
Abstract
Introduction:
The purpose of this study was to monitor and record the dynamic brain activity of patients with moyamoya disease (MMD), as well as to study the relationship between brain abnormalities and presenting clinical features.
Methods:
A total of 16 patients with MMD (2 males and 14 females) were invited to participate in the study, as were healthy controls (HCs) with the same number and sex ratio. In this study, the dynamic amplitude of low-frequency fluctuation (dALFF) was utilized to assess changes in spontaneous brain activity. Moreover, we also used correlation analysis to study the relationship among the measured mean of dALFF, behavioral performances, and the retinal nerve fiber layer and the Hospital Anxiety and Depression Scale (HADS) score to explore the potential relationship between MMD and anxiety and depression.
Results:
Our study reveals that in MMD, dALFF levels decreased in the left lingual gyrus, right insula, and occipital lobe.
Discussion:
In this study, we found and discussed the potential relationship between the abnormal activities in multiple brain regions and related functional network disorders in patients with MMD, as well as the damage to brain regions that process emotion and vision, in the hopes of providing more ideas for the clinical diagnosis and treatment of MMD.
Impact statement
The current studies do not provide a definitive understanding of the specific process and consequences of moyamoya disease. In this study, we evaluate the dynamic amplitude of low-frequency fluctuation to clarify the impact of Moyamoya disease on ocular disorders and aberrant brain function. We report functional impairments and potential consequences of the left lingual gyrus, right insula, and right occipital lobe, along with the associations between anxiety and depression ratings and specific brain regions. Our study helps facilitate the clinical diagnosis and treatment and appeals to healthcare professionals to focus on and prevent complications of Moyamoya disease.
Introduction
Moyamoya is the name given to a disorder characterized by the smog-like appearance of blood vessels on cerebral angiography. Moyamoya disease (MMD) is caused by arterial constriction or obstruction, such as the proximal carotid artery, which leads to abnormal proliferation of small blood vessels (Suzuki and Takaku, 1969). People with MMD may not have obvious symptoms in the early stages, but as the number of proliferating blood vessels increases, patients can experience symptoms such as headache and seizures (Sato et al., 2019). The most common clinical sign is cerebral ischemia, which can cause cerebral infarction or, in severe instances, death.
Previous research has found that MMD is present throughout the world, but it has a high incidence in East Asian countries such as Japan, China, and South Korea. Studies in Japan showed that the incidence and prevalence of MMD were lower than 0.001% and 0.01%, respectively (Baba et al., 2008), and there was a high possibility of occurrence around age 10 and 30–45 years (Fujimura et al., 2016). According to a survey from China, males had a lower frequency of MMD than females and ∼10% of MMD patients had a positive family history (Miao et al., 2010).
However, so far, the underlying pathogenesis of MMD is unclear and available therapeutic options are limited. Research has concentrated on elucidating its etiology.
Recent research on endothelial cells in cerebrovascular biology has focused on their critical function in vascular lesions, with one study discovering that intimal hyperplasia and abnormal angiogenesis occur in MMD (Pías-Peleteiro et al., 2016).
Such findings suggesting that patients with MMD may be more disposed to endothelial dysfunction have triggered research interest in the role of endothelial progenitor cells in the pathogenesis of the disease, with some progress (Yu et al., 2020). Other studies have focused on cerebral blood flow and found that narrowing or even occlusion of large blood vessels in areas such as the brain and neck can significantly reduce blood flow to the brain, leading to multiple brain injuries and an increased risk of stroke (Ladner et al., 2017), consistent with the clinical diagnosis and characteristics of MMD.
According to earlier studies, MMD not only affects the brain but also has links to eye diseases such as central retinal artery occlusion and ocular ischemia syndrome. Defects in neuroectoderm development (Bayan Al Othman, 2019) and subsequent mesodermal changes may be responsible for this association. Retinal examination is one of the primary means of preventing severe vision loss caused by MMD, although ophthalmic diseases do not usually present independently.
Methods used in detection and diagnosis of MMD include digital subtraction angiography (DSA) and magnetic resonance imaging (MRI). DSA is a commonly used method with clear imaging and high resolution, which aids in the observation of lesions and the location, measurement, and diagnosis of vascular stenosis and occlusion and is the main diagnostic method for MMD, but this method presents some risks.
DSA is an invasive test that requires a puncture and contrast injection around the groin. However, since the vessel wall plaque may separate, it might result in certain complications, such cerebral infarction (Al-Mufti et al., 2017). MRI examination is a commonly used imaging-assisted diagnostic method (Li et al., 2019). It uses magnetic resonance to detect electromagnetic signals from the body and provide relevant data.
There is growing evidence that brain activity and function are dynamic. Dynamic amplitude of low-frequency fluctuation (dALFF) is a type of functional MRI (fMRI) method based on synchronous electroencephalography power fluctuation, which can detect the dynamic brain activity changing with time (Li et al., 2016; Min et al., 2018; Wu et al., 2019). Unlike traditional static ALFF, dALFF focuses on temporal variability. So far, dALFF analysis has been widely used for neurological and brain-related diseases such as diabetic retinopathy, primary insomnia, generalized anxiety disorder, and schizophrenia (Cui et al., 2020; Huang et al., 2021; Li et al., 2020; Meng et al., 2020) (Fig. 1).
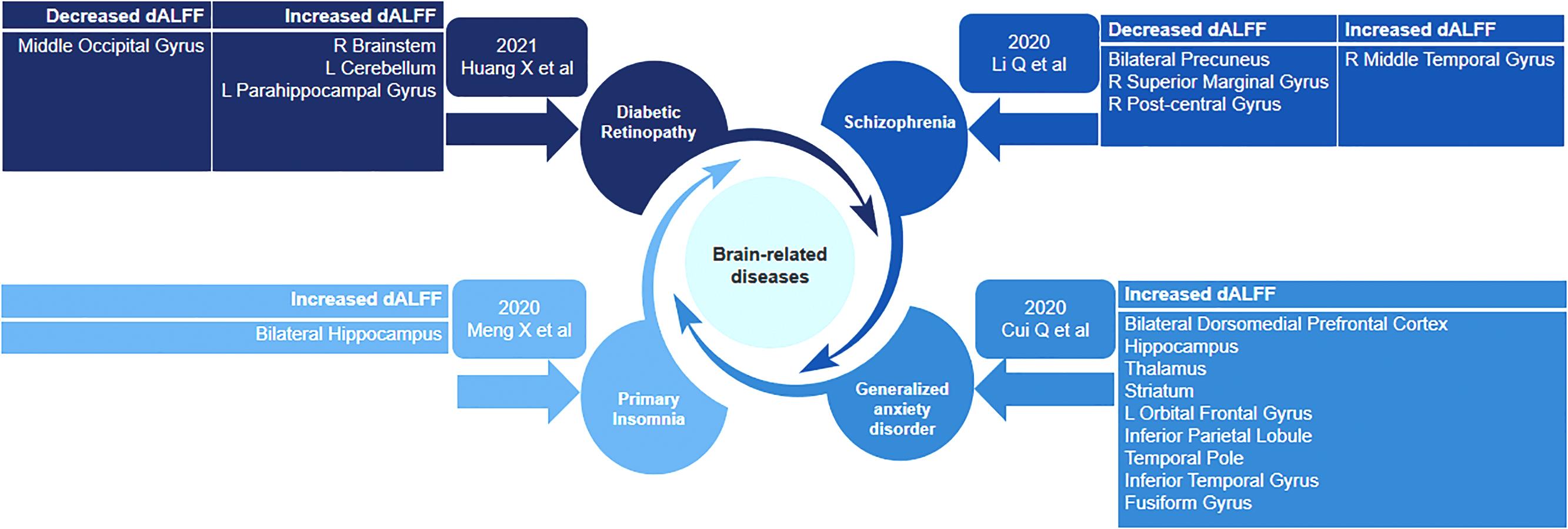
The articles using dALFF to study related encephalopathy in recent years. dALFF, dynamic amplitude of low-frequency fluctuation.
Previous studies have indicated that there are indeed differences in dALFF expression levels among different brain regions of patients and healthy controls (HCs) (Yang et al., 2022). Therefore, dALFF is very important to more effectively study the physiological mechanisms of the brain and emotion (Cakir, 2020). Although MMD is a cerebrovascular disease, there has been little research on the brain activity of patients with the disease (Li et al., 2021). At the same time, there is no precedent for using dALFF to study MMD.
Therefore, we use dALFF to investigate brain structure and spontaneous neural activity in MMD dynamics to further better the diagnosis and therapy of this disease. We not only use DSA to observe the vascular changes between MMD and HCs but also use optical coherence tomography (OCT) angiography to acquire blood flow motility information (Fig. 2) and to explore the relationship among dALFF, mood (anxiety and depression), and visual acuity, providing a new method for clinical diagnosis.
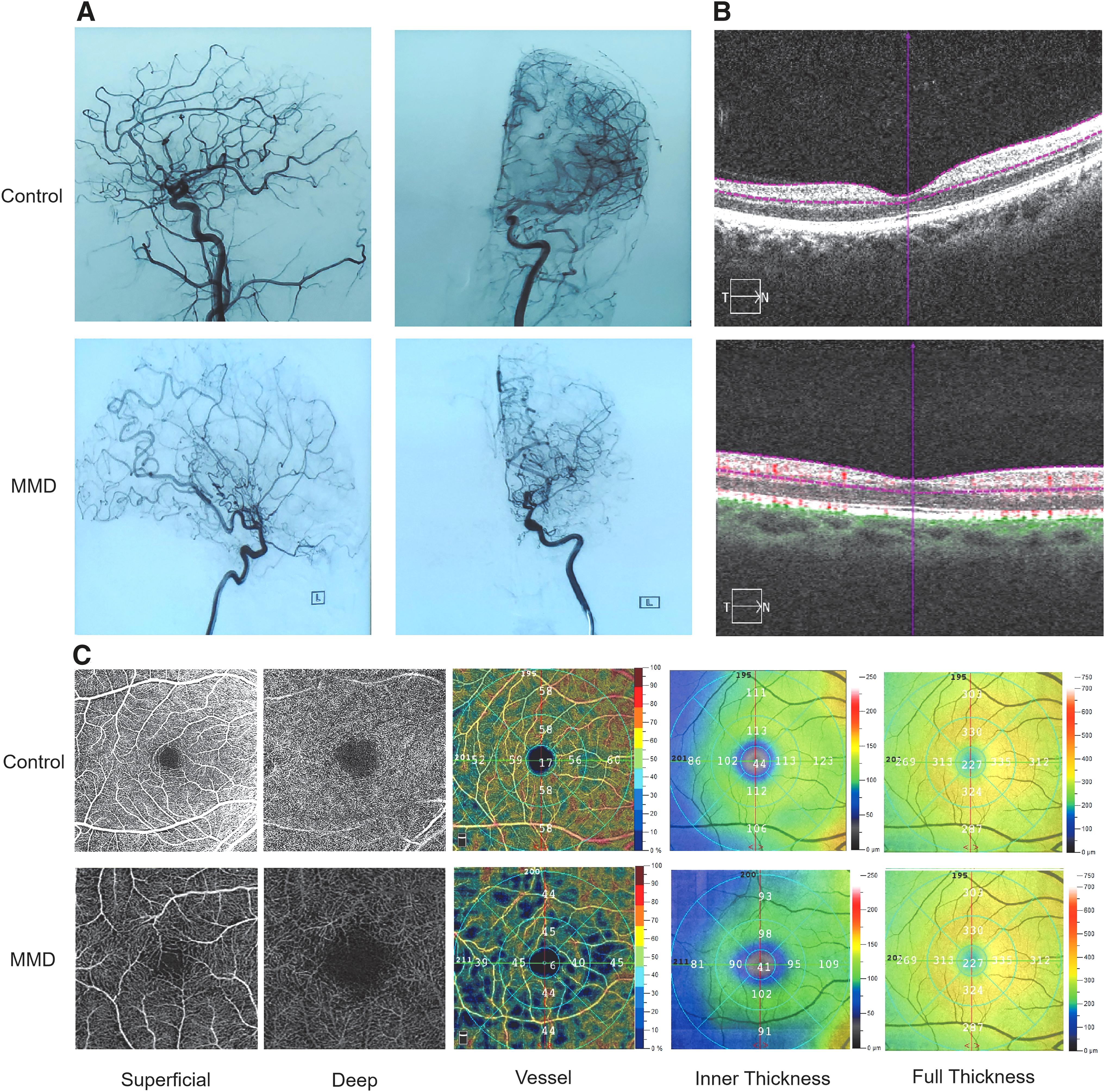
The differences of blood vessels and eyes between control and MMD groups.
Methods
Participants
Thirty-two age-, sex- (4 males and 28 females), and lifestyle-matched subjects were recruited from the First Affiliated Hospital of Nanchang University, including 16 patients with MMD (2 males and 14 females) and 16 healthy volunteers (2 males and 14 females). All subjects were informed of the purpose, methods, and potential risks of the tests and voluntarily signed a declaration of informed consent before participating. This study was approved by the Human Research Ethics Committee of the First Affiliated Hospital of Nanchang University.
All subjects underwent resting-state fMRI, OCT, and DSA and completed the Hospital Anxiety and Depression Scale (HADS). The dALFF value was used to measure levels of functional activity in brain regions.
Inclusion criteria in the MMD group were as follows: (1) typical bilateral MMD diagnosed by DSA; (2) 18 years < age <60 years; (3) no contraindications to MRI scanning; and (4) physically capable of completing HADS and OCT.
Exclusion criteria for this group were as follows: (1) history of craniocerebral surgery; (2) suffering from serious medical problems or audio–visual impairment; and (3) history of stroke.
All HCs met the following criteria: (1) without MMD; (2) no serious organic brain diseases such as cerebral infarction, hemorrhage, or cerebral embolism; (3) no smoking history; and (4) no contraindication to MRI.
MRI data collection
A Siemens Trio 3.0T MRI scanner (Siemens, Erlangen, Germany) was used to perform MRI scans with an 8-channel phased-array head coil. The subjects were placed in a supine position with sponge pads fixed on both sides of the head and earplugs worn during scanning to reduce noise. All participants were scanned using parameters described previously (Cai et al., 2015).
Resting-state fMRI data preprocessing procedure
The resting-state fMRI data were preprocessed using MRIcro software and DPARSFA software to remove incomplete data.
This preprocessing procedure was performed with the following steps: (1) 10 time points were excluded because of the unfamiliarity of participants with the environment and instability of the signal; (2) slice timing was done to correct time differences; (3) the Friston-24 model was used to correct head motion with realignment for personal-level correction; (4) mean framewise displacement minimized the potential influence of head motion; (5) several covariates were regressed; (6) fMRI was standardized to the Montreal Neurological Institute space by standard echo planar imaging (EPI) templates and EPI resampled all voxels to 3 × 3 × 3-mm3 resolution; (7) a low-frequency filtering range between 0.01 and 0.08 Hz was applied to dispel the impact of high-frequency noises; and (8) functional volumes were smoothed with a 6-mm full width at half maximum Gaussian kernel.
Calculation of dALFF values
A sliding window was applied to quantify dALFF values of each person using the DynamicBC toolbox (v2.0), which plays a crucial role in evaluating dynamic spontaneous neural activities in dynamic analysis (Liao et al., 2014). According to previous studies, we used the suitable window length range of 10–75 TR and step = 1 TR (Liu et al., 2017; Zalesky and Breakspear, 2015).
Therefore, an appropriate sliding window length was 30 TR (step = 1 TR) and 5 TR (10 s), which is used as the chosen step size to calculate dALFF of each person and maximize statistical power. dALFF maps for each participant were computed within each window, then a series of dALFF maps were generated. Afterward, we used standard deviation to measure the temporal variability of dALFF. dALFF variability was transformed into z-scores for statistical analysis.
HADS data acquisition
HADS, including the Anxiety-S Scale (Iwata and Mishima, 1999), and the Center for Epidemiological Research of Depression Scale (CES-D) (Lewinsohn et al., 1997) were used in this study. The anxiety and depression subscales each consist of seven questions in a 4-point sequential response format. Each subscale is scored on a scale from 0 to 21, with higher scores indicating higher levels of anxiety or depression. When answering each question, participants were required to consider how they felt and/or acted in the last week.
OCT data collection
The Spectralis OCT device (Heidelberg Engineering, Germany) and image-aligned eye-tracking software (TruTrack and Nsite Analytics; Heidelberg Engineering) were used. All scans were of image quality above 20 dB and parameters were as described previously (Albrecht et al., 2015) (Fig. 2).
Brain–behavior correlation analysis
GraphPad Prism 8 software (GraphPad, Inc., San Diego, CA) was applied to analyze Pearson's correlation and to evaluate the linear correlation among HADS scores, retinal nerve fiber layer thickness (RNFLT), and dALFF signal values. Significance was set at p < 0.05 with Bonferroni correction.
Statistical analysis
Participants' characteristics, including age, weight, height, and results from other visual test parameters, were compared with HCs using the Statistical Package for the Social Sciences, version 19.0 (SPSS, Inc., Chicago, IL). Independent sample t-test and chi-square tests were used to compare participants' characteristics, and a two-sample t-test compared differences in dALFF values between MMD patients and HCs; p < 0.05 indicated statistical significance.
Correlation between the dALFF in the brain areas and the clinical evaluation indicators of MMD patients was evaluated using Pearson's linear correlation analysis. The receiver operating characteristic (ROC) curve was used to detect whether MMD patients express decreased dALFF values in different brain regions, and the area under curve (AUC) of different brain regions can be used as the true positive rate for differential diagnosis of MMD and HCs.
Results
Demographics
No significant differences were found in age, weight, or height between MMD and HC groups. Significant differences between the two groups were found in anxiety (p = 0.036) and depression (p = 0.012) scores (Table 1).
Demographics and Behavioral Results of Moyamoya Disease Patients and Healthy Controls
Significant at * p < 0.05, using a chi-square test for sex data and an independent t-test for continuous data. Data are presented as mean ± SD.
AS, anxiety scores; DS, depression scores; HCs, healthy controls; IOP, intraocular pressure; MMD, moyamoya disease; N/A, not applicable; RNFLT, retinal nerve fiber layer thickness; VA, visual acuity.
Dynamic ALFF differences
MMD patients showed significantly reduced dALFF values in the left lingual gyrus, right insula, and right occipital lobe compared with HCs (Fig. 3A, B, and Table 2). Figure 3C shows the average change in dALFF values between MMD patients and HCs.
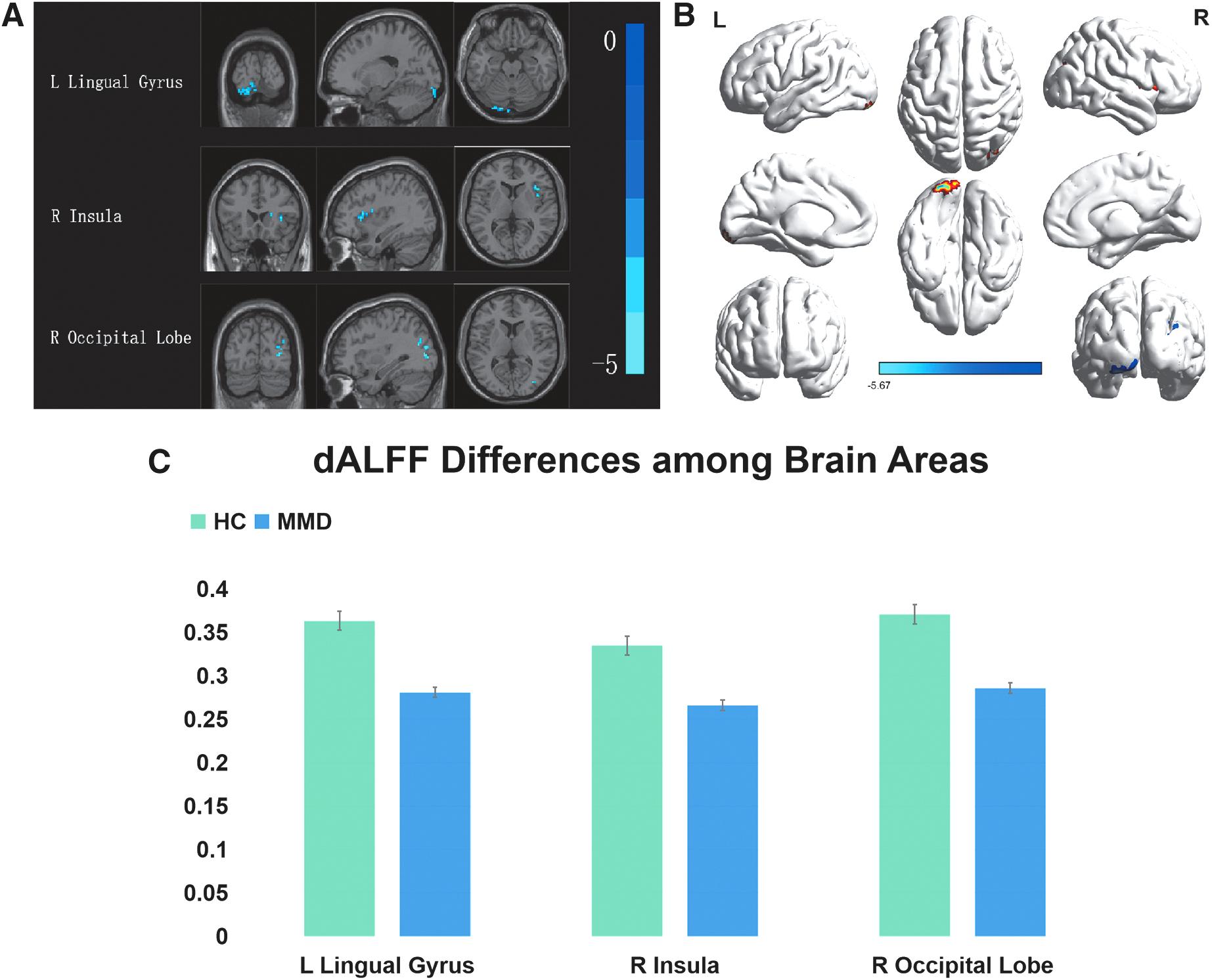
Voxel-wise comparison of dALFF in the MMDs and HCs.
Brain Regions with Significant Differences in Dynamic Amplitude of Low-Frequency Fluctuation Between Moyamoya Disease Patients and Healthy Controls
The statistical threshold was set at the voxel level with p < 0.005 for multiple comparisons using the Gaussian random field theory (p < 0.05, cluster-wise corrected).
dALFF, dynamic amplitude of low-frequency fluctuation; L, left; MNI, Montreal Neurological Institute; R, right.
Correlation analysis
In the MMD group, negative correlations were found between anxiety and depression scores and dALFF at the left lingual gyrus (anxiety: r = −0.631, p = 0.009; depression: r = −0.646, p = 0.007) and positive correlations were found between the RNFLT and right occipital lobe (right: r = 0.629, p = 0.009; left: r = 0.601, p = 0.014) (Fig. 4).
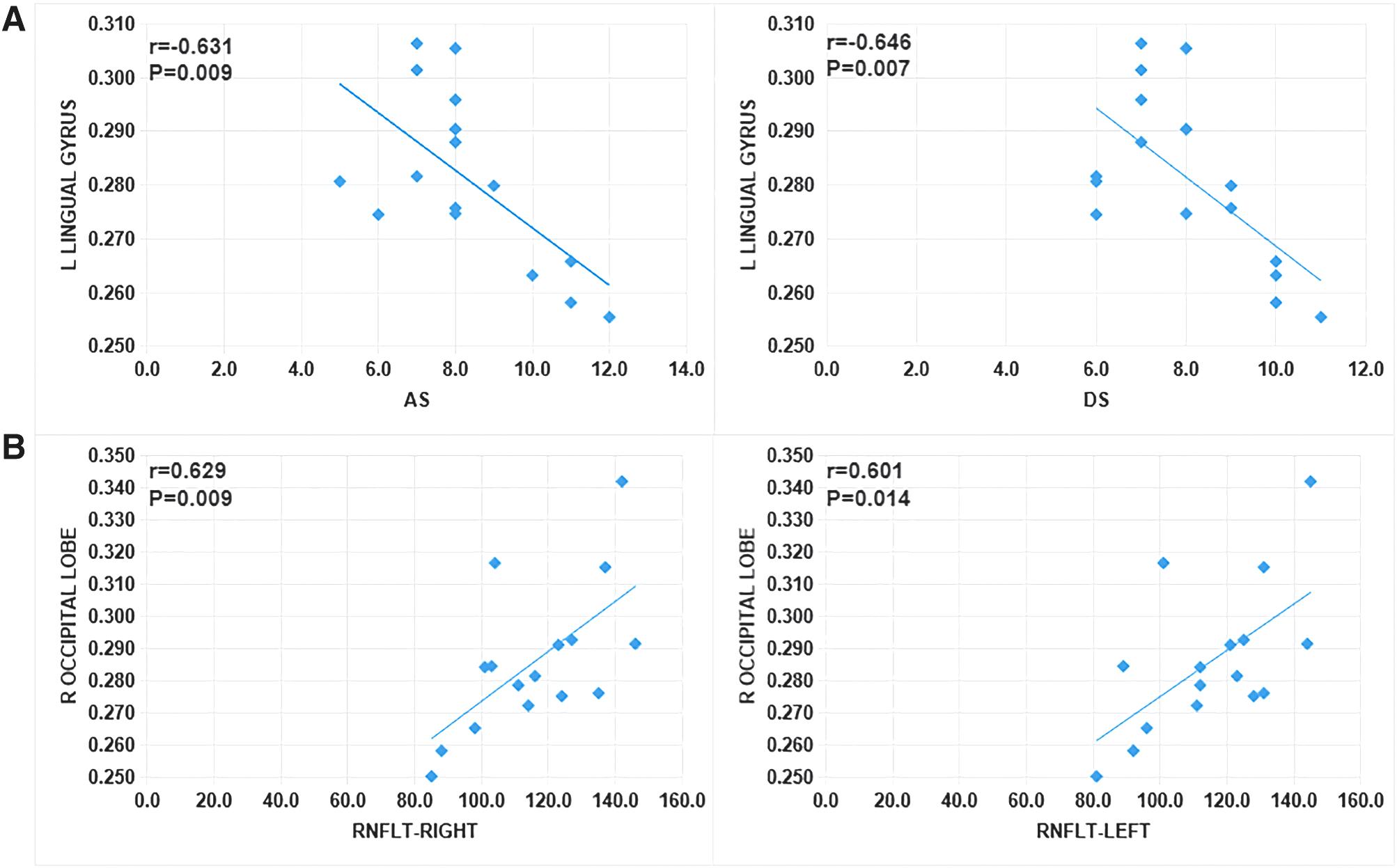
Correlations among dALFF, RNFLT, and AS/DS.
ROC curve
In this study, dALFF values at the left lingual gyrus, right insula, and right occipital lobe were significantly different between MMD and HC groups. The AUC was 0.990 (p = 0.01; confidence interval [95% CI]: 0.969–1.000) for the left lingual gyrus, 1.000 (p < 0.0001; 95% CI: 1.000–1.000) for the right insula, and 0.948 (p = 0.034; 95% CI: 0.881–1.000) for the right occipital lobe (Fig. 5).
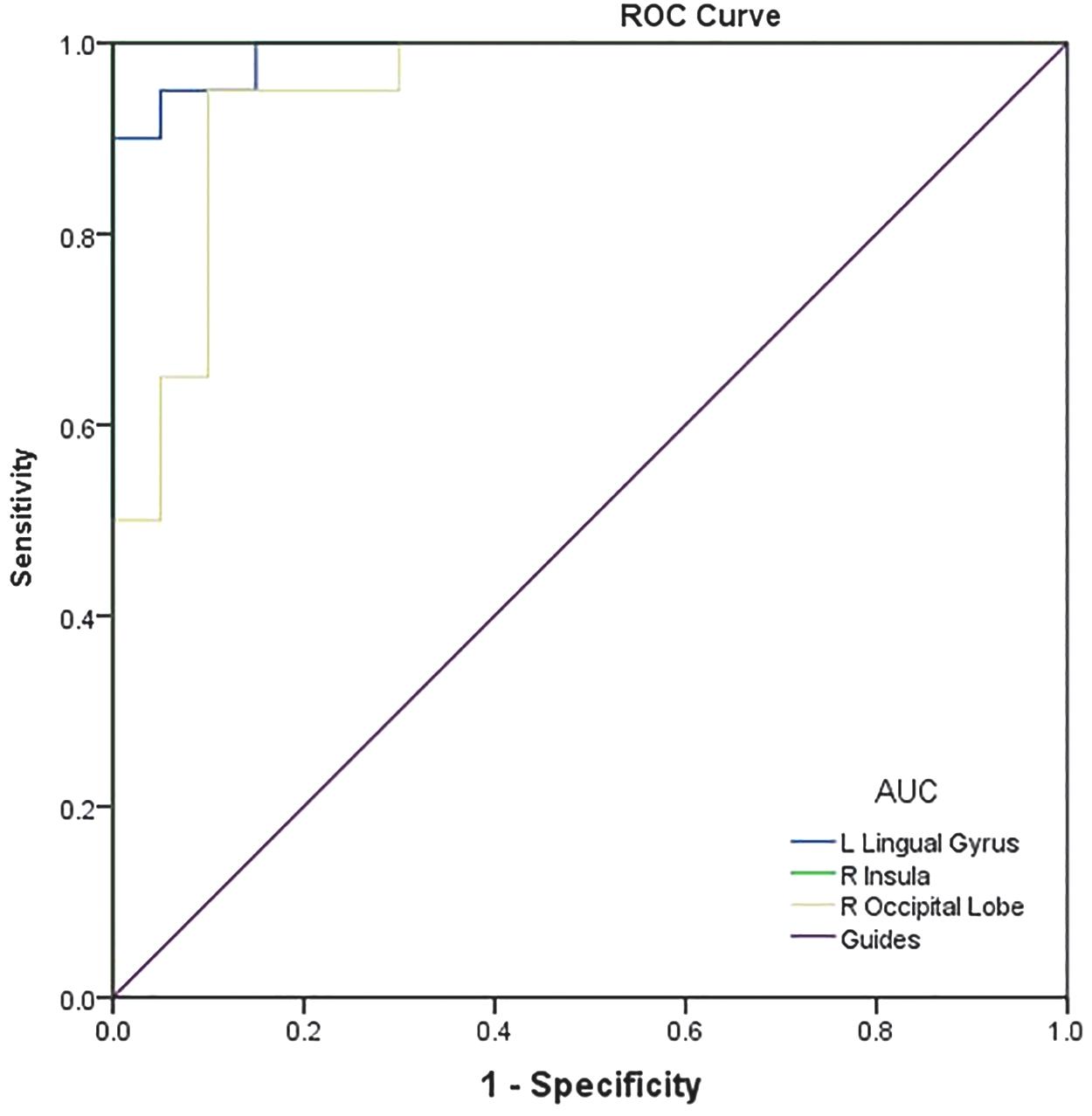
ROC curve analysis of the mean dALFF values for altered brain regions. AUC values were 0.990 (p = 0.01; 95% CI: 0.969–1.000) for the left lingual gyrus; 1.000 (p < 0.0001; 95% CI: 1.000–1.000) for the right insula; and 0.948 (p = 0.034; 95% CI: 0.881–1.000) for the right occipital lobe. AUC, area under the ROC curve; CI, confidence interval; ROC, receiver operating characteristic.
Discussion
To date, dALFF has not been applied in the detection and diagnosis of MMD, so in the present study, this approach was used for the first time to study brain activity in this disease.
The most prevalent clinical sign of MMD is ischemic or hemorrhagic stroke. Symptoms vary depending on patient's age (Sato et al., 2019). The vast majority of pediatric patients are hypotypic, presenting mostly with somatic dyskinesia. Intracranial hemorrhage affects over half of the adult patients, primarily causing disturbance of consciousness (Fukui, 1997).
In patients over the age of 40, blood outflow often exceeds blood deficiency and about 20% of patients with MMD develop headache due to decreased blood flow to the brain (Okada et al., 2012). In addition, various involuntary movements are common in MMD patients, which have a significant impact on their everyday life (Lee et al., 2014).
In this study, activity in three brain regions (right insula, right occipital lobe, and left lingual gyrus) was considerably reduced in patients with MMD (Fig. 6).
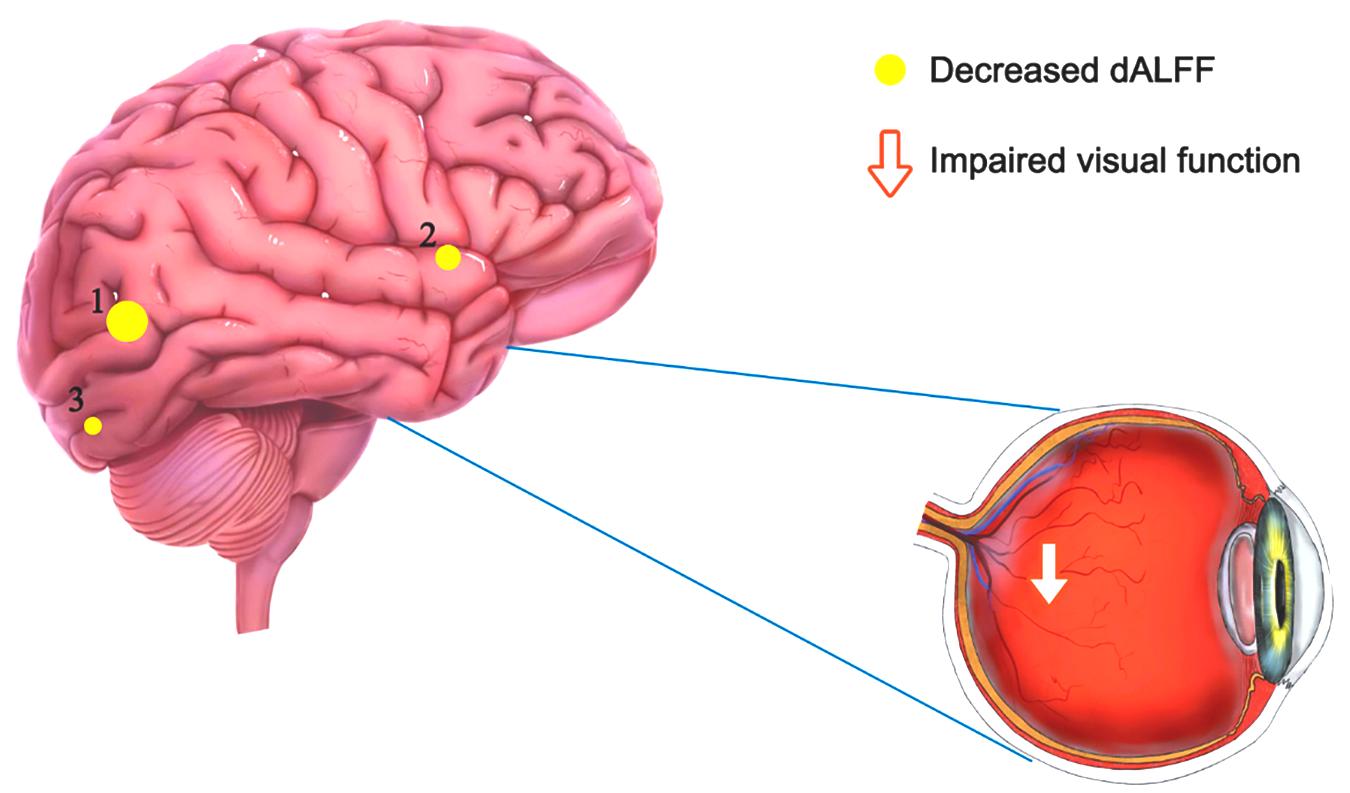
The mean dALFF values of altered brain regions. The sizes of yellow dots are a rough indication of how much the value has fallen. Compared with HCs, dALFF values of the following regions were decreased to various extents: 1–left lingual gyrus (t = −5.6699), 2–right insula (t = −5.4743), and 3–right occipital lobe (t = −5.0191).
The insula is positioned in the deep lateral sulcus, surrounded by Reil's sulci and bisected by the central suleus (Couvy-Duchesne et al., 2018). Due to technological constraints, researchers have been unable to explore insula functions in detail. A meta-analysis published in 2010 showed that the human insula has four regions with roles in sensorimotor, central olfactory and taste, social–emotional, and cognitive–dorsal functions (Kurth et al., 2010).
In addition, structural abnormalities of the insula, such as reduced volume and thickness and rotational changes, have been found in patients with schizophrenia, resulting in insular dysconnectivity (Sheffield et al., 2020; Tian et al., 2019). Our findings revealed that dALFF levels in the right insula of patients with MMD were significantly lower than those of HCs. This may indicate that the decrease in dALFF is due to abnormal neuronal activity in the brain.
The occipital lobe, including the lingual gyrus, is a prominent area of the central nervous system, which is prone to multiple lesions. The occipital lobe, located at the posterior end of the cerebral hemisphere and divided into dorsal, medial, and basal surfaces (Kandell and Jessell, 1995), contains the visual cortex and primary visual area, which are responsible for transmitting and processing information from the retina (Carlson, 2007) as well as participating in processing systems associated with language (Barr, 1988).
Seizures and visual impairment are the most prevalent postdamage dysfunctions. Occipital lobe epilepsy is a condition that affects the occipital lobe (Liu et al., 2019). Occipital lobe epilepsy is a comprehensive secondary convulsion induced by abnormal brain activity, with manifestations such as vomiting, visual hallucinations, neurological disorders, and other abnormal behaviors. Its clinical symptom mainly is acute and tonic deviation or clonus in both eyes (Liu et al., 2019). For patients with MMD, cerebrovascular abnormalities can result in transient cerebral ischemia or cerebral infarct, both of which cause visual impairment.
In this study, we discovered that the dALFF value of the right occipital lobe was positively correlated with RNFLT in both left and right eyes. The thinning of the retinal nerve fiber layer is most commonly associated with ocular diseases related to optic nerve atrophy. We hypothesized that lower levels of dALFF in the occipital lobe could reflect visual dysfunction in patients with MMD.
However, we did not explore whether the dALFF value could reflect the course and progression of MMD, so we cannot determine whether RNFLT is linked to disease progression, but according to previous reports, reduced RNFLT is associated with ocular disorders, including glaucoma (Mardin, 2019), retinitis pigmentosa (Oishi et al., 2009), and optic neuritis (Serbecic et al., 2012).
These findings and the correlation between dALFF values and RNFLT suggest that dALFF may be used as an effective indicator of ocular complications associated with MMD. At the same time, MMD patients have some degree of vascular abnormalities.
Therefore, we suspect that occipital lobe ischemia may directly or indirectly affect the oculomotor nerve and visual pathways, resulting in a variety of ocular manifestations such as transient black Mongolian spot, central artery obstruction, morning glory disc abnormality, ocular ischemic syndrome hemianopia, reduced vision, restricted eye movement, and eye pain (Scott and Smith, 2009, Bayan Al Othman, 2019), or affect nerves leading to neurological symptoms such as seizures. Moreover, ocular and neurological symptoms may also present at the same time.
As a medial part of the occipital lobe, the lingual gyrus is located below the sulcus. The lingual gyrus is connected to the occipital–temporal lobe of the brain and is responsible for integration of the language network information and word and letter processing. A previous study found that reduction in the lingual gyrus surface area was linked to depression in young people (Lim and Thomas, 2020).
In this study, our results showed that dALFF levels were significantly reduced in the left lingual gyrus in patients with MMD and were adversely correlated with anxiety and depression scores. The decreased dALFF value of the left lingual gyrus may reflect cognitive, language, memory, and other brain dysfunctions in patients with MMD.
All these physical symptoms may bring about emotional changes. Therefore, in addition to visual disorders, we considered mood disorders in MMD, which include irritability, anxiety, depression, and stress (Lai et al., 2018; Mavridis, 2014). We found that the dALFF level of the left lingual gyrus is negatively correlated with anxiety scores and depression scores, and in healthy groups, there are no particular relationships between HADS scores and dALFF, which may indicate that MMD patients have some degree of anxiety and depression symptoms (Fig. 7).
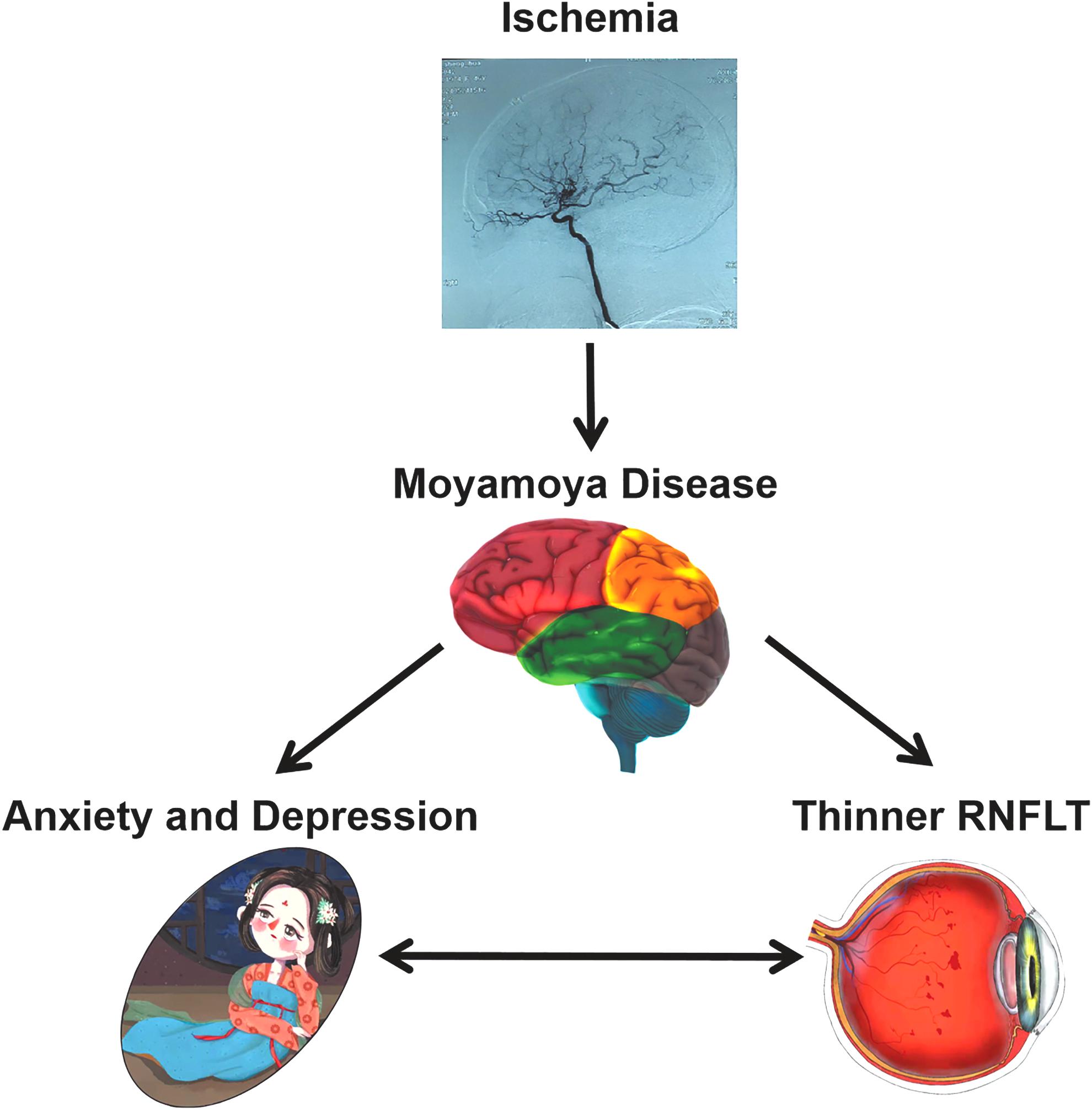
Relationship between MMD and related symptoms. Cerebral ischemia caused by MMD can affect the associated brain regions, thereby affecting visual function and mood.
ROC curve analysis of dALFF at the left lingual gyrus, right insula, and right occipital lobe in this study yielded AUCs at levels of high diagnostic significance, indicating that the dALFF value may be used as an important biological indicator to distinguish between MMD and a healthy state. In addition, this article has summarized the influence of functional activity abnormalities and related dysfunction in the aforementioned brain areas (Table 3).
Brain Region Alternation and Its Potential Impact
Conclusions
This study has two main shortcomings: first, the sample size is small. In the in-depth follow-up study, we will expand the sample size to eliminate the influence of regional and other environmental factors on the experimental results and to obtain more accurate data. Second, the inclusion criteria for participants in this experiment were not very detailed, therefore we were unable to differentiate between cerebral artery stenosis and other forms of occlusion. In the future, we will refine the inclusion criteria by drawing on the diagnostic criteria in the guidelines of each country or hospital.
In summary, we found abnormal brain activities and corresponding functional network disorders in multiple regions in MMD patients, indicating that brain regions involved in emotional, visual, and other processing were impaired in MMD patients. In addition, we discussed the functions of relevant brain regions and their possible involvement in the pathogenesis of this disease.
We hope that this study will provide new ideas for the clinical diagnosis and treatment of MMD, suggesting that clinicians should pay more attention to the changes of ocular illness and psychological symptoms in patients with MMD.
Footnotes
Authors' Contributions
Q.W. and X.-Y.W. analyzed the data and drafted the manuscript; L.-J.Z., C.-Y.Y., and S.-H.X. assisted with data interpretation and figure composing; H.-Y.S., X.-L.L., and M.K. collected the data; and T.S. and Y.S. conceived, designed, and directed the study and revised and approved the final manuscript.
Author Disclosure Statement
This was not an industry-supported study. The authors report no conflicts of interest in this work.
Funding Information
This research is supported by the National Natural Science Foundation of China (No. 82160195); Science and Technology Project of Jiangxi Provincial Department of Education (No. GJJ200169); Science and Technology Project of Jiangxi Province Health Commission of Traditional Chinese Medicine (No. 2020A0087); Science and Technology Project of Jiangxi Health Commission (No. 202130210).