
Abstract
Introduction:
Poststroke fatigue (PSF) is a disabling condition with unclear etiology. The brain lesion is thought to be an important causal factor in PSF, although focal lesion characteristics such as size and location have not proven to be predictive. Given that the stroke lesion results not only in focal tissue death but also in widespread changes in brain networks that are structurally and functionally connected to damaged tissue, we hypothesized that PSF relates to disruptions in structural and functional connectivity.
Materials and Methods:
Twelve patients who incurred an ischemic stroke in the middle cerebral artery (MCA) territory 1–3 years prior, and currently experiencing a range of fatigue severity, were enrolled. The patients underwent structural and resting-state functional magnetic resonance imaging (MRI). The structural MRI data were used to measure structural disconnection of gray matter resulting from lesion to white matter pathways. The functional MRI data were used to measure network functional connectivity.
Results:
The patients showed structural disconnection in varying cortical and subcortical regions. Fatigue severity correlated significantly with structural disconnection of several frontal cortex regions in the ipsilesional (IL) and contralesional hemispheres. Fatigue-related structural disconnection was most severe in the IL rostral middle frontal cortex. Greater structural disconnection of a subset of fatigue-related frontal cortex regions, including the IL rostral middle frontal cortex, trended toward correlating significantly with greater loss in functional connectivity. Among identified fatigue-related frontal cortex regions, only the IL rostral middle frontal cortex showed loss in functional connectivity correlating significantly with fatigue severity.
Conclusion:
Our results provide evidence that loss in structural and functional connectivity of bihemispheric frontal cortex regions plays a role in PSF after MCA stroke, with connectivity disruptions of the IL rostral middle frontal cortex having a central role.
Impact statement
Poststroke fatigue (PSF) is a common disabling condition with unclear etiology. We hypothesized that PSF relates to disruptions in structural and functional connectivity secondary to the focal lesion. Using structural and resting-state functional connectivity magnetic resonance imaging (MRI) in patients with chronic middle cerebral artery (MCA) stroke, we found frontal cortex regions in the ipsilesional (IL) and contralesional hemispheres with greater structural disconnection correlating with greater fatigue. Among these fatigue-related cortices, the IL rostral middle frontal cortex showed loss in functional connectivity correlating with fatigue. These findings suggest that disruptions in structural and functional connectivity play a role in PSF after MCA stroke.
Introduction
Poststroke fatigue (PSF) is a disabling condition that develops in upward of 70% of patients within the early months after acute stroke and persists chronically in about 50% of patients (Paciaroni and Acciarresi, 2019). PSF is characterized by pathological fatigue, which has been defined as an overwhelming feeling of exhaustion that is not ameliorated by rest and leads to difficulties in performing routine daily activities (Staub and Bogousslavsky, 2001). Despite the prevalence of PSF, its etiology is unclear. Multiple factors are thought to underlie PSF, including medical comorbidities, neurological/physical impairments, immune response to stroke, sleep disturbance, and prestroke depression and anxiety (Hinkle et al., 2017). The lesion caused by stroke is thought to be an important causal factor in PSF.
It is notable that patients who experienced a transient ischemic attack, an event that does not result in a permanent brain lesion, are less likely to develop pathological fatigue than patients who had a minor ischemic stroke, despite both patient groups having similar medical histories and lacking enduring neurological deficits (Naess et al., 2012; Winward et al., 2009). However, many studies investigating PSF in relation to lesion size or location found no association (Carlsson et al., 2003; Choi-Kwon et al., 2005; Ingles et al., 1999; Radman et al., 2012), and only a few reporting an association with lesion location (e.g., basal ganglia) (Snaphaan et al., 2011; Tang et al., 2010, 2013).
Importantly, an infarct causes not only focal tissue death, but also widespread changes in brain networks that are structurally and functionally connected to the damaged tissue (Gratton et al., 2012). Structural connectivity of a brain network has been defined as relying on monosynaptic white matter connections, whereas functional connectivity is correlated activity of gray matter regions that arise from monosynaptic and polysynaptic white matter connections (Park and Friston, 2013). Disruptions in structural and functional connectivity have been demonstrated to be key explanatory factors in poststroke deficits in sensorimotor function (Carter et al., 2012; Kessner et al., 2021), language (Baldassarre et al., 2019), and cognition (He et al., 2007; Salvalaggio et al., 2020; Siegel et al., 2016).
Recent evidence suggests that structural disconnection of gray matter after stroke leads to secondary disruptions in functional connectivity (Griffis et al., 2019, 2020; Olafson et al., 2021; Thiebaut de Schotten et al., 2020). Despite the role of disrupted structural and functional connectivity in behavioral and cognitive deficits after stroke, studies examining its role in PSF are lacking.
The primary hypothesis of the current study was that structural disconnection of gray matter is associated with PSF. To test this hypothesis, we assessed fatigue severity in relation to gray matter disconnection in patients with a middle cerebral artery (MCA) stroke incurred 1–3 years prior. Gray matter disconnection was measured using structural magnetic resonance imaging (MRI) data. The secondary hypothesis of this study was that fatigue-related disconnection of gray matter is associated with widespread disruption in functional connectivity measured using resting-state blood oxygenation-level-dependent (BOLD) functional MRI (fMRI) data.
Materials and Methods
Study design
This study was conducted at the Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital. The Institutional Review Board approved the protocol. All subjects provided written informed consent. Patients were recruited via several routes within the Mass General Brigham health care system: physicians, the Research Patient Data Registry, and the Rally website that advertises internal clinical research studies.
Participants
Twelve stroke patients completed the study. The inclusion criterion was a first-ever, unilateral ischemic stroke in the MCA territory 1–3 years prior. The lower limit of this chronic poststroke was selected because behavioral recovery has largely plateaued by 1 year after acute stroke (Kong and Lee, 2013; Wade et al., 1983), and the upper bound was selected to increase patient homogeneity and limit potential fatigue-inducing events occurring between the time of acute stroke and time of study enrollment.
The exclusion criteria were as follows: significant prestroke fatigue measured by a verbal rating score >3 (scale 0–10); significant prestroke disability measured by the modified Rankin Scale score ≥3 (scale 0–5) (Bruno et al., 2011); significant cognitive deficit measured by the NIH Stroke Scale (NIHSS) item 1b and 1c score ≥1 or NIHSS item 9 score ≥2 (Brott et al., 1989); MRI contraindication (e.g., certain metallic implants, claustrophobia); and neurological disorder other than chronic stroke. As we performed MRI simultaneous with 18 kDa translocator protein (TSPO) positron emission tomography (PET) to address other hypotheses (Schaechter et al., 2021), we also excluded patients with major kidney or liver disease, active infection, recent use of a drug with high TSPO binding affinity (e.g., benzodiazepine) or a systemic immunomodulator (e.g., prednisone), or low-affinity TSPO binding based on genotyping.
The PET data are beyond the scope of this study, and thus will not be discussed further here.
To construct reference functional connectivity maps, MRI data from 21 healthy adults (54 ± 8 years, 10 males) who participated in other MRI/PET studies (led by investigator M.L.L.) were selected to approximate the patient group in age and sex. Exclusion criteria for these subjects were an MRI contraindication, neurological disorder, major kidney or liver disease, and low-affinity TSPO binding based on genotyping.
Clinical testing
The Multidimensional Fatigue Inventory (MFI) was administered to all patients. The MFI is a self-report instrument that involves five subscales of fatigue: general fatigue, physical fatigue, mental fatigue, reduced motivation, and reduced activity (Smets et al., 1995). Scores for each subscale range from 4 to 20, with a higher score indicating higher fatigue. We elected to use the general fatigue subscale of the Multidimensional Fatigue Inventory (MFI-GF), which encompasses both physical and psychological aspects of fatigue, as the measure of fatigue in our patients because this subscale has shown the highest sensitivity to within-group differences in fatigue (Smets et al., 1995), and to have the highest convergent validity with other commonly used fatigue scales (Lin et al., 2009; Smets et al., 1995; Song et al., 2018).
The MFI-GF is also the only subscale for which a cutoff score (≥12) has been used to identify pathological fatigue in patients with chronic stroke (Christensen et al., 2008) and other clinical conditions (Holzner et al., 2003), thereby allowing us to better interpret fatigue severity in our patients. We sought to enroll patients who represented the range of MFI-GF scores.
To better characterize our patients, we measured depression using the depression subtest of the Hospital Anxiety and Depression Scale (HADS-D) that scales from 0 to 21, with cutoff scores distinguishing lack of depression (≤7), possibly depression (8–10), and clinically significant depression (≥11) (Zigmond and Snaith, 1983). In addition, we measured motor function using the upper limb subtest of the Fugl-Meyer Stroke Scale (FM-UL) that scales from 0 to 60, with higher scores indicating better motor function of the upper limb (Woodbury et al., 2007), and the 10-Meter Walk Test (10MWT) to assess comfortable walking speed (Flansbjer et al., 2005). As a normative reference for the 10MWT, community ambulation requires walking speed ≥0.8 m/sec (Middleton et al., 2015).
Image acquisition
MRI scanning was done using a Siemens 3T Tim Trio MRI scanner. Structural scans were acquired using a T1-weighted magnetization-prepared rapid gradient echo imaging sequence (repetition time [TR] 2.53 sec; echo time [TE]1–4 1.63/3.49/5.35/7.21 msec; voxel size 1 mm3) and a fluid-attenuated inversion recovery (FLAIR) sequence (TR 10 sec; TE 73 msec; voxel size 1.3 × 1.0 × 5.0 mm). Resting-state BOLD fMRI scans were acquired using a T2*-weighted gradient-echo echo planar sequence (TR 2 sec; TE 30 msec; voxel size 3.125 × 3.125 × 3 mm; 6 min) with each subject instructed to remain awake with eyes open.
Image analysis
Each patient's stroke lesion was labeled manually by an experienced stroke investigator (J.D.S.) on the T1-weighted images, with the FLAIR images used to help delineate lesion boundaries as needed. The T1-weighted images were spatially normalized to Montreal Neurological Institute (MNI) space using FMRIB's Nonlinear Image Registration Tool (FNIRT) from the FMRIB Software Library (FSL; version 6) (Smith et al., 2004), with the lesion masked out to eliminate those voxels from the optimization process (Brett et al., 2001). The resultant nonlinear warp was applied to the lesion labels to transform them into MNI space. To increase statistical power for localizing gray matter disconnection associated with fatigue independent of stroke hemisphere, the T1-weighted images and lesion labels from patients with a right-sided stroke (5 of 12 patients; see Table 1) were flipped across the midsagittal plane before spatial normalization, thereby lateralizing the lesion to the same hemisphere for all patients.
Patient Characteristics
10MWT, 10 Meter Walk Test; FM-UL, Fugl-Myer Stroke Scale for upper limb; HADS-D, Depression subtest of Hospital Anxiety and Depression Scale; MFI-GF, general fatigue subscale of the Multidimensional Fatigue Inventory.
TOAST criteria: LAAS, large artery atherosclerosis; CE, cardioembolism; SVO, small vessel occlusion; ODE, other determined etiology; UDE, undetermined etiology.
We also performed the alternative analysis that could localize fatigue-related gray matter disconnection dependent on the stroke hemisphere by spatially normalizing the T1-weighted images and lesion labels in their native orientation.
Structural disconnection in each patient was estimated using the Network Modification (NeMo) Tool (Kuceyeski et al., 2013). We used the online NeMo Tool (version 2.1) that uses a database of whole-brain, anatomically constrained probabilistic tractography streamlines computed from the Human Connectome Project 3T diffusion MRI data set of 420 healthy subjects (Kuceyeski, 2021). Each patient's lesion label (in MNI space) was entered into the NeMo Tool. The NeMo Tool determines the set of intersecting streamlines from the full set of streamlines, localizes the gray matter end-points of those streamlines in each reference subject, compiles those data across reference subjects, and outputs a voxel-wise “structural disconnection map” (2 mm resolution). The value at each voxel of a structural disconnection map is Change in Connectivity (ChaCo) score that reflects the percent disconnection in the reference data set, ranging from 0% (no disconnection) to 100% (complete disconnection).
Estimates of gray matter disconnection provided by the NeMo Tool have been shown to improve prediction of functional and tissue outcomes in acute stroke patients compared with lesion volume (Kuceyeski et al., 2015, 2016; Schlemm et al., 2021). The NeMo Tool has also been used to localize gray matter disconnection associated with somatosensory deficit (Kessner et al., 2021), recovery-related functional remapping (Olafson et al., 2021), and to predict future gray matter atrophy (Kuceyeski et al., 2014) in stroke patients. We used the structural disconnection maps from all patients to perform voxel-wise correlation analysis against fatigue severity.
As we found structural disconnection of ipsilesional (IL) and contralesional (CL) gray matter correlating significantly with fatigue severity in patients (see the Results section), which we hereafter refer to as fatigue-related gray matter, we went on to test whether structural disconnection of fatigue-related gray matter was associated with disrupted functional connectivity. For functional connectivity analyses, FSL tools were used to preprocess the resting-state fMRI images acquired from the patients and healthy subjects through slice timing correction, motion correction, removal of nonbrain tissue, distortion correction, and generation of a confound matrix of frame-based motion outliers. The preprocessed fMRI data were coregistered to the T1-weighted images, and then nonlinearly spatial normalized into MNI space. As done for image processing to assess structural disconnection, preprocessed fMRI data from patients with a right-sided stroke were flipped across the midsagittal plane to lateralize the lesion to the same hemisphere for all patients.
The fMRI images in MNI space were spatial smoothed using a 6-mm Gaussian kernel and high-pass temporally filtered (cutoff frequency 0.008 Hz). The mean fMRI time series was computed for each IL and CL fatigue-related gray matter region (see the Results section) for each patient, and the corresponding gray matter region for each healthy subject of the reference group. These mean fMRI time series served as seeds in functional connectivity analyses.
For each gray matter seed, a functional connectivity map of z-scores was computed in a general linear model (GLM) by correlating the seed time series against every other voxel in the brain while removing the following sources of variance unlikely to reflect spatially specific correlations of neural origin: (1) mean time series from deep white matter, (2) mean time series from lateral ventricles, and (3) six motion parameter time series (three rotations and three translations). The confound matrix of frame-based motion outliers was entered into the GLM to remove the effects of these time points (Power et al., 2012).
The functional connectivity maps from the healthy subjects were used to construct a reference functional connectivity map for each gray matter seed by computing mean z-score voxel-wise, and then thresholding the mean z-score map to retain only voxels with z-score ≥3.1. Each reference functional connectivity map reflected the network of gray matter regions with positively correlated fMRI signal. Of note, no mean functional connectivity map from healthy subjects had voxels with mean z-score ≤−3.1, indicating that fatigue-related gray matter regions in patients were not part of functional networks normally connected via an anticorrelated fMRI signal. A summary measure of network functional connectivity for each gray matter seed was computed for each patient by calculating mean z-score in the mask defined by the respective reference functional connectivity map after excluding all voxels containing an infarct in any patient.
Infarct volume in each patient was measured using the lesion label in native T1-weighted space, normalized by total intracranial volume to account for individual differences in brain size, and expressed in percent. Total intracranial volume was measured using the T1-weighted image that had been skull-stripped and binarized.
Statistical analysis
To test the primary hypothesis that structural disconnection of gray matter relates to PSF, the structural disconnection maps (ChaCo scores) from the patients were correlated voxel-wise against fatigue severity (MFI-GF scores) using FSL's nonparametric permutation test, randomise. The statistical output map was corrected for multiple comparisons for gray matter voxels of the Desikan–Killiany Atlas that includes all cortical and subcortical gray matter excluding brainstem (Desikan et al., 2006), using threshold-free cluster enhancement (TFCE) (Smith and Nichols, 2009). The family-wise error (FWE) rate was set conservatively to 0.01 to offset the known issue of false-positive connections of tractography streamlines (Tournier, 2019), which could have led to the reference tractography atlas, including some streamlines that are not neuroanatomically plausible. Clusters that survived the FWE rate were identified as fatigue-related gray matter.
To test the secondary hypothesis that structural disconnection of fatigue-related gray matter is associated with disrupted functional connectivity, we first calculated summary measures of disconnection severity for each patient. As the clusters exhibiting fatigue-related structural disconnection were found to span several gray matter regions defined by the Desikan–Killiany Atlas (see the Results section), we intersected the clusters with parcels of the Desikan–Killiany Atlas, and then calculated mean ChaCo score in each region of overlap for each patient. Using JMP software (version 16.2.0), the nonparametric Kendall's correlation coefficient was computed to assess the strength of association between the structural disconnection of each fatigue-related gray matter region (mean ChaCo scores) and the disrupted network functional connectivity of the respective gray matter region (mean z-scores), with significance set at 0.05.
A nonparametric, rather than parametric, test was applied because the mean ChaCo scores of each fatigue-related gray matter region did not fit a normal distribution based on the Shapiro–Wilk test, and therefore failed to meet an assumption for valid statistical inference of parametric tests.
The Kendall's correlation coefficient was also used to assess the association between fatigue severity (MFI-GF scores) and normalized lesion volume because the volume measurements were not normally distributed based on the Shapiro–Wilk test. The Pearson's correlation coefficient was used to assess the association between fatigue severity (MFI-GF scores) and network functional connectivity (mean z-scores) because both of these variables were normally distributed. For consistency, Kendall's correlation coefficient of this association was also calculated. The significance of coefficient coefficients was set at 0.05.
As we found a significant correlation between fatigue severity and network functional connectivity for a fatigue-related gray matter region (see the Results section), we went on to ask the ancillary question whether there were localized regions within the functional connectivity networks where functional connectivity correlated with fatigue severity. To address this question, functional connectivity maps (z-scores) from patients were correlated voxel-wise against fatigue severity (MFI-GF scores) using FSL's randomise. TFCE correction was applied with the FWE rate set at 0.05 within the mask of the reference functional connectivity map for the respective gray matter seed (excluding all lesion voxels).
Results
Clinical characteristics
Patient characteristics are shown in Table 1. MFI-GF scores ranged from 5 to 18 (scale 4–20), including 4 of 12 patients experiencing pathological fatigue (score ≥12). HADS-D scores ranged from 0 to 10 (scale 0–21), with no patient experiencing pathological depression (score ≥11). Overall, the patients had good to excellent upper limb motor function (FM-UL scores 40–60, scale 0–60) and lower limb motor function (10MWT 1.0–2.0 m/sec) with the exception of one patient with poor motor function (FM-UL score 5 and 10MWT 0.7 m/sec). Among the four patients with pathological fatigue, two had possible depression (score 8–10) and all had good motor function.
Lesion characteristics
The lesion varied across the patients in volume (Table 1) and location (Fig. 1). Normalized lesion volume correlated nonsignificantly with MFI-GF scores (Kendall's τ = 0.37, p = 0.11).
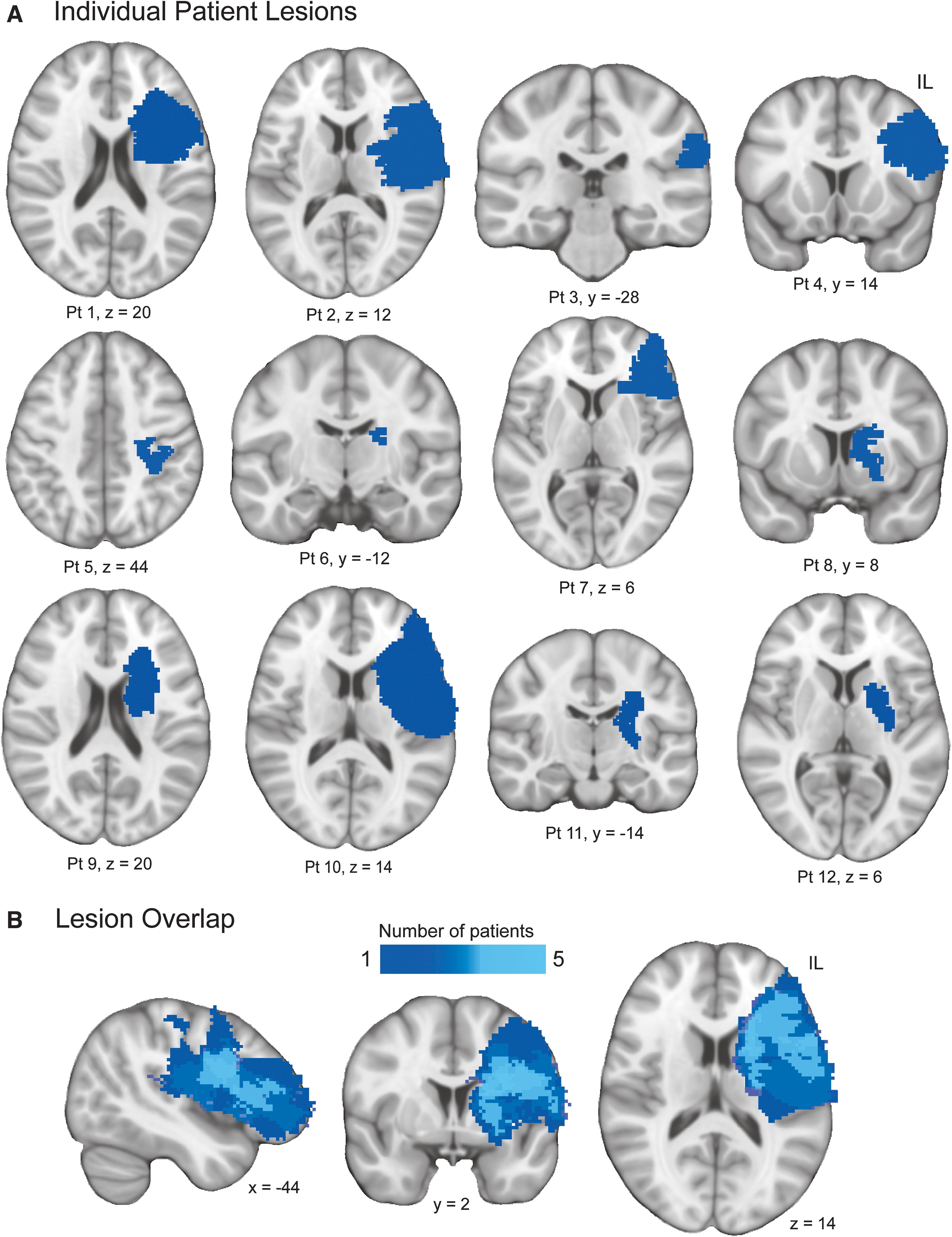
Location of stroke in MCA territory in patients. All lesions were lateralized to the same hemisphere in MNI space.
Structural disconnection
The spatial distribution and severity of gray matter disconnection, estimated by the NeMo Tool, varied across the patients (Fig. 2).
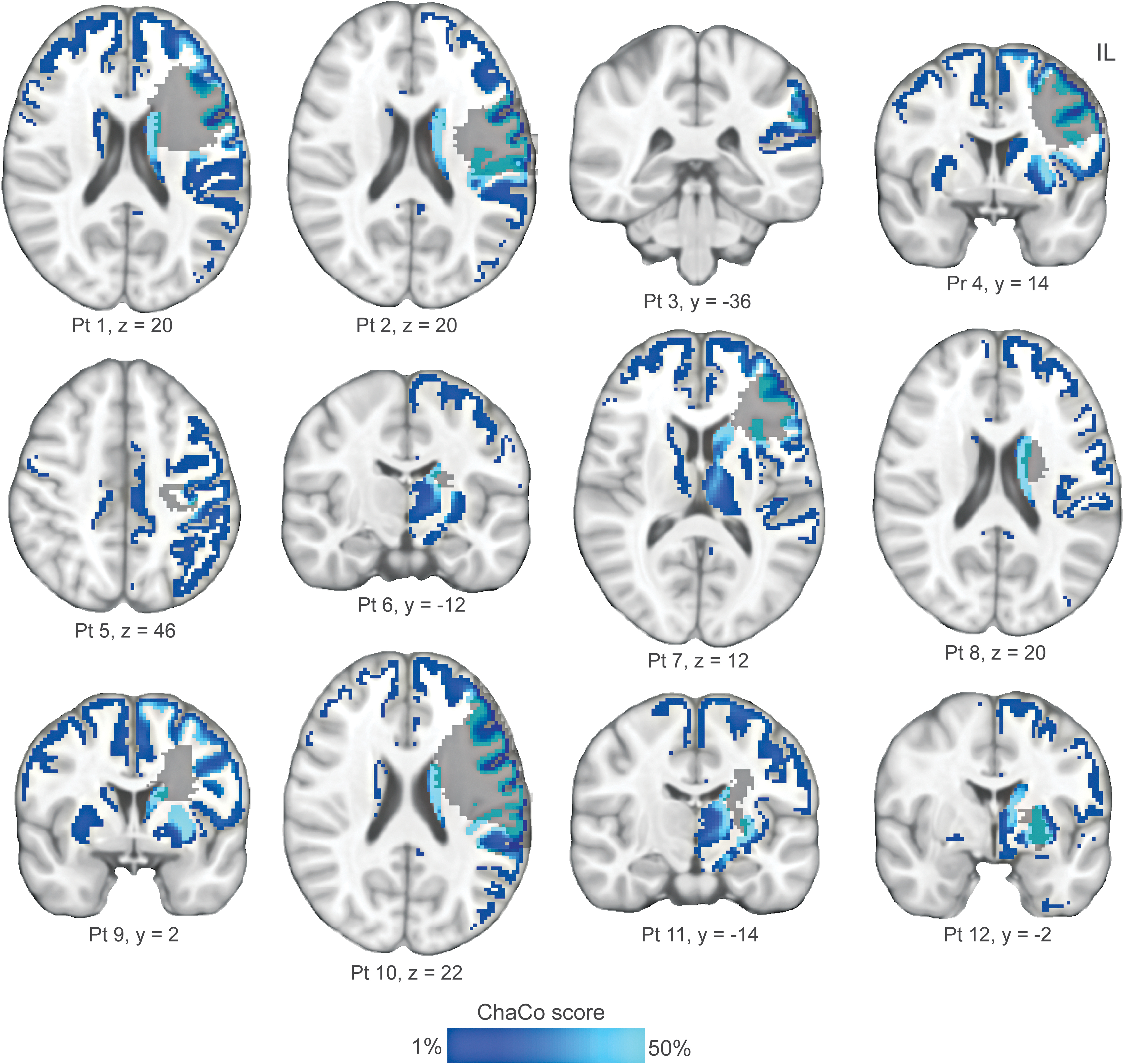
Structural disconnection in patients. Voxel-wise structural disconnection of gray matter is shown for each of the 12 patients. Each patient's lesion is also shown. For ease of visualization, ChaCo scores are displayed in the range of 1–50%. Patient numbers correspond to numbering in Table 1. ChaCo, Change in Connectivity.
Voxel-wise correlation analysis revealed that higher MFI-GF scores correlated significantly (PFWE < 0.01) with greater structural disconnection in an IL cluster and a CL cluster (Fig. 3a and Table 2). The IL cluster involved two frontal cortex regions, the rostral middle frontal cortex and superior frontal cortex, with no voxel overlapping the lesion in any patient. The CL cluster involved six frontal cortex regions—rostral middle frontal cortex, caudal middle frontal cortex, superior frontal cortex, inferior frontal cortex (pars triangularis and pars opercularis), and caudal anterior cingulate cortex. For illustrative purposes, in Figure 3b, we show the scatterplot of the relationship between fatigue severity and structural disconnection of the IL and CL rostral middle frontal cortices. This finding indicates that greater fatigue severity in patients with chronic MCA stroke is associated with greater structural disconnection of several frontal cortex regions in the IL and CL hemispheres.
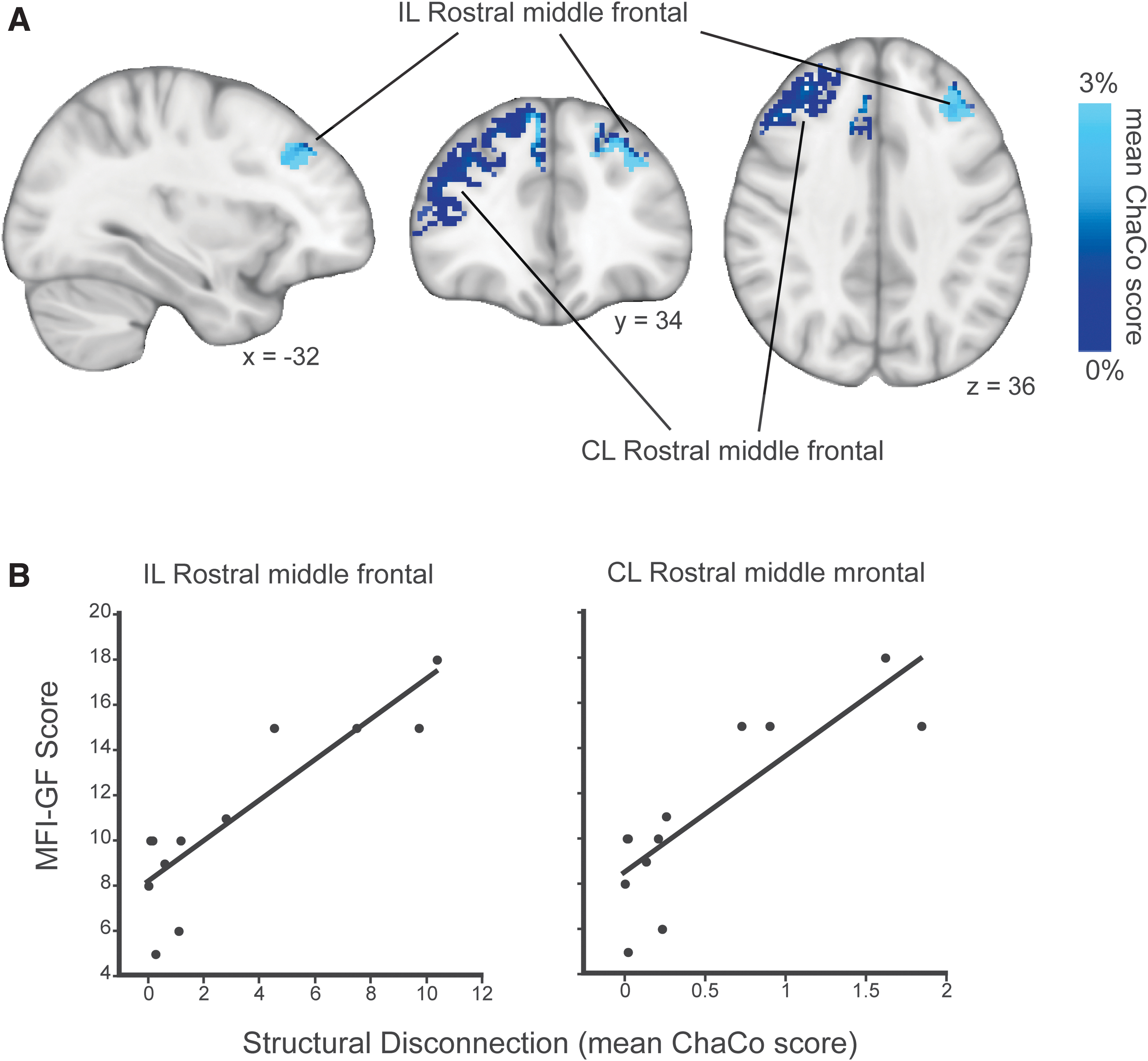
Fatigue-related structural disconnection.
Regions with Significant Structural Disconnection Correlated with Fatigue in Patients
ChaCo, Change in Connectivity; CL, contralesional; IL, ipsilesional; MNI, Montreal Neurological Institute.
No gray matter region showed greater structural disconnection correlating significantly with less fatigue severity. Also, no significant correlation was detected between fatigue severity and gray matter disconnection when the voxel-wise correlation analysis was performed using structural disconnection maps generated from lesion labels that were not lateralized to the same hemisphere in all patients (i.e., were retained in native right/left hemisphere).
Functional connectivity
Figure 4a shows an axial slice of the mean functional connectivity map from the patients for each IL and CL frontal cortex region exhibiting fatigue-related structural disconnection. The spatial pattern of each functional connectivity network was distinct, although there was substantial similarity between networks of the IL and CL rostral middle frontal cortices, and the IL and CL superior frontal cortices, as would be expected for homologous seeds. The functional connectivity networks of the two inferior frontal cortex regions in the CL hemisphere, the pars opercularis and triangularis, were also quite similar. To get a fuller picture of the functional connectivity network of the fatigue-related region in the IL rostral middle frontal cortex, Figure 4b shows several axial slices of its mean functional connectivity map.
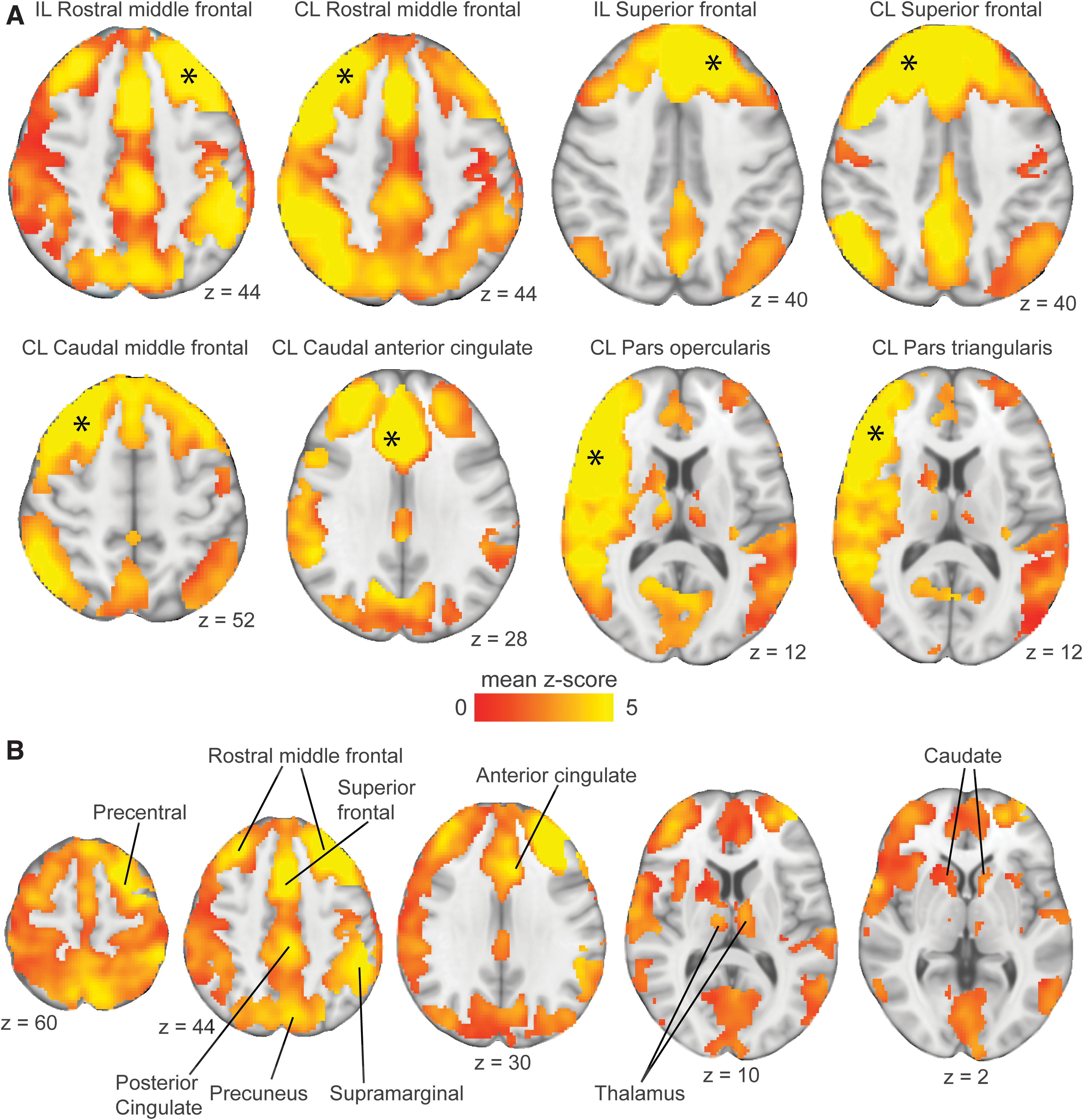
Functional connectivity of fatigue-related frontal cortex regions.
Upon testing the secondary hypothesis that structural disconnection is associated with disrupted functional connectivity, we found that greater structural disconnection of three of the eight fatigue-related frontal cortex regions trended toward correlating significantly with reduced network functional connectivity—the IL rostral middle frontal cortex (Kendall's τ = −0.36, p = 0.10), CL caudal anterior cingulate cortex (Kendall's τ = −0.39, p = 0.07), and CL pars opercularis (Kendall's τ = −0.36, p = 0.10; Fig. 5a). Among these three fatigue-related frontal cortex regions, only the IL rostral middle frontal cortex showed reduced network functional connectivity correlating significantly with greater fatigue severity (Pearson's r = −0.62, Kendall's τ = 0.51, both p < 0.05; Fig. 5b).

Relationships among disrupted structural disconnection, functional connectivity, and fatigue.
Ancillary voxel-wise correlation analyses did not detect a localized region exhibiting a significant correlation between fatigue severity and functional connectivity of any fatigue-related frontal cortex region. This finding, together with the aforementioned result, suggests that fatigue severity is associated with broad, rather than localized, disruptions in functional connectivity within the functional network of gray matter regions exhibiting fatigue-related structural disconnection.
Discussion
PSF is common among chronic stroke patients, but its etiology has been unclear. While the brain lesion has been implicated in the etiology of PSF (Naess et al., 2012; Winward et al., 2009), focal lesion characteristics such as size and location have generally not been found to be predictive of PSF. The current study sought to examine whether the secondary effects of the lesion on structural and functional connectivity in distributed brain networks play a role in PSF. The main finding of this study is that greater fatigue severity correlated significantly with greater structural disconnection of several frontal cortex regions in the IL and CL hemispheres in 12 patients with an ischemic MCA stroke incurred 1–3 years prior.
This study also demonstrated that among the frontal cortex regions with fatigue-related structural disconnection, only the IL rostral middle frontal cortex showed greater disruption in the functional connectivity network correlating significantly with fatigue severity. This study provides evidence that disruptions in structural and functional connectivity play a role in PSF after MCA stroke.
While our data suggest a role of structural disconnection of bihemispheric frontal cortical regions in PSF, they point to disruptions in the structural and functional connectivity of the IL rostral middle frontal cortex as having a central role. The severity of structural disconnection was estimated to be the highest in the IL rostral middle frontal cortex relative to all identified fatigue-related frontal cortex regions (∼1.5–13 times higher) (Table 2). The IL rostral middle frontal cortex was also among the subset of fatigue-related frontal cortex regions for which the level of disconnection trended toward a significant correlation with functional connectivity disruption, and the only fatigue-related frontal cortex region for which disruptions in functional connectivity correlated significantly with fatigue severity (Fig. 5).
The functional connectivity network of the fatigue-related IL rostral middle frontal cortex (Fig. 4b) overlaps appreciably with regions of the frontoparietal control and ventral attention cortical networks previously identified by Yeo and colleagues (2011), including regions in the lateral prefrontal cortex, supramarginal cortex, precuneus, and cingulate cortex. The frontoparietal control and ventral attention cortical networks have been posited to be involved in the cognitive control and attentional processes linked to goal-directed behavior (Corbetta et al., 2008; Seeley et al., 2007; Vincent et al., 2008). The functional connectivity network of the fatigue-related IL rostral middle frontal cortex also includes the subcortical caudate nuclei (Fig. 4b). The rostral middle frontal cortex and caudate are structures of the frontal-subcortical circuit that have been proposed to mediate executive functions involved in the planning and monitoring of task performance (Bonelli and Cummings, 2007).
Notably, acute stroke of the caudate has been reported to increase the probability of developing PSF (Tang et al., 2013). Taken together, structural disconnection of the IL rostral middle frontal cortex, leading to broad disruptions in its cortical-subcortical functional connectivity network, may impair the cognitive, attentional, and executive processes involved in goal-directed action, and be key to the development of PSF.
Our finding of fatigue-related structural disconnection after stroke differs from a recent study by Ulrichsen and associates (2021) that observed no relationship between fatigue severity and structural disconnection in patients with chronic stroke. An important distinction between the two studies is that we assumed that the structural disconnection important to PSF was independent of stroke hemisphere. The Ulrichsen and associates study, in contrast, assumed hemispheric specialization of fatigue, and thus that the structural disconnection important to PSF was dependent on stroke hemisphere. Stemming from these different assumptions, our analysis used structural disconnection maps of lesions that had been lateralized to the same hemisphere for all patients, whereas the Ulrichsen and associates study used structural disconnection maps of lesions with mixed laterality. When we repeated our analysis using structural disconnection maps of lesions in their native (mixed) laterality, we also failed to detect a significant correlation between structural disconnection and fatigue severity. Together, these studies suggest that PSF is not caused by structural disconnection of a functionally specialized gray matter region in the right or left hemisphere, but rather relates to structural disconnection of frontal cortex regions in both the IL and CL hemispheres.
Structural disconnection of IL frontal cortices likely results from damage to their IL white matter connections, whereas structural disconnection of CL frontal cortices likely results from IL damage to transcallosal pathways that have connections to CL frontal cortices. Structural damage to transcallosal pathways can occur after unilateral MCA stroke (Chen and Schlaug, 2013; Gupta et al., 2006). Gray matter disconnection resulting from lesion to interhemispheric white matter pathways has been suggested to contribute to several behavioral and cognitive deficits after stroke (Griffis et al., 2019; Kuceyeski et al., 2015, 2016).
The current study suggests that structural disconnection of frontal cortex regions due to lesion of interhemispheric white matter pathways also contributes to PSF. A recent study reported that disturbed interhemispheric connectivity between the IL and CL primary motor cortices predicts fatigue severity after stroke (Ondobaka et al., 2021). Altogether, these studies suggest that disruptions in structural and functional connectivity involving interhemispheric white matter pathways have a role in PSF.
Our finding of fatigue-related gray matter disconnections was afforded by using structural disconnection maps output by the NeMo Tool. As the NeMo Tool embeds patient lesions into a reference tractography atlas constructed from diffusion MRI data from healthy subjects, it provides an indirect measure of structural disconnection in patients. Use of the NeMo Tool or comparable software (Foulon et al., 2018; Griffis et al., 2021) that provides an indirect measure of structural disconnection avoids performing tractography on diffusion MRI data acquired from patients with brain lesions, the latter of which can be prone to errors in propagation and termination of streamlines due to the presence of white matter degeneration, tissue necrosis, and edema (Moura et al., 2019; Schilling et al., 2019). Indirect measurement of structural disconnection also avoids inaccuracies that could arise from direct measurements made using diffusion MRI data acquired from patients due to reduced quality (e.g., noise, motion).
Structural disconnection measured indirectly in patients with stroke has been shown to associate more strongly with behavioral/cognitive deficits (Hope et al., 2016; Kuceyeski et al., 2015, 2016) and functional connectivity disruptions (Griffis et al., 2019) than direct measures of the focal lesion. Similarly, we found that fatigue severity in our patients correlated significantly with gray matter disconnection measured indirectly, but only trended toward a significant correlation with total lesion volume measured directly. Our findings support the value of indirectly measuring the impact of a lesion on distributed structural networks for understanding stroke outcomes.
The current study has some limitations. First, the patient sample size was small, resulting, in part, from requiring patients to have incurred an ischemic stroke in a specific vascular territory (i.e., MCA) within a narrow window of stroke chronicity (i.e., 1–3 years), and to be free of prestroke fatigue and disability. Given that all patients had an MCA stroke, our study conclusions are not generalizable to patients with a stroke in a different cerebrovascular territory. As we lateralized the stroke in all patients to the same hemisphere to increase the statistical power of the voxel-based image analyses, our results require corroboration by a larger study that conducts analyses with all strokes in their native right and/or left hemisphere.
Among the enrolled patients, fatigue severity ranged from mild to severe, and none had severe depression, a common poststroke problem that can exacerbate PSF (Elf et al., 2016; Ingles et al., 1999). Also, no patient with severe fatigue had poor motor function, a poststroke impairment that might contribute to PSF (Hinkle et al., 2017). The stringent inclusion criteria together with clinical characteristics of the enrolled patients minimized confounding factors, and thus strengthen our attribution of frontal cortex disconnection as an important factor in PSF after MCA stroke.
A second limitation is that measurements of structural disconnection in patients were made using a reference tractography atlas constructed using diffusion MRI data from younger healthy adults (29 ± 4 years old) relative to the patients (56 ± 12 years old). This age difference could affect estimates of structural disconnection in the patients because white matter generally undergoes age-dependent loss in microstructural integrity (Isaac Tseng et al., 2021) due, in part, to increased impact of cerebrovascular risk factors (Kennedy and Raz, 2009). Given this age difference, our findings await corroboration by studies using a reference tractography atlas constructed from data acquired from older adults. Nonetheless, structural disconnection measurements are normalized estimates, which allowed us to test the impact of the stroke lesion on fatigue severity without the potential confound of differences in white matter integrity across patients that might exist due to differences in their age and severity of cerebrovascular risk factors.
A third limitation stems from the known propensity of false-positive connections of tractography streamlines (Tournier, 2019), which could lead in turn to a reference tractography atlas that includes inaccurate structural connectivity, inaccurate estimates of structural disconnection, and inaccurate localization of fatigue-related structural disconnection. However, these inaccuracies were minimized by the reference tractography atlas used by the NeMo Tool, which utilized diffusion MRI data acquired using state-of-the-art technologies (Van Essen et al., 2012) and analyzed using state-of-the-art approaches, including multishell, multitissue constrained spherical deconvolution (Jeurissen et al., 2014) and probabilistic tractography implemented with iFOD2 (Tournier et al., 2012) and anatomical constraint (Smith et al., 2012). Some prior studies have dealt with the possibility of false-positive connections in the reference tractography atlas by ignoring low-level disconnections (e.g., ChaCo scores <1%) (Griffis et al., 2019; Kuceyeski et al., 2014).
The current study opted to not ignore low-level disconnections in patients, yet to apply a conservative statistical threshold (PFWE < 0.01) to identify gray matter exhibiting structural disconnection related to fatigue severity. Nonetheless, it is possible that the breadth of frontal cortex regions with low-level structural disconnection identified as being related to fatigue was overestimated, such as those in the CL hemisphere. However, our retention of low-level structural disconnections does not affect the overall finding that structural disconnection of frontal cortex regions relates to PSF, and that disconnection of the IL rostral middle frontal cortex may play a central role via its broad impact on functional connectivity.
In conclusion, this study provides evidence that PSF after MCA stroke relates to structural disconnection and disruption in functional connectivity of bihemispheric frontal cortex regions. Future studies with a large patient cohort will be required to better understand the relationship between frontal cortex disconnection and functional connectivity disruption in PSF, including the possibility that functional connectivity disruption mediates the impact of frontal cortex disconnection on fatigue severity.
Footnotes
Acknowledgments
The authors thank Grae Arabasz, Shirley Hsu, Regan Butterfield, Kelly Anne Castro-Blanco, Amy Kendall, Natacha Nortelus, David Lin, and Julie DiCarlo for their help in this project.
Authors' Contributions
J.D.S.—conceptualization, methodology, software, formal analysis, investigation, writing: original draft, visualization, supervision, project administration, and funding acquisition; M.L.L.—conceptualization, writing: review and editing, supervision, funding acquisition, and investigation; M.K.—software, investigation, and writing: review and editing; B.G.H.—software, investigation, and writing: review and editing; T.R.—resources and data curation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The following grants provided financial support to conduct this research: 1R21-NS110982-01 (J.D.S. and M.L.L.); DoD-W81XWH-14-1-0543 (M.L.L.); R01-NS094306-01A1 (M.L.L.); and R21-NS087472-01A1 (M.L.L.).