
Abstract
Background:
The response to cholinesterase inhibitors (ChEIs) treatment is variable in patients with Alzheimer's disease (AD). Patients and physicians would benefit if these drugs could be targeted at those most likely to respond in a clinical setting. Therefore, this study aimed to evaluate the ability of cerebrospinal fluid (CSF) AD biomarkers, hippocampal volumes, and Default Mode Network functional connectivity to predict clinical response to ChEIs treatment in mild AD.
Methods:
We followed up on 39 mild AD patients using ChEIs at therapeutic doses. All subjects underwent clinical evaluation, neuropsychological assessment, magnetic resonance imaging examination, and CSF biomarkers quantification at the first assessment. The Mini-Mental Status Examination (MMSE) was used to measure the global cognitive status before and after the follow-up. “Responders” were considered as those who have remained stable or improved the MMSE score between evaluations and “Nonresponders” as those who have worsened the MMSE score. We performed univariate and multivariate logistic regressions to predict the clinical response from each biomarker.
Results:
About 35.89% of patients were classified as “Responders” to ChEIs treatment after the follow-up. The multivariate model with measures of Right Hippocampus (RHIPPO), adjusted for gender and interval between assessments, was significant (odds ratio: 1.09 [95% confidence interval, 1.00–1.19], p = 0.0392). This model achieved an accuracy of 77.60%.
Conclusion:
Our findings suggest that the functional connectivity of RHIPPO might be an early imaging biomarker to predict clinical response to ChEIs drugs in mild AD.
Impact statement
The functional connectivity of the right hippocampus showed a direct relationship with the clinical response to cholinesterase inhibitors (ChEIs) treatment in patients with mild Alzheimer's disease. Transposing our findings to clinical settings could allow physicians to prescribe ChEIs for patients for whom treatment would be most beneficial.
Introduction
Managing the clinical aspects triggered by Alzheimer's disease (AD) is a challenge. The most used drugs for symptomatic mild-to-moderate AD are cholinesterase inhibitors (ChEIs) (Kamkwalala and Newhouse, 2017). The rationale through ChEIs is the cholinergic hypothesis, which attributes part of the decline in learning and memory to the acetylcholine deficit (Hampel et al, 2018). ChEIs work by maximizing the availability of endogenous acetylcholine in the brain. However, ChEIs only slow or delay the deterioration rather than promote the retrieval of lost abilities. The average real benefit of these drugs is doubtful (Hansen et al, 2008).
The response to ChEIs therapy has been reported as heterogeneous among individuals with AD (Moreta et al, 2021). Meta-analyses of placebo-controlled data show only modest overall benefits of ChEIs for stabilizing or slowing decline in cognition, functional abilities, behavior, and clinical global change (Bond et al, 2012; Hansen et al, 2008; Tan et al, 2014). In clinical practice, about half or fewer patients treated with ChEIs show improvement in cognitive performance within time (Xu et al, 2021). Common reasons for deprescribing ChEIs are lack of response, impaired functional status, severe cognitive impairment, and significant side effects (Ruangritchankul et al, 2021). Patients' characteristics might affect the short-term clinical outcome of ChEIs treatment, and ∼7% develop adverse effects severe enough to stop the treatment (Lanctôt et al, 2003; Meng et al, 2018). Previous studies have demonstrated that higher doses of ChEIs may be more effective for AD, emerging the need for robust biomarkers that could aid in the selection of candidates responsive to ChEIs and tolerate potentially more aggressive treatment (Hampel et al, 2019; Meng et al, 2018).
The continuous use of ChEIs should be often weighed about risks and benefits. Patients and physicians would benefit if these drugs could be targeted at those most likely to respond in a clinical setting. Understanding the factors that may predict response to ChEIs is of utmost importance. We, therefore, evaluated the ability of biomarkers known to be impaired in AD, for instance: cerebrospinal fluid (CSF) biomarkers (Aβ1–42, p-Tau181, and t-Tau), hippocampal volumes (HV), and Default Mode Network functional connectivity, to predict clinical response to ChEIs treatment in mild AD.
Methods
Subjects
Thirty-nine individuals aged 60 years or older and diagnosed with mild AD were followed-up. All were using ChEIs at therapeutic doses for at least 24 weeks (donepezil 10 mg, rivastigmine 12 mg, or galantamine 24 mg), which is the minimum interval to obtain drugs' stability in the blood. The follow-up started after the stabilization of the full dose of ChEIs (first assessment). Patients were considered exposed throughout the whole follow-up period according to treatment status at the study baseline.
All patients included had a Clinical Dementia Rating (CDR) (Morris, 1993) score of 0.5 or 1.0, and the diagnosis of probable dementia owing to AD following the criteria set out by the National Institute on Aging and Alzheimer's Association (McKhann et al, 2011). Exclusion criteria included the following: another neurological or psychiatric disease, having suffered a head trauma that resulted in the loss of consciousness, drug or alcohol addiction, prior chronic exposure to neurotoxic substances, Fazekas Scale ≥2 (Fazekas et al, 1987), or Hachinski Ischemic score >4 (Hachinski et al, 2006).
CSF biomarkers analysis and magnetic resonance imaging (MRI) were performed at the first assessment. Mini-Mental Status Examination (MMSE) (Folstein et al, 1975) was utilized to measure the global cognitive status before (first assessment) and after (second assessment) the minimum interval of 6 months of follow-up. An experienced neuropsychologist, blinded to the patient's data, performed neuropsychological evaluations. “Responders” were considered as those who have remained stable or improved the MMSE score between evaluations and “Nonresponders” as those who have worsened the MMSE (have lost at least one point) score in the same circumstances. This study had a naturalistic design to mimic real life as closely as possible. Participants continued their normal lives and visited the site for the second assessment as part of their routine clinical assessment.
CSF analysis
CSF samples were collected from all participants by a lumbar puncture after fasting. No adverse events were reported. CSF (5mL) were collected in sterile polypropylene tubes, centrifuged (700 rpm × 10 min) at 4°C, aliquoted in polypropylene Eppendorfs, and stored at −80°C until analysis. AD biomarkers (Aβ1–42, p-Tau181, and t-Tau) were measured by InnoBIA AlzBio3 (Innogenetics), a multiplex microsphere-based xMAP platform that allows the simultaneous analysis of the three biomarkers. The laboratory technician was blinded to any data about the participants.
Image acquisitions
MRI images were acquired on a Philips® Achieva 3.0-T MRI scanner. A protocol with three steps was applied for each participant: (1) a sagittal high-resolution T1-weighted was used to calculate the HV. Parameters used were as follows: isotropic voxels of 1 × 1 × 1 mm3, repetition time (TR)/ echo time (TE) = 7/3.2 msec field-of-view (FOV) = 240 × 240 mm2, 180 slices; (2) to calculate the functional connectivity echo planar images (EPI) were used, TR/TE = 2000/30 msec, FOV = 240 × 240 mm2, isotropic voxels set to 3 × 3 × 3 mm3, no gap with a total scan time of 6 min, resulting in 180 full brain volumes with 40 axial slices each. Participants were instructed to keep their eyes closed, to be relaxed, to move as little as possible, and to not fall asleep; (3) to exclude vascular diseases: coronal and axial fluid-attenuated inversion recovery T2-weighted images, anatomically aligned at the hippocampus with image parameters set to TR/TE/TI (inversion time) = 12,000/140/2850, FOV = 220 × 206, voxels reconstructed to 0.45 × 0.45 × 4.00 mm3, and the gap between slices set to 1 mm.
Functional connectivity analyses
The UF2C toolbox was used to perform the functional connectivity analyses. This software runs in the MATLAB platform (The Math Works, Inc., USA) with SPM12.
Functional MRI (fMRI) volume realignment (using the mean image as a reference), image co-registration (fMRI mean image with T1-weighted image), spatial normalization (MNI-152), smoothing (kernel of 6 × 6 × 6 mm3 at FWHM) and T1-weighted image tissue segmentation, and normalization (MNI-152) were used to perform the preprocessing. In addition, six head motion parameters (three rotational and three translational) as well as white matter and CSF average signals were regressed out. Finally, linear trends were removed, and the time series bandpass filtered (0.008–0.1 Hz).
The individual DMN maps were created based on the time series of a seed (10 × 10 × 10 mm3) positioned in the posterior cingulated cortex (PCC) and applied to compute the voxel-wise connectivity using Pearson's correlation. We used a DMN template, previously created and published, to extract average connectivity values exclusively from DMN regions (Weiler et al, 2014).
In brief, the template was created by averaging the control subject's connectivity maps (using PCC as seed), binarizing (excluding all voxels with a correlation score lower than 0.2), and dividing supra-threshold clusters (parceled into regions with continuous voxels), resulting in the eight main DMN ROIs: the prefrontal cortex (FRONT), PCC, left parietal lobe (LPARIETO), right parietal lobe (RPARIETO), right temporal lobe (RTEMP), left temporal lobe (LTEMP), left hippocampus (LHIPPO), and right hippocampus (RHIPPO). The DMN ROIs were used to mask each individual's r-score map, extracting an average connectivity value (respective to the original seed definition: PCC) for each of the eight regions. The eight individual averaged values were converted to z-scores (Fisher's z-transformation) and were used for statistical analysis.
HV assessment
To perform cortical surface reconstruction and the anatomical segmentation of MRI brain scans, the FreeSurfer software v.5.3 was used. High-resolution T1-weighted MR volumetric images were processed through the default FreeSurfer processing stages to perform nonlinear registration (warping) from the original space to the MNI305 space (standard space), cortical thickness measurements, and cortical and subcortical segmentations. For smooth brain surface, a Gaussian filter with a kernel of 10-mm full width at half maximum was used in all analyses. Individual structure volumes were computed from labeled voxels and normalized to the total intracranial volume. To avoid the presence of macroscopic artifacts, we visually confirmed the accuracy of warping the T1-weighted MR volumetric images to the standard space.
Statistical analysis
Descriptive analyses between groups were presented as mean and standard deviation for quantitative variables and as frequencies for categorical variables. Univariate and multivariate logistic regression models were performed. The ChEIs response was the dependent variable. Multivariate logistic regression models were performed on each biomarker and adjusted for gender and the interval between assessments. Values of p < 0.05 were considered significant. All analyses were performed on Software R Core Team (2020), and the SAS System for Windows (version 9.4, 2002-2012).
Ethical aspects
This study was approved by the local research ethics of the University of Campinas and followed the Declaration of Helsinki. All participants or their legally authorized representative gave their written consent to participate.
Results
At the end of follow-up, 14 of 39 (35.89%) patients remained stable or improved the MMSE score and were classified as “Responders.” Table 1 provides the descriptive data of both groups, “Responders” and “Nonresponders,” besides the univariate and multivariate logistic regression results.
Descriptive Data Between Groups and Logistic Regression Analyses
Data are given as mean (standard deviation). Multivariate models were corrected by gender and the interval between assessments. Reference category: responsive to ChEIs. * p < 0.05 was considered significant. OR to an increment of 100 U.
Aβ1–42, amyloid-beta protein; CI, confidence interval; FRONT, prefrontal cortex; LHIPPO, left hippocampus; LPARIETO, left parietal lobe; LTEMP, left temporal lobe; MMSE, Mini-Mental Status Examination; OR, odds ratio; p-Tau181, phosphorylated Tau; PCC, posterior cingulate cortex; RHIPPO, right hippocampus; RPARIETO, right parietal lobe; RTEMP, right temporal lobe; t-Tau, total Tau.
Univariate logistic regression models for age, education, gender, and the interval between assessments have not reached statistical significance (Table 1). However, all the multivariate analyses were corrected for gender (almost significant in the univariate model) and the interval between assessments (relevant to this specific study). Age and education, although relevant to AD, were relatively homogenous in our sample.
Multivariate logistic regressions for each biomarker were performed (Table 1). Only the measure of RHIPPO was significant to the clinical response to ChEIs treatment in mild AD (odds ratio [OR]: 1.09 [95% confidence interval, 1.00–1.19], p = 0.0392). This model achieved an accuracy of 77.60%.
Figure 1 provides all the DMN subregions included and highlights the RHIPPO, the only subregion with statistical significance in the multivariate logistic regression model.
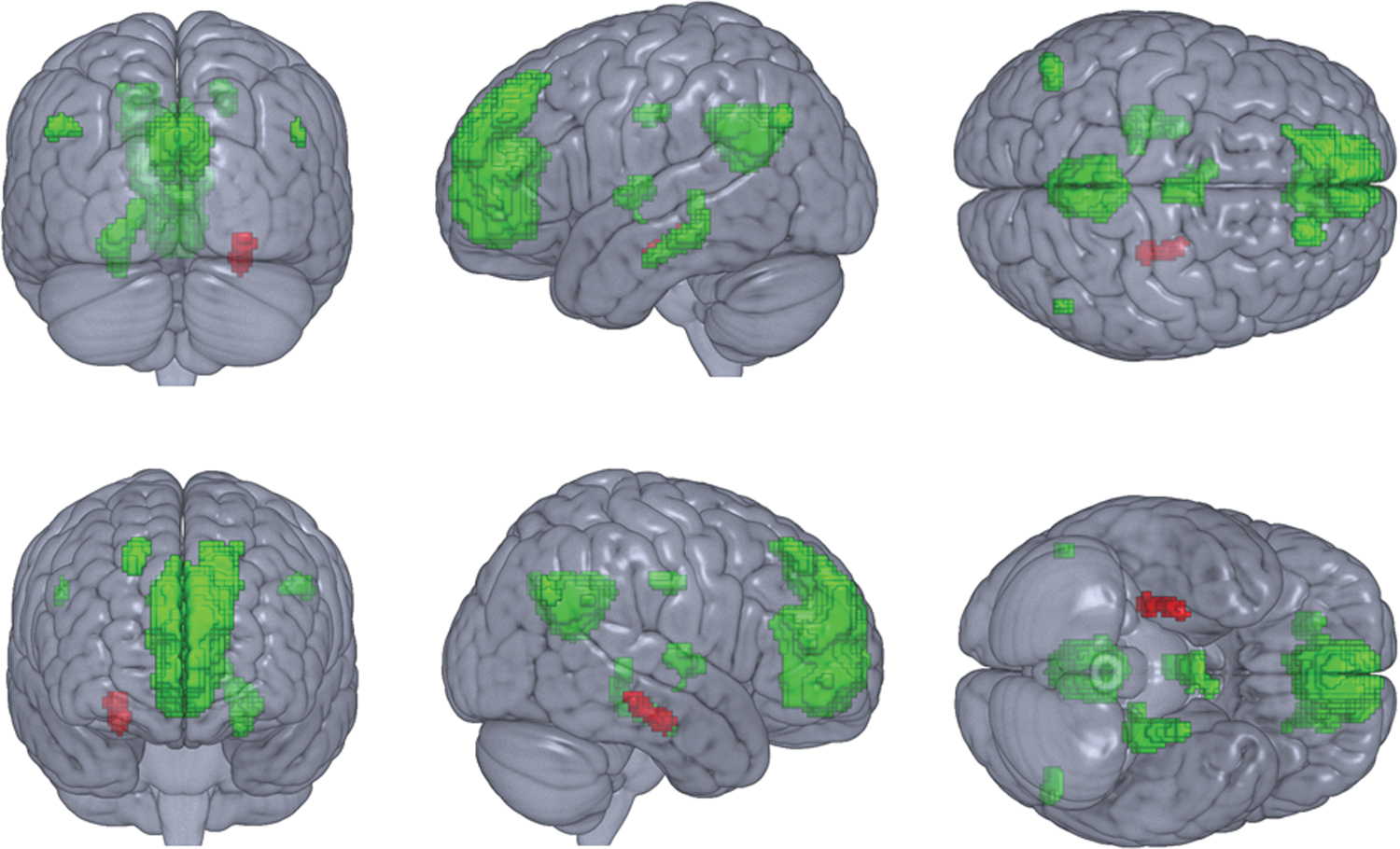
DMN subregions. The subregion in red color is the RHIPPO, with statistical significance in the multivariate logistic regression model, showing a direct relationship with the response to the ChEI drugs. All DMN subregions in green color did not present statistical significance. ChEI, cholinesterase inhibitor; DMN, default mode network; RHIPPO, right hippocampus.
Discussion
Approximately 35.8% of the mild AD patients assessed in this study remained stable or improved their global cognitive status after follow-up. The stability verified on MMSE may be attributed, at least partly, to the use of ChEI drugs. ChEIs are the most used drugs for symptomatic AD, owing to pieces of evidence of their effectiveness for improving cognition, behavior, and functional abilities when compared with untreated groups (Kamkwalala and Newhouse, 2017; Xu et al, 2021). However, studies have shown that only ∼40% of people who take these drugs have a good response in cognition (Ohnishi et al, 2014; Xu et al, 2021), which is in agreement with our follow-up study.
In our study, the connectivity of the RHIPPO showed a direct relationship with the response to ChEI drugs, predicting response to treatment. This result is of utmost importance because it is extremely difficult to predict in advance who will respond to ChEIs. The functional connectivity of RHIPPO could be a potentially useful biomarker to identify patients who would benefit from ChEIs to improve the treatment effectiveness for mild AD.
Brain functional connectivity has several advantages to potential clinical use outstanding its noninvasive nature (Hohenfeld et al, 2018). No exogenous contrast or radioactive tracer needs to be administered, relieving patients of the need for intravenous access or radiation exposure (Friston, 2011). However, the patterns underlying functional connectivity in AD remain poorly understood (Xue et al, 2019). Impairments in memory and cognitive decline in AD have been explained by disruptions to the functional connection of resting-state networks (Sohn et al, 2014). Whereas the hippocampus is the foremost brain region associated with learning and memory, changes in hippocampal functional connectivity are of particular interest (Xue et al, 2019). The significant contribution of the RHIPPO functional connectivity verified in our model might support a compensatory recruitment hypothesis (Agosta et al, 2012). We hypothesize that the RHIPPO functional connectivity might actively recruit additional neural resources to compensate for the declines in cognitive function, being a target to the action of ChEI drugs.
Supporting this, Sohn et al (2014) studied the functional connectivity in different brain regions in AD progression. They verified not a progressive loss of connectivity but a dynamics of deterioration and compensation. The decrease in functional connectivity might represent a deterioration of neural networks by the loss or weakening of synaptic connection and neuronal degeneration, whereas the increase might reflect the recruitment of resources to compensate for the neuronal loss or the breakdown of networks (Sohn et al, 2014).
Likewise, Dumas and Newhouse (2011) have proposed a cholinergic functional compensation model for age-related cognitive dysfunction. In this model, functional compensation recruits the cholinergic system to maintain good performance. Therefore, regional compensatory synaptic mechanisms could be stimulated by higher brain activity (Aganj et al, 2020). However, this mechanism works to a certain extent (Dumas and Newhouse, 2011). It has been observed that there is an asymmetry between left and right hemisphere networks (Daianu et al, 2013). Although hemispheric changes in functional connectivity are not well established, the left hemisphere seems to be the first and more severely affected in AD, being less susceptible to compensatory mechanisms (Sohn et al, 2014).
The most likely explanation for our results is that the functional connectivity of RHIPPO could be a target to the action of ChEI drugs, attempting to increase the cholinergic synaptic transmission and, consequently, improve cognitive performance. For this reason, patients with mild AD with increased functional connectivity at RHIPPO responded better to the treatment with ChEIs. However, further research with larger samples is needed to confirm this hypothesis.
We acknowledge some limitations. First is our relatively small sample size; thus, future larger studies are encouraged. Second, we have not evaluated the three available ChEI drugs separately. Third, regarding the observational study design, we cannot infer causality, and we acknowledge the possibility of residual or unknown confounding. Fourth, we did not assess the apolipoprotein E genotype. Finally, our data were collected in real-world clinical practice, not in a double-blind controlled study. The strengths of our study include that we have attempted to mimic the intention-to-treat to ensure a conservative estimate of the effects of ChEIs on cognition. In addition, blinded persons using validated methods conducted the biomarkers measures, MRI analyses, and cognitive tests.
In summary, our findings suggest that the RHIPPO functional connectivity might be an early imaging biomarker to predict clinical response to ChEI drugs in mild AD. The present findings may have important clinical implications, allowing physicians to prescribe ChEIs for preselected mild AD patients for whom treatment would be most beneficial. Future studies to test our compensatory recruitment hypothesis are encouraged.
Footnotes
Acknowledgment
The authors thank BRAINN—Brazilian Institute of Neuroscience and Neurotechnology.
Authors' Contributions
L.R.: Conceptualization, investigation, writing—original draft, visualization; T.N.C.M.: Investigation, methodology, software, formal analysis; N.L.: Conceptualization, software, investigation; A.S.M.: Methodology, software; R.F.C.: Software; C.V.L.T.: Investigation; B.M.d.C.: Software; T.J.R.d.R.: Software; L.L.T.: Software; O.V.F.: Software, resources; F.C.: Software, resources; M.L.F.B.: Conceptualization, supervision, resources, writing—review and editing, Project administration, funding acquisition. All authors have critically revised the article for intellectual content and approved the final version of the article for submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from São Paulo Research Foundation (FAPESP), Brazil (Grants Nos. 18/15571-7, 18/06055-5, 19/23028-4). The study funders had no role in study design, data collection, data analysis, data interpretation, writing of the report, or the decision to submit for publication.