
Abstract
Background:
Understanding how brain function and language skills change during early (acute and subacute) stroke phases is critical for maximizing patient recovery, yet functional neuroimaging studies of early aphasia are scarce. In this pilot study, we used functional near-infrared spectroscopy (fNIRS) to investigate how resting-state functional connectivity (rs-FC) in early aphasia differs from neurologically healthy adults and is related to language deficits.
Materials and Methods:
Twenty individuals with aphasia (12 acute and 8 subacute phase) and 15 healthy controls underwent rs-fNIRS imaging with a 46-channel montage centered over bilateral perisylvian language areas. FC was computed using a prewhitening, autoregressive Pearson correlation routine applied to preprocessed oxyhemoglobin (HbO) data. Connections were classified as left intra-, right intra-, or interhemispheric. We then compared rs-FC between groups by connection type and examined Spearman correlations between rs-FC averages and language measures within patients.
Results:
Participants in the acute phase had significantly reduced global rs-FC across all HbO-based connections compared to healthy controls. No significant differences were found in rs-FC between controls and patients in the subacute phase. Controlling for days since stroke, stronger right intra- and interhemispheric rs-FC was related to milder aphasia across all patients. Exploratory correlations revealed that relationships between language measures and rs-FC differed between acute and subacute patient groups.
Conclusion:
This study provides preliminary evidence that fNIRS-based rs-FC measures may be a viable metric to index the early impacts of stroke in people with aphasia.
Impact statement
Questions regarding the nature of neural recovery in early poststroke aphasia mostly remain unanswered, largely due to the shortage of functional imaging studies in this population. Logistical challenges of magnetic resonance imaging are central barriers to early stroke imaging. Functional near-infrared spectroscopy (fNIRS) is a promising alternative as it is relatively inexpensive and portable. Resting-state functional connectivity (rs-FC) provides an avenue to avoid the confounds of task demands and difficulties inherent in task-based imaging studies. The importance of this pilot study lies in its first-ever application of fNIRS-based rs-FC to investigate brain–behavior relationships in acute and subacute aphasia.
Introduction
Stroke is a leading cause of adult long-term disability for more than 15 million individuals who experience a new stroke each year (Strong et al., 2007; Virani et al., 2021). One of the most life-changing poststroke conditions is aphasia, a communication disorder characterized by receptive and/or expressive language deficits due to damage in the language-dominant (typically left) hemisphere. Approximately 30% of stroke survivors present with aphasia in the acute (i.e., <2 weeks poststroke) hospital setting, with aphasia persisting in around 16–30% of these individuals by 1 year poststroke (Flowers et al., 2016). Aphasia adds to the cost of stroke-related care in both acute (Boehme et al., 2016) and chronic (Flowers et al., 2016) stages and has a high negative impact on health-related quality of life (Hilari et al., 2003; Lam and Wodchis, 2010).
Because of the negative consequences of persistent aphasia, a priority in patient care must be early and effective intervention to maximize recovery before the onset of the chronic time point (i.e., around 6 months poststroke), after which the extent and rate of recovery slow. In the first hours to days following a stroke (the acute phase), recovery is mediated by medical interventions (e.g., thrombolytic therapy) and/or the spontaneous resolution of ischemic events (e.g., cerebral edema, hypoperfusion) (Cramer, 2008; Hartwigsen and Saur, 2019; Hillis and Heidler, 2002; Kiran, 2012). Before such recovery, the neurophysiological consequences of acute ischemia can cause hypometabolism throughout the brain that manifests as widespread decreases in activation or connectivity in functional imaging studies. In the subacute phase and beyond, recovery of language is driven by behavioral intervention.
The efficacy of speech-language therapy is contingent on the capacity of treatments to promote neural plasticity, characterized by functional reorganization of the language system through which intact brain regions presumably assume new or extended functions to compensate for damaged left hemisphere (LH) tissue (Hartwigsen and Saur, 2019; Hillis and Heidler, 2002; Kiran, 2012; Stefaniak et al., 2020; Turkeltaub, 2019).
A prevailing debate within aphasiology has revolved around whether neural plasticity occurs within residual LH tissue in the premorbid language network, homotopic right hemisphere (RH) regions of damaged LH areas, areas implicated in domain-general processes outside the canonical language network, or some combinations of the above (Stefaniak et al., 2020; Wilson and Schneck, 2020). A scant minority of functional imaging studies weighing in on this debate have included people with aphasia (PWA) in the acute or subacute phases of recovery (Stefaniak et al., 2021). The results of the few existing longitudinal early aphasia recovery studies are highly variable with small samples (Kwon et al., 2017; Long et al., 2018; Nenert et al., 2018; Saur et al., 2006; Sebastian et al., 2016; Stockert et al., 2020; Yang et al., 2017; Zhu et al., 2014), yet the most consistent finding is that persistent language impairment is associated with decreased LH activity or connectivity.
The dearth of early aphasia recovery neuroimaging studies is perhaps unsurprising due to the logistical challenges (e.g., cost, access, contraindications) of the most-often used functional imaging modality, functional magnetic resonance imaging (fMRI). As an alternative to fMRI, functional near-infrared spectroscopy (fNIRS) is a low-cost, portable, and noninvasive neuroimaging method that can be used in a variety of settings (e.g., at bedside, within the clinic) and allows for greater flexibility and better patient access to research opportunities than fMRI. While fNIRS has its limitations (e.g., inability to capture signals from deep brain structures, poorer spatial resolution than fMRI, poorer temporal resolution than electroencephalography [EEG]), its additional advantages (e.g., greater temporal resolution than fMRI, safety for patients with MR contraindications, higher robustness to motion artifacts than fMRI or EEG) make it an ideal imaging modality to study clinical populations (Boas et al., 2014; Butler et al., 2020).
fNIRS capitalizes on the absorption sensitivity of hemoglobin chromophores (i.e., oxyhemoglobin [HbO] and deoxyhemoglobin [HbR]) to different wavelengths of light (typically between 650 and 900 nm) and the fact that changes in hemoglobin concentration over time reflect changes in the hemodynamic response (Boas et al., 2014). HbO and HbR are both highly correlated with the blood-oxygen-level-dependent signal in fMRI (Huppert et al., 2006; Strangman et al., 2002). HbO has better signal-to-noise than HbR (Pan et al., 2019; Strangman et al., 2002), and as such, we elected to focus on HbO in this study.
Similar to fMRI, fNIRS can be used to measure functional connectivity (FC)—that is, temporal correlations in fNIRS signals—during task or rest. Use of resting-state (rs) imaging over task-based sequences has been suggested for PWA to avoid potential confounds of task type and difficulty (Klingbeil et al., 2019). Thus far, none of the five existing fNIRS studies in poststroke aphasia (Chang et al., 2022; Gilmore et al., 2021; Hara et al., 2017; Merzagora et al., 2008; Obayashi, 2020; Sakatani et al., 1998) incorporated fNIRS-based rs-FC measurements or centered on early poststroke aphasia recovery.
Therefore, this pilot study has two aims. First, we aimed to assess the viability of rs-fNIRS as an alternative to fMRI by characterizing how rs-FC patterns (in terms of left intrahemispheric, right intrahemispheric, and interhemispheric connectivity) differ between (1) PWA in the acute phase, (2) PWA in the subacute phase, and (3) neurologically healthy controls. Based on the knowledge of the neurophysiological consequences of stroke (Cramer, 2008; Hartwigsen and Saur, 2019; Hillis and Heidler, 2002; Turkeltaub, 2019) and consistent with prior evidence in acute aphasia (Kwon et al., 2017; Nenert et al., 2018; Saur et al., 2006; Stockert et al., 2020), we hypothesized that acute functional brain patterns would be characterized by global reductions in rs-FC compared to healthy controls. Studies generally have reported that activity or connectivity increases from the acute to subacute phases in PWA (Kwon et al., 2017; Nenert et al., 2018; Saur et al., 2006; Stockert et al., 2020), and thus, we expected to observe global hyperconnectivity in subacute compared to acute patients.
Second, we sought to determine relationships between fNIRS rs-FC patterns and language deficits in PWA in the acute and subacute recovery phases. While not specific to aphasia, Siegel et al. (2016) interrogated relationships between fMRI-based rs-FC and language skills in 98 LH and RH stroke survivors at 1–2 weeks post-stroke and found that patients with the poorest language outcomes (likely PWA) demonstrated reduced interhemispheric homotopic connectivity and decreased left intrahemispheric connectivity, particularly within the auditory network. This latter finding accords with the limited early stroke connectivity work specifically in PWA (Kwon et al., 2017; Sebastian et al., 2016; Zhu et al., 2014), and therefore, we also hypothesized that stronger left intrahemispheric and possibly greater interhemispheric rs-FC would be associated with better language abilities in acute and subacute stroke survivors.
Materials and Methods
Participants
Individuals with a history of a recent LH ischemic infarct who participated in one of two ongoing studies at Johns Hopkins School of Medicine were recruited for this study. In addition to LH stroke, the inclusion criteria for patients were (1) normal or corrected-to-normal vision and hearing, (2) no history of other neurological disease affecting the brain besides prior small lacunes, (3) presence of aphasia as determined by the Western Aphasia Battery-Revised (WAB-R) (Kertesz, 2007), and (4) adequate alertness to engage in behavioral testing and fNIRS imaging.
The final patient sample included 20 participants with aphasia, including 2 groups, distinguished by time postonset: (1) 12 PWA (mean age: 63.2 ± 11.5 years, mean education: 14.9 ± 2.2 years, 2 women, 11 right-handed) in the acute poststroke phase (mean time poststroke: 5.9 ± 3.1 days) and (2) 8 PWA (mean age: 62.6 ± 14.5 years, mean education: 15.5 ± 2.4 years, 2 women, 7 right-handed) in the subacute poststroke phase (mean time poststroke: 47.9 ± 20.0 days) at the time of study enrollment. See Table 1 for patient demographic and stroke information.
Demographic, Stroke, and Language Data in Participants with Aphasia
Object naming as per the BNT.
Action naming as per the HANA.
AQ, aphasia quotient; AVC, auditory verbal comprehension; BNT, Boston Naming Test; HANA, Hopkins Action Naming Assessment; N/A, not administered; N/R, no response; NWF, naming and word finding domain scores; PWA, people with aphasia; Rep, repetition; SS, spontaneous speech; TMA, transcortical motor aphasia; TSA, transcortical sensory aphasia; WAB-R, Western Aphasia Battery-Revised.
A group of 15 neurologically healthy adults also participated in the study (mean age: 58.9 ± 17.4 years, mean education: 17.6 ± 2.9 years, 4 women, 14 right-handed). Inclusion criteria for healthy controls were (1) normal or corrected-to-normal vision and hearing, (2) no history of neurological disease affecting the brain, and (3) adequate alertness to engage in fNIRS imaging.
Study protocols were approved by the Institutional Review Board at Johns Hopkins University and adhered to the Declaration of Helsinki. All participants provided their verbal assent, and they or their health care proxy (in the case of PWA with impaired comprehension) provided written informed consent.
Behavioral testing protocol
Upon study entry, all PWA were administered part 1 of the WAB-R to determine their aphasia classification and overall aphasia severity as per the Aphasia Quotient, a summary measure that reflects performance on multiple subtests of spontaneous speech, auditory verbal comprehension, repetition, and naming and word finding abilities. Given that word retrieval difficulties are the most common and persistent deficits in chronic aphasia (Goodglass and Wingfield, 1997) and that naming recruits the majority of canonical language network regions (Indefrey and Levelt, 2004), we also administered the Boston Naming Test (BNT) (Kaplan et al., 2001) and the Hopkins Action Naming Assessment (Breining et al., 2021) to further characterize object and action naming impairments, respectively. See Table 1 for language scores.
Neuroimaging protocols
Structural imaging
PWA underwent structural imaging either as part of their routine clinical care or research participation. To estimate stroke volumes, trained technicians initially blinded to language data manually traced lesioned tissue in the axial plane of diffusion-weighted images (DWI; n = 16 patients), T1- or T2-weighted images (n = 2), or computed tomography scans (n = 1). * We subsequently warped lesion maps to a standard template using the Clinical Toolbox (Rorden et al., 2012) in SPM12 and estimated lesion volumes in MATLAB based on routines from MarsBaR (Brett et al., 2002).
fNIRS imaging
During fNIRS imaging, source optodes (i.e., low-powered light-emitting diodes) situated on a cap worn by the participant project near-infrared light through the scalp into the brain. Detector optodes affixed to the cap capture the optical signal re-emerged from the head surface after it interacts with hemoglobin chromophores in cortical tissue. Each source-detector pair forms a measurement channel, and cortical brain activity at a depth of ∼1–3 cm is measured at the midpoint of each measurement channel. During data processing, changes in chromophore intensity are converted to changes in optical density, which are in turn transformed into relative changes in oxygenated and deoxygenated hemoglobin, providing an indirect measure of brain activity.
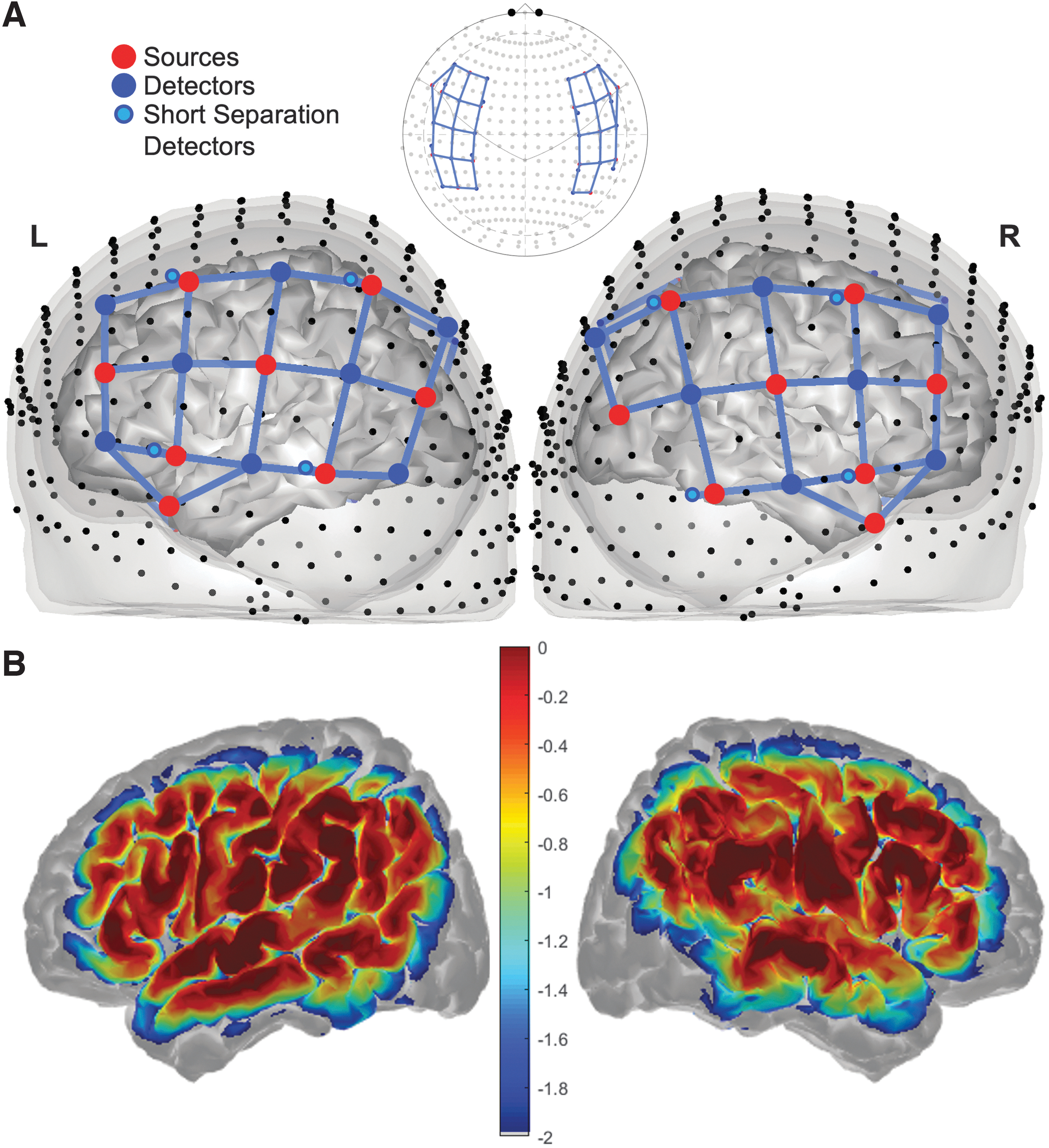
In our study, we acquired fNIRS data using an NIRx NIRSport2 device. Sixteen sources (8 per hemisphere) and 16 detectors (8 in the LH and 7 in the RH) formed a total of 46 long-distance measurement channels arranged over LH perisylvian language areas (24 channels) and their RH homologues (22 channels). In addition, eight short-separation detectors affixed near sources were used to obtain shallow measurements of physiological noise (e.g., blood flow and oxygenation changes in the scalp). Of note, a detector in the RH and two corresponding RH long-distance channels were sacrificed to form the short-distance channels, resulting in the hemispheric difference in number of channels. The montage situated on the scalp surface is shown in Figure 1A. Figure 1B shows the sensitivity profile of the montage projected onto the brain, illustrating areas of higher (warmer colors) and lower (cooler colors) measurement sensitivity.
At the beginning of each fNIRS session, the examiner situated the appropriately sized cap on the participant's head, ensuring correct placement based on the location of fiducial markers (e.g., center of the cap, Cz) relative to the participant's anatomy (e.g., nasion, inion, and preauricle points). Signal quality (i.e., signal-to-noise ratios, dark noise levels) was checked using the NIRx-provided fNIRS acquisition software, Aurora. For channels with poor signal, the examiner took extra measures to block environmental light and ensure adequate optode-to-scalp coupling (by e.g., moving hair aside, placing higher-tension spring-loaded tops over problematic optodes). Participants then completed two runs of a 7-min, 14-sec resting-state sequence. † Data were recorded in Aurora at a sampling rate of 7.6 Hz. During fNIRS acquisition, participants were instructed to stay as still as possible with eyes open and fixated on a cross on a monitor in front of them.
We used the NIRS Brain AnalyzIR Toolbox (Santosa et al., 2018) to preprocess the data. Preprocessing steps included (1) raw data to optical density conversion, (2) data resampling to 1 Hz to reduce autocorrelation, (3) optical density to hemoglobin conversion via the Modified Beer-Lambert Law (Kocsis et al., 2006) with a partial path length factor of 1, and (4) removal of shallow physiological noise via the short distance filter routine as per recommendations described in Santosa et al. (2020) that can be applied to rs-fNIRS data. To further reduce serial correlations in the time series, account for statistical outliers due to motion artifacts, and reduce the likelihood of type I errors in fNIRS rs-FC data, we followed recommendations from Santosa et al. (2017) and applied a prewhitening, robust fit Pearson correlation model to the processed hemoglobin data.
This approach resulted in a 46 × 46 correlation matrix for each run, reflecting channel-to-channel pairwise FC between the 46 montage channels. We extracted Fisher-transformed Z values for each connection for oxyhemoglobin (i.e., HbO-HbO correlation coefficients). After removing 24 LH self-connections (e.g., channel 1-to-channel 1 values) and 22 self-connections in the RH, the final matrix included 276 left intrahemispheric, 231 right intrahemispheric, and 528 interhemispheric correlation coefficients per participant and run. Additional statistical analyses completed within and outside of the AnalyzIR Toolbox are described below.
Statistical approach
For aim #1, we first conducted second-level analyses within each group (i.e., PWA in the acute phase, PWA in the subacute phase, and healthy controls) within the AnalyzIR Toolbox using the MixedEffectsConnectivity routine, predicting Z correlation coefficients from the condition of rest and random intercepts of subject and run; connectivity maps were corrected at the connection level at a false discovery rate (FDR) of q < 0.05. To address our research question with regard to connectivity patterns, we labeled each participant's extracted Z values by connection type (i.e., left intrahemispheric, right intrahemispheric, or interhemispheric connection). All connections were included in the subsequent analyses. We then conducted a series of linear mixed-effects models using the lmerTest package (Kuznetsova et al., 2017) in R, with Z values as the dependent variable, group as the independent variable, and random intercepts of subject and run for each model.
We compared connectivity coefficients between PWA in the acute phase and healthy controls, PWA in the subacute phase and healthy controls, and PWA in the two recovery stages with each other across all connections and across each connection type, resulting in four models for each set of group comparisons. We applied an FDR correction at q < 0.05 at the model level.
For aim #2, we first averaged the connectivity coefficients by connection type for each participant with aphasia. To determine relationships between language skills and rs-FC, we conducted partial Spearman correlations between these averaged connectivity values and language measures (i.e., WAB-R Aphasia Quotient and BNT total accuracy), controlling for days since stroke onset across PWA. We next conducted Spearman correlations between language and rs-FC measures within separate patient groups, applying an FDR correction at q < 0.05 across all correlations within each set of tests.
Data availability
Data will be made available upon reasonable request.
Results
First, we conducted a series of analyses to determine whether groups differed by demographics or, in the case of the patient groups, lesion size. Confirmed via Wilcoxon rank sum and chi-square tests, controls were matched to PWA in age (W = 128.50, p = 0.484), sex (χ 2 = 0.003, p = 0.954), and handedness (χ 2 = 0.802, p = 0.670). In contrast, controls had significantly more years of education than PWA (W = 213.50, p = 0.013). To ensure this group difference did not influence the results, we reran the models comparing rs-FC between controls and the patient groups controlling for years of education.
The acute and subacute PWA groups did not differ in demographics (p > 0.337 across tests). Lesion volumes are reported in Table 1. A lesion overlay map across all PWA is shown in Figure 2A, with lesion overlays for PWA in the acute and subacute phases shown in Figure 2B and C, respectively. As a group, PWA in the subacute phase tended to have larger lesions than PWA in the acute stroke stage (W = 23.00, p = 0.059). However, across patients, lesion volume was not significantly associated with average rs-FC values for any connection (p > 0.538 across tests, Table 2).
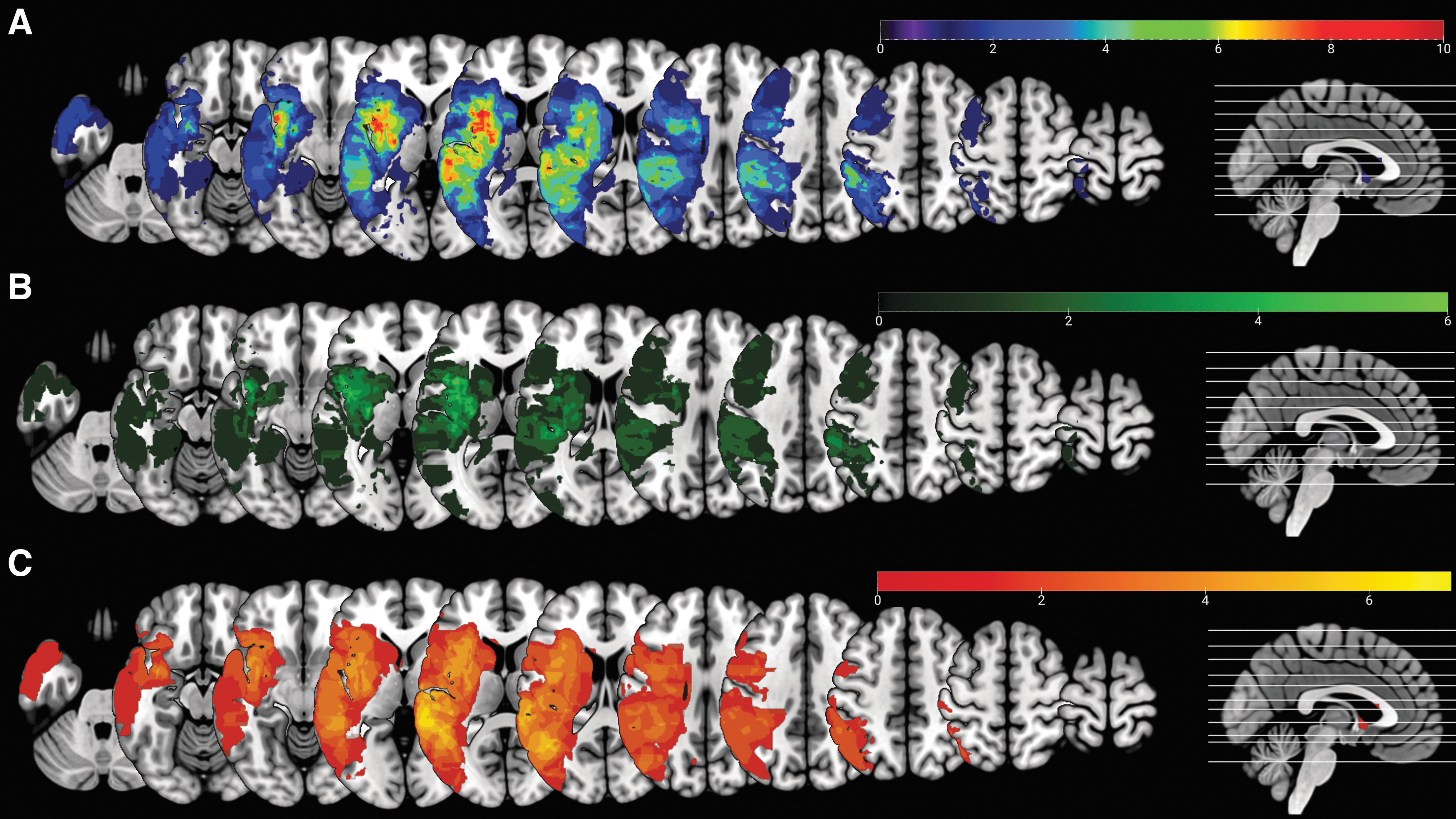
Lesion overlay maps in PWA, including
Relationship Between Resting-State Functional Connectivity and Language Abilities in All People with Aphasia (n = 20), Controlling for Days Poststroke Onset
For language analyses, multiple comparison correction was done at a false discovery rate of q < 0.05.
Avg. InterHem, average interhemispheric functional connectivity; Avg. IntraLH, average left intrahemispheric functional connectivity; Avg. IntraRH, average right intrahemispheric functional connectivity.
Aim #1: between-group differences in fNIRS rs-FC
Connectivity maps that reflect significant connections after FDR correction at the connection level within each group are shown in Figure 3A. Violin plots that depict rs-FC by group and connection type are included in Figure 3B.

Compared to healthy controls, patients in the acute phase had significantly weaker connectivity across all connections within the montage (β = −0.220, standard error [SE] = 0.056, t = −3.896, q = 0.009); this included significantly weaker FC for left intrahemispheric (β = −0.209, SE = 0.061, t = −3.400, q = 0.023), right intrahemispheric (β = −0.195, SE = 0.061, t = −3.186, q = 0.013), and interhemispheric (β = −0.236, SE = 0.056, t = −4.241, q = 0.008) connections. Including years of education as a nuisance regressor slightly altered the strength, but not the direction of group differences, and no changes were observed in model significance (Supplementary Table S1).
PWA in the subacute phase at study enrollment did not significantly differ from controls in terms of functional coupling across all connections (β = 0.025, SE = 0.094, t = 0.271, q = 0.987) despite demonstrating generally higher mean rs-FC than controls. These groups did not statistically differ in the strength of connections within the LH (β = 0.039, SE = 0.090, t = 0.435, q = 0.987), within the RH (β = 0.023, SE = 0.099, t = 0.230, q = 0.987), or between hemispheres (β = 0.020, SE = 0.098, t = 0.207, q = 0.987). There were no notable changes to these comparisons when including years of education as a nuisance regressor in the models (Supplementary Table S1).
Aligning with the other sets of results, we found that PWA in the acute phase demonstrated significantly weaker rs-FC than PWA in the subacute phase. Specifically, PWA in the acute stage had significantly weaker rs-FC across all montage connections (β = 0.245, SE = 0.083, t = 2.948, q = 0.011), including connections within the LH (β = 0.243, SE = 0.077, t = 3.155, q = 0.011), within the RH (β = 0.219, SE = 0.095, t = 2.298, q = 0.034), and between hemispheres (β = 0.259, SE = 0.087, t = 2.968, q = 0.011).
To account for the fact that these models contain multiple measurements per participant, we conducted two sets of follow-up analyses. First, for each group comparison, we conducted two-sample t-tests for each connection, correcting for multiple comparisons (Supplementary Tables S2–S4). Second, we averaged connectivity values for each participant by type and compared averaged connectivity via one-way analyses of variance (Supplementary Table S5). Although many between-group comparisons at the connection level did not survive multiple comparison correction, the overall pattern of the results in these two sets of follow-up analyses remained the same as the original models, that is, that acute PWA had significantly lower connectivity across connection types than the other two groups, but subacute PWA and controls did not differ from each other.
Aim #2: relationships between language deficits and fNIRS rs-FC in PWA
The results of the partial correlations between language data and fNIRS rs-FC correlation coefficients across all PWA are summarized in Table 2. Controlling for days poststroke onset, we found that stronger rs-FC within the RH and between hemispheres was significantly related to higher WAB-R Aphasia Quotients (r = 0.546, p = 0.015, q = 0.023) and better word retrieval as per the BNT (r = 0.588, p = 0.008, q = 0.023). Relationships between rs-FC and language measures within each patient group are depicted in Figure 4 and summarized in full in Supplementary Table S6. While none of these results was significant (q > 0.05), the trends by patient group can assist in the interpretation of the partial correlation findings, which we address in further detail in the Discussion section.

Relationships between fNIRS rs-FC and overall aphasia severity and naming abilities within each patient group. BNT, Boston Naming Test; InterHem, interhemispheric connections; IntraLH, left intrahemispheric connections; IntraRH, right intrahemispheric connections; WAB-R AQ, Western Aphasia Battery-Revised Aphasia Quotient.
Discussion
In this study, we investigated how patterns of fNIRS rs-FC in early poststroke aphasia differed from neurologically healthy adults and were related to language impairments. We found that compared to neurologically healthy controls, PWA enrolled in the study at the acute phase had global reductions in rs-FC within our language network montage, including weaker rs-FC within each hemisphere and between hemispheres for all connections. In contrast, there were no significant differences between healthy controls and individuals in the subacute phase of recovery, but notably, average rs-FC tended to be higher in these PWA than controls at a group level. Controlling for days postonset, we found that across the entire group of PWA, greater right intra- and interhemispheric connectivity was significantly related to less severe aphasia with similar trends by connection type for naming abilities.
Comparisons of fNIRS rs-FC across groups
As predicted, the results of our cross-sectional comparisons between PWA in the acute phase and healthy controls align with global reductions in brain function reported in PWA at the acute stage in previous studies of rs-FC (Kwon et al., 2017; Sebastian et al., 2016) and task-based activation (Fig. 3) (Nenert et al., 2018; Saur et al., 2006; Stockert et al., 2020). Siegel et al. (2016) found that compared with rs-FC in controls, reduced interhemispheric homotopic connectivity characterized rs-FC of several cognitive and sensorimotor networks in patients at 1–2 weeks post-LH or RH stroke, a pattern they suggested was a network phenotype of stroke injury at that stage. However, the phenotype reported by Siegel et al. (2016) did not include reduced intrahemispheric connectivity, unlike the findings of the present and aforementioned aphasia studies.
Another study with contrasting findings is that by Yang et al. (2017), who instead found that 37 PWA in the acute phase (<4 days) after lacunar infarct demonstrated increased voxel-mirrored homotopic connectivity compared with healthy controls. The manifestation of hypo- versus hypermetabolism after infarct depends on stroke severity and extent as well as the timing of ischemic events and their resolution (Hartwigsen and Saur, 2019; Hillis and Heidler, 2002), all of which vary greatly from person to person. Nonetheless, aphasia is most often caused by a relatively large, cortical infarct, so it stands to reason that the disruptions in metabolic processes would be widespread in most acute PWA—including the current sample. In contrast, metabolic abnormalities may occur more locally in studies that definitely (Yang et al., 2017) or likely (Siegel et al., 2016) included patients with smaller strokes or may manifest as hyperconnectivity compared with controls as patients recover (perhaps as in Yang et al., 2017).
Related to this latter point, the upregulation of brain activity in subacute stroke is considered a key recovery mechanism at this stage (Hartwigsen and Saur, 2019; Hillis and Heidler, 2002; Saur et al., 2006; Stockert et al., 2020). Consistent with this notion, subacute patients in the present study had significantly stronger rs-FC than acute patients for all connections and trended toward greater rs-FC than controls (Fig. 3). These findings align with results from a seminal study by Saur et al. (2006) who reported that by the early subacute phase (around 2 weeks poststroke), 14 PWA exhibited an upregulation of activation in bilateral regions that exceeded acute-stage activation as well as activity levels in healthy controls.
However, despite visible differences in rs-FC between controls and subacute PWA at the group level (Fig. 3), we found no statistical differences between groups, likely due to a high degree of interindividual variability within our small subacute sample. Neural plasticity during the subacute phase is time dependent (Hillis and Heidler, 2002; Stockert et al., 2016; Turkeltaub, 2019), and thus, one reason for high variability in rs-FC values within the subacute group may have been differences between patients in time since stroke onset. Interindividual differences in lesion location likely also contributed to the variability in subacute rs-FC values. Stockert et al. (2020) found that PWA with anterior lesions engaged spared temporal cortex even during the acute phase, whereas frontal lobe engagement occurred later in the recovery time course for PWA with posterior lesions.
Consistent with the notion that resolution of diaschisis contributes to recovery, Wawrzyniak et al. (2022) found that compared to brain areas with low lesion connectivity, regions with high lesion FC demonstrated a greater increase in language network reactivation from the acute to subacute phases in 71 PWA. Due to the small sample and other methodological limitations (see Limitations and Future Considerations), we were unable to interrogate how rs-FC varied by lesion site, but this remains an important future direction of rs-fNIRS work in stroke patients.
Relationships between fNIRS rs-FC and language abilities in PWA
Contrary to our hypotheses, we found no significant relationships between left intrahemispheric rs-FC and language abilities in our combined sample of acute and subacute PWA (Table 2). The pattern of stronger left intrahemispheric connectivity coinciding with better language skills is an often-reported finding in prior studies of early stroke (Kwon et al., 2017; Sebastian et al., 2016; Siegel et al., 2016; Zhu et al., 2014) as well as chronic aphasia (e.g., Chu et al., 2018; Hallam et al., 2018; Harvey et al., 2013; Meier et al., 2018; Tao and Rapp, 2020). Nonetheless, trends between increased left intrahemispheric rs-FC and less severe aphasia and better naming were found, similar to the direction of associations between language measures and other connection types across the combined sample.
While merging patient groups improved statistical power and allowed for testing a hypothesis that applied to both acute and subacute stroke stages, the mixed chronicity of the group resulted in nuanced relationships between language and left intrahemispheric connectivity to be lost. Interestingly, within the subacute group, the strongest (although not significant) relationship between rs-FC and language metrics was a positive correlation between left intrahemispheric rs-FC and the WAB-R Aphasia Quotient (Fig. 4), meaning that individuals with stronger rs-FC tended to have milder aphasia.
While not predicted, an association between RH engagement and good language performance in acute/subacute aphasia is not without precedence (Saur et al., 2006; Stockert et al., 2020; Zhu et al., 2014). The significant relationship between higher right intrahemispheric connectivity and better WAB-R and BNT scores in the combined-sample partial correlations was likely driven by the acute patients (Table 2). In contrast, the positive relationship between the WAB-R Aphasia Quotient and interhemispheric connectivity trended in both patient groups (Fig. 4), likely leading to the significant combined sample result. As part of their network phenotype, Siegel et al. (2016) similarly found that higher interhemispheric connectivity weights (indicative of stronger connectivity) were related to better behavioral performance across sensorimotor and cognitive domains, although it should be noted that their language analysis subsample of 98 patients included only 31 PWA.
While the relationships between fNIRS rs-FC and language metrics appear promising, it is important to emphasize the exploratory nature of these analyses, in particular the low-powered correlations conducted within each patient group. Even more importantly, aphasia is a heterogeneous disorder, and the fact that our acute and subacute analyses were not performed on the same, longitudinal sample diminishes the generalizability of our findings.
Limitations and future considerations
Additional limitations of this pilot study must be acknowledged. We created our montage to align with regions associated with language activity based on prior neuroimaging reviews and meta-analyses (Indefrey and Levelt, 2004; Price, 2012; Stefaniak et al., 2021; Wilson and Schneck, 2020), but it lacked whole brain coverage due to the number of optodes at our disposal and the inability of fNIRS to sample deep brain structures. Without control channels (i.e., channels unexpected to change), we cannot ascertain whether the patterns observed in aim #1 were specific to language areas. We were also unable to attempt replication of some important findings demonstrated in other studies.
For example, Siegel et al. (2016) found that decreased homotopic network connectivity was associated with increased segregation of ipsilesional networks (particularly the dorsal attention network) from the default mode network, a finding that has implications for the balance between network integration and segregation in early stroke recovery. However, examining default mode network connectivity was not possible due to poor sampling of medial structures and limited coverage of other network regions within our montage.
Our connection type approach was informed by the literature but also by our inability to ensure precise spatial correspondence of channels to anatomical regions of interest due to the lack of source localization. The combined factors of our small sample, no source localization, and lack of domain-general coverage meant that we were unable to address more nuanced questions regarding how rs-FC varied by region and lesion location. Relatedly, we did not mask out lesioned tissue due to the absence of precise lesion-to-channel correspondence. In fMRI, cost function masking and other methods for dealing with lesioned tissue are often used, yet the lesion remains largely unaddressed in fNIRS stroke studies to date (cf. Gilmore et al., 2021).
Finally, we decided to only include HbO-based rs-FC metrics given the exploratory nature of this study and advantages of HbO over HbR. Nonetheless, the utility of HbO versus HbR measures in the study of human cognition and stroke recovery remains an open question in the fNIRS literature and must be investigated more thoroughly in future work.
Conclusion
In this study, we found that PWA in the acute poststroke phase exhibited global reductions in fNIRS-based rs-FC compared to PWA in the subacute phase and neurologically healthy adults. Controlling for time since stroke, we also found that stronger right intrahemispheric and interhemispheric connectivity was associated with better language abilities across all PWA. To our knowledge, this is the first study to investigate rs-FC in early stroke-induced aphasia using fNIRS. Despite several limitations, this pilot study demonstrates that fNIRS imaging in early stroke aphasia is not only possible but yields potentially important information about brain–behavior relationships in these understudied poststroke time points. Important future directions include addressing methodological concerns in fNIRS imaging specific to stroke (e.g., lesion masking) and longitudinal investigation of brain–behavior relationships using fNIRS in PWA along the acute-to-chronic recovery time line.
Footnotes
Acknowledgments
Research assistants in the Stroke Cognitive Outcomes and REcovery (S.C.O.R.E.) Lab were instrumental in administering behavioral assessments to participants with aphasia. We extend our thanks to all individuals who participated in the study and made this work possible.
Authors' Contributions
E.L.M.: Conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, visualization, and project administration. L.D.B.: Conceptualization, methodology, investigation, data curation, writing—review and editing, and project administration. H.K.: Conceptualization, methodology, investigation, data curation, writing—review and editing, and project administration. A.E.H.: Conceptualization, resources, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by the National Institutes of Health, National Institute on Deafness and Other Communication Disorders grants R01DC005375 and P50DC014664.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.