLPFC thickness [p = 0.15]; left DLPFC volume [p = 0.20] and thickness [p = 0.38]; sham: right DLPFC volume [p = 0.043] and thickness [p = 0.35]; left DLPFC volume [p = 0.58] and thickness [p = 0.74]).
Side effects and integrity of blinding
There were no significant differences in the number of reported side effects from the participants between active and sham tDCS (p = 0.35; Supplementary Table S1). Eight out of 13 patients guessed correctly whether they received active or sham tDCS with a confidence level of 80% as determined on a visual analog scale. The outcome assessors had minimal interaction with the patients and remained blinded to the stimulation conditions with a confidence level of 100%.
Discussion
Our findings indicate that active compared with sham tDCS increased rsFC of a frontoparietal network. This circuit encompassed the right DLPFC seed (under the anode electrode) and the right superior parietal lobule. This is in line with previous results in healthy individuals showing rsFC strengthening of this network during and after tDCS (Mondino et al., 2020). Increasing rsFC of the frontoparietal network may be clinically relevant in gambling disorder. The frontoparietal circuit has been reported to be altered in gambling disorder (Bae et al., 2017), as well as in internet gaming disorder (Yuan et al., 2016) and substance-related and addictive disorders (Sutherland et al., 2012). Specifically, patients with gambling disorder displayed weaker rsFC between a left DLPFC seed and the left postcentral gyrus compared with healthy individuals (Bae et al., 2017). Furthermore, the frontoparietal network is implicated in cognitive control (Seeley et al., 2007), which may suppress craving (Verdejo-Garcia et al., 2019). For instance, 10 tDCS sessions over both DLPFCs improved cognitive control, which correlated with reduced craving in patients with methamphetamine use disorder (Alizadehgoradel et al., 2020).
Results from this work also suggest that a larger right DLPFC volume correlated with greater strengthening of the frontoparietal rsFC induced by tDCS. A voluminous DLPFC might contain more pyramidal neurons that respond more to tDCS. Indeed, pyramidal neurons respond better to direct current (Radman et al., 2009) and more neurons are seen in a more voluminous structure (de Sousa and Proulx, 2014), as shown in animal studies. Brain volume might thus be a useful predictor of tDCS-induced changes in rsFC and neurotransmitter levels (Bouchard et al., 2020). This also indicates that tDCS parameters may be tailored to a patient's brain morphometry, especially for the regions under the electrodes, to achieve the optimal dosage to modulate brain activity.
Moreover, as seen in this study (Mondino et al., 2020), there was a decrease in rsFC of the frontoparietal network for the sham tDCS condition. This decrease may reflect a time-related variation in the intrinsic BOLD signal occurring while subjects are at rest for more than half an hour in the MRI scanner. An fMRI study reported time-varying functional connectivity in the right frontoparietal network (Gonzalez-Castillo et al., 2014). Also, a resting-state fMRI/EEG study found diminished BOLD signal in the frontotemporal network with increased alpha activity (Goldman et al., 2002), and a resting-state PET/EEG study observed decreased blood flow in the left dorsomedial PFC and augmented alpha activity (Sadato et al., 1998). Our findings might thus indicate that DLPFC activity reduces and decorrelates from the other structures such as the parietal regions during the sham tDCS condition, whereas active tDCS interrupts this. Finally, there was no significant difference in the left frontoparietal network. One possible explanation that warrants further investigation is that greater rsFC changes are observed with frontal seeds ipsilateral to the anode electrode, as previously observed (Mondino et al., 2020; Shahbabaie et al., 2018; Yang et al., 2017), or in networks ipsilateral to the anode electrode (Holla et al., 2020).
Some limitations of this study should be addressed. Our sample was relatively small; yet, we used strict processing measures to control for type 1 error to provide adequate power analysis for needed replication studies. Also, about half of the patients took medications. Although this reflects the gambling disorder (GD) population (Potenza et al., 2019), we cannot rule out the potential influence of medications on tDCS-induced effects on rsFC. Furthermore, although our functional seeds and anatomical areas of the DLPFC overlapped, the use of identical anatomical and functional areas in future work may further strengthen the association between rsFC and DLPFC volume.
Conclusions
Altogether, modulation of frontoparietal rsFC with tDCS may be clinically relevant for gambling disorder, especially for patients with greater DLPFC volume. The next step in terms of developing an effective tDCS intervention for gambling disorder implies the delivery of repeated tDCS sessions to induce lasting clinical benefits. As this frontoparietal circuit is known to be associated with cognitive control, such increased rsFC may translate to improved cognitive functioning that may help patients resist gambling.
Footnotes
Acknowledgments
We thank the participants for their interest in this project. We also thank Dr. Alfonso Nieto-Castañón for his help with CONN.
Authors' Contributions
S.F. and F.F. designed the study. M.D. and F.F. recruited the patients. M.D., C.L., and S.F. collected data. A.E.B. led the data analysis with the participation of M.D. and E.R. A.E.B. led the interpretation of results with the participation of M.D. A.E.B. and M.D. drafted the article. All authors critically reviewed the article and approved the finalized article.
Data Statement
Data are available upon request to the corresponding author.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Parkinson Society Canada grant (FO103232) to S.F. A.E.B. was supported by a Canadian Institutes of Health Research Frederick Banting and Charles Best Doctoral award. M.D. was supported by a Fonds de Recherche du Québec-Santé Doctoral award. S.F. was supported by the Canada Research Chair in Cognitive Neuroplasticity.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.