
Abstract
Introduction:
Cognitive impairment in multiple sclerosis (MS) is increasingly being investigated with resting-state functional MRI (rs-fMRI) functional connectivity (FC). However, results remain difficult to interpret, showing both high and low FC associated with cognitive impairment. We conducted a systematic review of rs-fMRI studies in MS to understand whether the direction of FC change relates to cognitive dysfunction, and how this may be influenced by the choice of methodology.
Methods:
Embase, Medline, and PsycINFO were searched for studies assessing cognitive function and rs-fMRI FC in adults with MS.
Results:
Fifty-seven studies were included in a narrative synthesis. Of these, 50 found an association between cognitive impairment and FC abnormalities. Worse cognition was linked to high FC in 18 studies, and to low FC in 17 studies. Nine studies found patterns of both high and low FC related to poor cognitive performance, in different regions or for different magnetic resonance (MR) metrics. There was no clear link to increased FC during the early stages of MS and reduced FC in later stages, as predicted by common models of MS pathology. Throughout, we found substantial heterogeneity in study methodology, and carefully consider how this may impact on the observed findings.
Discussion:
These results indicate an urgent need for greater standardization in the field—in terms of the choice of MRI analysis and the definition of cognitive impairment. This will allow us to use rs-fMRI FC as a biomarker in future clinical studies, and as a tool to understand mechanisms underpinning cognitive symptoms in MS.
Impact statement
We present the first systematic review of resting-state functional MRI functional connectivity (FC) studies to investigate cognitive impairment in multiple sclerosis (MS). We assess whether this magnetic resonance (MR) metric is a suitable biomarker of cognitive decline in MS. We demonstrate that while there is a strong link between FC abnormalities and cognitive impairment, the direction of abnormalities varies considerably across studies. We also demonstrate that there is substantial methodological heterogeneity across studies, which makes results difficult to interpret. From this, we highlight the urgent need for more standardization in FC studies in MS, and offer potential ways forward to achieve this.
Introduction
Multiple sclerosis (MS) is a chronic immune-mediated disorder of the central nervous system that predominantly affects young adults (Dobson and Giovannoni, 2019; Filippi et al., 2018; Thompson et al., 2018). Inflammatory demyelination is pathognomonic with neurodegeneration insidiously dominating over time (Lassmann, 2018).
Cognitive impairment is common in all MS phenotypes (Charcot, 1888; Benedict, 2020; Benedict et al., 2020) with an estimated prevalence of 43–70% dependent on factors, including phenotype and the cognitive diagnostic criteria used (Fischer et al., 2014; Sumowski et al., 2018). Cognitive impairment is associated with several adverse outcomes, including a higher risk of depression, unemployment, and reduced quality of life (Ruet et al., 2013c; Strober et al., 2014; Sumowski et al., 2018). A more progressive MS phenotype and longer disease duration have been shown to be associated with greater cognitive impairment (Baird et al., 2019; Connick et al., 2013; Johnen et al., 2017, 2019; Patti et al., 2010).
There are currently no licensed treatments for cognitive symptoms in MS, however, exercise (Motl and Sandroff, 2020) and behavioral therapy show promise (Sandroff and DeLuca, 2020). Disease modifying therapies show positive outcomes on cognitive dysfunction in MS, despite no routine evaluation in phase 3 clinical trials currently. However, effects are small and at present understudied, and there are to date no approved pharmaceutical treatments for cognitive symptoms (Benedict et al., 2020; Landmeyer et al., 2020).
Gaining an understanding of the underlying pathophysiology of cognitive dysfunction is essential for diagnosing, monitoring, and developing treatments for this debilitating aspect of MS. The “clinico-radiological” paradox highlights the mismatch of MS cognitive symptoms and conventional MRI measures, such as lesion volumes (Rocca et al., 2015). It is widely accepted that cognitive function is supported by a complex network of structurally interconnected brain regions supporting a highly dynamic functional network, which is researched with advanced MRI tools such as resting-state functional MRI (rs-fMRI), in MS and other neurodegenerative diseases (Batlle et al., 2017; Castellazzi et al., 2014; Mori et al., 2011; Rocca et al., 2015; Schoonheim et al., 2015b).
The main measure derived from rs-fMRI is the functional connectivity (FC) metric. It is a measure of the statistical correlation of blood-oxygenation-level-dependent (BOLD) signal time course between any selection of voxels. The underlying assumption is that voxels with similar BOLD time courses are connected in the performance of a function (Bijsterbosch et al., 2017) (Fig. 1). FC has the potential to be an imaging biomarker of cognitive performance in neurodegenerative disease (Hohenfeld et al., 2018) and is the subject of a growing research field in MS (Benedict et al., 2020). Such a marker could offer a fast, noninvasive way to detect imminent cognitive decline, which is often underdiagnosed on routine neurological examinations (Romero et al., 2015).

Schematic of FC and a functional network. FC is a measure of the statistical correlation of BOLD signal timecourses
For a measure to be suitable as a clinical biomarker, it needs to be able to identify those with cognitive dysfunction from those without it, and to show acceptable repeatability and reproducibility across studies. In some diseases, such as Alzheimer's disease, the rs-fMRI literature shows consistently low FC in the default mode network (DMN) (Badhwar et al., 2017), yet a recent review of rs-fMRI studies in several neurodegenerative diseases, including Alzheimer's, argued that the evidence is not yet strong enough for rs-fMRI FC measures to be suitable biomarkers (Hohenfeld et al., 2018). This review cited a lack of standardized protocols as a challenge in the field.
The rs-fMRI FC literature on cognition in MS has not yet been subject to systematic review, and so, the specificity and reliability of FC as a marker of cognitive dysfunction have not been established. Correlations between FC metrics and cognition have been frequently reported (Hawellek et al., 2011; Lin et al., 2020; Schoonheim et al., 2012; Tona et al., 2014), but in studies comparing FC between cognitively impaired (CI) and cognitively preserved (CP) patients, results have shown both high and low FC linked with worse cognitive function (Basile et al., 2014; Bonavita et al., 2011; Cruz-Gómez et al., 2014; Faivre et al., 2012; Rocca et al., 2018).
A common interpretation of increases in any type of brain function is that of functional “reorganization”: a compensatory mechanism that enables the functioning of networks in the presence of structural damage, hence delaying clinical progression. This compensatory mechanism is thought to be sustainable only up to a critical point, at which the structural damage becomes too great to compensate for, leading to the hypothesized “network collapse,” manifested as decreases in FC and clinical progression (Schoonheim et al., 2015b, 2017).
In support of this, several studies indicate different patterns of FC changes at different disease stages, such as high FC in clinically isolated syndrome (CIS), the earliest stage of MS, and low FC in progressive MS (Basile et al., 2014; Cocozza et al., 2018; Rocca et al., 2010; Roosendaal et al., 2010a, 2010b). However, high FC has also been related to the severity of impairment (Hawellek et al., 2011), casting doubt on the beneficial nature of these changes. As such, it is not yet clear whether the pattern of results from rs-fMRI studies consistently fits the predictions of this model. This may be complicated by the heterogeneity in methodological aspects of studies, which could influence the direction of findings (Tewarie et al., 2018).
In this study, we carry out a systematic review of rs-fMRI FC studies of cognitive dysfunction in MS to outline the state of the field and provide a critical analysis of findings to date. We considered directionality of results and the influence of methodological aspects on findings of FC alterations. Through doing so we offer key points that need to be addressed to develop a parsimonious account of why FC may change in MS and what it may mean for clinical practice.
Methods
Protocol and registration
The design of the systematic review and article preparation were based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Moher et al., 2015). The systematic review protocol was developed in advance and, in accordance with the PRISMA guidelines, registered with the International Prospective Register of Systematic Reviews (PROSPERO) on May 18, 2020, and last updated on August 31, 2020 (Registration No. CRD42020154415).
Information sources and search strategy
Literature searches were conducted in Embase (accessed through the Ovid interface, 1974 onward), Medline (accessed through Ovid, 1946 onward), and PsycINFO (accessed through Ovid, 1806 onward) on October 31st, 2019, with no limits imposed on the searches. The search strategy used terms for “multiple sclerosis,” “functional connectivity,” and “cognition” and was tailored for each database to use both controlled terms where available and uncontrolled keywords to capture any synonym, abbreviation, and related term of the keywords of interest. The searches were repeated on October 22nd, 2020, to capture any studies published since the original searches. The same search strategy was used, but limits were added to capture only results that had been added or updated in the period November 1st, 2019, to October 22nd, 2020. The full search strategy used in each database is available in Supplementary Table S1.
Study eligibility and selection
Records returned by each search were imported into the Mendeley Reference Management Software v 1.19.4, and duplicates were removed using the tool's deduplication function. Titles and abstracts were then manually screened by two independent reviewers (D.J. and R.S.). Full-text publications were obtained for all articles chosen for full-text review by one or both reviewers and assessed for inclusion in the review against predefined eligibility criteria. Any disagreements about study inclusion were resolved through discussion and reasons for study exclusion were recorded. This process was then repeated for the search conducted on October 22nd, 2020. The results at each stage, for the combined two searches, are presented in Figure 2.
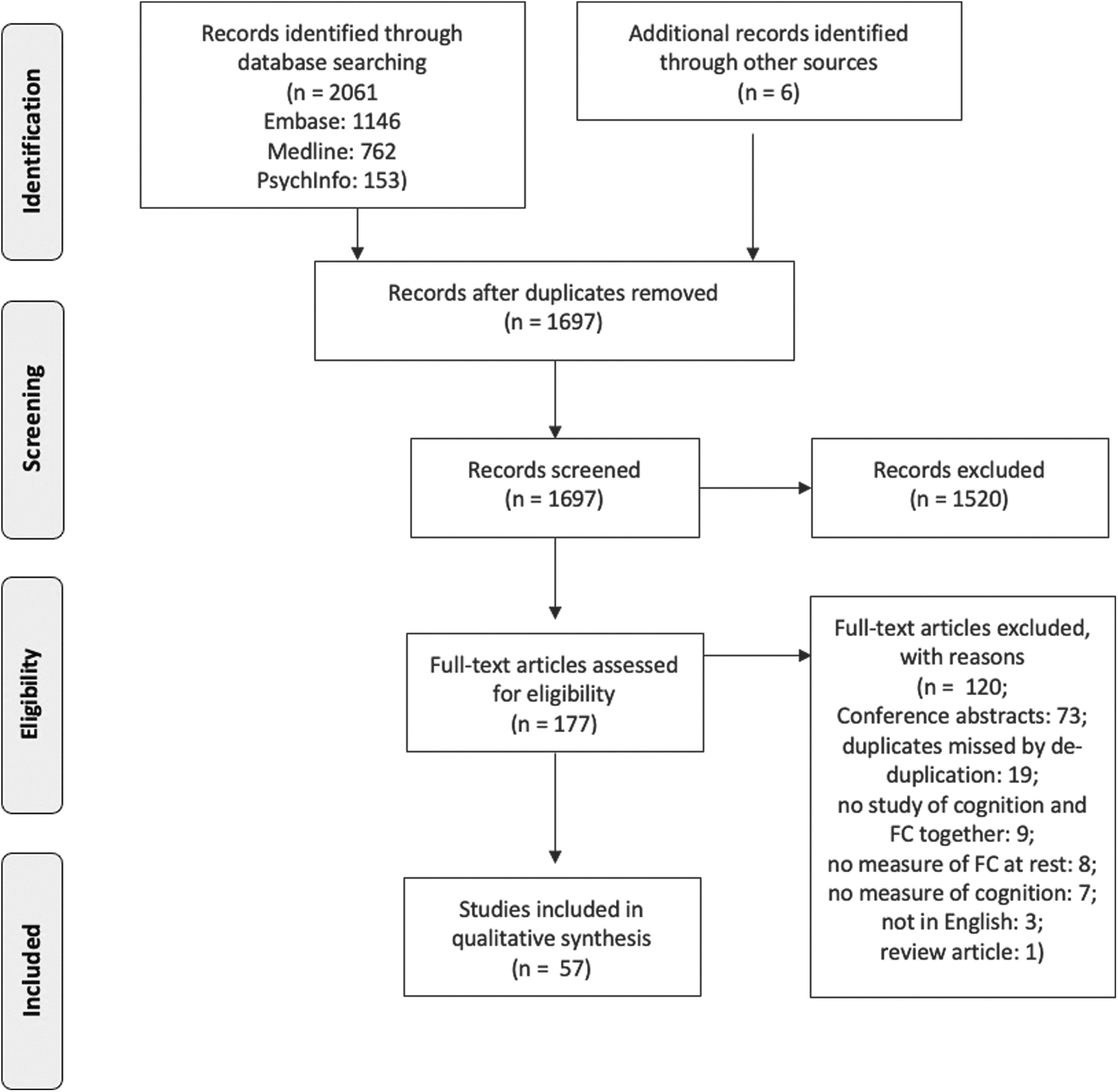
Flow diagram showing identification, screening, and selection of records. Outlines combined database searches conducted on October 31st, 2019, and on October 22nd, 2020, using the PRISMA protocol for studies of rs-fMRI and cognitive function in MS. Template from Moher et al. (2015). MS, multiple sclerosis; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis; rs-fMRI, resting-state functional MRI.
Eligibility criteria were as follows: original peer-reviewed research studies reporting on cognitive function and FC metrics derived from rs-fMRI in adult MS patients. Review articles, book chapters, and conference abstracts were excluded, as were any original research studies in a pediatric population, on diseases other than MS, studies that had not measured cognitive function and/or FC, studies focusing on cognitive rehabilitation, studies that had assessed social cognition only, and any articles that were not available in English.
Data collection and synthesis
Data extraction was performed by D.J. and R.S. and the following data items were recorded: (1) study characteristics (authors, year of publication, journal); (2) aims of the study; (3) participant details (MS subtype, control group, sample size, disease duration of MS sample, Expanded Disability Status Scale [EDSS] score of MS sample); (4) MR methodology (scanner field strength, MR metrics); (5) FC analysis (data preprocessing, method for analysis, whether analysis was global or regional [and if so, which regions], use of covariates); (6) cognitive testing (cognitive test(s) used, definition of cognitive impairment, number of CI/CP patients if applicable); and (7) results from FC analysis and from other MR metrics.
To understand whether there might be a link between methodological aspects and FC results, we examined whether a particular feature was commonly present in studies that report links between worse cognition and either high or low FC. The features we examined were the MS subgroup studied, the average disease duration of patient samples, the rs-fMRI analysis method, and the brain region or resting-state network (RSN) investigated. Because the studies included were too heterogeneous for a meta-analysis, data synthesis was done by tallying the number of studies sharing a specific methodological feature or FC result.
Assessment of study quality
A quality assessment approach was chosen over a risk-of-bias tool because most articles for inclusion in this review were expected to be cross-sectional. The AXIS tool was designed for cross-sectional studies across a range of scientific disciplines (Downes et al., 2016) and was therefore selected to judge the quality of the evidence included in the review. The AXIS tool is a 20-item checklist that asks “yes/no” questions about important elements of a study. Three of the 20 items in the tool were not relevant for the studies selected for this review, as they refer to responding to an intervention, and so, quality assessment was based on the remaining 17 items. The items of the AXIS tool are not scored, but instead recorded in a similar way to the Cochrane risk-of-bias tool (Higgins et al., 2011), allowing review authors to make an overall assessment of the quality of the study based on the presence or absence of reporting of the items covered by the tool.
Results
Study selection and quality assessment
The systematic review process is outlined in Figure 2. The database searches yielded 2061 results, and in addition, 6 were identified from other sources. After removal of duplicates 1697 remained, which were screened for eligibility until 177 remained for full-text assessment. At this point, 120 records were excluded, most of which were conference abstracts (see Fig. 1 for reasons for exclusion). Fifty-seven studies met eligibility criteria and were included in the review. These studies are summarized in Table 1. All studies were of high quality, as measured by the AXIS tool (Downes et al., 2016). Eighteen studies did not include clear details of where participants were recruited from for the study, and very few studies (5/57) had a justification for the sample size used.
Study Characteristics, Cognitive Assessment, and Relationship Between Cognition and Functional Connectivity
Subtypes not specified.
Number of PPMS relative to SPMS not reported.
↑arrow up indicates that high FC is associated with worse cognition; ↓ arrow down indicates that low FC is associated with worse cognition; — dash indicates negative result or that the study did not assess directionality in the relationship between FC and cognition.
Participant characteristics
The studies that were included differed in the clinical and demographic details of the MS samples used. The majority of studies used a mixed sample of different MS phenotypes (29/57 studies), and slightly over a third used a sample of relapsing-remitting MS (RRMS) patients only (22/57 studies). The remaining six studies used a primary progressive MS sample (1/57), CIS sample (2/57), a benign MS sample (1/57), or did not specify the MS subtype (2/57). See Table 1 for details on the cohort of each study.
The average disease duration ranged from as little as 4.2 months (Koubiyr et al., 2019) to 21.9 years (Lin et al., 2019) from either time from first symptom or from diagnosis, and median EDSS ranging from 1 (Faivre et al., 2012; Koubiyr et al., 2019) to 6.5 (Manca et al., 2019).
Most studies (54/57) used healthy volunteers as a control group. In one study, normative data from age-matched healthy controls were used for neuropsychological assessments, but no control group was used for comparisons of MRI metrics (Manca et al., 2019). In one study, no control group was specified (Leavitt et al., 2014), and in one longitudinal study, no control group was used (Petsas et al., 2019). Out of the studies using healthy controls, many did not report matching groups on any demographic variables (18/54), while some reported matching groups but not on which variables (3/54) and one reported not matching the groups. Of the studies reporting the variables groups were matched on, most were on age and sex (15/54), followed by age, sex, and education (10/54), age only (2/54), sex only (2/54), or age, sex, education, and premorbid intelligence quotient (1/54). In this review, we have interpreted the words “sex” and “gender” to both refer to sex, given that MS is a disease characterized by sex differences in prevalence (Krysko et al., 2020; Thompson et al., 2018).
Neuropsychological assessment
Most studies (34/57) looked at relationships between cognitive test performance and MR metrics through correlations or regressions, and 19 studies examined group differences in MR metrics between patients who met the criteria for cognitive impairment and those who did not. Of the remaining four studies, one looked at FC only in MS patients with intact spatial memory (Roosendaal et al., 2010b), and three did not directly assess the relationship between cognition and FC. Despite this, they were included in the review for the following reasons: the authors of one study expressed intentions to correlate FC measures with clinical measures, but did not because the FC measure did not show any abnormalities in MS patients (Romascano et al., 2015); two studies indirectly explored the relationship between FC and cognition and did not meet any exclusion criteria (van Geest et al., 2017, 2018).
To assess cognitive function, most studies used either the Brief Repeatable Battery of Neuropsychological tests (BRB-N), which have been validated for use in MS (Amato et al., 2006), alone or in combination with other tests (20/57), or a collection of individual tests (22/57). The remaining studies used either another cognitive battery; Brief International Cognitive Assessment for MS (BICAMS) n = 2 (Langdon et al., 2012), Minimal Assessment of Cognitive Function in MS (MACFIMS) n = 2 (Benedict et al., 2002), or a single test; Paced Auditory Serial Addition Test (PASAT) n = 6, Symbol Digit Modalities Test (SDMT) n = 1, Location Learning Test n = 1, Short test of mental status n = 1, the computerized test of information processing n = 1, or a cognitive reserve index (n = 1). See Figure 3A for an overview of the tests used across the reviewed studies. The specific battery or tests used by each study are summarized in Table 1.

Neuropsychological tests used in the reviewed studies. (
Within the 19 studies that split the MS sample into CI and CP subsamples, there were 12 different definitions of cognitive impairment. Some definitions are likely guided by the test(s) used to assess cognition, but even among studies using the BRB-N, there were five different definitions of cognitive impairment (Fig. 3B). These include the following: ≥1.5 standard deviation (SD) below normative values on ≥1 test (n = 1); ≥1.5 SD below controls scores on ≥2 tests (n = 5, but note that four used this definition of a mildly CI group), ≥2 SD below normative values on ≥1 test (n = 1); ≥2 SD below normative values on ≥2 tests (n = 9); and performance in the fifth percentile of scores on either the Selective Reminding Test or Spatial Recall Test compared with normative data (n = 1).
FC analysis
Half of all studies (28/57) used a seed-based connectivity analysis (SCA) method for assessing FC. In this category, we have included studies that used one or a few specific regions of interest (ROIs; regional SCA) or divided the whole brain into ROIs and created a connectivity matrix (global SCA). The second-most common method was independent component analysis (ICA) (14/57), and the remaining studies calculated graph theory metrics (7/45), used a principal component analysis (1/45), or used a combination of SCA and graph theory (1/45) or ICA and graph theory (1/45). See Table 1 for the design and rs-fMRI analysis method of each study.
A wide range of regions and RSNs were investigated, either as a priori defined areas of interest or as patterns emerging from a data-driven analysis, of which the most common were the DMN (21/57), thalamus and thalamic networks (9/57), and the frontoparietal network (FPN), including the right, left, dorsal, and ventral FPNs (7/57). Other RSNs and regions investigated include the attentional network including left, right, dorsal, ventral variants, the salience network, the executive network, the working memory network, the motor network, the sensorimotor network, the visual processing network, the auditory network, the auditory and language processing network, visual processing networks, including medial and lateral variants, the cerebellar network, the medial prefrontal cortex, anterior cingulate cortex, posterior cingulate cortex, precuneus, basal ganglia, hippocampus, and cerebellum. Ten studies conducted a whole-brain analysis and did not report regional FC changes.
FC results
The main result of the relationship between FC and cognition of each study is summarized in Table 1 and Figure 4A. Overall, 18 studies found worse cognition to be linked with high FC and 17 found it to be associated with low FC. Nine studies found patterns of both high and low FC to be associated with cognitive impairment, in different regions or for different MR metrics, and seven studies found no significant relationship between cognitive and FC measures. Six studies had a methodology that did not measure the direction of FC change in relation to cognitive impairment.
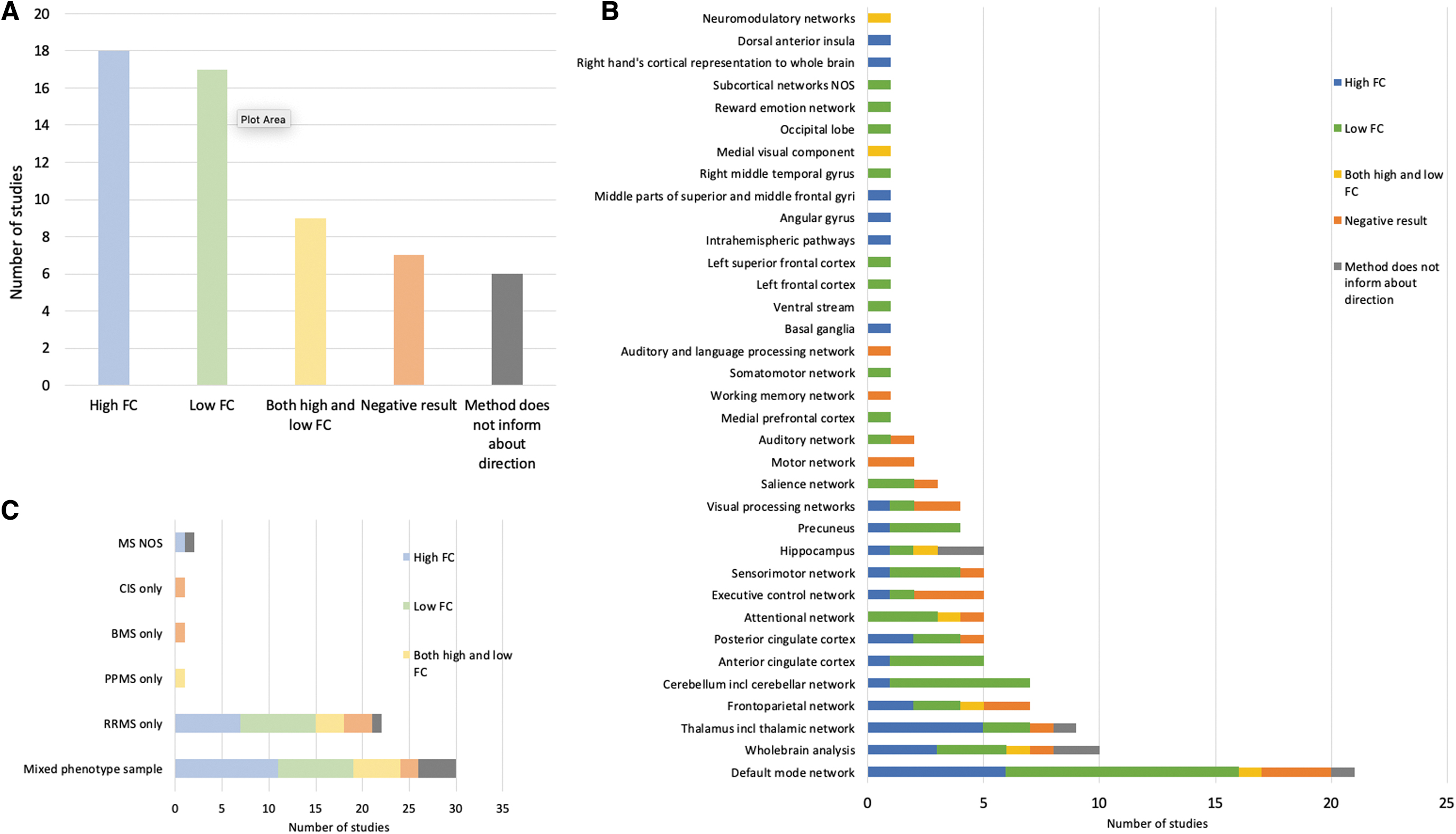
Number of studies reporting an association between poor cognitive test performance and high or low FC.
When grouping studies based on methodological and clinical features to assess whether one direction of FC change associated with worse cognition is more commonly seen in studies with that feature, we found no trend to suggest that one FC direction change associated with worse cognition is more commonly seen in studies using a specific method or studying a specific type of sample. This includes grouping studies based on the RSN or network assessed. For example, of the 21 studies measuring FC in the DMN, 10 found worse cognition to be associated with low FC, 6 with high FC, 1 with both high and low FC, 3 obtained a negative result, and 1 study did not test the relationship directly. See Figure 4B and Supplementary Table S2 for a full overview of study results by regions investigated.
We also considered the role of disease phenotype, however, most studies used either a mixed sample consisting of several phenotypes or a sample of RRMS patients only. Of the 22 studies that used an RRMS sample, 11 reported worse cognition to be associated with high FC and 10 with low FC. Three studies reported a negative result and one had a study method that does not inform about the direction of FC changes. Similarly, within the mixed-sample studies, almost half of the studies reported worse cognition to be associated with high FC (13/29) and more than half with low FC (16/29). Some studies reported both high and low FC to be associated with worse cognitive function and have therefore been counted twice. See Figure 4C for an overview. In seven of the studies with mixed phenotype samples, subgroup analyses were conducted to compare FC changes between different MS phenotypes in the sample, but only two included cognition in these analyses. One found a stronger positive correlation between FC in the DMN and errors on the PASAT in secondary progressive MS (SPMS) compared with RRMS, while another found differences between RRMS and SPMS in the spatial location of FC abnormalities that correlated with cognitive test performance.
Finally, we ordered studies by the average reported disease duration of the sample used, to see if patterns of FC changes differ from early to late in the disease and found no such trend (Fig. 5 and Supplementary Table S3).

Direction of FC abnormalities sorted by average disease duration. Direction of FC abnormalities associated with worse cognition, sorted by average disease duration of the sample in each study. Disease durations reported in months in the original study have been converted to years by dividing by 12. Because several studies used samples of mixed phenotypes and different disease durations, the following decisions were taken when ordering studies by the disease duration: (1) studies were ordered by the overall disease duration of the sample, when given; (2) studies were ordered by the disease duration of the CI group; (3) if there were two CI groups, studies were ordered by the disease duration of the more impaired group, or the CI group with atrophy, in one case; (4) when the disease duration was only reported for each MS phenotype, or sex, studies were ordered by the disease duration of the larger sample; (5) for a study that had equal numbers of males and females, the study was ordered by the sex with the longer disease duration; (6) for one study that used a subset of MS patients who were matched to HC, the study was ordered by the disease duration of the matched subset. References are provided in Supplementary Table S3. HC, healthy controls. Color images are available online.
Discussion
In this systematic review, we examined the consistency and direction of findings of studies investigating associations between rs-fMRI FC measures and cognition in MS. Overall, the studies reviewed support the notion of FC alterations associated with cognitive dysfunction in MS (Filippi and Rocca, 2013). Although most changes were related to cognitive dysfunction, the direction of FC changes varied considerably between studies and was not clearly linked to any methodological factors. There was substantial heterogeneity in clinical and rs-fMRI methodology, as has previously been noted in nonimaging cognition studies in MS (Benedict et al., 2020; Sumowski et al., 2018).
We therefore consider ways in which the field can reflect on what has been learned to date and improve future study designs to more clearly understand the mechanisms and consequences of changes in rs-fMRI FC. Specifically, we propose that future studies should consider the following points that are the source of much heterogeneity identified in this review: (1) the possibility of different network degeneration patterns in different MS clinical and cognitive phenotypes; (2) the role of disease duration and aging processes; (3) the definition and measurement of cognitive impairment; (4) the spatial topography of brain regions of RSNs of interest; and (5) the investigation of the mechanisms of FC abnormalities. A discussion of each follows below.
Models of network changes in MS
To consider how FC should relate to cognitive function in MS, and what results to expect from rs-fMRI studies, a model of the relationship is useful. The most commonly used model for understanding FC changes in MS is the “network collapse” model, which postulates three main stages (Schoonheim et al., 2015b). In the first early stage, network efficiency remains normal, at this point structural damage can be compensated by increases in local activation. This predicts early increases in FC, reflecting these compensatory processes. The second stage is where structural damage accrues to a critical point, at which compensatory processes become less effective. Finally, in the third stage, structural damage exceeds the critical point with associated “network collapse,” and concomitant decreases in FC.
Computational modeling of empirical data on FC in MS supports this model (Tewarie et al., 2018). Similarly, longitudinal studies demonstrate a reorganization of structural and functional networks in early stages of MS (i.e., CIS) despite intact cognitive performance, suggesting that compensatory processes are at work (Koubiyr et al., 2019). Cross-sectional, task-related fMRI studies also indicate increasing deviation from healthy control patterns of brain activation during cognitive tasks, consistent with functional reorganization, as patients progress from CIS to RRMS to SPMS (Loitfelder et al., 2011). Together, these theories predict early adaptive reorganization of functional networks, followed by a failure of effective network organization in MS over time (Chard et al., 2021).
Role of clinical phenotype, disease duration, and age
In our review, when ordering studies by the average disease duration of the sample, we did not observe a trend in the direction of FC findings from early to advanced MS, as predicted by the network collapse model and as observed in some studies (Castellazzi et al., 2018). We therefore consider whether the lack of fit to the model relates to the particular samples or methods of analysis used. Many of the studies included in this review used samples of mixed clinical phenotypes. The MS phenotype has previously been reported to influence resting network FC alterations, and so, the inclusion of mixed MS samples could contribute to the lack of consistency in findings.
However, in our review, only two studies assessed the relationship between FC, phenotype, and cognition, and these found both abnormally increased (Meijer et al., 2018a) and abnormally decreased (Rocca et al., 2018) FC in patients with progressive MS. This suggests that even in specific MS subgroups, there remains considerable variability in the direction of findings. More evidence is needed to determine whether FC changes vary between phenotypes, and whether any model of network changes has different explanatory power for the different phenotypes.
A further important consideration is the effect of disease duration and how it may mediate the relationship between FC, phenotype, and cognition. Longer disease duration in RRMS is associated with FC changes in attentional, executive, and DMNs (Castellazzi et al., 2018). This suggests that disease duration may have an important influence on FC changes associated with cognitive impairment, possibly due to increased structural damage with longer disease duration. While we did not find such a trend in our review, our analysis of disease duration was confounded by samples of mixed phenotypes, the study of many different spatial regions of the brain, and the vast number of definitions of cognition. Therefore, the effect of disease duration should be formally tested in studies in which other variables, such as neuropsychological tests and spatial regions, are kept constant.
Those studying patients with longer disease duration (such as those with SPMS) will also have to account for age-related atrophy in these samples (Azevedo et al., 2019), which will be exacerbated when studying those patients with relapsing as well as progressive subtypes of MS.
Cognitive tests and definition of cognitive impairment
We also considered whether the direction of FC change relates to definitions of cognitive impairment and choice of FC analysis. Studies of cognition in MS use a vast array of definitions of cognitive impairment (Benedict et al., 2020; Fischer et al., 2014; Sumowski et al., 2018), as reflected in this review. For example, of the studies using the BRB-N to assess cognitive function, most use a more conservative definition of cognitive impairment of at least two SDs below controls on two or more tests (Bonavita et al., 2011; d'Ambrosio et al., 2017, 2020; Eijlers et al., 2017, 2019; Meijer et al., 2017, 2018a; Rocca et al., 2018; Schoonheim et al., 2015a), but other, less conservative definitions are used too (Cruz-Gómez et al., 2014, 2018; Eijlers et al., 2018).
The definition of cognitive impairment has been shown to have effects on underlying FC alterations of MS CI by the classification used (Doshi et al., 2019). A few studies have compared different thresholds of cognitive impairment and found the greatest FC abnormalities in those participants meeting the more conservative thresholds (i.e., more than two SDs from controls on two or more tests). In contrast, less clear FC abnormalities were observed in samples performing between 1.5 and 2 SDs below controls on 2 tests (“mild cognitive impairment”) (Doshi et al., 2019; Eijlers et al., 2017; Meijer et al., 2017; Schoonheim et al., 2015a). This demonstrates the possible effect of the definition of cognitive impairment on FC findings and the arbitrary nature of these thresholds. Such findings highlight the importance of using a consistent measure of cognitive dysfunction and definition of impairment across studies.
As a further challenge there is no consistency in the use of specific cognitive tests or batteries for defining cognitive dysfunction in MS, with many studies using impairments on multiple separate tests to assess global cognitive function. There are documented phenotypic differences in impairments by test and domain (Chan et al., 2017; Connick et al., 2013; Johnen et al., 2017; Ruet et al., 2013a), yet very few studies have looked at network alternations associated with deficits in specific cognitive domains, such as information processing speed or memory, and those that have used a range of cognitive tests to probe the same domain, further complicating comparisons. The use of consistent measures of cognition and definitions of cognitive impairment, and possibly conducting subgroup analyses of different cognitive domains, should therefore be an aim for future studies.
Spatial topography
Separately, we found scant evidence to support a consistent direction of FC change in CI patients when using model-based (e.g., seed) or data-driven (e.g., ICA) approaches, or when considering specific RSNs. Indeed, the DMN, the most commonly studied RSN across the literature, showed both increases and decreases in CI MS patients. One explanation of increases in FC is that processing moves from local networks to hub regions when the former accumulates structural damage (Meijer et al., 2017; Stam, 2014; Tahedl et al., 2018), but this explanation fails to account for the findings in this review. Attempting to understand these findings is complex. The role of disease stage in the samples studied could influence the FC directions reported, in line with the network collapse model.
Another consideration is the spatial location of the regions investigated. It must be remembered that the DMN consists of several key “hub” regions, which are heavily interconnected and involved in several additional networks. For example, the anterior cingulate cortex is also a key hub in the salience network. Moreover, the regions making up a network can vary between studies, often depending on the analysis method used. In a seed-based connectivity study, the extent of the network of interest will depend on how and where the seed is defined. The idea that different networks or even subregions of a network hub have different patterns of connectivity is evidenced by the thalamus, a network hub that has shown both hypo- and hyperconnectivity in MS, depending on the thalamic nucleus and pathways investigated (Lin et al., 2019).
Despite this, the topography of a network might not be the full explanation of the inconsistent results observed. A meta-analysis of mild cognitive impairment prodromal to Alzheimer's disease did not find consistent FC abnormalities even when using a voxel-wise analysis to assess the same spatial regions, suggesting that directional inconsistencies of FC findings cannot be fully explained by the spatial extent of the region(s) studied (Eyler et al., 2019). Nevertheless, to rule out the potential influence of topography, and enable comparisons between studies, care should be taken to define a specific region consistently with previous research.
Mechanisms of FC changes
There also needs to be a greater understanding of the mechanisms through which FC changes in MS. The “network collapse” model suggests that network efficiency reduction is a function of accumulation of structural damage. In support of this, work focusing on structural connectivity in MS has found consistent evidence for structural network alterations associated with cognitive dysfunction (Llufriu et al., 2017, 2019; Solana et al., 2018). However, these studies have considered white matter in isolation, and so, conclusions about the effect of anatomical network changes including gray matter on FC cannot be drawn. In contrast, multimodal MRI studies of diffusion-weighted MRI (DWI) and rs-fMRI can assess the relationship between changes in structural and FC. Those that have been conducted support the influence of alterations in white matter linked to FC abnormalities in MS, and fit the predictions of the “network collapse” model (Enzinger et al., 2016; Lowe et al., 2008; Patel et al., 2018; Tewarie et al., 2014, 2018).
Future multimodal studies using DWI and rs-fMRI can test the predictions of the “network collapse” model further and to develop this or new models as needed to better characterize progression and the influence of pathology in MS brains, to develop clinically useful disease markers. In addition, there is evidence of physiological abnormalities in MS that are associated with cognitive dysfunction, such as cerebral hypoperfusion and sodium accumulation in the gray and white matter (Lapointe et al., 2018; Maarouf et al., 2017; Paling et al., 2013), and additional proton spectroscopic changes (Solanky et al., 2020). Considering how these are related to network changes can help us understand the mechanisms of network abnormalities and aid in the search for a biomarker of cognitive impairment.
FC as a biomarker of cognitive impairment in MS?
This systematic review provides a call to arms for the need to standardize the study of cognitive impairment in MS, but also the use of specific rs-fMRI methodology and interpretations of results. Eleven years ago, Fox and Greicius (2010) identified inconsistent results of FC changes across rs-fMRI studies as a barrier to the clinical applicability of this modality, and suggested a set of guidelines for rs-fMRI studies of clinical populations.
Despite this, heterogeneity in study methodology seems to be a challenge across neurodegenerative diseases investigated by rs-fMRI, and the rs-fMRI-derived FC measure is not yet suitable as a biomarker of disease (reviewed by Hohenfeld et al., 2018). Even in Alzheimer's disease, where there is evidence of consistent hypoconnectivity compared with controls, there is a problem of inconsistent directional results in the prodromal stages (i.e., mild cognitive impairment) of this disease (Badhwar et al., 2017; Eyler et al., 2019). A recent systematic review and meta-analysis found inconsistent results across 56 studies in mild cognitive impairment and concluded that while FC changes may be a marker of Alzheimer's disease, at present the evidence for FC to be a biomarker of the risk of developing Alzheimer's disease is limited (Eyler et al., 2019).
In this review, we have shown that, similarly, the FC measure is not yet a suitable biomarker for cognitive impairment in MS. Unlike Alzheimer's disease, the use of rs-fMRI in MS has not been the subject of many systematic reviews, and so, we do not at present know whether FC results become more consistent at a certain stage of the disease. In this review, we found considerable variability in the study of cognitive impairment in MS by rs-fMRI, both in study methods and findings, posing a challenge for the interpretation of results.
Standardization of FC studies of cognition in MS and future directions
The FC measure shows promise; most studies suggest that FC alterations are a key pathological feature. Therefore, we argue that standardization of study methods and more model-driven research would lay a clearer path toward understanding directional FC changes, and thereby clinical utility of the FC metric and the potential use as a biomarker of MS disease state.
First, clinical studies using the rs-fMRI method should ensure that the guidelines suggested by Fox and Greicius (2010) are followed: “(1) A priori hypotheses regarding a region or network with abnormal [rs-fMRI FC] and clear criteria for selecting this region or network; (2) a priori hypothesis and demonstration of a region or network with normal [rs-fMRI FC] to serve as a control; (3) correlation with clinical variables whenever possible; (4) stringent correction for multiple comparisons; (5) an analysis of movement in patients and control subjects; (6) an analysis of the differential impact of preprocessing in patients and control subjects; and (7) a discussion of how current findings relate to prior [rs-fMRI FC] findings.” In the studies considered in this systematic review, point 3 is necessarily met. Points 4, 5, and 6 are typically met. Points 1, 2, and 7 are occasionally met.
Going forward, research using FC as a marker of cognitive impairment in MS should consider the following to meet points 1, 2, and 7: (1) studying different clinical and cognitive phenotypes of a disease separately to identify phenotype-specific influences; (2) controlling for age and disease duration, where this is known to have an influence on the clinical symptom of interest; (3) using well-established and validated measures of the symptom of interest for the disease being investigated; (4) defining regions of interest consistently with previous research; and (5) conducting model-led research to understand the underlying pathophysiological basis of any alterations in FC, for example, in MS this might involve multimodal diffusion MRI and rs-fMRI studies to test the network collapse model and its prediction of FC being driven by structural changes.
The studies so far have been useful to establish that effects do exist and that there is an association with cognitive impairment, but what is needed now is the equivalent of a well-powered multisite phase 3 trial to establish that the effect is robust. This will help to determine whether FC measures can indeed be used as biomarkers of cognitively relevant network degeneration in MS.
Limitations
This review is the first to systematically summarize the rs-fMRI FC literature on cognitive impairment in MS. However, there are some limitations to consider. First, rs-fMRI is not the only imaging modality for studying FC. While they were outside the scope of this review, electroencephalography and magnetoencephalography studies may offer additional insights into FC changes associated with cognitive impairment in MS. Similarly, there are other network measures that can be derived from rs-fMRI in addition to FC, such as dynamic FC and graph theory measures. At present the number of studies reporting these measures is small and so we did not consider them separately, but rather grouped them with the FC measure for the purposes of the review. Nevertheless, these metrics provide somewhat different information to the FC metric, which has not been captured in detail in this review.
In addition, we compared results from studies that looked at the same networks or regions of interest, but using different analysis methods, and vice versa. It could be argued that differences in methods and spatial topography of networks limit the information that can be gained from this approach, however, grouping studies that shared similarities on several methodological variables, such as networks studied and analysis method, would have created very small groups from which it would have been difficult to infer anything with confidence. Previous systematic reviews of rs-fMRI FC changes in mild cognitive impairment find inconsistent directions of altered FC in patient groups even when using a voxel-wise analysis (Eyler et al., 2019). This suggests that the findings of inconsistency in FC results are not entirely due to variation in networks studied or spatial topography. Finally, we did not carry out a formal statistical meta-analysis of the studies in this review. Instead, due to the low numbers of homogeneous studies, we were limited to tallying the number of studies with a specific feature. As studies start to become more consistent in their use of methods, it will become easier to determine across the field whether the hypotheses including disease-specific effects, such as the “network collapse” model, can suitably explain the patterns of associations that are observed.
Conclusion
In conclusion, this systematic review shows that cognitive impairment in MS is associated with both high and low FC, indicating that any network change seems related to poorer functioning. This is an important finding that shows that rs-fMRI FC is sensitive to cognitively relevant brain changes. However, because of the inconsistencies in the direction of FC results, this measure needs further exploration in consistently designed studies to become a suitable biomarker of cognitive impairment in MS. To better understand the relationship between worsened cognitive function and FC abnormalities, including directional FC changes, there must be standardization in the field of the definition and measurement of CI, rs-fMRI methodology, and correction and allowances for the MS phenotype, and non-MS-related pathology from aging. We have outlined five recommendations to this effect for future research, based on the sources of heterogeneity we have identified in literature, and welcome a discussion of these with our colleagues in this field.
Footnotes
Acknowledgments
This article has been published on preprint server medRxiv, DOI 10.1101/2021.03.18.21253878, and is available on the following weblink:
Authors' Contributions
A.D. and D.J. contributed to the conception and design of the study. The data were acquired and analyzed by A.D., D.J., and R.S. All authors contributed to drafting and reviewing the text and figures.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by grants held by D.J. and A.D. D.J. was supported by a Medical Research Council Doctoral Training Partnership grant (MR/N013751/11). A.D. was supported by the Multiple Sclerosis Progressive Multi-arm Randomisation Trial, an investigator-led project sponsored by the University College London.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.