
Abstract
Background:
The emergence of COVID-19 was rapidly followed by infection and the deaths of millions of people across the globe. With much of the research and scientific advancement rightly focused on reducing the burden of severe and critical acute COVID-19 infection, the long-term effects endured by those who survived the acute infection has been previously overlooked. Now, an appreciation for the post-COVID-19 condition, including its neurological manifestations, is growing, although there remain many unknowns regarding the etiology and risk factors of the condition, as well as how to effectively diagnose and treat it.
Methods:
Here, drawing upon the experiences and expertise of the clinicians and academics of the European working group on COVID-19, we have reviewed the current literature to provide a comprehensive overview of the neurological sequalae of the post-COVID-19 condition.
Results:
In this review, we provide a summary of the neurological symptoms associated with the post-COVID-19 condition, before discussing the possible mechanisms which may underly and manifest these symptoms. Following this, we explore the risk factors for developing neurological symptoms as a result of COVID-19 and the post-COVID-19 condition, as well as how COVID-19 infection may itself be a risk factor for the development of neurological disease in the future. Lastly, we evaluate how the post-COVID condition could be accurately diagnosed and effectively treated, including examples of the current guidelines, clinical outcomes, and tools that have been developed to aid in this process, as well as addressing the protection provided by COVID-19 vaccines against the post-COVID-19 condition.
Conclusions:
Overall, this review provides a comprehensive overview of the neurological sequalae of the post-COVID-19 condition.
Impact statement
With our understanding of the neurological complications of the post-COVID-19 condition currently lacking sufficient depth, this review aimed at highlighting the current knowns and unknowns of the post-COVID-19 condition. In this review, we draw upon the experiences and expertise of the clinicians and academics of the European working group on COVID-19, as well as explore the current published literature, to evaluate a range of topics associated with the neurological complications of the post-COVID-19 condition. As a result, we have provided a comprehensive review of the topic.
The European Working Group on SARS-CoV-2
Many essential questions surrounding COVID-19 remain unanswered, including its neurological complications and associated sequalae. In this review, we aim at identifying the current gaps in our understanding of post-COVID-19 neurological sequalae and suggest how future studies should be undertaken to fill these gaps. This review will draw upon the current biological and mechanistic understanding of COVID-19 and post-COVID-19 complications to discuss the clinically relevant aspects associated with the neurological manifestations of post-COVID-19 syndrome.
From our discussions, the following questions were considered highly relevant for contemplation:
What are the neurological syndromes associated with the post-COVID-19 condition and the pathological mechanisms underlying neurological symptoms and signs?
How are those with pre-existing neurological disorders affected by the post-COVID-19 condition?
How do the neurological complications associated with the post-COVID-19 condition affect long-term disability and quality of life?
Can we identify risk factors for developing the post-COVID-19 condition and, specifically, how do COVID-19 strains affect risk for the development of neurological disorders in the future?
Can the post-COVID-19 condition be accurately and rapidly diagnosed?
How should we treat the neurological symptoms of the post-COVID-19 condition?
Introduction
COVID-19 and the post-COVID-19 condition
T
Acute COVID-19 can be diagnosed by direct SARS-CoV-2 detection with nucleic acid amplification tests during infection, by antigen testing, by serology to identify prior infection, or by clinical diagnosis where it is reasonable to assume the patient has/had COVID-19 (Caliendo and Hanson, 2022). Although the majority of acute COVID-19 cases manifest in mild to moderate symptoms (Bliddal et al, 2021; Grant et al, 2020), disease severity can be extremely variable, ranging from asymptomatic to fatal (Kronbichler et al, 2020; Pijls et al, 2021). Acute COVID-19 is usually defined as lasting for <4 weeks (Datta et al, 2020).
Although most studies have defined the late sequelae associated with SARS-CoV-2 infection as those occurring after at least 4 weeks since the initial infection, many definitions of the long-term condition that can develop in some COVID-19 survivors have been proposed.
One of the first terms coined to define this condition was “long COVID,” a patient made term that gained traction in the early stages of the pandemic (Callard and Perego, 2021; Perego et al, 2020). Ever since, many terms have been used to identify this long-term condition, including post-COVID-19 syndrome, post-acute COVID-19 syndrome, post-acute sequelae of SARS-CoV-2, acute post-COVID symptoms, long post-COVID symptoms, persistent post-COVID symptoms, and post-COVID-19 condition.
These terms and their definitions are outlined in Supplementary Table S1. On behalf of the WHO Clinical Case Definition Working Group on post-COVID-19 condition, a team utilized the Delphi consensus method to develop a definition of the post-COVID-19 condition that could be widely used (Soriano et al, 2022). This method resulted in 12 domains achieving consensus by the participants, and the following definition of “post-COVID-19 condition” was published: Post COVID-19 condition occurs in individuals with a history of probable or confirmed SARSCoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include fatigue, shortness of breath, cognitive dysfunction but also others and generally have an impact on everyday functioning. Symptoms may be new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms may also fluctuate or relapse over time.
The US Centers for Disease Control and Prevention (CDC) also use the term “post-COVID-19 condition” to describe the wide range of new, returning, or ongoing health complications that patients can experience 4 or more weeks after initial SARS-CoV-2 infection (CDC, 2021a). Herein, we will use the WHO definition of post-COVID-19 condition when referring to the symptoms associated with the long-term effects of COVID-19.
The neurological symptoms associated with the post-COVID-19 condition
Neurological symptoms of acute COVID-19 that could have long-term impacts
Acute SARS-CoV-2 infection is associated with a myriad of neurological manifestations, ranging from non-specific symptoms to well-defined neurological, psychiatric, or cognitive disorders (Ellul et al, 2020). Neurological symptoms of acute COVID-19 include headache, nausea, dizziness, fatigue, generalized exhaustion, anorexia, lack of concentration, attention deficits, and impairment of sleep (Lechien et al, 2020; Mao et al, 2020; Wang et al, 2020). Further, para-infectious or critical-illness related neurological disorders, including delirium, new onset of seizure, confusion, encephalopathy, reduced level of consciousness, or psychiatric features, can present during the acute phase of COVID-19 (de Erausquin et al, 2021; Hosseini et al, 2020; Rogers et al, 2021).
A variety of pathological mechanisms, including neuronal damage, systemic inflammation, neuroinflammation, hypoxia, and altered blood–brain barrier (BBB) dynamics, may result in the development of neurological symptoms during COVID-19. In severe cases, a cytokine storm can manifest (Jiang et al, 2022), characterized by the excessive production of inflammatory cytokines that can exert deleterious effects within the central nervous system (CNS) (Balcioglu et al, 2020). Acute COVID-19 patients may also exhibit a pro-thrombotic state (Franchini et al, 2020; Paterson et al, 2020), which may result in cerebrovascular events, including those of a thromboembolic and/or hemorrhagic nature (Nannoni et al, 2021; Parauda et al, 2020; Sluis et al, 2021).
Moreover, patients with acute COVID-19 can have significant hypoxia, even in pauci-symptomatic individuals (Brouqui et al, 2021; Simonson et al, 2021). Acute neuroinflammatory disorders (Chou et al, 2021), cranial neuropathies, dysautonomia (Ghosh et al, 2020; Goodman et al, 2021), dysfunctions of smell and/or taste (Lee et al, 2020; Parma et al, 2020), nerve root and plexus disorders (Guerrero et al, 2021), immune-mediated myopathy (Aschman et al, 2021), para- or post-viral rhabdomyolysis (Hannah et al, 2021; Haroun et al, 2021), and myositis (Hannah et al, 2021) can manifest during the acute stages of COVID-19.
The acute neurological impacts of COVID-19 are now well appreciated through the lived experience of patients and clinicians alike. Conversely, numerous questions remain with regards to the long-term neurological complications of COVID-19.
Neurological symptoms of post-COVID-19 condition
The post-COVID-19 condition is associated with a range of neurological manifestations. Frequently reported symptoms include impairments of smell and taste (Fjaeldstad, 2020; ONS, 2021; Otte et al, 2020; Paderno et al, 2020), headache (Boesl et al, 2021; Fernandez-de-Las-Penas et al, 2021a), and fatigue (Arnold et al, 2021a; Dennis et al, 2021; Goertz et al, 2020; Mandal et al, 2021). Autonomic dysfunction has also been implicated in the post-COVID-19 condition, specifically orthostatic intolerance syndromes, including orthostatic hypotension, vasovagal syncope, and postural orthostatic tachycardia syndrome (POTS) can occur (Blitshteyn and Whitelaw, 2021; Buoite Stella et al, 2022; Dani et al, 2021).
Cerebrovascular manifestations are also reported (Huang et al, 2021; Kamal et al, 2021) and are more likely to occur in individuals at high risk of cardiovascular complications. In convalescent COVID-19 patients, the incidence of acute ischemic stroke has been found to be more than double that of a matched, historical cohort (Tu et al, 2021). Stroke itself, meanwhile, can have profound long-term effects on cognition, anxiety, and depression, as well as increase the risk of further complications, including seizures, recurrent stroke, and mortality (Singh et al, 2018).
Another phenomenon of the post-COVID-19 condition is diminished cognition, with “brain fog,” a commonly used term to describe self-reports of impaired concentration or mental abilities (Asadi-Pooya et al, 2022). Objective cognitive impairment after SARS-CoV-2 infection has been found in both those hospitalized for acute COVID-19 (Frontera et al, 2021; Mazza et al, 2021; Savarraj et al, 2020; Tomasoni et al, 2021) and those who developed only mild illness (Del Brutto et al, 2021; Woo et al, 2020).
The risk of developing cognitive impairment varies with disease severity, with persistent impairments especially prevalent in patients who developed neurological complications during hospitalization (Hosp et al, 2021; Ortelli et al, 2021). However, in hospitalized patients, the risk of late cognitive sequalae is not clearly related to the severity of the acute illness (van den Borst et al, 2021). Impairments mostly affect attention, episodic and working memory, as well as visuospatial and executive functions, whereas orientation and language are usually spared, and psychomotor speed is inconsistently affected (Beaud et al, 2021; Crivelli et al, 2022; Hosp et al, 2021; Ortelli et al, 2021).
COVID-19 survivors with persisting neurological sequalae usually exhibit deficits in tasks probing recognition memory and speeded visual detection, in the absence of broader cognitive deficits (Zhao et al, 2022). This profile of cognitive impairment mirrors neuroimaging data, showing diminished cortical glucose metabolism in regions belonging to the Default Mode and Cognitive Control Networks (Hosp et al, 2021).
Many of the neurological symptoms associated with the post-COVID-19 condition are analogous to those observed in patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and, therefore, possibly have shared etiologies (Sukocheva et al, 2022). Some consequences, however, such as olfactory/gustatory dysfunction, vascular complications, and the effects of hypoxia, are specific to the post-COVID-19 condition.
The exact underlying mechanisms of post-COVID-19 neurological symptoms, therefore, require elucidation, a process that may also allow for insight into the mechanisms involved in ME/CFS. It is worth noting that since the development and rollout of COVID-19 vaccines, studies have identified the protective effects of vaccination against the post-COVID-19 condition, which is discussed further in COVID-19 Vaccination section. Whether vaccination protects against the development of specific post-COVID-19 symptoms remains to be seen.
Table 1 details studies reporting the prevalence of common symptoms of the post-COVID-19 condition. Gaining a full understanding of the spectrum of post-COVID-19 condition symptoms, and whether any of these form into clusters of related symptoms, is fundamental for both future research and clinical management of patients.
Neurological Symptoms of the Post-COVID-19 Condition and Their Estimated Prevalence
POTS, postural orthostatic tachycardia syndrome.
Neurological Complications of the Post-COVID-19 Condition
Possible mechanisms underlying the neurological symptoms of post-COVID-19 condition
Numerous possible mechanisms, including various combinations, may result in the development of the neurological symptoms of post-COVID-19 condition. These mechanisms are discussed here and summarized in Figure 1.
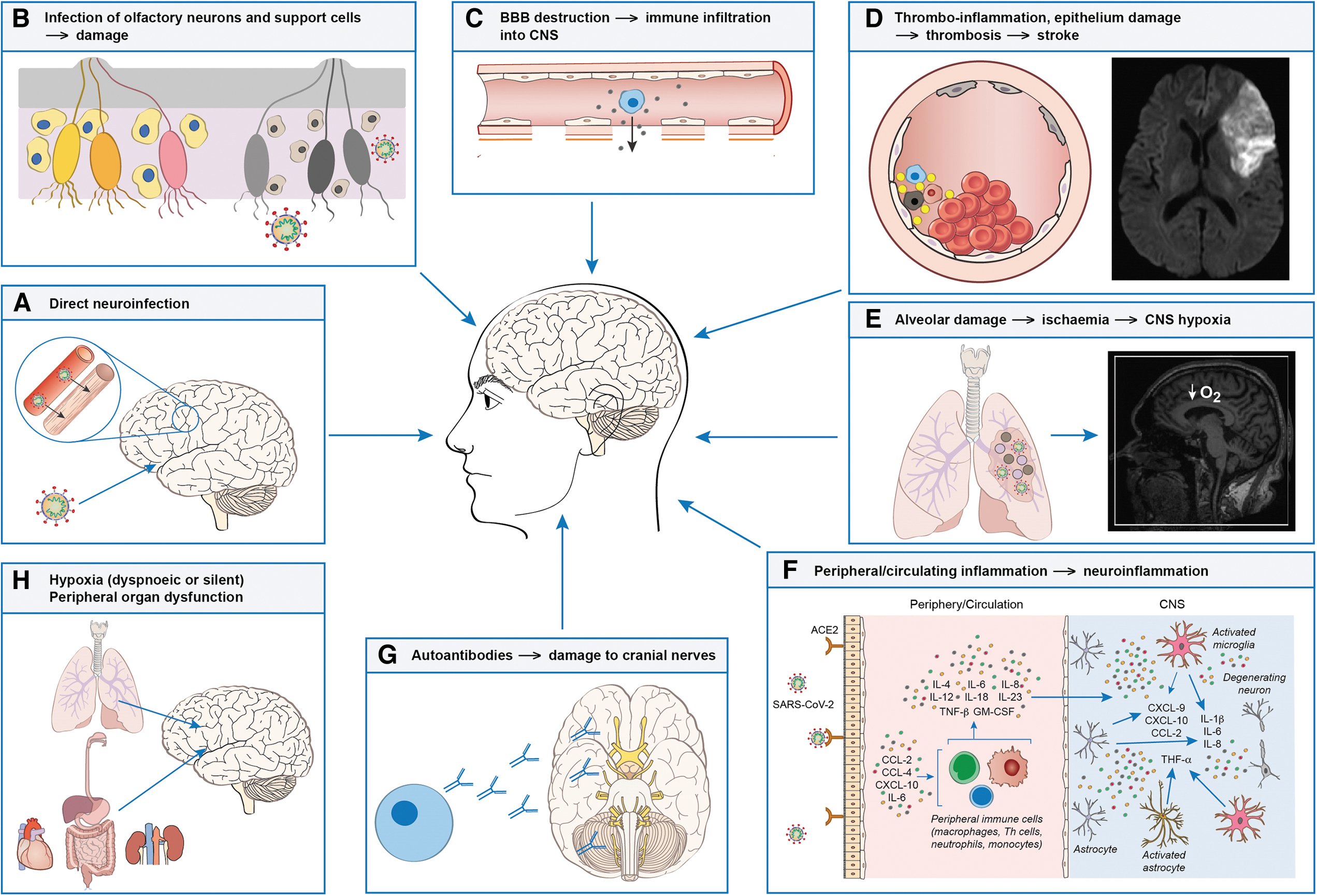
The proposed wide-ranging effects of SARS-CoV-2 on the CNS. Current research suggests that several pathological mechanisms may occur in the CNS either during or after SARS-CoV-2 infection, including:
Direct infection
The SARS-CoV-2 virus can infect the CNS through numerous routes. First, the transolfactory route of neuroinvasion, whereby SARS-CoV-2 directly infects the brain via olfactory nerves, primarily results in damage to these neurons, causing olfactory impairment (Meinhardt et al, 2021; Vavougios, 2020). Olfactory nerve infiltration by SARS-CoV-2 was noticeable among the first neuropathological studies of COVID-19 (Solomon et al, 2020). Further, extensive inflammation has been found in the olfactory bulb and medulla oblongata (Matschke et al, 2020), which may contribute to olfactory impairment.
Non-neuronal expression of the angiotensin-converting enzyme 2 (ACE2) receptor may also provide a route of infection for SARS-CoV-2 to infect olfactory support cells, stem cells, and perivascular cells, altering local water and ionic balance, resulting in an indirect reduction of sensory neuronal signaling to the brain (Brann et al, 2020). Further, although the olfactory epithelium can regenerate, the regenerative process rarely completes fully after viral infection (Yamagishi et al, 1988) and damage can be cumulative, resulting in an increased pathogenic epithelial vulnerability in later life (Doty et al, 2011).
It is likely that a combination of these mechanisms drives the long-term olfactory dysfunction seen in many COVID-19 survivors. It is suggested that damage to olfactory neurons and support cells may also contribute to post-COVID-19 fatigue by increasing resistance to cerebrospinal fluid (CSF) drainage through the cribriform plate and subsequently congesting the glymphatic system (Wostyn, 2021).
Direct infection through olfactory routes could provide SARS-CoV-2 with access to the limbic system and frontal cortex, as clinical and neuroimaging findings may suggest (Douaud et al, 2022; Lu et al, 2020). Indeed, SARS-CoV-2 viral particles have been detected in the frontal lobe of post-mortem patients infected with SARS-CoV-2 (Paniz-Mondolfi et al, 2020), indicating that the virus can directly infect the brain. Although the ACE2 receptor is expressed in the CNS on vascular endothelium cells (Bhatnagar et al, 2021), whether this receptor is expressed by neurons or glia, and whether neuronal infection by SARS-CoV-2 occurs, is controversially discussed (Khan and Gomes, 2020; Liang and Wang, 2021).
This may cast doubt onto the ability of SARS-CoV-2 to replicate and spread within the CNS. Conforming with the suggestion that SARS-CoV-2 related damage may propagate along functionally associated brain systems, neuroimaging studies have reported hypometabolism in the frontal cortex, temporal lobe, amygdala, and brainstem in patients with post-COVID-19 condition (Delorme et al, 2020; Guedj et al, 2021). These limbic region-associated changes highlight how SARS-CoV-2 may cause damage and dysfunction to pathways through direct infection of olfactory neurons and subsequent spread throughout the brain.
One study observed a greater reduction in total brain size and larger cognitive decline in those who had COVID-19 at 141 days after infection, compared with uninfected controls (Douaud et al, 2022), emphasizing the profound effect that COVID-19 can have on the brain.
The associations between olfactory dysfunction and cognition may also be prominent, with “mental clouding” suggested to negatively affect the identification and discrimination of odours (Di Stadio et al, 2022). The relationship between olfactory dysfunction and cognitive decline in older adults (Graves et al, 1999), and olfactory dysfunction often preceding the development of neurodegenerative and motor symptoms in Parkinson's disease (PD) by 4 years (Ross et al, 2008), highlights the association between olfactory dysfunction and cognition. It can, therefore, be postulated that those with olfactory dysfunction after COVID-19 might have an increased risk of neurological disorders in the future (Xydakis et al, 2021).
Haematogenous infection
The CNS may become infected by SARS-CoV-2 through hematogenous routes, whereby circulating cells become infected and cross the BBB into the brain parenchyma (Yachou et al, 2020). Breakdown and destabilization of the BBB has been proposed to enhance the entry of SARS-CoV-2 (Buzhdygan et al, 2020; Pezzini and Padovani, 2020). This is supported by evidence of neuronal damage and neuroinflammation in lower brain regions such as the dorsolateral prefrontal cortex, medulla oblongata, and choroid plexus where, in post-mortem COVID-19 patients, increases in the proportion of stromal cells, monocytes, and macrophages have been observed (Fullard et al, 2021).
Further, this study detected cortical microglial transcriptional changes associated with activation, mobility, and phagocytosis (Fullard et al, 2021). Corresponding to concepts developed considering BBB neuroinvasion, brainstem and hippocampal microglial activation was found to be the hallmark of SARS-CoV-2 replication in one neuropathological study, rather than cortical neuronal apoptosis secondary to lytic replication (Poloni et al, 2021). Meanwhile, a case-series identified that neuroinflammation of lower brainstem cranial nerves without extensive axonal damage or apoptosis was the neuropathological hallmark (Matschke et al, 2020).
Exosomes represent a less explored avenue of interaction between the CNS and the periphery in SARS-CoV-2 neuroinfection, which may yet hold clues on the effects of COVID-19. A primary clue into the importance of exosomes in COVID-19 is the inclusion of SARS-CoV-2 RNA fragments as cargo, implicating endosomal trafficking in the viral lifecycle (Barberis et al, 2021). Indeed, whether SARS-CoV-2 directly infects the CNS through retrograde transduction through the olfactory nerve, through haematogenous routes, or via other mechanisms, inflammation plays a key role in pathogenesis of the long-term symptoms associated with the post-COVID-19 condition.
Inflammation
Although viral particles are usually cleared rapidly after COVID-19, studies have demonstrated that SARS-CoV-2 can be detected for many months after initial positive diagnosis, with prolonged viral shedding from the respiratory tract (Hirotsu et al, 2021; Li et al, 2020) and the gastrointestinal tract (Natarajan et al, 2022; Park et al, 2021; Wu et al, 2020) in some patients for many months after acute infection. This highlights that SARS-CoV-2 may persist within the body in some patients and contribute to chronic immune activation.
Indeed, inflammation has been found to persist long after the acute COVID-19 stage (Sollini et al, 2021a; Yong, 2021). At 5 months post-hospital discharge after SARS-CoV-2 infection, 13 proteins were identified as being significantly increased in participants with a poor recovery from COVID-19. Many of the proteins identified were related to inflammatory mechanisms, including proteins such as interleukin (IL)-6, CD83, and urokinase plasminogen activator surface receptor (Evans et al, 2022).
Further, greater levels of inflammation correlate with worse depressive and cognitive symptoms in post-COVID-19 condition patients (Mazza et al, 2021). It is likely that a combination of cellular and cytokine/chemokine responses drive the persistent levels of inflammation in post-COVID-19 condition. T cell dysfunction was proposed to promote post-COVID-19 condition pathophysiology in a similar manner to autoimmune diseases (Karlsson et al, 2020), supported by evidence that CD8+ T cells, a crucial mediator of autoimmune reactions, have been found in infiltrates in lungs and other organs in deceased COVID-19 patients (Ehrenfeld et al, 2020).
Moreover, at 3–6 months after acute infection, CD8+ T cells demonstrated continued alteration with cytotoxic effects, whereas B cell cytokine imbalance during the acute stage was restored (Shuwa et al, 2021). Functioning B cell activity may be protective from long-term symptoms of COVID-19, as B cell depleted patients can endure long-term SARS-CoV-2 infection (D'Abramo et al, 2021; Nussenblatt et al, 2021).
Levels of circulating pro-inflammatory markers, including IL-6, and C-X-C motif chemokine ligand 10 (CXCL10), have been shown to be constant up to 8 months after COVID-19; however, CXCL10 levels were higher in hospitalized participants across the study period (Peluso et al, 2021). IL-6 levels, in particular, demonstrate a positive association with post-COVID-19 neurological complaints (Sun et al, 2021). Tumor necrosis factor alpha (TNF-α) is often elevated in patients with acute COVID-19 (Tang et al, 2020) and has been associated with the development of persistent psychotic symptoms after infection with SARS-CoV-2 (Lim et al, 2020).
Excess cerebral TNF-α has also been linked to the mechanisms that cause post-COVID-19 symptoms, including anosmia, ageusia, fatigue, neurogenic pain, and suicidal tendencies (Clark, 2022). Moreover, TNF-α, IL-6, and various other inflammatory markers have been found to be associated with post-COVID-19 depression (Lorkiewicz and Waszkiewicz, 2021). Neuroinflammatory mechanisms have been implicated in headache syndromes, whereby mast cells, cytokines, and chemokines trigger nociceptive sensory neurons and trigger headache pain (Conti et al, 2019).
The excessive release of cytokines and chemokines during and after COVID-19 infection may result in similar mechanisms that lead to the development of headache (Ye et al, 2020; Yong, 2021). Sleep disturbances have also been reported to persist in those experiencing post-COVID-19 condition (Evans et al, 2021; Frontera et al, 2021), which may also have some underlying inflammatory mechanisms. For example, restless leg syndrome, a sleep disorder that is possibly due to underlying inflammatory processes (Weinstock et al, 2012), was found to occur more commonly in post-COVID-19 patients compared with controls (Weinstock et al, 2022). Indeed, inflammation is highly implicated in the mechanism of the post-COVID-19 condition and its neurological sequelae.
Hypercoagulability and cardiovascular damage
After SARS-CoV-2 infection, recovered individuals have a significantly increased risk of negative cardiovascular outcomes, including cerebrovascular disorders, dysrhythmia, inflammatory heart disease, ischemic heart disease, and thrombotic disorders (Xie et al, 2022), highlighting the significant long-term effects that SARS-CoV-2 can inflict on survivors of the acute infection. Thrombosis leading to cerebral infarction possibly poses the greatest risk to the CNS.
Samples collected from patients with the post-COVID-19 condition have been found to contain large amounts of micro-clots, which are resistant to fibrinolysis (Pretorius et al, 2021), whereas elevated D-dimer levels were observed up to 4 months after SARS-CoV-2 infection in both hospitalized and non-hospitalized individuals (Townsend et al, 2021). Hypercoagulation, thrombosis, and the overwhelming of vascular mechanisms that clear microclots are, therefore, likely to be implicated in patients with post-COVID-19 condition and are the cause of the increased risk of cerebrovascular disorders after COVID-19.
Sepsis-induced coagulopathy (Hess et al, 2020), presence of anti-phospholipid antibodies (Zhang et al, 2020b), hypercoagulation (Spence et al, 2020), endothelial dysfunction (Sardu et al, 2020), promotion of atherosclerosis by cytokine storm (Huang et al, 2020), myocardial injury (Cheng and Leedy, 2020; Larson et al, 2020), hypoxemia (Fan et al, 2020), and cerebral hypoperfusion (Helms et al, 2020; Williams et al, 2020) are all proposed mechanisms involved in developing a pro-thrombotic state and initiating cerebral ischemic events.
Coagulopathy secondary to fibrinogen-depletion (Valderrama et al, 2020) is another proposed mechanism of bleed strokes in patients with COVID-19. In patients with the post-COVID-19 condition, cardiovascular and cerebrovascular health should be an important factor to monitor, whereas future research is required to elucidate the risk factors that may identify individuals at risk from post-COVID-19 associated cerebrovascular complications.
Hypoxia
Hypoxia is a common cause of cognitive deficits in various diseases associated with acute respiratory distress syndrome (ARDS) (Hopkins and Brett, 2005), whereas its duration has been shown to correlate with the extent of cognitive deficits, which, similar to the post-COVID-19 condition, predominantly impact attention, verbal memory, and executive functions (Hopkins et al, 2005; Mikkelsen et al, 2012). In patients requiring ventilation during ARDS, memory impairment has been reported by up to 78% of individuals, sometimes lasting up to 2–5 years after ventilation (Hopkins et al, 2005).
With many COVID-19 patients suffering from ARDS and requiring mechanical ventilation during the acute disease stage, it is likely that many patients will develop long-term neurological symptoms as a result from hypoxia. Indeed, the distribution of multifocal microvascular hemorrhagic lesions in the subcortical and deep white matter on magnetic resonance imaging (MRI) scans of patients with severe COVID-19 is similar to those with hypoxic respiratory failure, sepsis, and disseminated intravascular coagulation (Conklin et al, 2021). This suggests that cerebral hypoxia can be a causal or contributing factor for the parenchymal injury in COVID-19 (Conklin et al, 2021).
Without ARDS, patients with COVID-19 frequently suffer from silent hypoxia, with a prevalence of 32–68% (Busana et al, 2021), which could partly explain cognitive deficits in patients who have not been ventilated. Further, in patients ready to be discharged from hospital, 50% developed exercise-induced hypoxia without dyspnea (Fuglebjerg et al, 2020). Inflammatory processes and capillary dysfunction have also been postulated to reduce tissue oxygen transfer and evoke hypoxia (Ostergaard, 2021).
Both acute and chronic hypoxia as a result of COVID-19 poses a significant predicament for the neurological health of patients and should be monitored accordingly by treating clinicians. Future studies should aim at assessing the long-term effect of hypoxia in the CNS of post-COVID-19 patients, including studies lasting years.
Autoimmunity
SARS-CoV-2 infection may trigger autoimmune manifestations, including the production of autoantibodies (Dotan et al, 2021) and, hence, lead to the development of autoimmunity, which could explain some of the symptoms associated with the post-COVID-19 condition. One study of post-COVID-19 patients found that all participants had between two and seven different functionally active autoantibodies against G-protein coupled receptors (GPCRs), which were a mixture of neuro-active, vasoactive or targeted the ACE2 receptor (Wallukat et al, 2021).
Further, in acute COVID-19 patients, levels of autoantibodies, including those targeting GPCRs, renin-angiotensin system-related molecules, and interferon activities, are associated with clinical severity, with higher concentrations of autoantibodies correlating with more severe disease (Bastard et al, 2020; Cabral-Marques et al, 2022; Khamsi, 2021). Many similarities can be drawn between post-COVID-19 condition and other disorders, including CFS and fibromyalgia, with symptoms such as fatigue, widespread pain, and cognitive deficits shared by these disorders (Dotan et al, 2022). CFS and fibromyalgia are thought to have underlying autoimmune dysautonomia features (Hartwig et al, 2020; Scheibenbogen et al, 2018; Shoenfeld et al, 2020), which is likely also the case for the post-COVID-19 condition.
Some of the mechanisms that may contribute to the development of an autoimmune disorder after SARS-CoV-2 infection include over-activation of the immune system, excessive neutrophil extracellular trap formation, and SARS-CoV-2 cross-reaction with host self-protein epitopes.
Peripheral organ dysfunction
After the acute phase of COVID-19, patients experience a range of respiratory, cardiovascular, metabolic, neurological, and psychiatric symptoms (Taquet et al, 2021b). However, the relationship between systemic comorbidities and neurological impairment remains unclear. In hospitalized COVID-19 patients, overall cognitive impairment and executive dysfunction correlated with level of pulmonary function and severity of current respiratory symptoms (Miskowiak et al, 2021).
Similarly, in COVID-19 survivors, who had required mechanical ventilation, hypoxemia on admission was a strong, direct predictor of cognitive impairment 6 months post-discharge, whereas the effects of inflammatory markers were mediated by the pulmonary variable (Garcia-Grimshaw et al, 2022). Post-COVID-19 patients exhibit a greater risk of kidney injury and dysfunction (Bowe et al, 2021), with the prevalence of kidney impairment estimated to be around 4% of post-COVID-19 patients who had mild acute disease (Dennis et al, 2021).
These findings are significant considering the negative consequences of both acute and chronic kidney injury on the brain (Malek, 2018; Steinbach and Harshman, 2022). Indeed, peripheral organ dysfunction and neurological symptoms of the post-COVID-19 condition may be closely linked, and the relationships between the two should be explored in detail.
Are those with pre-existing neurological disorders affected differently to those without pre-existing conditions by post-COVID-19 condition?
Those living with pre-existing conditions that effect their cognition may be more greatly affected by living through the COVID-19 pandemic or becoming infected with the virus. Indeed, COVID-19 patients with dementia are at a greater risk of severe disease, the development of delirium, and death, compared with those without dementia (Pisaturo et al, 2019), highlighting their vulnerability to the virus. People living with dementia in care homes were found to become more greatly depressed, anxious, agitated, and lonely during periods of isolation, which had a negative impact on quality of life (Velayudhan et al, 2020), whereas both cognitively impaired patients and their caregivers report increased psychological and physical burden during periods of government-imposed lockdown (Tsapanou et al, 2021).
Social isolation also resulted in the exacerbation of neuropsychiatric and behavioural disturbances in people living with dementia in care homes during the COVID-19 pandemic (Manca et al, 2020; Simonetti et al, 2020). Moreover, COVID-19 infection has been found to significantly worsen motor and non-motor symptoms in patients with PD when compared with patients who did not become infected with SARS-CoV-2 (Cilia et al, 2020).
Together, these findings demonstrate the significant impact that both SARS-CoV-2 infection and the impact of the pandemic elicits on individuals living with dementia. These profound effects may incur long-lasting consequences for these individuals and, if these patients also develop symptoms of the post-COVID-19 condition, this may pose significant issues for their future quality of life and treatment strategies.
Those with pre-existing neurological conditions such as multiple sclerosis (MS), motor neuron disease, fibromyalgia, or neuromuscular disorders could potentially be severely affected by the development of the symptoms of post-COVID-19 condition due to their underlying condition. For instance, myalgia inflicted as part of the post-COVID-19 syndrome (Taquet et al, 2021b) could exacerbate the pain experienced, whereas autoimmune mechanisms (Dotan et al, 2021) and chronic inflammation (Sollini et al, 2021a; Yong, 2021) may result in the worsening of MS symptoms.
Another damaging factor to those with pre-existing neurological conditions as a result of the COVID-19 pandemic is the reduction of care either due to the hospital's canceling appointments and services or due to individuals' reluctance to travel to hospital in the height of the pandemic.
It is highly likely that both the post-COVID-19 condition and the COVID-19 pandemic itself has resulted in extreme burden to those living with pre-existing neurological conditions. It is, therefore, imperative to give specialist attention to this group of people when treating post-COVID-19 symptoms and consider the heightened impact that post-COVID-19 symptoms have on their pre-existing symptoms.
Risk Factors
Risk factors for acute COVID-19 infection and associated neurological symptoms
Risk factors for severe acute COVID-19 are outlined in Figure 2.
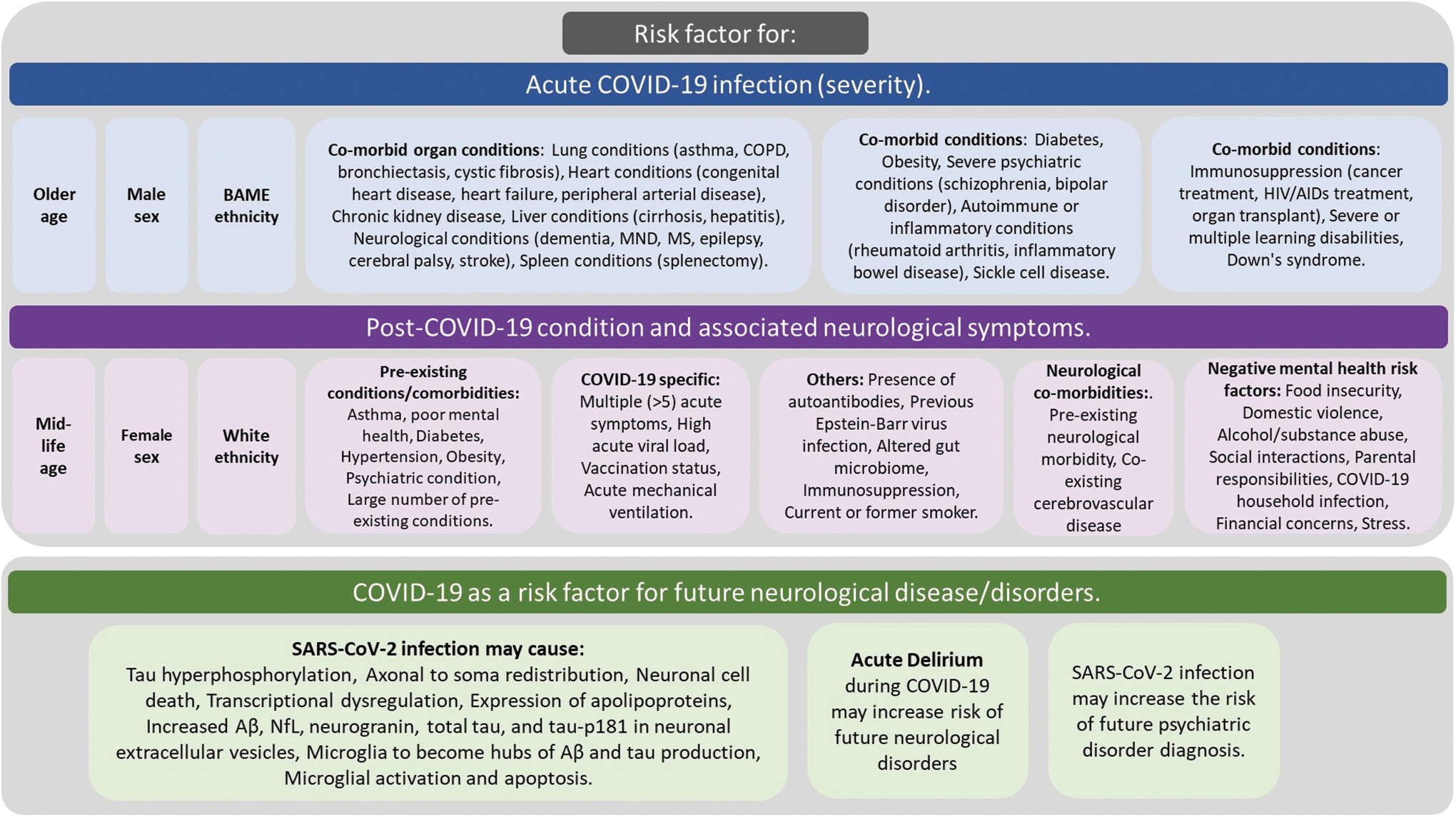
Possible risk factors for acute COVID-19 infection, post-COVID-19 condition, and the suggested relationships between COVID-19 and the risk of future development of neurological disorders. Color images are available online.
Risk factors for post-COVID-19 condition and associated neurological symptoms
It is understood that certain individuals are more significantly affected than others by COVID-19. Likewise, there is an individual susceptibility to develop post-COVID-19 condition, which seems to be independent of the severity of the acute pulmonary and systemic illness (Amalakanti et al, 2021; Nakamura et al, 2021). The risk factors associated with developing post-COVID-19 condition are described in Figure 2. When considering the risk factors for neurological symptoms of the post-COVID-19 condition, individual factors should be considered.
For example, one study found that those hospitalized with acute COVID-19 were more likely to present to primary care for post-COVID-19 with mental health symptoms compared with community infections, whereas community infections were more likely to present with CNS symptoms compared with hospitalized patients (Meza-Torres et al, 2022).
Of the risk factors associated with acute and post-COVID-19, one of the intriguing factors is ethnicity, with Black, Asian and minority ethnic ethnicity associated with a poorer outcome for acute COVID-19 severity (Gao et al, 2021) and white ethnicity associated with an increased risk of post-COVID-19 condition (Thompson et al, 2022). Although it is unclear why this is the case, a range of biological, cultural, and socioeconomical factors likely play a role, as well as the availability and access to medical services available to these groups for the treatment of acute and post-COVID-19.
Sex is another factor that shows opposing risks for acute COVID-19 and post-COVID-19 condition, with males at a greater risk of severe acute COVID-19 (Hippisley-Cox et al, 2021; Kim et al, 2021; Parohan et al, 2020) and females at a higher risk of developing post-COVID-19 manifestations (Munblit et al, 2021; Taquet et al, 2021a), including specific neurological symptoms (Asadi-Pooya et al, 2022; Méndez et al, 2021; Schou et al, 2021). Males may exhibit a greater risk of severe acute COVID-19 due to genetic and immunological differences compared with females (Bwire, 2020), whereas they may also have a “less responsible” attitude toward COVID-19 (de la Vega et al, 2020).
Conversely, the robust immune response that may slightly protect females against acute infection, in comparison to males, could contribute to making them more susceptible to autoimmune-related manifestations and long-term neurological symptoms of COVID-19 (Sylvester et al, 2022). Sex hormone differences may also play a role in a female's enhanced susceptibility to the post-COVID-19 condition (Stewart et al, 2021).
Is COVID-19 a risk factor for future neurological disease/disorders (e.g., dementia)?
It has been postulated that acute COVID-19 infection could elicit an increased risk for the development of neurological conditions, including, but not limited to PD, Alzheimer's disease (AD), psychiatric disorders, seizures, and stroke (Nagu et al, 2021; Serrano-Castro et al, 2020). Some post-COVID-19 condition patients demonstrate a cognitive performance similar to a patient with moderate traumatic brain injury, whereas others demonstrate cognitive scores similar to a patient with mild AD (Mainali and Darsie, 2021).
SARS-CoV-2 infection may have serious long-term consequences that could potentially lead to the development of neurological disease, for example, infection with the virus has been found to trigger pathological pathways that are key processes in neurological and neurodegenerative disease. Infection of three-dimensional brain organoids with SARS-CoV-2 triggers tau hyperphosphorylation, axonal to soma redistribution, and apoptosis (Ramani et al, 2021).
Further, SARS-CoV-2 has been shown to readily infect and replicate within choroid plexus organoids, with the ensuing transcriptional dysregulation involving pathways that include apolipoprotein E (APOE), 14-3-3 protein epsilon (YWHAE), aquaporin 1 (AQP1), and aquaporin 4 (AQP4) (Jacob et al, 2020), which are implicated in several CNS disorders. Infection of mature choroidal plexus cells by SARS-CoV-2 in organoid experiments has been associated with the expression of apolipoproteins, indicating a potential role in selective susceptibility (Pellegrini et al, 2020) beyond the virus receptors available at the neurovascular interface (Torices et al, 2021).
This concept has been shown to be APOE isoform-dependent, indicating that ɛ4/ɛ4 neurons and astroglia are preferentially vulnerable (Wang et al, 2021a). This latter finding may be of particular importance in linking ɛ4 carrier status to the post-COVID-19 dyscognitive phenomenology (Kurki et al, 2021) and comorbidity-independent severity (Kuo et al, 2020).
Exosomes may transport SARS-CoV-2 as cargo and allow cellular entry via lipid rafts within the CNS (Barberis et al, 2021; Palacios-Rapalo et al, 2021). Neuronal-enriched extracellular vesicles (nEVs), isolated from plasma, have been found to contain higher concentrations of amyloid-beta (Aβ), neurofilament light chain (NfL), neurogranin, total tau (t-tau), and phosphorylated tau181 (p-tau181) in COVID-19 patients compared with uninfected controls (Sun et al, 2021). Αβ extracellular release has been shown to occur in association with exosomes and their cargo in AD (Rajendran et al, 2006).
Considering that exosomes carrying viral particles can be antigenic (Hong et al, 2021), the inclusion of SARS-CoV-2 RNA with Αβ may function as an immune stimulus similarly to the antigenic HSV-1—Αβ (Roy et al, 2020) and DENV-IFITM3 containing exosomes (Zhu et al, 2015) for microglia and peripheral immune cells, respectively. Aside from nucleic acids, viral protein components of exosomal cargo, such as the SARS-CoV-2's spike protein (S), enhance proteopathic seeding by promoting neuronal exosome uptake (Liu et al, 2021a). Taking into account SARS-CoV-2's amyloidogenic scaffolding of α-synuclein (Idrees and Kumar, 2021), the stressors necessary to initiate prion-like pathology within the CNS may be provided or enhanced during COVID-19.
SARS-CoV-2 interacts with pathological proteins associated with dementia-causing diseases. In silico docking has demonstrated that SARS-CoV-2's S-1 can bind Aβ, α-synuclein, tau, prion, and TDP-43 (Idrees and Kumar, 2021), proteins that may alter its spatial dynamics and its binding to heparan sulfate peptidoglycans (HSPGs)—receptors that assist its entry (Zhang et al, 2020a). This has been corroborated by in vitro studies for the Aβ1-42—S1 interaction (Hsu et al, 2021).
Notably, α-synuclein interacts with SARS-CoV-2's nucleocapsid (N) protein, with consequent formation of Aβ fibrils (Hsu et al, 2021). The latter interaction may be of particular interest, considering that α-synuclein containing Lewy body formation and microgliosis secondary to SARS-CoV-2 infection have been reported in a primate model (Philippens et al, 2021).
Amyloidogenic molecules native to the CNS milieu may interact with SARS-CoV-2 proteins. Amyloids in the CNS have been shown to enhance antigenicity for out-of-place nucleic acids, regardless of whether their source is endogenous, or HSV-1 derived, culminating to their activation and the elicitation of local type I interferon (IFN-I) responses in AD (Roy et al, 2020). Further, HHV-6A neuroinfection has demonstrated that microglia permissive to infection may themselves become hubs of Αβ and tau production (Bortolotti et al, 2019).
These paradigms appear to be supported in the case of SARS-CoV-2—microglia interaction. Microglial permissiveness to SARS-CoV-2 has been shown to lead to activation and apoptosis (Jeong et al, 2022; Olivarria et al, 2022), a finding confirming the overlap between AD microglial signatures and COVID-19 transcriptomes (Magusali et al, 2021; Vavougios et al, 2021a). Notably, a link between IFN-I signaling and Αβ oligomerization was found in the antiviral protein and gamma secretase modulator IFITM3 (Hur et al, 2020), whose expression, structural conformations, and membrane stabilization, in turn, affect SARS-CoV-2 ACE2 independent entry (Grodzki et al, 2022; Shi et al, 2021).
Single nucleus transcriptomics of CNS samples donated by COVID-19 patients provide further corroboration to this concept by indicating that microglia produce gene signatures that overlap with those found in neurodegenerative disease (Yang et al, 2021). Further, a consensus gene module associated with CNS microglial (Vavougios et al, 2021a) and entorhinal cortex neurons containing neurofibrillary tangles (Vavougios et al, 2021b) donated by AD patients were independently and significantly enriched by COVID-19 derived transcriptomes, with IFN-I signatures at the epicenter.
In this quasinfectious model of SARS-CoV-2's neuropathic effects, microglial activation would promote Αβ and tau accumulation, tissue-wide IFN-I signaling, and neurodegeneration. In turn, neurodegeneration would culminate in IFN-I signaling (Nazmi et al, 2019). Subsequently, feed forward activation of microglia would be modulated by the operational status of enhancers (Vavougios et al, 2021b) or abrogators (Magusali et al, 2021) of neuroinflammation defined by both host genetics and epigenetics, as well as SARS-CoV-2's differential modulation of IFN-I cascades per host (Kim and Shin, 2021). The information presented here strongly links SARS-CoV-2 infection with the pathogenesis of neurodegenerative diseases. It is, therefore, possible that COVID-19 infection may represent a risk factor for future neurodegenerative/neurological disorders.
Based on cognitive impairments that can persist beyond acute COVID-19, several studies have investigated biomarkers indicative of neurodegeneration in patients with neurological symptoms associated with the post-COVID-19 condition. Elevated serum levels of the axonal protein NfL is an established marker of neuronal cell death in many neurodegenerative diseases and neurological conditions. Acid gliofibrillary protein (GFAP), meanwhile, is an astrocytic protein associated with neuroinflammation and its serum levels are increased in neurodegenerative diseases (Oeckl et al, 2019).
Elevated concentrations of serum NfL and GFAP have been found in acute COVID-19 patients, whereas elevated serum levels of either NfL or GFAP are associated with an unfavorable COVID-19 outcome (Aamodt et al, 2021; De Lorenzo et al, 2021; Kanberg et al, 2020; Prudencio et al, 2021; Sutter et al, 2021). Frontera et al examined serum GFAP, NfL, and other serum-based biomarkers in 251 hospitalized COVID-19 patients with no previous history of dementia. NfL, GFAP, p-tau181, t-tau, and ubiquitin carboxy-terminal hydrolase L1 (UCHL1) were all significantly elevated in patients who died with COVID-19, whereas low levels of tau, GFAP, and NfL were associated with a higher probability of survival. Interestingly, NfL, GFAP, and UCHL1 were higher in COVID-19 patients than in AD patients without COVID-19 (Frontera et al, 2022).
A small clinical trial showed that the CSF of patients with COVID-19 and neurological symptoms demonstrated increased NfL, whereas the increased CSF concentration was associated with the severity of neurological symptoms, including an altered mental status, headache, and central and peripheral weakness (Virhammar et al, 2021).
Interestingly, 6 months after acute infection, one study found no detectable elevation of NfL or GFAP, although 50% of participants suffered from persistent neurological symptoms (Kanberg et al, 2020). This suggests that neuronal damage may occur exclusively during acute COVID-19, and post-COVID-19 symptoms are not a result of a neurodegenerative process. This is substantiated by another study, which found a normalization of abnormally elevated serum NfL seen during the acute phase 6-month follow-up (Bozzetti et al, 2021).
Acute rises in serum or CSF NfL and GFAP indicate neuronal damage and neuroinflammation, respectively, which may have negative long-term impacts for COVID-19 survivors and their future risk of neurological disease and cognitive impairment. However, one study comparing CSF and serum NfL in COVID-19 encephalopathy detected no strong correlation (Paterson et al, 2021), with normal CSF NfL and elevated serum NfL. Therefore, it cannot be excluded that serum NfL levels in the acute COVID-19 stage may be indicators of peripheral neuronal injury, although further studies are needed to substantiate this hypothesis.
Another link to the long-term risk of neurological conditions after SARS-CoV-2 infection is acute stage delirium, which can occur during acute COVID-19 (Fleischer et al, 2021; Garcia-Azorin et al, 2021; Kennedy et al, 2020; Pun et al, 2021). A large meta-analysis reported that delirium was present in 34% of acute COVID-19 patients aged 60 years or older (Misra et al, 2021).
Many risk factors for developing delirium during acute COVID-19 have been identified (Martinotti et al, 2021; Pun et al, 2021), whereas delirium is associated with increased risk of death during acute COVID-19 (Mendes et al, 2020; Shao et al, 2021). Delirium during critical illness is a risk factor for long-term cognitive impairment (Arnold, 2020; Pandharipande et al, 2013), with large cohort studies (Ehlenbach et al, 2010) and meta-analysis (Goldberg et al, 2020) demonstrating that critical illness and delirium predict future cognitive decline.
This trend has been observed with COVID-19. One study assessed COVID-19 survivors at 6 months after hospital discharge and compared them with a group of uninfected controls. Delirium during the acute disease stage was a risk factor for cognitive impairment and longitudinal cognitive decline at 6 months (Liu et al, 2021b), highlighting the magnitude of the risk of impaired cognition after COVID-19-associated delirium.
These findings confirm that delirium during acute COVID-19 infection is almost certain to increase an individual's risk of long-term cognitive decline. However, the mechanisms by which this process occurs, and whether and how COVID-19-associated delirium differs from delirium due to other causes remain unknown.
COVID-19 may also inflict a future risk of psychiatric disorders. One study found that, in patients with no previous history of psychiatric disorders, the risk of a psychiatric diagnosis after infection was significantly higher for COVID-19 infection compared with six other heath events, including influenza and other respiratory tract infections. The incidence was particularly high for the development of disorders such as anxiety disorder, insomnia, and dementia after COVID-19 infection (Taquet et al, 2021c).
Can Post-COVID-19 Condition Be Accurately Diagnosed?
Acute COVID-19 can be quickly diagnosed with real-time quantitative polymerase chain reaction or with point-of-care testing such as lateral flow tests. The post-COVID-19 condition and its associated neurological manifestations, however, are more difficult to diagnose. Clinical guidelines to diagnose and treat the generalized post-COVID-19 condition have been proposed (Greenhalgh et al, 2020; NICE, 2021; Siso-Almirall et al, 2021); however, specific guidelines for the neurological aspects of post-COVID-19 condition remain elusive. Here, we will outline the possible assessments and examinations that may prove useful in diagnosing post-COVID-19 condition and its neurological sequelae.
Clinical assessments
Specific guidelines and assessments are likely to differ depending on the type of care being offered: primary, secondary, or tertiary. However, when a patient presents for care, a detailed clinical history should be taken, with electronic health records a useful tool to determine whether the individual was an inpatient due to COVID-19, whether and when they had been vaccinated against COVID-19, and whether they have any other diagnoses of pre-existing conditions.
If not hospitalized by acute COVID-19, the period of time that has passed since the acute infection should be considered to determine whether the patient is experiencing post-acute effects of COVID-19 or true post-COVID-19 condition. Based on the current definitions, at least 12 weeks should have passed since the initial acute infection to be considered post-COVID-19 condition (Soriano et al, 2022). Another important aspect to examine is the symptomatology of the patient.
The symptoms elicited by both acute and post-COVID-19 are extremely heterogeneous, with acute COVID-19 suggested to be able to be characterized into one of six clusters (Sudre et al, 2021a; Zoe Health Study, 2020). To accurately diagnose such a heterogeneous condition, universally accepted symptom clusters and an understanding of the systems they affect must be developed. It is likely that one of these clusters will primarily affect the nervous system and will be of particular interest to neurologists.
When assessing a patient, it is important to develop a comprehensive list of differential diagnoses (Jain, 2017). This list is important to exclude any other possible conditions that may be causing the symptoms as well as not to overlook any serious issues that could be time-sensitive and life-threatening. Further, clinical history and medical record reviews could uncover pre-existing conditions that may be exacerbated after SARS-CoV-2 infection and may be the primary cause of the current symptoms.
When post-COVID-19 condition with neurological involvement is suspected, it may be useful to explore specific neurological functions in detail. In this instance, a range of cognitive and neuropsychological tests can be implemented. Examples of such tests are outlined in Table 2. These tests should be administered by discretion of the examiner and be tailored in accordance with the specific symptomatic domains that the patient is complaining of. Certain clinical tests can possibly predict other manifestations; for example, Calabria et al (2022) found that certain cognitive and neuropsychiatric symptoms were a predictor of fatigue in their study cohort of 136 COVID-19 survivors at 8 months after acute infection.
Possible Clinical Tools That Could Be Employed to Assess Patients with Suspected Neurological Sequalae of Post-COVID-19 Condition
ASL, arterial spin labeling; CSF, cerebrospinal fluid; CT, computed tomography; ECG, electrocardiogram; EEG, electroencephalogram; FACIT, Functional Assessment of Chronic Illness Therapy; FDG, fluorodeoxyglucose; GAD-7, Generalized Anxiety Disorder 7-item scale; IES-R, Impact of Event Scale–Revised; IgG, immunoglobulin; IL, interleukin; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; MRI, magnetic resonance imaging; Neuro-QOL, quality of life in neurological disorders; NfL, neurofilament light chain; p-tau181, phosphorylated tau181; PCL-5, Post-Traumatic Stress Disorder Checklist; PET, positron emission tomography; PHQ, Patient Health Questionnaire; QAlb, albumin quotient; SAQ, Sleep Assessment Questionnaire; SQS, Sleep Quality Scale.
Imaging
Neuroimaging allows us to evaluate the structural and functional changes occurring in the CNS of patients with post-COVID-19 condition. Computed tomography (CT) and MRI may be useful in this instance to exclude other neurological conditions. Further, using 1.5 T or 3 T MRI, gray matter thickness was reduced in the orbitofrontal cortex and parahippocampal gyrus of participants at 141 days after SARS-CoV-2 infection compared with uninfected individuals, whereas markers of tissue damage in functionally connected regions to the primary olfactory cortex were also detected (Douaud et al, 2022).
Meanwhile, gray matter abnormalities in the limbic system and basal ganglia of COVID-19 survivors have been identified at 2 weeks after hospital discharge was associated with greater fatigue levels (Hafiz et al, 2022). Although subtle structural changes may be difficult to identify individually, these studies demonstrate that structural changes may be present within the CNS of patients with post-COVID-19 condition.
Another study showed similar findings in patients with no post-COVID-19 neurological manifestations, with those who experienced severe acute COVID-19 exhibiting decreased volume of subcortical nuclei compared with those who experienced mild disease and uninfected controls (Tian et al, 2022), further highlighting the possible uses of MRI in the diagnostic procedure of post-COVID-19 condition. Measuring CNS perfusion using arterial spin labeling may also demonstrate changes occurring during the post-COVID-19 condition, with olfactory dysfunction being associated with decreased perfusion in the orbital and medial frontal regions in patients with post-COVID-19 condition (Yus et al, 2022).
The MRI also provides the opportunity to investigate cerebral changes in fundamentally different ways (van Bussel et al, 2017). The MRI can be used to detect abnormalities at the micro-structural and micro-vascular level, which are expected to precede macro-structural abnormalities and are possibly detectable earlier in the disease process. Further, acquiring data at ultrahigh field 7 T MRI enriches the images with better signal-to-noise and spatial details not visible at lower field strengths.
As a result, 7 T imaging exhibits increased diagnostic power due to enhanced sensitivity to detect fine-scale properties and changes in the brain (Canjels et al, 2020) and could be a useful technology to explore the CNS of patients with the post-COVID-19 condition neurological sequalae.
Fluorodeoxyglucose (FDG)-positron emission tomography (PET) offers another avenue to explore the neurological dysfunction associated with the post-COVID-19 condition. Using FDG-PET, hypometabolism has been observed in the frontal, parietal, and temporal lobes, as well as in the brainstem, cingulate gyrus, thalamus, and parahippocampal gyrus of patients with the post-COVID-19 condition and neurological symptoms (Delorme et al, 2020; Grach et al, 2022; Guedj et al, 2021; Hugon et al, 2022a; Hugon et al, 2022b; Sollini et al, 2021b).
This pattern of hypometabolism is consistent with the neuropsychological profile observed in patients with changes in cognition. Similar patterns of hypometabolism have been observed in pediatric patients with the suspected post-COVID-19 condition (Morand et al, 2022). Although partial resolution of hypometabolism and associated cognitive impairment is seen, some residual hypometabolism has been identified in post-COVID-19 patients at 6 months after acute infection (Blazhenets et al, 2021).
Moreover, the pattern of brain hypometabolism displayed in post-COVID-19 patients with hyposmia appears to differ from the pattern of hypometabolism observed in PD patients with hyposmia (Morbelli et al, 2022), suggesting that the pattern exhibited in post-COVID-19 may be specific to this condition and, hence, provide a useful diagnostic feature. Examining patients with FDG-PET imaging would be useful. Translocator protein PET imaging, including [18F]DPA-714 (Visser et al, 2022), has demonstrated increased neuroinflammation in post-COVID-19 condition patients. Interestingly, another study using [11C]PBR28 PET (Brusaferri et al, 2022) demonstrated heightened neuroinflammation in those who have lived through the pandemic compared with pre-pandemic levels.
These modalities, including those that quantify metabolism, neuroinflammation, pathological proteins, or other pathological processes, will have potential in understanding the pathological basis of neurological complications of post-COVID-19 conditions. Table 3 provides examples of neuroimaging data obtained from patients with post-COVID-19 condition.
Studies Exploring Neuroimaging Data Obtained from Patients with Post-COVID-19 Condition
CBF, cerebral blood flow; DTI, diffusion tensor imaging; PTSD, post-traumatic stress disorder; TSPO-PET, translocator protein.
Fluid biomarkers
Blood-based biomarkers may hold potential for detecting and diagnosing neurological issues in individuals experiencing post-COVID-19 condition. One study compared blood plasma biomarkers and nEVs of post-COVID-19 condition patients at 1–3 months after infection. Plasma IL-4 was higher in the whole COVID-19 positive group compared with controls, whereas IL-6 concentration was greater in COVID-19 survivors with neurological problems compared with those without.
Moreover, plasma markers, including Aβ, t-tau, p-tau181, NfL, and neurogranin, were significantly increased in the nEVs of COVID-19 survivors compared with control samples (Sun et al, 2021). Persisting lymphopenia, and elevated d-dimer and C reactive protein levels have been detected in hospitalized COVID-19 patients, 54 days after discharge (Mandal et al, 2021), indicating a decreased number of lymphocytes, an increased risk of thrombosis, and increased levels of inflammation, respectively.
Quantification of nitrite (NO2−) and nitrate (NO3−) levels in blood serum have been suggested as potential biomarkers for the post-COVID-19 condition. Although no significant differences were observed between currently infected COVID-19 patients and uninfected controls, recovered patients had significantly lower NO2− and NO2−/NO3− ratio, and higher NO3− compared with uninfected patients (Wang et al, 2021b), highlighting the relationship between previous COVID-19 infection and NO2−/NO3− levels.
As longitudinal studies take place, further blood-based biomarkers of post-COVID-19 condition and its neurological sequelae will likely be identified. Whether these biomarkers will be specific and sensitive enough to accurately diagnose the neurological sequelae of post-COVID-19 condition is yet to be seen.
In acute COVID-19 patients with neurological manifestations, one study found CSF abnormalities in 62.7% of patients with neurological manifestations (Garcia-Azorin et al, 2021). Albumin quotient (QAlb) is an indicator of blood-CSF barrier (BCB) permeability or dysfunction, with higher levels corresponding to greater dysfunction. In a study of COVID-19 patients with neurological symptoms, 50% of those without pre-existing CNS disorders had BCB dysfunction, as measured with QAlb.
Further, this elevated level of QAlb remained elevated for more than 30 days after COVID-19 onset (Jarius et al, 2022). Total protein content measures the concentration of immunoglobulin (IgG) in the CSF, with increased concentrations indicative of a CNS disorder. The CSF total protein has been shown to be elevated in 45.8% of acute COVID-19 patients with neurological symptoms (Jarius et al, 2022). This study also found abnormal CSF white cell count (11% of patients) and
Similarly, a case report of six COVID-19 patients with neurological symptoms found that concentrations of CSF neopterin and β2-microglobulin, markers of inflammation, were elevated in all patients, whereas CSF NfL level was also increased in two patients (Eden et al, 2021). How long these abnormal CSF measurements in some COVID-19 patients with neurological manifestations last remains unknown. Indeed, longitudinal follow-up studies that assess possible CSF biomarkers of the post-COVID-19 condition are required.
One such study, the Karolinska NeuroCOVID study, aims at assessing participants who were treated for severe COVID-19 in an intensive care unit (ICU) longitudinally after discharge. This study aims at identifying and relating serum-, plasma-, and CSF-borne molecular and cellular markers of inflammation, coagulopathy, cerebral damage, neuroinflammation, and degeneration, to MRI findings and cognitive and neurological deficits (Nelson et al, 2022). The goal of this work is to improve the understanding of the mechanisms driving this pathology and the neurological consequences of COVID-19 and post-COVID-19.
Monitoring
Clinical scales to accurately measure outcomes of acute COVID-19 have been developed, with the WHO publishing ‘a minimal common outcome measure set for COVID-19 clinical research’ in 2020 (Marshall et al, 2020). Creation of a similar set of outcomes for the post-COVID-19 condition has been slow due to the enigmatic nature of the condition and our developing understanding of it. An international group known as the “PC-COS Project Steering Committee” outlined a core outcome set for research and clinical practice in the post-COVID-19 condition (Munblit et al, 2022). The rigorous methodology resulted in 11 outcomes meeting the “in” criteria, which are detailed next:
Physiological/clinical outcomes: Cardiovascular functioning, symptoms, and conditions. Fatigue or exhaustion. Pain. Nervous system functioning, symptoms, and conditions. Cognitive functioning, symptoms, and conditions. Mental functioning, symptoms, and conditions. Respiratory functioning, symptoms, and conditions. Post-exertion symptoms.
Life impact outcomes:
Physical functioning, symptoms, and conditions.
Work/occupational and study changes.
Survival:
Survival.
Outcome from previous core outcome set:
Recovery.
This list of core outcomes should be examined in clinical settings when assessing and monitoring patients with suspected post-COVID-19. One notable aspect of this core outcome set that is the number of physiological/clinical outcomes that are, at least in part, a result of neurological pathophysiology after COVID-19, highlighting the importance of the neurological impacts of the post-COVID-19 condition.
Although unspecific to neurological symptoms, the CDC website offers a comprehensive overview of guidance for evaluating and caring for patients with the post-COVID-19 condition, including guidance on taking patient history, undertaking physical examinations, undertaking clinical assessments, and managing conditions associated with post-COVID-19 (CDC, 2021b).
In addition, the symptom burden questionnaire for long covid (SBQ-LC) has been developed as a novel tool for evaluating post-COVID-19 symptoms (Hughes et al, 2022). The SBQ-LC is a set of 17 independent scales that covers 16 symptom domains and 1 measurement of symptom impact on daily life that can be administered in its entirety or as a subset to explore specific domains.
The modified COVID-19 Yorkshire Rehabilitation Scale (C19-YRSm) is another patient-reported outcome scale for the post-COVID-19 condition (Sivan et al, 2022). This 17-item measure includes subscales for symptom severity, functional disability, other symptoms, and overall health. These tools are likely a useful and simple to implement in clinics supporting patients with the post-COVID-19 condition.
Overall, the post-COVID-19 condition poses significant challenges in monitoring patients appropriately to record their symptoms, objectively evaluate their neurological complications, and monitor early signs of change in different parameters, particularly in cognition and mental health. It should be considered that neurological complications could also be resulting from complications of systemic illness affecting the pulmonary function leading to hypoxia, autonomic dysfunction leading to significant irregularity in the heart rate, general fatigue, and lack of exercise. Future monitoring should generate a significant amount of data—with the help of mobile devices and other advanced A1 algorithms, to assist in capturing the neurological complications of post-COVID-19.
Can the neurological symptoms associated with post-COVID-19 condition be distinguished from the effects of lockdown?
Patients with persisting symptoms after COVID-19 may present with a range of heterogeneous symptoms (Crook et al, 2021). Government-imposed restrictions including lockdowns, and the subsequent changes in individual circumstances in professional and personal life may have played a role in the development of many of these symptoms.
Belief in having been infected with COVID-19 has been found to be associated with persistent symptoms to a greater degree than actually being infected with SARS-CoV-2 (Matta et al, 2022), highlighting the psychological effect the COVID-19 pandemic may have had on individuals. Whether the neurological symptoms experienced by these patients are a direct consequence of the viral infection or because of the psycho-social stressors associated with the pandemic may cause difficulty when attempting to diagnose patients with post-COVID-19 condition.
Government-imposed restrictions to life that aimed at reducing the spread of SARS-CoV-2 were found to have a negative effect on the population, especially on mental health. Anxiety, feelings of defeat and entrapment, depressive symptoms, loneliness, suicidal thoughts (O'Connor et al, 2021), as well as worsening or new onset of obsessive-compulsive disorder (Guzick et al, 2021) and panic disorder (Javelot and Weiner, 2021) were associated with the COVID-19 pandemic.
In addition, the longer a person was confined to quarantine, the poorer the outcomes for their mental health (Brooks et al, 2020). Living through a global health crisis is thought to lead to avoidance behaviors and behavioral changes (Usher et al, 2020). The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability study assessed the effect of the COVID-19 pandemic and the infection-control measures on people in Finland, finding that 33% of participants reported doing less exercise, 15% reported sleeping problems, 21% reported loneliness, and 15% felt that their memory got worse during the pandemic (Lehtisalo et al, 2021).
Women, young people, elderly people, those from socially disadvantaged backgrounds, and those with pre-existing mental health problems exhibited worse mental health outcomes during the pandemic (Creese et al, 2021; O'Connor et al, 2021; Sayin Kasar and Karaman, 2021). Women who were pregnant, miscarrying, postpartum, or experiencing domestic violence were at particular risk for developing mental health conditions (Almeida et al, 2020).
In adolescents, increases in depressive symptoms and anxiety were found when comparing measures from before and during the pandemic, a finding that was most prominent in girls (Magson et al, 2021), with disengagement from school, social, and outdoor activities having significant negative impacts on the mental health of young people during the pandemic (de Figueiredo et al, 2021).
Reduced levels of physical activity and increased sedentary time during the pandemic was shown to have a negative effect on mental health (Violant-Holz et al, 2020), whereas the maintenance of physical activity was found to positively impact stress and depressive symptoms in older people (Solianik et al, 2021). Further, infants born during the COVID-19 pandemic were found to have lower motor and personal-social assessment scores when compared with a historical cohort of the same age, regardless of in utero exposure to maternal SARS-CoV-2 infection (Shuffrey et al, 2022). Relationship quality was also associated with mental health measures (Pieh et al, 2020), whereas social support was a protective factor against mental health problems associated with the pandemic (Almeida et al, 2020).
The symptomatic spectrum that manifested due to government-imposed restrictions is closely related to mental health, as opposed to the spectrum of manifestations associated with the virus infection itself. However, there is a current unmet need to develop tools to differentiate patients from the post-COVID-19 condition secondary to direct viral infection from the neuropsychiatric manifestations of lockdown. These tools will prove useful when assessing and attempting to diagnose individuals with the post-COVID-19 condition. In any case, long-term monitoring of mental health, especially that of at-risk groups including women and young people, is of vital importance.
How Can the Neurological Symptoms of Post-COVID-19 Condition Be Effectively Treated?
Although neuronal involvement and neuropsychiatric manifestations are common after COVID-19, no novel therapeutic strategies have been developed that can treat the neurological complications and potential long-term processes that occur after infection. Due to the heterogeneity of the post-COVID-19 condition and the fluctuating nature of the symptoms, treating patients with post-COVID-19 is likely a challenging task. For example, headache appears to gradually resolve after COVID-19 infection (Fernandez-de-las-Penas et al, 2021a).
The timing and intensity of offered treatment, therefore, will require accounting for how advanced and how likely the symptom will resolve without any intervention. Further, due to the heterogeneity of neurological symptoms associated with the post-COVID-19 condition based on sex differences (Sylvester et al, 2022), it is likely that a personalized approach that includes sex-specific treatments is required.
Although specific treatments for post-COVID-19 condition and its neurological manifestations are lacking, several groups are currently undertaking studies to assess therapies to treat the condition (Clinicaltrials.gov, 2022; Haroon et al, 2022; Pang et al, 2022).
COVID-19 vaccination
Since COVID-19 vaccinations have become widely available, a positive impact of vaccination on post-COVID-19 symptoms has been observed. Compared with unvaccinated individuals, those who have received at least one dose of a COVID-19 vaccination have been found to be less likely to develop long-term symptoms or have seen improvements in their persistent post-COVID-19 symptoms after vaccination (Al-Aly et al, 2022; Antonelli et al, 2022; Arjun et al, 2022; Arnold et al, 2021b; Ayoubkhani et al, 2022; Gaber et al, 2021; Herman et al, 2022; Kuodi et al, 2022; Scherlinger et al, 2021; Senjam et al, 2021; Sherwood et al, 2021; Simon et al, 2021; Strain et al, 2022; Taquet et al, 2022; Tran et al, 2021; Wanga et al, 2021).
As vaccination rates are high for much of the Americas, Europe, Asia, and Australia/Oceania (WHO, 2022b), many potential cases of the post-COVID-19 condition may have been avoided. Africa, however, has vastly lower rates of vaccination (WHO, 2022b); therefore, an effort to increase vaccination rates in this continent may contribute to reducing the prevalence of the post-COVID-19 condition in this continent.
Pharmacological agents
Pharmacological interventions have been proposed and their effectiveness for treating certain neurological symptoms caused by the post-COVID-19 condition are being explored. For instance, simultaneous treatment with intranasal insulin, zinc, and gabapentin are being tested for its effectiveness to ameliorate smell and taste dysfunctions in patients with the post-COVID-19 condition (NCT05104424), whereas gabapentin alone is also being assessed for its use in reducing dysfunctions of smell (NCT05184192).
Cerebrolysin is also being examined in patients post-COVID-19 infection for its efficacy at treating smell and taste dysfunctions, due to its neurotrophic and neuroprotective properties (NCT04830943). Meanwhile, ruconest, a c1 esterase inhibitor that inhibits the complement system, is being assessed for its efficacy in improving the neurological symptoms associated with the post-COVID-19 condition (NCT04705831).
The use of AXA1125, an orally active mixture of amino acids, is being assessed against a placebo for its use to treat fatigue in patients with the post-COVID-19 condition (NCT05152849). Additional therapeutic strategies for treating the neurological complications of the post-COVID-19 condition need to be evaluated. This could include anti-IL-6, anti-TNF, or drugs that modulate neuroinflammation and astrocytic activation. Pharmacological agents that have antioxidating effects may also have benefits, with melatonin postulated to have potential uses in treating the post-COVID-19 condition due to its ability to activate nuclear factor (erythroid-derived 2)-like 2 (Nrf2), which has antioxidant actions (Jarrott et al, 2022).
BC 007, a DNA aptamer, has a high affinity and neutralization ability to autoantibodies targeting GPCRs and, in one case study, was found to functionally inactivate these autoantibodies within 48 h after a single treatment in a patient suffering from post-COVID-19 condition. These autoantibodies remained inactive throughout the entire 4-week observation period, whereas fatigue and taste dysfunction improved after the treatment (Hohberger et al, 2021).
Drugs that neutralize certain autoantibodies could be useful in treating post-COVID-19 condition patients with neurological symptoms such as fatigue. Therapeutic strategies could also include pharmacological agents that modulate the hypercoagulable state at different stages of the disease. In addition to the various pharmacological agents that have been proposed, apheresis has emerged as a contentious treatment targeting the neurological symptoms of the post-COVID-19 condition.
Apheresis, a technology that separates blood components to treat certain diseases, can be implemented to remove autoantibodies, neurotoxins (Bornstein et al, 2021), or microclots (Davies, 2022) in patients with post-COVID-19 condition and has been shown to slow cognitive decline in AD (Boada et al, 2020). This therapy remains controversial in post-COVID-19, however. Due to the complex and diverse nature of the post-COVID-19 condition, there could be several other potential strategies that modulate various systems. Continued research and trials are required to identify the most advantageous drugs for treating the neurological symptoms of the post-COVID-19 condition.
The role of immunosuppressants
Current evidence supports the notion that neurological impairment observed in COVID-19 patients is likely due to the CNS damage caused by the immune response triggered by SARS-CoV-2, rather than a direct consequence of the cytopathic effect of the virus (Pignataro et al, 2022). This inflammatory response to the virus is both local, activated by direct viral CNS invasion, and systemic, which, in turn, affects the BBB permeability allowing an influx of systemic cytokines within the brain (Correia et al, 2020). In some patients, the inflammatory response necessary to control SARS-CoV-2 replication induces a “cytokine storm,” leading to exaggerated systemic inflammation (Thepmankorn et al, 2021).
Cytokine levels are associated with disease severity: COVID-19 patients in the ICU have higher serum levels of cytokines compared with COVID-19 patients in the general wards (Huang et al, 2020). Also, critically ill patients have more frequent neurologic manifestations than patients with less severe illness (Liotta et al, 2020), still indirect evidence of the detrimental role of overactivated inflammation in the brain.
It has been investigated whether the mitigation of the uncontrolled inflammation may be protective for the neurological manifestations of COVID-19. Pignataro et al (2022) provided an interesting review on the potential neurological effects exerted by drugs targeting different cytokines, still under investigation in COVID-19. This article highlights relevant points that need to be addressed in future studies, such as: (1) identify cytokine patterns mainly involved in the acute and chronic nervous tissue damage; (2) once the best targets are identified, cytokine-based treatments will have specific pharmacological features depending on whether the neuropathological cytokines are CNS-synthesized or circulating; (3) understand the best timing of a treatment based on targeting cytokines, as the CNS and systemic inflammation occur later in the disease course; and finally, (4) how to balance the suppression of the cytokines with their positive role in virus replication control and neurogenesis.
Apart from the immunomodulant and immunosuppressive drugs under consideration for their efficacy and safety in COVID-19, it would be important to study the disease course in pathological or therapeutic immunosuppressant status, as an additional clue on the relationship between overactivated inflammation and neuro-COVID manifestations. For instance, the incidence and severity of neurological symptoms and syndromes could be explored, as well as long-term psychiatric and cognitive sequelae, in immunocompromised populations such as solid organ transplant (SOT) recipients.
It is still uncertain whether chronic use of immunosuppressive drugs worsens or improves clinical outcomes in COVID-19 patients, with convincing hypotheses for both possibilities (Andersen et al, 2021): On one hand, early immunosuppression would be detrimental, promoting virus replication and increasing the risk of opportunistic infections; on the other, immunosuppressants, at least theoretically, could counteract inflammatory response to virus replication, the main suspected contributing factor to neurological impairment. Also, some immunosuppressant agents, specifically calcineurin inhibitors (CNIs) and rapamycin inhibitors (mTORi), are known to inhibit virus replication (Hasbal et al, 2021; Kindrachuk et al, 2015; Ma-Lauer et al, 2020) and control cytokine synthesis.
Reported outcomes in SOT patients affected by COVID-19 are inconsistent. A number of studies have confirmed the vulnerability of SOT recipients to SARS-CoV-2 infection, with higher rates of SARS-CoV-2 RNAemia (Christensen et al, 2020), and higher mortality compared with the general population (Dumortier et al, 2021; Kedzierska-Kapuza et al, 2021; Requiao-Moura et al, 2021), whereas others find the opposite (Chavarot et al, 2021; Colmenero et al, 2021).
It is worth clarifying when a poor outcome is described if this is conditioned by the demographic fragile profile and by the burden of concurrent comorbidities in this specific population, or by immunosuppression alone (Linares et al, 2021). This clarification would be propaedeutic to determine whether it is better to withhold or to withdraw immunosuppression. Rituximab, for example, is an immunosuppressant drug used to treat rheumatological disease, the use of which has been found to be associated with an increased risk of in-hospital death due to COVID-19 (Anderson et al, 2022) and a prolonged infection time (Thornton et al, 2022).
Conversely, immunosuppressive corticosteroids, such as prednisone, may alleviate persisting neurological manifestations, possibly by regulating the altered adaptive immunity seen in patients with post-COVID-19 symptoms (Utrero-Rico et al, 2021). Further, the JAK-inhibitor baricitinib may also assist in reducing neurological manifestations of COVID-19. The appropriate management of different classes of immunosuppressive drugs should be addressed also from a neurological viewpoint, once the higher or lower risk of neuro-impairment in COVID-19 is described in this particular population.
In summary, the impact of immunosuppression in SARS-CoV-2 infected SOT recipients or other immunosuppressed conditions on the occurrence and severity of neurological consequences requires to be characterized in new well-designed clinical studies. Being a heterogenous group of therapies, it is worth exploring which category of immunosuppressant drugs is deleterious and which is protective for neurological manifestations, and at what point of the disease course should the immunological response activated by the virus be minimized. This would lead to a better pathogenetic understanding of the contribution of the cytokine storm on neurological symptoms of the post-COVID-19 condition.
Post-infection rehabilitation
Physical rehabilitation may provide a non-pharmacological approach to treat patients with neurological symptoms associated with the post-COVID-19 condition. A consensus statement from experts in rehabilitation, as well as other clinical fields, from the Defence Medical Rehabilitation Centre, Stanford Hall, United Kingdom, proposes recommendations for neurological rehabilitation after COVID-19 (Barker-Davies et al, 2020).
These recommendations highlight the importance of reviewing neurological symptoms and using cognitive screening tools, inpatient multidisciplinary rehabilitation for patients with moderate-to-severe neurological symptoms, and physical, cognitive, and functional assessments to support a return to work. A range of lifestyle changes is implemented, including pacing/energy management, strength training for muscular weakness, and smell/taste training for anosmia/ageusia.
Currently, several trials are ongoing to assess the use of certain technologies that could be implemented to reduce the impact of neurological symptoms after COVID-19. Trials of transcranial direct current stimulation for fatigue (NCT04876417), neurological rehabilitation combined with a rehabilitation robot for fatigue (NCT05130736), and Resistive Capacitive Monopolar Radio Frequency at 448 kHz to reduce pain and inflammation (NCT04920890) are all underway.
Similarly, mental health rehabilitation is important and will be useful for a patient's reintegration into society. The aforementioned Stanford Hall consensus statement suggests that reassurance should be given that milder neurological symptoms are likely to improve with limited intervention, whereas patients are also likely to fully recover from mild-to-moderate neurological symptoms (Barker-Davies et al, 2020). Mindfulness exercises may prove useful for patients experiencing mild anxiety or depression, whereas those with more severe neuropsychiatric manifestations associated with the post-COVID-19 condition could benefit from more intense therapeutic strategies such as counseling/psychotherapy, cognitive behavioural therapy, cognitive training, and occupational therapy.
Overall, the development of an effective program of physical and mental health rehabilitation to treat the neurological manifestations of the post-COVID-19 condition is salient and they should be tailored to the requirements of each patient on a patient-by-patient basis.
Conclusion
Overall, several questions remain regarding the pathogenesis and symptomatology of the neurological symptoms of the post-COVID-19 condition. With many millions of people having been infected with the virus, and many developing long-term manifestations after the acute infection that elicit deleterious effects on their quality of life, the creation of treatment and management strategies is vital to address the neurological symptoms of the post-COVID-19 condition. With studies beginning and ongoing, including studies involving members of this working group, the scientific community must aim at uncovering the mysteries surrounding the post-COVID-19 condition and the neurological sequelae it inflicts.
Footnotes
Authors' Contributions
This manuscript is the product of the weekly meeting of the European Working Group. P.E. along with all the collaborators (authors) were responsible for the conceptualisation and design of the manuscript. H.C. and A.R. led the writing of the original manuscript. All other authors contributed to different sections and critically reviewed and contributed to the writing and discussion of the manuscript. P.E. and H.C. revised and edited the final drafts.
Author Disclosure Statement
The authors report no competing financial interests.
Funding Information
No relevant funding was acquired for the production of this manuscript.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.