
Abstract
Introduction:
Persisting imbalance and falls in community-dwelling traumatic brain injury (TBI) survivors are linked to reduced long-term survival. However, a detailed understanding of the impact of TBI upon the brain mechanisms mediating imbalance is lacking. To understand the state of the art concerning the brain mechanisms mediating imbalance in TBI, we performed a systematic review of the literature.
Methods:
PubMed, Web of Science, and Scopus were searched and peer-reviewed research articles in humans, with any severity of TBI (mild, moderate, severe, or concussion), which linked a postural balance assessment (objective or subjective) with brain imaging (through computed tomography, T1-weighted imaging, functional magnetic resonance imaging [fMRI], resting-state fMRI, diffusion tensor imaging, magnetic resonance spectroscopy, single-photon emission computed tomography, electroencephalography, magnetoencephalography, near-infrared spectroscopy, and evoked potentials) were included. Out of 1940 articles, 60 were retrieved and screened, and 25 articles fulfilling inclusion criteria were included.
Results:
The most consistent finding was the link between imbalance and the cerebellum; however, the regions within the cerebellum were inconsistent.
Discussion:
The lack of consistent findings could reflect that imbalance in TBI is due to a widespread brain network dysfunction, as opposed to focal cortical damage. The inconsistency in the reported findings may also be attributed to heterogeneity of methodology, including data analytical techniques, small sample sizes, and choice of control groups. Future studies should include a detailed clinical phenotyping of vestibular function in TBI patients to account for the confounding effect of peripheral vestibular disorders on imbalance and brain imaging.
Impact statement
Postural imbalance after moderate-to-severe traumatic brain injury (TBI) is virtually ubiquitous. However, a detailed understanding of the brain mechanisms mediating imbalance in TBI is lacking. Thus, we synthesized the literature linking brain imaging with postural balance in TBI. We found that cerebellum was commonly linked with postural imbalance in TBI. However, these findings are limited due to inappropriate selection of participants, lack of peripheral vestibular assessments, inappropriate control groups, and selection bias due to regions of interest analysis in brain imaging. Based on our findings we provide recommendations for future studies investigating brain mechanisms of imbalance in TBI.
Introduction
Traumatic brain injury (TBI) is the commonest cause of chronic disability in young adults (Langlois et al., 2006). TBI can result in vestibular dysfunction with dizziness and/or postural imbalance in up to 86% of patients acutely (Marcus et al., 2019). Unintentional trauma, including falls from imbalance, has also been identified as one of two factors (the other being neurodegeneration) linked to worse long-term survival in community-dwelling TBI survivors (Elser et al., 2023).
However, TBI patients are often unaware of their poor balance, for example, 50% of patients with clinically apparent gait ataxia did not report feeling unbalanced (Marcus et al., 2019; Sargeant et al., 2018; Wood et al., 2022). This can also be observed during clinical evaluation as a “vestibular agnosia,” where patients with manifest peripheral vestibular activation report little or no vertigo, and hence, vestibular dysfunction and linked imbalance in TBI could go unnoticed (Calzolari et al., 2021; Rust et al., 2022).
The mechanisms underlying balance deficits in TBI are poorly understood due to its relative neglect as a research topic. The vestibular control of balance has multiple levels of vulnerability, from the vestibular organ, the nerve, brainstem and cerebellar circuits, thalamic relay areas, and cortical processing pathways.
That the corpus callosum is particularly susceptible to damage in TBI because of the biomechanics of shear injury (Ghajari et al., 2017; Jolly et al., 2021), combined with our recent demonstration that imbalance in acute TBI was linked to damage to the genu of the corpus callosum (Calzolari et al., 2021), explains why imbalance is so common in TBI. An additional vulnerability for balance function arises from the bi-hemispheric processing of vestibular signals, which is disrupted with callosal injury (Kirsch et al., 2016).
Subcortically, vestibular afferent pathways project to the thalamus and basal ganglia (Cai et al., 2018; Stiles and Smith, 2015). In the brainstem, the pedunculopontine nucleus (PPN) plays a key role in postural balance whose neurons show high levels of vestibular reactivity (Aravamuthan and Angelaki, 2012). Degeneration of the PPN is implicated in the imbalance related to neurodegenerative diseases (i.e., Parkinson's) (Bohnen et al., 2012; Müller et al., 2013). Indeed, deep brain stimulation of the PPN in Parkinson's disease patients with severe imbalance (Yousif et al., 2016) improved their balance.
A clinically well-characterized TBI cohort is of critical importance for studying brain mechanisms mediating postural imbalance post-TBI. This includes the exclusion and/or treating of peripheral vestibular disorders and common diagnoses such as vestibular migraine. Without a detailed acute clinical assessment of the TBI patients before neuroimaging, any measured imbalance will likely be confounded by undiagnosed and untreated peripheral vestibular disorders.
The relative lack of understanding concerning the mechanisms explaining postural imbalance in TBI could thus be partially attributed to inconsistencies in (i) detailed clinical phenotyping and excluding (or treating) patients with additional peripheral vestibular dysfunction (and other common vestibular diagnoses such as vestibular migraine) and the secondary impact of adaptation (Conrad et al., 2022; Dieterich and Brandt, 2008; Dieterich et al., 2007; Helmchen et al., 2014) and maladaptation (Trinidade et al., 2023) upon brain correlates; (ii) variation in brain imaging modality (e.g., functional magnetic resonance imaging [fMRI], diffusion tensor imaging [DTI], and electroencephalography [EEG]); (iii) type of analysis (e.g., whole-brain and region of interest [ROI]) (Surgent et al., 2019); and (iv) type of balance assessment (e.g., objective posturography and subjective scales).
We thus performed this systematic review to (i) synthesize the evidence linking brain imaging with imbalance in TBI to provide an understanding of the underlying brain mechanisms that mediate postural imbalance in TBI; and (ii) identify the limitations of the current literature to provide direction for future studies.
Methods
We followed PRISMA guidelines (Page et al., 2021) while performing this systematic review. The complete PRISMA checklist is provided as Supplementary Data.
Eligibility
Inclusion criteria for studies was as follows: (i) articles: peer-reviewed research articles; (ii) participants: humans with traumatic brain injury of any severity (concussion, mild, mild-moderate, moderate, moderate-severe, or severe) and any age group; (iii) balance assessment: performed balance assessment (subjective scales or objective measurement [e.g., center of pressure-based measures]); (iv) brain imaging: performed either magnetic resonance imaging (T1-weighted imaging, fMRI, resting-state fMRI, and DTI), computed tomography (CT), single-photon emission computed tomography (SPECT), positron emission tomography (PET), magnetic resonance spectroscopy (MRS), EEG, magnetoencephalography (MEG), near-infrared spectroscopy (NIRS), or functional NIRS (fNIRS); (v) performed analysis linking balance measures (objective or subjective) with brain imaging; (vi) articles in English language; (vii) studies with any design are included (acute or chronic and prospective, cross-sectional, or interventional). Exclusion criteria was failing inclusion criteria, case reports, conference proceedings, research reports, and letter to the editors.
When studies used subjective symptom scales that included questions about vestibular dysfunction (including imbalance), then the study was only included if it performed an analysis linking vestibular subdomain scores of the subjective scale with brain imaging.
Literature search
A literature search was conducted by first author using PubMed, Scopus, Web of Science core collection, and Web of Science—All databases (MEDLINE, Web of Science core collection, BIOSIS Citation Index, CABI: CAB Abstracts, SciELO Citation Index) from the inception of these databases until March 14, 2023. The detailed search terms for each database are provided in the Appendix A1 section.
Data extraction
For the studies retrieved for detailed screening, notes were tabulated indicating inclusion or exclusion and the reason for decision by Z.H., which were independently reviewed by M.M. A detailed summary of the included studies was then prepared, after which the study details were tabulated. The first author (with suggestions from M.M. and B.M.S.) then extracted following information from studies that were included in the systematic review: (i) study and participant characteristics; (ii) scanning parameters; (iii) methodological characteristics; and (iv) findings reported in studies.
In terms of study and participant characteristics, we extracted information regarding first author, year of publication, study design, age, sample size, and gender for both patient and control groups. In addition, for patients we extracted time from injury to behavioral testing, time from injury to scan, the information regarding the mode of injury (fall, traffic accident, etc.), details of injury severity, and the information regarding clinical vestibular assessment and clinical scales.
For T1-weighted, DTI, fMRI, and resting-state imaging studies, we also extracted information about scanning parameters, including scanner vendor, magnetic field strength, number of head coil channels, type of scan (DTI, resting state, etc.), repetition time, echo time, data matrix, field of view, voxel size, and number of slices. For DTI, we further extracted information regarding diffusion directions, b-value, and number of b0 images.
Moreover, number of volumes was also extracted for resting-state scans. We also extracted information regarding type of imaging analysis (ROIs, whole brain, etc.), balance assessments, and lastly, we extracted information about the findings showing link between brain imaging and balance assessments within TBI or comparison of TBI with controls. If multiple measures were used and reported, we extracted information for all measures and all reported findings.
For EEG/fNIRS/MEG studies, we extracted information about recording setup (electrode cap, amplifier, sampling frequency, choice of ground- and reference-electrodes, electrode locations, and the analysis software). Moreover, we also extracted information about the balance measure and the EEG/fNIRS/MEG measure used for analysis, and the electrodes that were included in the analysis.
Quality assessment
We used the risk of bias assessment tool for nonrandomized studies (RoBANS) (Kim et al., 2013). The studies were rated for selection bias due to inadequate selection of study participants, controlling for confounding variables, measurement of exposure, blinding of outcome assessments, incomplete outcome data (attrition bias), and reporting bias (selective reporting of outcomes). Two authors (Z.H. and M.M.) rated the studies for risk of bias and in case of disagreement, ratings were discussed and agreed upon with the senior author (B.M.S.).
Results
Study selection
Figure 1 shows the PRISMA flowchart (Haddaway et al., 2022) for the selection procedure. Our search resulted in a total of 1940 articles (415 articles from PubMed, 548 from Scopus, 429 from web of science core collection, and 548 from web of science all databases). Sixty full-length articles were retrieved and assessed for eligibility. After excluding 35 articles that failed inclusion criteria, a total of 25 articles were included in this systematic review.

PRISMA flowchart of the selection procedure.
Study and participant characteristics
The study and participant characteristics of the included T1-weighted, DTI, fMRI, and resting-state imaging studies (n = 18) are detailed in Table 1 and the clinical characteristics of injury are stated in Table 2. Importantly, due to limited EEG/fNIRS studies, and focus solely on “concussed” individuals, we decided not to compare or critically appraise EEG/fNIRS data with other imaging modalities. However, the characteristics of n = 8 EEG/fNIRS studies and their findings are summarized in Tables 6 and 7, respectively. Important characteristics of the participants from the T1-weighted, DTI, fMRI, and resting-state imaging studies (n = 18) are listed as follows.
Study and Participant Characteristics (T1-Weighted, Diffusion Tensor Imaging, and Resting-State Imaging)
At least 1 year since injury.
Gender not stated.
—, not applicable; F, female; M, months; NA, not available; SD, standard deviation; SE, standard error.
Participant Injury and Clinical Characteristics (T1-Weighted, Diffusion Tensor Imaging, and Resting-State Imaging)
ABC, Activity-Specific Balance Confidence Scale; ACE-R, Addenbrooke's Cognitive Examination Revised; ANAM, Automated Neuropsychological Assessment Metrics; AOC, alteration of consciousness; AUDIT, Alcohol Use Disorders Identification Test; BAI, Beck Anxiety Inventory; BBS, Berg Balance Scale; BDI, Beck Depression Inventory; BESS, balance error scoring system; BOT-2, Bruininks-Oseretsky Test of Motor Proficiency–Second Edition; BSI-18, Brief Symptom Inventory; CDC, Centers for Disease Control and Prevention; CNT, Computerized NeuroCognitive Function Test; CT, computed tomography; CVLT-II, California Verbal Learning Test–Second Edition; DAST-10, Drug Abuse Screening Test; DGI, Dynamic Gait Index; DHI, Dizziness Handicap Inventory; GCS, Glasgow coma scale; GOAT, Galveston Orientation and Amnesia Test; GOSE, Extended Glasgow Outcome Scale; HISC, Head Injury Symptoms Checklist; ImPACT, Immediate Postconcussion Assessment and Cognitive Testing battery; LOC, loss of consciousness; M-ABC, Movement Assessment Battery for Children; MRI, magnetic resonance imaging; mTBI, mild traumatic brain injury; NSI, Neurobehavioral Symptom Inventory; PCL-M, Post-Traumatic Stress Disorder Checklist Military; PTA, post-traumatic amnesia; RGA, retrograde amnesia; RPCSQ, Rivermead Post-Concussion Symptoms Questionnaire; SAC, standardized assessment of concussion; SCAT3, Sport Concussion Assessment Tool-Third Edition symptom checklist; SF-36, Short-Form Health Survey; TBI, traumatic brain injury; TOMM, Test of Memory Malingering; WTAR, Wechsler Test of Adult Reading.
This review is composed of the findings from n = 925 participants (n = 444 patients and n = 481 healthy controls) in n = 18 T1-weighted, DTI, fMRI, and resting-state imaging studies with median number of participants per study n = 41 (median n = 17.5 patients; median n = 20 healthy). It is important to highlight that there was only one acute-prospective study of moderate-severe TBI (Calzolari et al., 2021). Moreover, there were only two studies in the general population of age 18–65 years (Calzolari et al., 2021; Handiru et al., 2021). Most of the other studies (n = 8 of 18; 44.44%) were in young athletes or children/adolescents.
Since most of the studies performed comparisons with control group (between-group analysis), the sample sizes of studies were considered small to medium with only two studies having relatively larger sample of patients n = 95 (Adam et al., 2015) and n = 62 (Kaushal et al., 2019), where n = 51 were included in the imaging analysis in Kaushal et al. (2019). Most importantly, peripheral vestibular dysfunction (i.e., problem with vestibular organ or vestibular nerve) or other vestibular diagnoses, for example, vestibular migraine, were not ruled out in any of the studies nor was it mentioned as exclusion criteria, except in one study (Calzolari et al., 2021).
Three studies (of n = 18; 16.67%) had partially overlapping patient cohorts (Caeyenberghs et al., 2012; Caeyenberghs et al., 2011; Caeyenberghs et al., 2010). Similarly, five other studies (of n = 18; 27.78%) also had a partially overlapping patient cohorts (Caeyenberghs et al., 2015; Diez et al., 2017; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b; Liang et al., 2021). This is based on a detailed comparison of participant information, and injury details stated in these articles (i.e., demographics, Glasgow coma scale score, and injury specifics on MRI and CT). One study (Liang et al., 2021) did explicitly declare the use of previously published data (Drijkoningen et al., 2015a).
Quality assessment
Selection of participants
The methodological quality of the studies is visualized in Figure 2 using robvis tool (McGuinness and Higgins, 2021). Two studies (Handiru et al., 2021; Kim et al., 2019) included TBI patients with mild and moderate or higher severity in the same analysis; moreover, the cause of injury (fall, traffic accident, etc.) for patients was also not available in both studies. Kim et al. (2019) included seven moderate and eight mild TBI in the brain imaging analyses and also reported to not having obtained informed consent of the study participants due to the retrospective nature of their study.

Quality assessment of studies using ROBANS risk of bias assessment tool.
Handiru et al. (2021) originally had a sample of n = 17 (3 mild, 3 moderate, 3 moderate/severe [diagnosis not confirmed], and 8 severe TBI); however, only n = 12 were included in the imaging analysis. The proportions of mild, moderate, or severe TBI in this sample of n = 12 were not stated in the study. Given that moderate-severe TBI patients' structural imaging analysis is more likely to influence the findings as compared with mild TBI and for reasons listed earlier, we decided to rate (Handiru et al., 2021; Kim et al., 2019) as “high risk” for selection of participants.
Kaushal et al. (2019) did not specify the gender of study participants and was thus rated as “unclear risk” on selection of study participants. Although Delano-Wood et al. (2015) combined the analysis of moderate TBI patients (n = 5) and mild TBI (n = 33), they report that the inclusion or removal of the moderate severity TBI did not affect the results. Calzolari et al. (2021) had 4 participants with mild-probable TBI severity in a sample of n = 37; however, a subsample of n = 30 of 37 was included in imaging analysis such that only 2 mild/probable TBI were included in analysis, and thus we considered it to be a “low risk.”
Hou et al. (2022) used the U.S. Department of Defense (DoD) and Veteran Affairs (VA) criteria to classify patients as “mild to moderate” TBI. Notably, DOD/VA criteria differentiates between “mild” and “moderate” but does not specify a category label of “mild to moderate.” However, the proportions of mild or moderate TBI patients were not explicitly stated in the study (Hou et al., 2022).
Moreover, as the study (Hou et al., 2022) an interventional study, there was no control group to assess whether the pre–post intervention change of balance outcome in the patients was not due to test–retest variability. Thus, due to lack of information regarding injury classification and the lack of appropriate control group, we rated Hou et al. (2022) as “high risk” on selection of participants.
In the studies included in this review, mild/concussed TBI patients were classified based upon absence of CT abnormalities. As mild TBI (Bonow et al., 2017; Sharp and Ham, 2011) and concussed individuals could still have MRI abnormalities (Bigler et al., 2016; Bonow et al., 2017; Yuh et al., 2014), the studies with mild and concussed athletes were also rated as “unclear risk” if: (i) they did not explicitly state the exclusion of participants with a lesion or incidental MRI finding; or (ii) if the mild traumatic brain injury/concussion definition did not explicitly address the exclusion of imaging findings. Lancaster et al. (2018) used the U.S. DOD definition of “mild” TBI to define sports-related concussion. Notably, U.S. DOD definition requires normal brain imaging for participants to be considered mild TBI; however, the definition stated in Lancaster et al. (2018) does not include any mention of normal brain imaging as inclusion criteria. Similarly, Wang et al. (2019) stated no details in study regarding the definition of injury or concussion. Thus, both of these studies were rated as “unclear risk” on selection of participants.
Control for confounding variables
Regarding accounting for confounding variables, none of the studies performed lesion mapping as part of their analysis. Adam et al. (2015) stated that no MRI abnormalities were detected in participants, whereas Liang et al. (2021) explicitly addressed the issue of lesion mapping and given the heterogenous lesions among their participants, they chose not to perform lesion masking.
Similarly, Calzolari et al. (2021) chose not to perform lesion mapping since some of the severe TBI patients did not show lesions (as a result of diffuse axonal injury). Since lesion volume could instead be used as a confound regressor (given the heterogeneity of lesions in TBI), all studies that did not account for lesions or did not explicitly address the issue of lesion mapping were rated as “unclear risk” for confounding variables.
Scanning characteristics
The details of scanning parameters of T1-weighted, DTI, fMRI, and resting-state imaging studies are listed in Table 3. From the included studies, n = 11 (of 18; 61.11%) performed DTI, n = 5 (of 18; 27.78%) performed resting-state fMRI, n = 1 (of 18; 5.5%) performed only T1 scan for volumetric analysis, and n = 1 (of 18; 5.5%) performed arterial-spin labeling (ASL), which is a form of fMRI that measures relative cerebral blood flow (rCBF). One of the studies (Diez et al., 2017) performed both DTI and resting-state imaging.
Scanning Characteristics (T1-Weighted, Diffusion Tensor Imaging, and Resting-State Imaging)
Voxel size not provided.
ASL, arterial-spin labeling; DTI, diffusion tensor imaging; FOV, field of view; TE, echo time; TR, repetition time; VBM, voxel-based morphometry.
All studies used a 3 T scanner except one study (Adam et al., 2015) that used 1.5 T scanner. One study (Wang et al., 2019) used ASL, which is an fMRI technique, and also had two different study sites, using a slice thickness of 4 mm and 4.5 mm as a scanning parameter. Notably, Wang et al. (2019) and Kaushal et al. (2019) only reported slice thickness but did not report voxel sizes of the scans acquired. Two resting-state studies (Bittencourt et al., 2022; Hou et al., 2022) also had voxel size of 3.5 mm (isotropic) that were relatively larger than other studies.
Methodological characteristics
Balance assessments
The measure used for balance assessment, type of analyses used for analyzing T1-weighted, DTI, fMRI, and resting-state images, and the imaging metric used for correlating with balance measure are listed in Table 4. Eight (of n = 18; 44.44%) studies used subjective balance scales, of which four studies used balance error scoring system (BESS) (Adam et al., 2015; Kaushal et al., 2019; Lancaster et al., 2018; Wang et al., 2019), one study used Movement Assessment Battery for Children (Caeyenberghs et al., 2011), one study used Neurobehavioral Symptom Inventory (NSI)—vestibular subscale (Delano-Wood et al., 2015), and one study used Head Injury Symptoms Checklist (HISC; vestibular subdomain) (Bittencourt et al., 2022). One study (Handiru et al., 2021) used both, a subjective (Berg balance scale [BBS]) and objective balance assessment (posturography).
Analysis Methods and Balance Assessment in Included Studies (T1-Weighted, Diffusion Tensor Imaging, and Resting-State Imaging)
AD, axial diffusivity; COP, center of pressure; FA, fractional anisotropy; FC, fiber cross-section; FCD, functional connectivity density; FD, fiber density; FDC, combined measure of FD and FC; GM, gray matter; LOS, limits of stability; MA, mode of anisotropy; MD, mean diffusivity; PPA, point process analysis; RD, radial diffusivity; ROI, region of interest; RWS, rhythmic weight shifting; SOT, sensory organization test; TBSS, tract-based spatial statistics; WM, white matter.
Ten studies (of n = 18; 55.56%) used objective balance assessments, of which five studies used sensory organization test (SOT) (Caeyenberghs et al., 2015; Caeyenberghs et al., 2012; Caeyenberghs et al., 2010; Hou et al., 2022; Liang et al., 2021), three studies used posturography (Calzolari et al., 2021; Handiru et al., 2021; Kim et al., 2019), and three studies used SOT, limits of stability (LOS) test, and rhythmic weight shift (RWS) test, together (Diez et al., 2017; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b).
Types of brain imaging analyses
Analyses using selected ROIs
Six studies (of n = 18; 33.33%) used selected ROIs for the analysis (Caeyenberghs et al., 2011; Caeyenberghs et al., 2010; Delano-Wood et al., 2015; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b; Hou et al., 2022). Out of these, four studies performed DTI (Caeyenberghs et al., 2011; Caeyenberghs et al., 2010; Delano-Wood et al., 2015; Drijkoningen et al., 2015a), one study performed volumetric analysis using T1 scans (Drijkoningen et al., 2015b), and one study performed resting-state analysis (Hou et al., 2022).
Caeyenberghs et al. (2010) used nine subcortical white-matter tracts/regions as ROIs including superior-middle-inferior cerebellar peduncles (SCP, MCP, and ICP), cerebellum, brainstem, pons, corticospinal tract (CST), medial lemniscus (ML), cerebral peduncles (CP), and three cortical white-matter tracts anterior–posterior limb of the internal capsule (ALIC and PLIC), and posterior thalamic radiation. Caeyenberghs et al. (2011) used seven subcortical ROIs, including CST, SCP, ICP, CP, thalamus, cerebellum, brain stem, and four cortical ROIs, including corpus callosum, anterior corona radiata, ALIC, and PLIC.
Drijkoningen et al. (2015a) mainly focused on subcortical ROIs, including SCP, MCP, ICP, and cerebellum. Similarly, Drijkoningen et al. (2015b) also only focused on subcortical ROIs, including cerebellum and brain stem. Delano-Wood et al. (2015) also used subcortical tracts as ROIs, including CST, pontine tegmentum, ML, and central tegmental tract. Hou et al. (2022) used 35 ROIs from sensory/somatomotor resting-state network atlas, 31 ROIs from visual network, and 4 ROIs from cerebellar network.
Whole-brain analyses
Twelve studies (of n = 18; 66.67%) performed whole-brain-level analysis of which eight studies (Adam et al., 2015; Caeyenberghs et al., 2012; Calzolari et al., 2021; Diez et al., 2017; Handiru et al., 2021; Kim et al., 2019; Lancaster et al., 2018; Liang et al., 2021) used DTI scans, four studies used resting-state scans (Bittencourt et al., 2022; Caeyenberghs et al., 2015; Diez et al., 2017; Kaushal et al., 2019), and one study used ASL scan (Wang et al., 2019). One of these studies used both DTI and resting-state analysis (Diez et al., 2017).
From 12 studies (of n = 18; 66.67%) that performed whole-brain-level analysis, 6 studies performed whole-brain analysis at ROI/network level (Adam et al., 2015; Bittencourt et al., 2022; Caeyenberghs et al., 2012; Diez et al., 2017; Kaushal et al., 2019; Wang et al., 2019) and 6 studies performed whole-brain voxel-level analysis (Caeyenberghs et al., 2015; Calzolari et al., 2021; Handiru et al., 2021; Kim et al., 2019; Lancaster et al., 2018; Liang et al., 2021).
Brain imaging measures linked to balance assessments
The findings of the studies linking brain imaging with balance assessments are listed in Table 5 and are detailed in text as follows.
Findings Reported in Studies (T1-Weighted, Diffusion Tensor Imaging, and Resting-State Imaging)
Fornix (column, body).
Fornix (cres)/stria terminalis.
ACR, anterior corona radiata; ALIC, anterior limb of internal capsule; BCC, body of corpus callosum; CP, cerebral peduncles; CST, corticospinal tract; EC, external capsule; GCC, genu of corpus callosum; ICP, inferior cerebellar peduncle; MCP, middle cerebellar peduncle; MNI, Montreal Neurological Institute; None, no statistically significant differences; MTG, middle temporal gyrus; PCR, posterior corona radiata; PLIC, posterior limb of internal capsule; PTR, posterior thalamic radiations; rCBF, relative cerebral blood flow; RLIC, retrolenticular internal capsule; SCC, splenium of corpus callosum; SCP, superior cerebellar peduncle; SFOF, superior fronto-occipital fasciculus; SLF, superior longitudinal fasciculus; SPG, superior parietal gyrus; SS, sagittal stratum; TAP, tapetum; UNC, uncinate fasciculus.
Findings in studies using selected ROIs
Findings from six studies that used selected ROIs in their analyses are displayed on a representative brain in Figure 3. Five studies (of six) using selected ROIs (Caeyenberghs et al., 2011; Caeyenberghs et al., 2010; Delano-Wood et al., 2015; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b) reported significant link of imaging measures with balance, whereas one study found no link (Hou et al., 2022).

Brain regions showing link between balance and brain imaging measures in regions of interest analysis. Note: representative figure only with no right/left localization as the MNI coordinates are not available from studies. ALIC, anterior limb of internal capsule; CST, corticospinal tract; ICP, inferior cerebellar peduncle; MCP, middle cerebellar peduncle; ML, medial lemniscus; SCP, superior cerebellar peduncle.
Caeyenberghs et al. (2010) reported lower fractional anisotropy (FA) values linked to poor balance of TBI patients in the following: (i) SCP, ALIC, cerebellum, and ML during the eyes open with fixed surface and surround condition; (ii) MCP during eyes open with fixed surface but sway referenced visual surround. Caeyenberghs et al. (2011) also found that lower FA values linked to poor balance but in the CST.
Drijkoningen et al. (2015a) studied the effect of balance training and found (i) at baseline, low FA in cerebellum and SCP, and high mean diffusivity (MD) values in MCP and SCP, were linked to poor balance of TBI patients in RWS test; (ii) within TBI patients, lower FA in ICP at baseline linked to improved balance scores post-training in the LOS test (uncorrected for multiple comparisons); (iii) within TBI patients, the increased performance in RWS test after training was linked to increase in FA values of ICP.
Drijkoningen et al. (2015b) only used cerebellum and brain stem as selected ROIs and found (i) within TBI, worse RWS test performance was linked to lower gray-matter volume in vermal and paravermal regions of cerebellum lobule I–IV, V, and VI; (ii) correlation between RWS performance of all participants (controls and TBI) showed that worse RWS performance linked to lower gray-matter volume in vermal and paravermal regions of cerebellum lobules I–IV, V, and VI and to lower white-matter volume in pons, dorsal medulla, midbrain (tegmentum), SCP, MCP/pons, MCP/cerebellar white matter; and (iii) correlation between SOT performance of all participants (controls and TBI) showed that worse SOT performance linked to lower white-matter volume in MCP/pons.
Delano-Wood et al. (2015) reported that lower FA in pontine tegmentum linked with poor vestibular subscale score within TBI patients; however, there were no group differences between TBI and controls in the diffusion parameters of the three selected ROIs.
Findings in studies using whole-brain analysis
Findings from 12 studies that performed whole-brain analysis are displayed on a representative brain in Figure 4. Five studies (of 12) that performed whole-brain analysis (at voxel or ROI level) reported no link of imaging measures with balance measures (Adam et al., 2015; Handiru et al., 2021; Kaushal et al., 2019; Lancaster et al., 2018; Liang et al., 2021). Bittencourt et al. (2022) reported link of vestibular subscores in HISC scale with brain regions, that is, left mid-temporal gyrus within cognitive/language resting-state functional network (nb: language network contains regions considered important for vestibular processing, i.e., superior, middle, and inferior temporal gyri), and cerebellum VI and crus I within visual and cerebellar resting-state functional network.
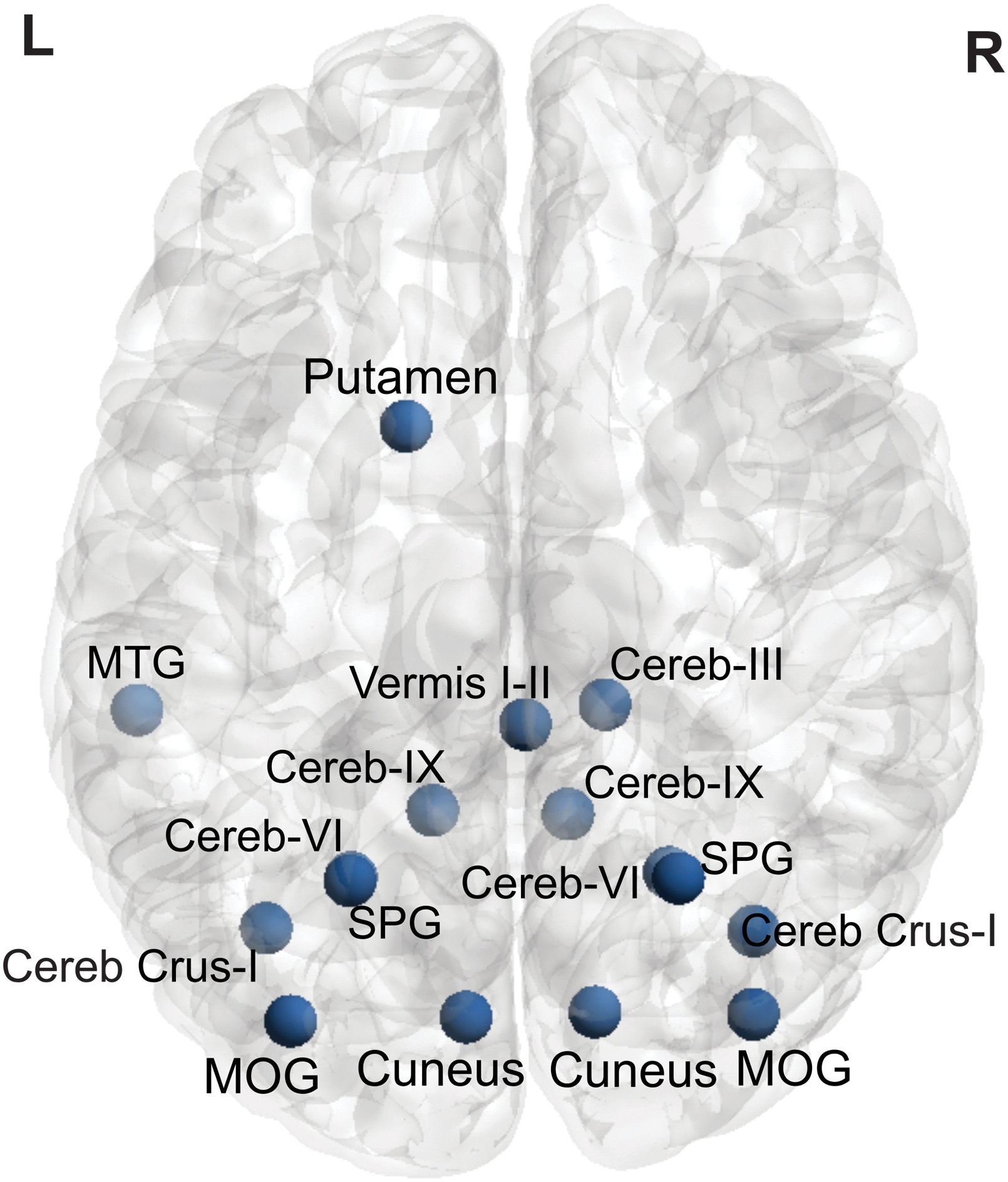
Brain regions showing link between balance and brain imaging measures in whole-brain analysis. Note: representative figure only for gray-matter regions, with no right/left localization as the MNI coordinates are not available from studies. Cereb, cerebellum; MOG, middle occipital gyrus; MTG, middle temporal gyrus; SPG, superior parietal gyrus.
Caeyenberghs et al. (2012) performed a graph theoretical analysis and reported that lower connectivity degree values linked with poor balance of TBI patients in SOT (composite score of all balance conditions) in the superior parietal gyrus, whereas in condition with compromised visual and proprioceptive feedback, low connectivity degree was linked to poor balance in superior parietal gyrus and cerebellar lobule IX.
Caeyenberghs et al. (2015) reported that (i) in condition with eyes open and compromised proprioception, poor balance scores were linked to lower long-range functional connectivity density (FCD) of left putamen within TBI patients, as well as in all participants (controls and TBI); (ii) in condition with both vision and proprioception compromised, poor balance scores were linked to lower long-range FCD of right cerebellar vermis I–II within TBI patients, right cerebellar vermis I–II, and right cerebellum III in all participants (controls and TBI).
Calzolari et al. (2021) compared acute TBI patients with impaired balance versus acute TBI patients with normal balance, whereby the normal range was based upon a healthy matched controls' posturography performance standing on a soft surface with eyes closed. Calzolari et al. (2021) reported that (i) FA was lower in genu of corpus callosum and left anterior corona radiata when comparing TBI with impaired balance to TBI with normal balance; (ii) MD was higher in the genu of the corpus callosum, left anterior corona radiata, and external capsule when comparing TBI with impaired balance to TBI with normal balance. The remaining findings from Calzolari et al. (2021) are detailed in Table 5 due to numerous other comparisons.
Diez et al. (2017) reported that increased dynamic BOLD activation of a prefrontal network was linked to poor balance. Kim et al. (2019) reported that poor balance score (during standing on soft surface with eyes closed) linked with lower axial diffusivity in left ICP. Wang et al. (2019) reported that poor scores in BESS linked with increased relative cerebral blood flow (rCBF) in left occipital gyrus in TBI.
Statistical considerations
All studies' statistical analyses were reviewed and only notable practices, such as the absence of multiple comparison correction or absence of direct comparison with appropriate control groups, are mentioned in this study.
Caeyenberghs et al. (2015) performed correlations between the balance measures and the brain regions that were significantly different between controls and TBI patients. Notably, these correlations were performed within groups, that is, a correlation of balance measure with functional imaging connectivity measure within the patient group, and within the control group. Similar correlation was also performed with all participants included in same analysis (patients and controls combined). However, a direct statistical comparison of correlations, indicating whether the correlation of balance measure with imaging connectivity measure was statistically different between control and patient groups, was not listed.
From Calzolari et al. (2021), we included results from 8 (of 19) statistical comparisons reported in the study, which were relevant to this systematic review, that is, comparisons linking brain imaging measures and balance measures. Four of these comparisons were performed using FA and four using MD diffusion imaging measures. The eight comparisons included two correlation contrasts within all TBI patients, two correlation contrasts including all participants (patients and controls together), two comparisons of “TBI patients with impaired balance” with healthy controls, and two comparisons within TBI patients (“TBI with impaired balance” vs. “TBI with normal balance”). However, the study does not indicate that if the comparisons were corrected for the number of total comparisons performed.
Delano-wood et al. (2015) found no significant difference between TBI and controls in the functional connectivity of selected ROIs. Despite the lack of a group difference, a within patient correlation of the NSI (vestibular subscale) with FA values was performed in the study. A direct statistical comparison, indicating whether the correlation of imaging connectivity measure and balance measure in patients was statistically different from that of healthy controls, was not available.
Diez et al. (2017) performed correlation of three balance measures with connectivity of a functional network. However, the study did not explicitly state that the p values were corrected for three comparisons.
Two of the five significant findings reported in Drijkoningen et al. (2015a) (and included in this systematic review) were labeled as exploratory analysis without correction for multiple comparisons. Notably, correlations of DTI measures and balance measures were performed separately in TBI, and the control groups, and the direct statistical comparison indicating a statistical difference in correlations of the two groups was not available.
Drijkoningen et al. (2015b) linked the three balance measures (SOT, LOS, and RWS) with subcortical ROIs in all participants' gray- and white-matter as well as within TBI group only. The findings were not significant for the correlations within controls and were not reported. The study does not indicate if the p values used in the study for indicating statistical significance were corrected for the total number of comparisons.
Kim et al. (2019) performed a comparison of diffusion imaging scans between patient and a control group, resulting in six significant findings (of which four were unique brain regions); and then the diffusion parameters from these significant brain regions were correlated with balance scores. However, only one correlation of a DTI measure with the balance measure is reported (within TBI group) without explicit mention of correction for multiple comparisons.
Wang et al. (2019) also performed within group (patients only) correlational analysis and used a cluster height threshold of p < 0.05; but also reported that the findings did not survive correction at cluster height threshold of p < 0.01.
EEG and fNIRS studies
Notably, there were five EEG and three fNIRS studies that we found as part of the systematic review (Handiru et al., 2021; Helmich et al., 2020; Helmich et al., 2016; Jacob et al., 2022; Slobounov et al., 2012; Teel et al., 2014; Thompson et al., 2005; Urban et al., 2021). The comparisons within these studies were often between TBI patients versus healthy controls (Handiru et al., 2021; Helmich et al., 2016; Teel et al., 2014; Thompson et al., 2005; Urban et al., 2021) or in patients with and without concussion (Helmich et al., 2020; Helmich et al., 2016).
EEG studies reported link of imbalance with decrease of beta, delta, and theta (Teel et al., 2014) as well as decrease of alpha (Slobounov et al., 2012). Similar decrease in delta was also reported in one other study in concussed individuals (Thompson et al., 2005). One study reported a negative correlation between theta band modularity (a graph-theoretical measure) and BBS (Handiru et al., 2021), whereas one study found no EEG changes linked to imbalance (Jacob et al., 2022).
The findings of the three fNIRS (Helmich et al., 2020; Helmich et al., 2016; Urban et al., 2021) studies were predominantly in the frontal regions, mainly because the electrodes were only placed on frontal ROIs. Thus, due to limited studies, all of which focused on concussed athletes (except one), we avoided discussing these studies in context of the imaging findings in mild-moderate-severe TBI. The study characteristics and the findings from these studies are listed in Tables 6 and 7.
Study and Participant characteristics (Electroencephalography and Functional Near-Infrared Spectroscopy Studies)
Methodology and Findings (Electroencephalography and Functional Near-Infrared Spectroscopy Studies)
↓: decreased; ↑: increased.
DLPFC, dorsolateral prefrontal cortex; EC, eyes closed; EEG, electroencephalography; EO, eyes open; EoB, effort of balance; fNIRS, functional near-infrared spectroscopy; IPC, inferior parietal cortex; PCS, post-concussive symptoms; PL, path length; SMG, supramarginal gyrus; SPC, superior parietal cortex; SuP, surface of pressure.
Excluded studies
There were 26 full-length articles (out of 35 excluded articles) relevant to the topic that were retrieved but excluded after detailed screening as they did not fulfil inclusion criteria. They are briefly mentioned in this study as per the PRISMA protocol. Some studies performed a balance assessment and brain imaging but were excluded as they did not state whether an analysis linking brain imaging and balance measure is performed (Churchill et al., 2021; Churchill et al., 2017; Hammeke et al., 2013; Jang et al., 2016a; Jang et al., 2016b; Meier et al., 2020; Muftuler et al., 2020; Vartanian et al., 2021).
Some of the studies either did not report data from postural balance assessment (Charney et al., 2020; Madaan et al., 2021; Madhavan et al., 2019; Sours et al., 2015; Toth et al., 2021; Weng et al., 2017) or from brain imaging (Shetty et al., 2018). One study focused on acquired brain injury and thus also had stroke patients (n = 22) combined with TBI (n = 9) (Joubran et al., 2022), whereas one study looked at working memory of TBI with impaired balance (Woytowicz et al., 2018).
One study mainly looked at the link between poor sleep and number and volume of perivascular spaces (PVS) but also reported link of PVS with balance (using a symptom scale); however, the study did not report or link it with gray- or white-matter regions or networks in the brain (Piantino et al., 2021). There were eight EEG-based studies that did not fulfil inclusion criteria (Allexandre et al., 2019; Devilbiss et al., 2019; Handiru et al., 2022; Howell et al., 2018; Seo et al., 2011; Slobounov et al., 2005; van der Veen et al., 2023; Walter et al., 2017).
There was no PET or SPECT study that passed the screening stage. One study, Charney et al. (2020), performed MRS; however, it was excluded as it did not report a postural balance assessment.
Discussion
This systematic review focused on identifying brain regions that are linked to postural imbalance in TBI patients, with the aim to understand underlying brain mechanisms that could explain imbalance in TBI. However, the findings from this systematic review are quite heterogeneous with low consistency in findings reported by the studies included in review. Hereunder we first critically appraise the important methodological characteristics of studies and highlight the need for clinically well-characterized patient cohorts. We then discuss the findings reported by the studies in light of previous literature, the reproducible findings among these studies, as well as current limitations, and the recommendations for future studies.
Cohort: timing of recruitment, clinical assessment, and treatment
TBI is the commonest cause of injury-related death and disability, where c. 60 million people have a TBI every year (Maas et al., 2022; Maas et al., 2017) with further increased falls risk post-TBI (Elser et al., 2023). Despite the post-TBI falls related risks, we only found one acute-prospective study in moderate-severe TBI that assessed post-TBI vestibular-mediated balance problems and its brain mechanisms through neuroimaging (Calzolari et al., 2021). Given that TBI is common in relatively young adults (Calzolari et al., 2021; Marcus et al., 2019; Rust et al., 2022) and results in socioeconomic costs of up to U.S. $400 billion (Maas et al., 2022), it is also surprising to notice the lack of studies that assessed vestibular-mediated balance problems and their brain mechanisms in the general population ranging between 18 and 65 years.
Notably, none of the studies included in this systematic review, except Calzolari et al. (2021), performed or reported upon acutely performed clinical vestibular assessment of peripheral vestibular damage or diagnoses such as benign paroxysmal positional vertigo (BPPV). Recent work shows that there is a high burden of vestibular disorders in TBI, both from central injury and peripheral injury, including BPPV (Calzolari et al., 2021; Harrell et al., 2023; Marcus et al., 2019) and vestibular nerve transection (Arshad et al., 2017; Marcus et al., 2019) as well as associated diagnoses such as vestibular migraine (Marcus et al., 2019), whose commonest manifestation is objective imbalance (Von Brevern et al., 2005).
Even though the cross-sectional studies of moderate-severe TBI in this review had average time of circa 3 years from injury to testing, some patients were also tested as early as 4 months after the injury (Diez et al., 2017; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b). Notably, previously reported recurrence rate of BPPV was up to 67% in TBI (Calzolari et al., 2021; Gordon et al., 2004), which was supplemented by recent studies showing that recurrence can occur in a period ranging from up to 4 (Smith et al., 2020) to 6 months (Hadi et al., 2024, in preparation; recurrence rate of 31.6%) post-TBI.
It follows that any study aiming to understand the brain correlates of imbalance should assess all these clinical features both acutely and at follow-up to exclude or treat patients for these additional vestibular diagnoses, before balance and imaging assessment. In addition, some maladaptive syndromes that are linked to imbalance, for example, persistent postural perceptual dizziness (Seemungal and Passamonti, 2018), may also develop chronically and must be controlled for in chronic TBI studies.
Notably, characterization of injury severity is key for TBI studies. In this review, multiple studies were rated as high risk on selection of participants due to lack of details on how the injury severity was defined. Combining brain imaging of mild and moderate TBI within same analysis can be problematic as moderate TBI often have more structural imaging deficits compared with mild. In that case, brain imaging findings are more likely to be driven by severe injury in moderate TBI and are less likely to reflect the brain imaging changes in mild TBI.
Reproducible findings
The most consistent findings reported in this systematic review are mainly from six studies (Caeyenberghs et al., 2015; Caeyenberghs et al., 2012; Caeyenberghs et al., 2011; Caeyenberghs et al., 2010; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b) from the same research center or authors, with partially overlapping patient cohorts across the studies (nb: some studies also showed an apparent complete overlap of sample (Caeyenberghs et al., 2012; Caeyenberghs et al., 2011; Caeyenberghs et al., 2010) however, we can only speculate about cohort overlap since we did not contact the authors to confirm about the potential overlap in reported cohorts.
In three studies with overlapping samples (Caeyenberghs et al., 2012; Caeyenberghs et al., 2011; Caeyenberghs et al., 2010), the cerebellum was shown to link with imbalance in two studies (Caeyenberghs et al., 2012; Caeyenberghs et al., 2010). Other findings were not reproduced among the three studies (Caeyenberghs et al., 2012; Caeyenberghs et al., 2011; Caeyenberghs et al., 2010), possibly due to difference in sample sizes and analysis methods.
From five other studies with partially overlapping patient cohorts (Caeyenberghs et al., 2015; Diez et al., 2017; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b; Liang et al., 2021), Caeyenberghs et al. (2015), Drijkoningen et al. (2015a), and Drijkoningen et al. (2015b) reported link of imbalance with cerebellum. However, the cerebellar lobules reported in Drijkoningen et al. (2015b) are not consistent with findings of Caeyenberghs et al. (2015), whereas Drijkoningen et al. (2015a) reported no subregion.
In general, despite selecting participants from a patient cohort pool with partial or complete overlap in participants between studies, the findings do not overlap within these eight studies (Caeyenberghs et al., 2015; Caeyenberghs et al., 2012; Caeyenberghs et al., 2011; Caeyenberghs et al., 2010; Diez et al., 2017; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b; Liang et al., 2021). Although the lack of reproducibility can be attributed to the methodological differences or low sample sizes, a general lack of reproducible findings in overlapping patients maybe due to factors beyond simple methodology, including maladaptive clinical disorders (Seemungal and Passamonti, 2018), which may develop over the time such that individual patients' performance could vary over time.
Sample size and statistical considerations
Multiple studies performed correlations between balance measures and the brain regions within groups (within controls and within TBI) and with all participants together (controls and TBI combined) (Caeyenberghs et al., 2015; Calzolari et al., 2021; Delano-Wood et al., 2015; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b; Kim et al., 2019; Wang et al., 2019). However, a direct statistical comparison of the two groups' correlation was often missing. Moreover, if studies performed multiple comparisons (multiple contrasts) or had multiple outcomes measures to assess balance, whether the p values were corrected for multiple contrasts and/or the multiple balance measures was not explicitly stated.
It is worth highlighting that the analysis within TBI subgroups could be useful, if performed between TBI patients with and without impaired balance, as it could control for TBI-specific findings. Only one study in this review performed such analysis, using TBI group without imbalance (n = 11) as a control group and compared it with TBI with imbalance (n = 19) (Calzolari et al., 2021). Notably, two EEG studies (Helmich et al., 2020; Helmich et al., 2016) also performed similar analysis to compare balance of mild TBI with and without post-concussive symptoms. However, notably the groups in this case were categorized on the basis of post-concussive symptoms rather than imbalance, and thus the EEG findings during a balance task would reflect the functional brain changes linked to the post-concussive symptoms and not due to imbalance.
The sample sizes of studies we included in this systematic review were considered low, given the recent recommendations of sample sizes (n ∼ 75) for brain-wide association studies (Marek et al., 2022; Spisak et al., 2023). Thus, we include a cautionary note, to interpret the findings from the studies included in this systematic review in the context of all available information.
Consideration of lesion mapping
In this review, studies that did not clearly address the brain lesions were classified as unclear risk. Lesion mapping or controlling for lesions may have relevance for a few reasons. First, if the lesion is not automatically masked out during the segmentation process during preprocessing, it could be incorrectly characterized as gray- or white-matter tissue, which could later result in false positives due to abnormal signal intensity values. Second, mapping lesions can differentiate between the different mechanisms of injury and its recovery, for example, a significant finding on brain imaging could indicate the presence of a lesion or it could represent a secondary compensatory functional/structural changes in response to injury (Liang et al., 2021).
Even mild/concussed individuals with normal CT findings could still have observable lesions on an MRI (Kurča et al., 2006; Kushner, 1998). Up to 25% of uncomplicated mild TBI could have lesions of sizes ranging from 1 to 10 mm in diameter (van der Horn et al., 2018) and these lesions could potentially result in neuropsychological differences between mild TBI with and without lesions (Kurča et al., 2006). Thus, we think that all studies in TBI should address their approach to lesion identification to increase sample homogeneity, which is important when studying individuals with brain injury to reduce false positives in the significant brain imaging findings.
Imbalance in TBI and proprioception
It is also worth mentioning that none of the studies systematically assessed proprioception. The participant exclusion criteria in studies often listed any “musculoskeletal condition,” but it was not always clear if this was a reference to post-injury “condition.” Proprioception has not been directly measured in TBI however its functioning can be partially inferred from posturography. Specifically, if there is a deficient proprioceptive signal (or its processing) then simply closing the eyes while standing upon a hard surface should greatly compromise balance. However this was not born out in the one acute prospective study in moderate-to-severe TBI (Calzolari et al., 2021) where there was an outsized impact of impaired vestibular signal processing (as evidenced by the disproportionate impact of sway in the “eyes closed soft surface” condition).
A search on “Web of Science” relating imbalance, TBI, and proprioception or somatosensory system (without including imaging search terms) only resulted in 29 articles. Within these 29 studies, no study directly and prospectively assessed proprioception or linked it with brain imaging. A recent study in concussed individuals also claimed that the proprioception has never been systematically assessed in concussion (Lempke et al., 2023).
Thus, a systematic assessment of proprioception is needed in future studies, which can shed some light on proprioceptive contribution in deficits of postural balance post-TBI.
Current evidence of neural correlates of imbalance in TBI
The findings of our systematic review with respect to the literature is discussed below.
Cerebellum
The recurring finding from all included studies was cerebellum, which was reported in three studies that performed whole-brain analysis (Bittencourt et al., 2022; Caeyenberghs et al., 2015; Caeyenberghs et al., 2012), and in three studies that used cerebellum as an ROI (Caeyenberghs et al., 2010; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b). However, among these studies, the subregions localized within the cerebellum were not consistent. Caeyenberghs et al. (2010) used cerebellum (as a whole) in ROI analysis and thus no specific subregion is reported.
Caeyenberghs et al. (2012) reported lower connectivity degree (a structural connectivity measure) linked to poor balance in cerebellar lobule IX, which is considered an important site for processing vestibular signals in humans and is often termed as vestibular cerebellum (Barmack, 2003; Kheradmand and Zee, 2011; Nigmatullina et al., 2015). Skilled dancers with high balance ability are also reported to have lower gray-matter volume in cerebellum lobule IX (Nigmatullina et al., 2015), which could reflect the important role of cerebellum lobule IX in vestibular function, including postural balance.
An important consideration is the impact of injury distant to the site of the observed brain imaging effect. In this regard, one study showed that balance impaired individuals due to incomplete spinal cord injury had reduced volume in cerebellum lobule IX (Villiger et al., 2015), implying a component of this atrophy is secondary Wallerian degeneration from disrupted proprioceptive signal input after spinal cord injury (and hence, it further emphasizes the need for detailed clinical assessment to account for or exclude peripheral vestibular or proprioceptive dysfunction).
Caeyenberghs et al. (2015) reported involvement of cerebellar vermis I–II in mediating postural imbalance in TBI. The flocculonodular lobe and adjacent caudal vermis (the vestibulocerebellum) is key for postural control. The vermis per se (the spinocerebellum) is involved in purposeful limb coordination and hence cooperates with the vestibulocerebellum particularly during walking. A systematic review and meta-analysis, looking at studies that performed a mental imagery of a postural task in healthy individuals, reported that six out of eight included studies reported activation in cerebellar vermis (Dijkstra et al., 2020). One study, using mobile PET scan while standing on one foot (Ouchi et al., 1999), showed an increased activation of anterior cerebellar vermis, highlighting the active role of this region in mediating the postural balance.
Drijkoningen et al. (2015a) did not report a subregion in cerebellum, whereas Drijkoningen et al. (2015b) found that reduced gray- and white-matter volume in cerebellar lobules I–IV, V, and VI were linked to imbalance. Another study included in this review (Bittencourt et al., 2022) reported that post-TBI vestibular symptoms (including imbalance) were linked to altered connectivity of cerebellar lobule VI and crus I.
In individuals with balance impairment (incomplete spinal injury) (Villiger et al., 2015) and Parkinson's disease (Sehm et al., 2014), balance training caused an increase in volume of cerebellum lobules V and VI, suggesting their link with balance training and their possible role in post-TBI imbalance. Similarly, reduced volume in cerebellum lobules IV, V, and VI have also been linked to postural imbalance in multiple sclerosis (Prosperini et al., 2013).
Cerebellar peduncles
The second most consistent finding from the included studies was the cerebellar peduncles, including superior, middle, and inferior cerebellar peduncles (SCP, MCP, and ICP). SCP and MCP are reported to be linked with imbalance in TBI in the three studies (Caeyenberghs et al., 2010; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b), all of which used SCP and MCP tracts as ROIs, whereas ICP was linked with imbalance in two studies (Drijkoningen et al., 2015a; Kim et al., 2019).
One of the study reported that the FA value in ICP increased with balance training (Drijkoningen et al., 2015a). In contrast, a previous study in multiple sclerosis patients with impaired balance (Prosperini et al., 2014) reported that ICP did not show significant improvement in DTI parameters in response to balance training, whereas an increase in FA and radial diffusivity (RD) in SCP was observed. Thus, SCP and ICP seems to be linked with imbalance and may also respond to balance training, whereas MCP is only reported to be linked with imbalance on baseline testing of TBI patients but not to balance training. Note that we cannot systematically suggest that MCP is not involved when performing balance training as it is implausible.
Multiple studies in MS patients have previously reported the link between postural deficits and low FA and increased RD values in SCP (Gera et al., 2020), MCP (Odom et al., 2021), and ICP (Gera et al., 2020; Odom et al., 2021); notably, both these studies also used analysis in which cerebellar peduncles were selected as ROIs. Similar association of diffusion parameters with SCP and MCP has also been reported in Parkinson's disease patients (using SCP, MCP, and ICP as ROIs) with freezing of gait (Bharti et al., 2019), suggesting their link with postural balance in neurodegeneration.
In general, there is existing evidence of altered diffusion parameters of cerebellar peduncles and linked imbalance in neurodegeneration. Notably, however, the studies that used these tracts (SCP, MCP, and ICP) as ROIs were often the ones that reported them to be linked with balance (Caeyenberghs et al., 2010; Drijkoningen et al., 2015a; Drijkoningen et al., 2015b), which is important to consider in terms of analysis to avoid selection bias in reported findings.
Other inconsistent reported findings
Most of the studies included in this systematic review reported brain regions or white-matter tracts, which were not reported in any of the other T1-weighted, DTI, fMRI, and resting-state imaging studies. These included ML (Caeyenberghs et al., 2010), CST (Caeyenberghs et al., 2011), superior parietal gyrus (Caeyenberghs et al., 2012), left putamen (Caeyenberghs et al., 2015), a prefrontal functional network (Diez et al., 2017), pons and medulla (Drijkoningen et al., 2015b), left occipital gyrus (Wang et al., 2019), pontine tegmentum (Delano-Wood et al., 2015), and ALIC (Caeyenberghs et al., 2010; Calzolari et al., 2021). A comprehensive review of literature discussing these findings is provided in Supplementary Data.
Conclusions and Recommendations
Our findings indicate that the mechanisms underlying postural deficits in TBI are poorly understood. Given the multiple levels of vulnerability ranging from the vestibular organ, the nerve, brainstem and cerebellar circuits, thalamic relay areas, and cortical processing pathways, it is likely that traumatic brain injury could result in imbalance through multifocal injury to the central nervous system. This could also explain the inconsistency in findings of current literature.
Thus, apart from controlling for peripheral diagnoses (vestibular organ and nerve-related problems), studies should account for multiple models of postural control to avoid selection bias in reporting and inconsistent findings. Individual studies looking at subcortical function separate from cortical function may also produce findings biased toward certain regions, thus a whole-brain analysis approach is recommended. Vestibular dysfunction in TBI can go unnoticed since patients' subjective reports of their balance do not correlate well with clinical and objective assessment of balance (Marcus et al., 2019; Sargeant et al., 2018; Wood et al., 2022) and thus a subjective balance assessment is recommended.
Finally, none of the studies included in this review accounted for brain lesions, and it is possible that the lesions and their spatial location might contribute to the findings in the studies and hence could also be a predictor of imbalance. It is also important to state that sample sizes in the studies were low, which contribute to the lack of replicable findings across studies with independent samples.
Based on our findings, following are some key recommendations for an ideal study in TBI investigating the brain mechanisms of imbalance: (i) clear statement of what scale is used for defining severity of traumatic brain injury; (ii) clinically well-characterized TBI cohort to indicate the presence of peripheral sensory and motor dysfunction (including vestibular and proprioceptive) and chronic neurological, psychiatric, and medical conditions to enable either their exclusion or allow their presence to be factored into an adequately powered study assessing the impact of these comorbidities upon balance function and its longitudinal recovery; (iii) objective (i.e., instrumented) assessment of postural balance is important to accurately measure the degree of imbalance; (iv) selecting appropriate patient control groups instead of using healthy participants for comparisons to reduce findings that are nonspecifically linked to TBI; and (v) a wholebrain analysis approach, in comparison with ROI analysis, to avoid selection bias in reported findings. Finally given recent recommendations (Marek et al., 2022; Spisak et al., 2023), sample sizes of at least n = 75 (ideally more) are needed to estimate accurate effect sizes and for reproducible findings.
Footnotes
Data Availability
All data produced in this study are summarized in the form of tabulated information and is provided along with the article.
Authors' Contributions
Conceptualization, investigation, methodology, software, formal analysis, visualization, and writing—original draft by Z.H. Methodology and writing—review and editing by M.M. Project administration, funding acquisition, resources, supervision, and writing—review and editing by B.M.S.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by the Medical Research Council (MRC) (MR/P006493/1), The Jon Moulton Charity Trust, and the US Department of Defense—Congressionally Directed Medical Research Program (CDMRP).
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Appendix A1.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.