
Abstract
Traumatic brain injury (TBI) and stroke are the most common causes of acquired brain injury (ABI), annually affecting 69 million and 15 million people, respectively. Following ABI, the relationship between brain network disruption and common cognitive issues including attention dysfunction is heterogenous. Using PRISMA guidelines, we systematically reviewed 43 studies published by February 2023 that reported correlations between attention and connectivity. Across all ages and stages of recovery, following TBI, greater attention was associated with greater structural efficiency within/between executive control network (ECN), salience network (SN), and default mode network (DMN) and greater functional connectivity (fc) within/between ECN and DMN, indicating DMN interference. Following stroke, greater attention was associated with greater structural connectivity (sc) within ECN; or greater fc within the dorsal attention network (DAN). In childhood ABI populations, decreases in structural network segregation were associated with greater attention. Longitudinal recovery from TBI was associated with normalization of DMN activity, and in stroke, normalization of DMN and DAN activity. Results improve clinical understanding of attention-related connectivity changes after ABI. Recommendations for future research include increased use of electroencephalography (EEG) and functional near-infrared spectroscopy (fNIRS) to measure connectivity at the point of care, standardized attention and connectivity outcome measures and analysis pipelines, detailed reporting of patient symptomatology, and casual analysis of attention-related connectivity using brain stimulation.
Impact statement
This systematic review concisely and meaningfully synthesizes a large heterogenous body of research relating to the association between attention and brain connectivity to identify clear trends in traumatic brain injury (TBI) and stroke and recommend a path forward in clinical prognosis in children and adults. We consider a broad range of structural and functional connectivity measures (e.g., diffusion tensor imaging [DTI], functional magnetic resonance imaging [fMRI], electroencephalography [EEG], and functional near-infrared spectroscopy [fNIRS]) and analyses (e.g., voxel- and region of interest [ROI]-based, graph theory, network-based statistics, and others) and examine both cognitive and behavioral measures of attention (e.g., executive, spatial or sustained attention, or inhibition), and conclude with recommendations for further research and clinical practice.
Introduction
Outcomes after acquired brain injury
Acquired brain injury (ABI) is a leading cause of death and disability worldwide (Greenwald et al., 2003). ABI is defined as injury occurring to the brain after birth and can present focally (e.g., after stroke), or diffusely (e.g., after traumatic brain injury [TBI]) (Pudenz and Shelden, 1946). TBI and stroke are two of the most common causes of ABI, affecting 69 million (Dewan et al., 2018) and 15 million (Ekker et al., 2019) people worldwide each year, respectively. TBI occurs most frequently in children and youth, with more than 640/100,000 people under 24 years of age sustaining an injury annually (FitzGerald et al., 2008).
Diffuse injuries such as TBI are commonly seen due to high-energy acceleration–deceleration forces, resulting in diffuse axonal injury (DAI) (Gennarelli, 1983; Gennarelli et al., 1982). In contrast, stroke is usually focal and results from a vascular ischemic or hemorrhagic event (Fan et al., 2002; Tsze and Valente, 2011). Less well appreciated is that stroke also occurs in children (Lynch, 2004), with an incidence of 1 in 2500–4000 live births and 2–8 in 100,000 infants and children (DeVeber, 2000). Depending on the extent and type of injury sustained, ABI often results in ongoing symptoms that can often be present for months to years after injury (Lannoo et al., 2004).
Outcomes after ABI are variable due to the heterogeneous nature of the injury and the pre-existing and environmental factors that influence recovery (Covington and Duff, 2021). After TBI, motor, cognitive and behavioral problems are found in 53% of TBI patients at 1 year postinjury (Dikmen et al., 2010), where poorer outcomes often occur with higher injury severity and greater diffuse injury (Martin and Falcone Jr., 2008; McAllister and Arciniegas, 2002).
After acute stroke, mortality occurs in 38% of adult hemorrhagic stroke and 8% of ischemic cases (Rosamond et al., 1999), and ∼50–60% of children with stroke have long-term neurological morbidity (DeVeber, 2005; Kirton et al., 2007; Lanthier et al., 2000). Although most people achieve functional independence after stroke, 15–30% have permanent disability (Zorowitz et al., 2002) and decreased quality of life due to speech, sensory, mobility, and/or executive function (EF) deficits (Zorowitz et al., 2002).
Impairments in EF are the hallmark of cognitive sequelae after ABI (Caeyenberghs et al., 2014; Ewing-Cobbs et al., 2004; Kumar et al., 2013; Levin et al., 2004; O'Keeffe et al., 2014). EF describes a set of complex inter-related complex cognitive functions. Attention, which is the process of selectively filtering for behaviorally relevant stimuli in the environment (Alves et al., 2022), is a key component of EF, which is most commonly affected after ABI (Arciniegas et al., 2002; Markovic et al., 2020).
Attention facilitates the synthesis of external stimuli, goal formation, preparation for action, and monitoring of plans and actions (Anderson, 2002). Long-term attention problems can occur after childhood ABI, where children have a 4–5 times greater likelihood of developing secondary attention-deficit disorder (Schachar and Logan, 1990; Schachar et al., 2004) and after stroke 46% of children develop attention-deficit/hyperactivity disorder (ADHD) (Max et al., 2003).
Attention deficit is complex and may be caused by dysfunction in one or several inter-related functions, including executive attention, spatial attention, attentional inhibition, or sustained attention. Often, the extent of disruption depends on the type of damage sustained during an ABI. For example, spatial deficits are common after a focal, nontraumatic injury such as stroke (Cassidy et al., 1999), and deficits in attentional inhibition are common after TBI (Dockree et al., 2004; Hooper et al., 2004). These deficits relate to damage in structural and functional brain networks (Sharp et al., 2014) and, therefore, are best understood by considering changes in brain connectivity.
Brain networks and attention function
There are several distinct brain networks that facilitate attention-related functions (Fig. 1) (Barkley, 1997; Krauzlis et al., 2023). Executive attention is primarily controlled by the executive control network (ECN), a frontoparietally oriented network that interfaces with several attention-related networks. These include the salience network (SN), dorsal attention network (DAN), ventral attention network (VAN), and default mode network (DMN) (Li et al., 2023; Sharp et al., 2014; Wong et al., 2023). Attentional inhibition is a related attention function, which facilitates attention to behaviorally relevant stimuli while ignoring distracters. Inhibition is coordinated by the SN, a bottom-up attention network that is responsible for coordinating involuntary shifts in attention in response to unexpected stimuli (Aron, 2011; Meyer and Bucci, 2016). Sustained attention allows the continued detection of rarely and unpredictably occurring signals over prolonged periods of time (Mackworth, 1968; Sarter et al., 2001), and similar to inhibition, is necessary for concentrated goal-directed behavior. Sustained attention is primarily facilitated by the ECN, DAN, VAN, and task-negative DMN (Esterman and Rothlein, 2019). Finally, spatial attention is a form of selective attention, which is allocated to a specific location in the visual space while filtering out visual input from unattended locations (Kim and Kastner, 2019). Spatial attention is facilitated primarily by the DAN and VAN (Weissman and Prado, 2012), and is commonly affected after stroke, where ∼70% of stroke patients experience spatial neglect in the visual field (Stone et al., 1993) (Fig. 1).
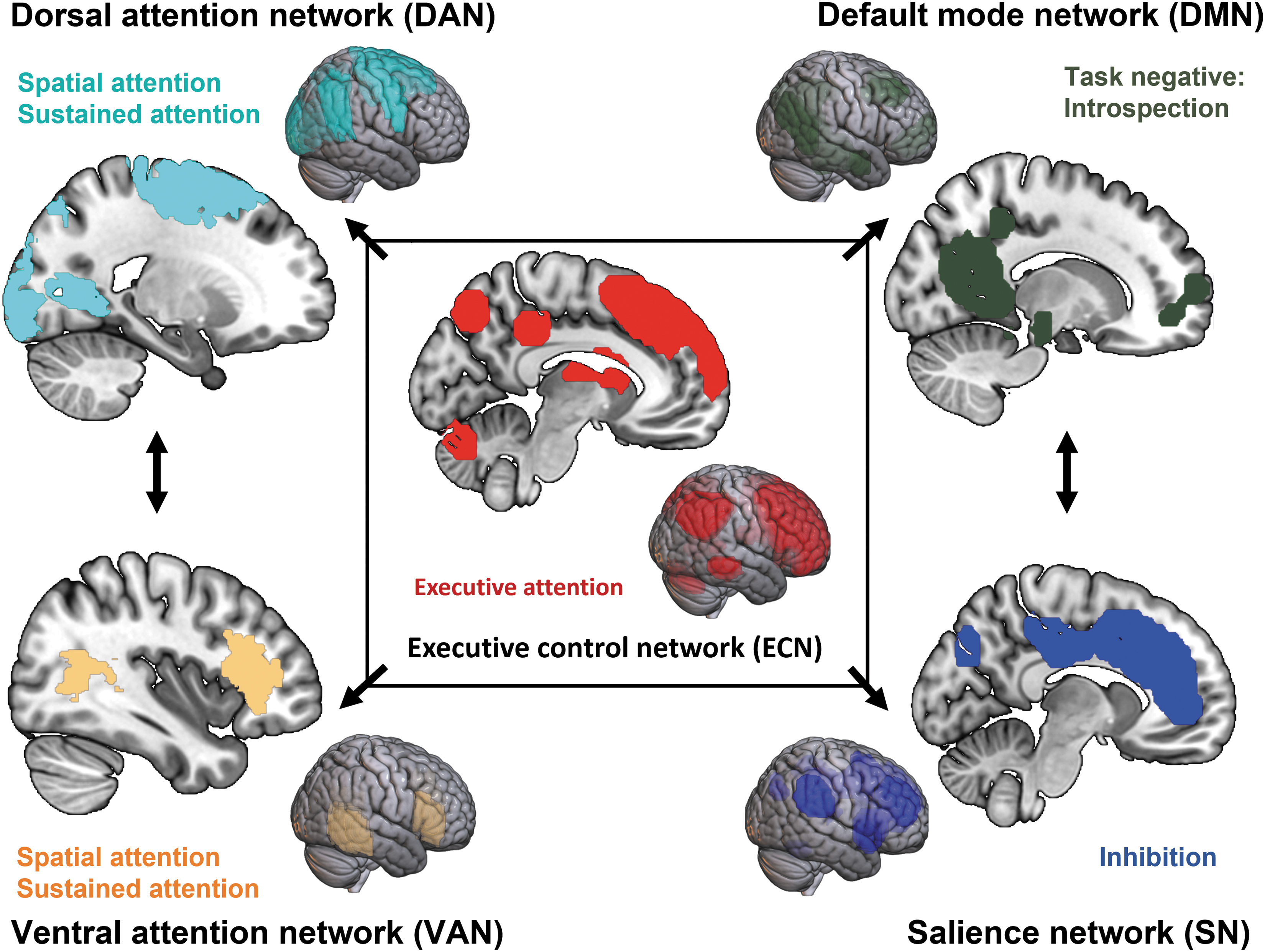
Core attention networks and predominant attention-related functions. Brain network masks created using FMRIB Software Library (FSL) and Avants (2015).
Measuring attention-related brain network disruption
Attention functions are underpinned by a complex system of structural and functional brain networks. These networks comprise interconnected brain regions (nodes) that integrate locally and distally through axons and white matter tracts (edges) to facilitate information transfer both locally and distally (Van Den Heuvel and Sporns, 2011; Xiao et al., 2015). The most well-studied brain networks implicated in attention are task-active networks including the DAN (frontoparietal network), VAN, SN, as well as the resting state DMN (Li et al., 2023; Sharp et al., 2014; Wong et al., 2023).
Brain connectivity can be examined in several ways, for example, by considering whole-brain network architecture through graph theory approaches, or through other structural, functional, or effective connectivity approaches, which may consider network synchronization, correlation, or coherence patterns, among others (Farahani et al., 2019).
Seed-based analysis is a traditional connectivity approach, quantifying correlation between activity in a predefined region of interest (ROI) and other brain regions. In contrast, graph theory is a mathematical framework facilitating representation of complex networks. According to graph theory, the brain is composed of nodes that represent regions, as well as edges, which represent structural or functional connectivity within or between nodes (Bullmore and Sporns, 2012; Sporns, 2013). Common graph metrics include modularity, which reflects the strength of network division into modules; efficiency, which reflects the capacity for parallel information transfer and integrated processing (Bullmore and Sporns, 2012); and path length, which describes the efficiency of information transfer (Bassett and Bullmore, 2006). These connectivity analysis approaches can be applied to structural or functional network analysis.
Quantitative structural imaging
Structural connectivity (sc) in vivo commonly uses diffusion tensor imaging (DTI) techniques, including diffusion tensor tractography, to model white matter pathways on a voxel-by-voxel basis (Mori and Van Zijl, 2002; Xiao et al., 2015), or using measures of water diffusion such as fractional anisotropy (FA) and mean diffusivity (MD), which provide information about the structural integrity of a white matter tract (Haris et al., 2006; Le Bihan et al., 2001). These anatomical metrics enable quantification of potential macro- and microscale changes to structural brain networks and their reorganization after ABI (Puig et al., 2011; Wang et al., 2011).
Functional connectivity
Effective cognitive processing relies on the integration of information across different regions of the brain. This integration is made possible by well-organized functional networks that exhibit statistical dependencies over time (Friston, 2011). Functional connectivity (fc) provides a direct quantification of these statistical dependencies, providing insights into coordinated activations in distinct brain regions.
Functional connectivity can be assessed during cognitive engagement to explore the functional organization related to task demands (Gonzalez-Castillo and Bandettini, 2018) or in the absence of a specific task, providing valuable information about the inherent functional organization during periods of rest (Gusnard and Raichle, 2001). Imaging measures such as functional magnetic resonance imaging (fMRI), electroencephalography (EEG), and functional near-infrared spectroscopy (fNIRS) are commonly employed used to measure fc (Friston, 2011).
In summary, structural and functional connectivity analyses not only provide valuable insights into the neurological determinants of clinical outcome but also offer the opportunity of a brain-based biomarker that could help monitor recovery and response to treatment after ABI (Irimia et al., 2012). Given that attention deficits are among the most prevalent cognitive issues after ABI, our objective was to synthesize the existing evidence on the link between brain connectivity and attention in individuals affected by ABI. Using a systematic review approach, we investigated the association between structural and functional connectivity and attention performance in both children and adults after ABI.
Methods
Literature search
Articles were identified through a systematic search of seven computerized databases: Medline, CINAHL, EMBASE, PsycINFO, the Cochrane Library, Scopus, and Web of Science. To comprehensively capture relevant literature, the following keywords were included: “acquired brain injury or traumatic brain injury or concussion or brain injury or stroke or brain infection and EEG or quantitative EEG or MRI or diffusion tensor imaging or functional near infrared spectroscopy and connectivity or network analysis or graph theory or network or independent component analysis or deep learning and recovery or cognition or neurocognition or neuropsych or neurological or clinical or symptom or memory or attention or inhibition.”
After the initial search, we used a Covidence keyword search to specifically isolate attention and inhibition-related outcomes from the larger search pool: “attention”, “inhibition”, “reaction time”, “stop signal”, “no go”, “flanker”. See Supplementary Methods in the Supplementary Data for full search strategy.
Inclusion and exclusion criteria
ABI was defined as any traumatic (e.g., TBI) or nontraumatic injury occurring to the brain after birth (Greenwald et al., 2003). Studies were included if they included participants of any age with ABI and measured brain connectivity (either at rest or task-based) at any time postinjury using (1) conventional, quantitative, or high-density EEG, (2) DTI (if measured within white matter tracts or between ROIs), task-based fMRI or resting-state fMRI, or (3) fNIRS. Studies were excluded if they involved nonhuman participants (i.e., animal studies); if the sample size was n = 1 (i.e., clinical case studies); if participants had a developmental or progressive brain injury (including congenital brain defects or progressive diseases such as Parkinson's or Alzheimer's diseases) or were diagnosed with brain neoplasm/tumor [due to significant differences in injury mechanisms (Ownsworth et al., 2009)]; if reported outcomes only related to measurements taken using tools other than EEG, magnetic resonance imaging (MRI), or fNIRS; or if studies were published in languages other than English or German.
Screening
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews (Moher et al., 2015) and was registered in PROSPERO (CRD42022273141). After the search, EndNote (Version 20; Clarivate) was used for deduplication. References were then imported into the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia).
Title and abstract screening was conducted by A.S., J.R.T., and K.M.B. Each article was screened by two reviewers. Disagreements were resolved through joint meeting and consensus. Full text screening was independently undertaken by A.S. and J.R.T., and any disagreements were resolved by K.M.B. (Fig. 2).
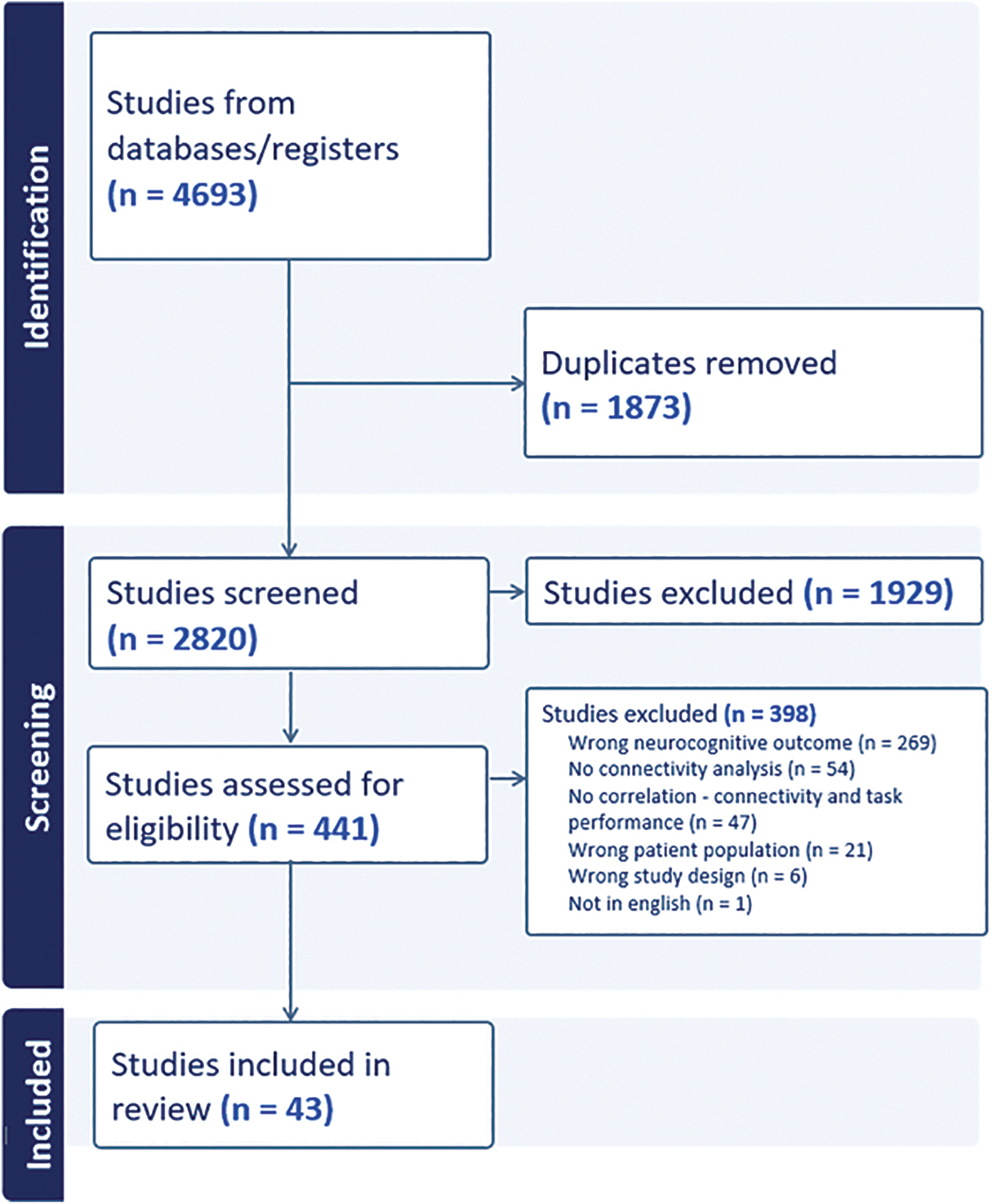
PRISMA flowchart of included studies. Note: Results are shown from two searches—(1) initially conducted in August 2021 and (2) an updated search in February 2023. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality assessment
The quality of included studies was assessed by three independent reviewers (A.S., J.R.T., and K.M.B.) using the AXIS tool (Supplementary Table S1 in the Supplementary Data) (Downes et al., 2016). This tool was uniquely developed to assess the quality of cross-sectional studies (the main research methodology employed by the relevant literature) (Downes et al., 2016). The specific interpretation of items was adapted to improve applicability to the neuroimaging field (see Supplementary Table S1 in the Supplementary Data for interpretation specific to this systematic review).
After discussion between assessors, consensus was reached on the final quality scores (Supplementary Table S5 in the Supplementary Data). The AXIS tool does not provide an overall rating of quality and instead specifies that studies should receive one point for each criterion satisfied (for a total of 20 points) (Harst et al., 2019; Sahu et al., 2020). As up to two criteria were disregarded as being applicable for studies in this review, studies were rated out of 18 or 19 and an adjusted score (calculated out of 20) was reported to maintain convention (Supplementary Table S1 in the Supplementary Data). No articles were excluded based on the quality assessment.
Data extraction
Forty-three articles were included in the final analysis. Demographic characteristics are recorded in Tables 1 and 2. Details of attention tasks, imaging technique, and type of correlation statistic used to examine the association between attention and brain connectivity (i.e., Pearson or Spearman) are recorded in Tables 3 and 4. The interpretation and effect size of correlations between connectivity and attention, as well as AXIS quality score are presented in Tables 5 and 6.
Demographics Traumatic Brain Injury
DTI, diffusion tensor imaging; fMRI, functional magnetic resonance imaging; rs-fMRI, resting state functional magnetic resonance imaging; SD, standard deviation; SES, socioeconomic status; TBI, traumatic brain injury.
Demographics Stroke
AIS, arterial ischemic stroke; MCA, middle cerebral artery; N/A, not applicable (not given); PVI, periventricular venous infarction; SEM, standard error of the mean.
Imaging and Attention Task Parameters in TBI
AD, axial diffusivity; ANT, Attention Network Test; BRIEF, Behavior Rating Index of Executive Function; CPT, Continuous Performance Task; CRT, choice reaction task; D-KEFS CWIT, Delis-Kaplan Executive Function System Color-Word Interference Test; EEG, electroencephalography; FA, fractional anisotropy; fc, functional connectivity; FDR, false discovery rate; fNIRS, functional near-infrared spectroscopy; FWE, Family-Wise Error Rate; GEC, Global Executive Composite; GNG, Go/No-Go Task; ICA, independent component analysis; LGT, Local-Global Task; MI, Metacognition Index; MOCA, Montreal Cognitive Assessment; NBS, network-based statistics; PPI, psychophysiological interaction; ReHo, regional homogeneity; ROI, region of interest; RT, reaction time; SART, Sustained Attention to Response Task; SSRT, Stop Signal Reaction Time; TEA, Test of Everyday Attention; TMT, trail-making test; VSAT, Visual Search and Attention Test.
Imaging and Attention Task Parameters in Stroke
ADHD-5, Attention Deficit Hyperactivity Disorder Rating Scale 5; BIT, Behavioral Inattention Test; iCAP, innovation-driven co-activation patterns; MD, mean diffusivity; PCA, principal component analysis; WASI, Wechsler Abbreviated Scale Intelligence; WISC, Wechsler Intelligence Scale for Children.
Associations Between Connectivity and Attention in Traumatic Brain Injury
Effect sizes expressed as Pearson or Spearman correlation coefficients (direction of correlation not shown for simplicity). Refer to Supplementary Results (Supplementary Table S6) in the Supplementary Data for more detail.
p Values not given.
ACC, anterior cingulate cortex; ACR, anterior corona radiata; AG, angular gyrus; AI, anterior insula; ATL, anterior temporal lobe; CB, cingulum bundle; CC, corpus callosum; CG, cingulate gyrus; CP, cerebral peduncle; dACC, dorsal anterior cingulate cortex; DAN, dorsal attention network; dlPFC, dorsolateral prefrontal cortex; DMN, default mode network; EC, external capsule; ECN, executive control network; FG, fusiform gyrus; IFG, inferior frontal gyrus; IOC, inferior occipital cortex; IPL, inferior parietal lobule; ITG, inferior temporal gyrus; MFG, middle frontal gyrus; MN, motor network; MOG, middle occipital gyrus; MTG, middle temporal gyrus; PCC, posterior cingulate cortex; PPC, posterior parietal cortex; post-CG, post-central gyrus; pre-CG, pre-central gyrus; pre-SMA, pre-supplementary motor area; rIFG, right inferior frontal gyrus; sc, structural connectivity; SFG, superior frontal gyrus; SLF, superior longitudinal fasciculus; SMA, supplementary motor area; SMG, supramarginal gyrus; SN, salience network; STG, superior temporal gyrus; TP, temporal pole; UF, uncinate fasciculus; VAN, ventral attention network; VN, visual network.
Associations Between Connectivity and Attention in Stroke
Effect sizes expressed as Pearson or Spearman correlation coefficients (direction of correlation not shown for simplicity). Refer to Supplementary Results (Supplementary Table S7) in the Supplementary Data for more detail.
dIPS, dorsal intraparietal sulcus; FEF, frontal eye fields; mIPS, medial intraparietal sulcus; pIPS, posterior intraparietal sulcus; PMC, primary motor cortex; SMC, supplementary motor cortex; SPC, superior parietal cortex; SPL, superior parietal lobule; STS, superior temporal sulcus; TPJ, temporoparietal junction; vIPS, ventral intraparietal sulcus.
Data synthesis
Meta-analysis was not possible due to the heterogeneity of research studies. Instead, an adopted alternative synthesis methodology was used known as synthesis without meta-analysis (SWiM) guidelines (Campbell et al., 2020) [previously described (Torres-Simón et al., 2022)]. Using these guidelines, included studies were first grouped into (1) injury type (TBI, stroke, or other), then (2) neuroimaging modality (structural: DTI; functional [resting or task-based]: fMRI, EEG, and fNIRS). Within these modalities, results were further classified by (3) attention domain (executive attention, inhibition, sustained attention, or spatial attention), (4) age group (where 0–18 years was classified as pediatric; 19–65 years classified as adult, and 66+ years classified as older adult), (5) recovery phase (where 0–6 days was classified as acute; 7–29 days as subacute, and 30+ days as chronic), and (6) brain network or region of connectivity.
All results are included in Tables 2 to 6. Information regarding the classification of brain regions into respective brain networks are given in Supplementary Table S4.
Results
Description of studies
After deduplication, a total of 2820 studies were initially identified from a search in August 2021 and an updated search in February 2023. After title and abstract screening, 441 studies were sought for retrieval for full text screening. Studies were excluded due to neurocognitive outcome not of interest (269), lack of connectivity analyses (54), no correlation made with task performance (47), wrong patient population (21), study design (6), and language other than English or German (1). Forty-three studies were included in the systematic review (Fig. 2). The mean AXIS quality assessment score (adjusted to reflect a score out of 20) was 16.01, where the lowest was 12.2 (one study) and the highest 18.9 (four studies) (Supplementary Table S5 in the Supplementary Data).
Sample characteristics
Studies all involved TBI or stroke as mechanism of injury (see Tables 1 and 2 for demographics). There were 24 TBI studies recruiting n = 974 TBI patients (adults: n = 858, mean 36.09 [standard deviation, SD 7.3] years, 55.4% male; and children: n = 116, mean 14.6 [SD 1.3] years, 57.8% male). Participants were predominantly in the chronic phase of TBI recovery (adults: mean 26.1 months [SD 31.5 months, range <3 days to 11.4 years] postinjury; and children mean 10.11 months [SD 6.4 months, range <6 months to 1.7 years] postinjury).
In most cases, studies did not report details of injury severity in each participant, and instead reported an overall description (e.g., “moderate to severe TBI”). Therefore, the proportion of participants included across injury severities could not be calculated. Included studies predominantly reported on mild TBI but ranged from mild to severe. Two TBI studies were interventional: a 10-week program to improve attention (Yuan et al., 2017) and a 13-week Brain Fitness Program for auditory processing (Lindsey et al., 2022). All studies included healthy controls, except one that included a TBI comparison group (Table 1) (Lindsey et al., 2022).
Nineteen stroke studies recruited a total of n = 1209 patients (adults: n = 1147, mean 58.0 [(SD 5.7] years, 58.2% male; and children: n = 72, mean 13.7 [SD 1.8] years, 61.1% male). Participants were predominantly in the subacute recovery stage (adults: mean 3.9 months [SD 6.0 months, range 9 days to 13.2 months] postinjury and children: mean 126.4 months [SD 41.8 months, range 96.8–156 months] postinjury).
Stroke categories included both left and right ischemic and hemorrhagic stroke but were predominantly ischemic and located in middle cerebral artery (MCA) territory or subcortical regions. All studies included healthy controls (Table 2). These demographics in TBI and stroke populations were calculated using summary statistics reported by studies and, therefore, may not precisely reflect participant characteristics in individual studies.
Outcome assessments
Most studies employed DTI or resting state fMRI (rs-fMRI) or to assess brain connectivity (Fig. 3 and Tables 3 and 4). Two studies employed EEG and one study used fNIRS. Structural connectivity was assessed using ROI or voxel-based FA (n TBI = 6, stroke = 1); tractography (n TBI = 4, stroke = 3); graph theory and/or network-based statistics (NBS; n TBI = 4, stroke = 1).

Data synthesis structure. Note: two TBI studies reported both fMRI and DTI outcomes and are counted separately. DTI, diffusion tensor imaging; EEG, electroencephalography; fMRI, functional magnetic resonance imaging; fNIRS, functional near-infrared spectroscopy; rs-fMRI, resting state functional magnetic resonance imaging; TBI, traumatic brain injury.
Functional connectivity techniques included resting or task-based ROI/voxel-based fc (n TBI = 14, stroke = 12); graph theory and/or NBS (n TBI = 3, stroke = 1). Overall, the most common structural connectivity techniques were ROI-based FA (TBI) and voxel-based FA/tractography (stroke), and the most common functional connectivity technique was ROI-based fc (both TBI and stroke). Please refer to Supplementary Table S2 in the Supplementary Data for a description and explanation of connectivity metrics used.
Attention tasks were categorized as (1) executive attention, (2) spatial attention, (3) inhibition, and (4) sustained attention tasks. Executive attention was the most assessed category in TBI (n = 15 [62.5%] studies), whereas spatial attention was the most assessed category in stroke (n = 11 [57.9%] studies) (Tables 3 and 4 for TBI and stroke, respectively). Details of the attention tasks are summarized in Supplementary Table S3 in the Supplementary Data.
Of the 43 studies included in this review, 42 studies (∼98%) reported at least 1 statistically significant correlation between sc or fc and an attention-related outcome (Figs. 4 and 5). A summary of associations between attention and connectivity are presented in Tables 5 and 6. Notable relationships between attention and connectivity (according to strength of correlation and quality assessment score) are discussed in text (refer to Tables 5 and 6 for full description of results, and Supplementary Tables S6 and S7 in the Supplementary Data for details about correlations).

Graphical representation of white matter tracts where structural integrity displayed significant correlations with attention. Axial and sagittal orientations are shown. All regions in TBI participants except dark green (anterior forceps) reported in stroke participants. Structural integrity in all regions showed a directly proportional relationship with attention, except for uncinate fasciculus, which demonstrated an inversely proportional relationship. Light green, external capsule; dark green, anterior forceps; orange, corona radiata; yellow, cerebral peduncles; pink, genu of corpus callosum; purple, body of corpus callosum; light blue, superior longitudinal fasciculus; dark blue, cingulum bundle; red, uncinate fasciculus (left only). Top panel: axial view, inferior to superior (left to right); bottom panel: sagittal view, left medial to right lateral (left to right).
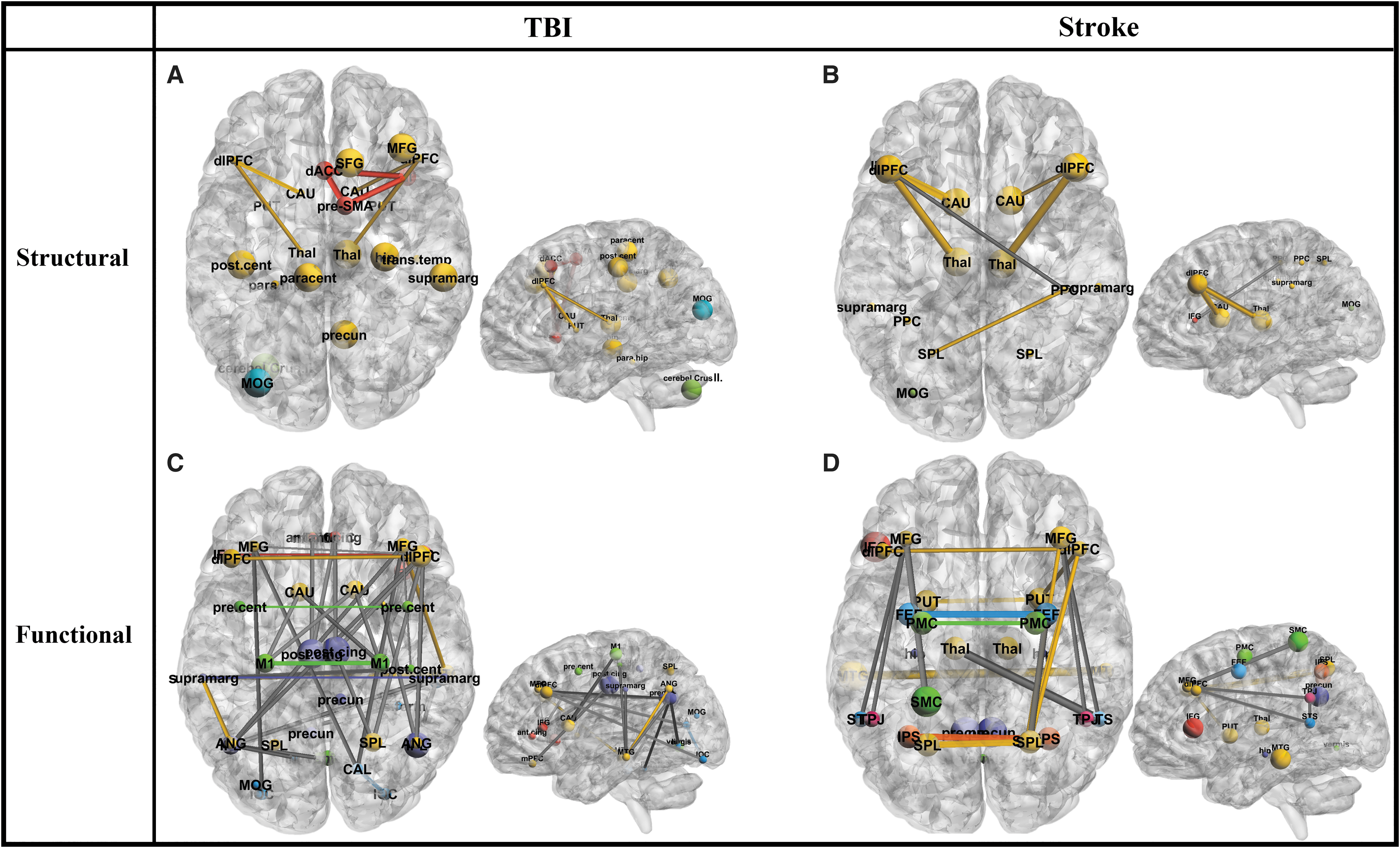
A graphical representation of significant correlations reported between structural or functional connectivity and attention within and between brain regions after TBI and stroke. Axial and sagittal representations of
Greater structural and functional connectivity within and between executive, salience, and DMNs is related to greater attention after TBI
A study with a moderately high-quality rating found that, using structural graph theory approaches, lower mean structural global efficiency was strongly associated with lower executive attention, whereas greater global efficiency was strongly associated with greater spatial attention in 21 participants with chronic moderate to severe TBI (Caeyenberghs et al., 2014). Furthermore, lower structural nodal efficiency of the left postcentral gyrus, right hippocampus, or left cerebellar lobule (somatomotor network and DMN) was strongly associated with lower executive attention. Greater nodal efficiency of the right superior frontal gyrus, right middle frontal gyrus (MFG), right inferior frontal gyrus, right hippocampus, left middle occipital gyrus, left postcentral gyrus, right supramarginal gyrus, right precuneus, or right thalamus (ECN, SN, DMN, and somatomotor network) (Aron and Poldrack, 2006; Behrmann et al., 2004) was strongly associated with greater executive attention (Caeyenberghs et al., 2014).
DMN functional connectivity was directly associated with attention. A study with a moderately high-quality rating in 21 adults with chronic mild-severe TBI found greater functional connectivity within the posterior cingulate cortex (ROI approach) to be strongly associated with greater executive and spatial attention (Sharp et al., 2011). A similar trend was found in another study involving the same population, but with a lower quality assessment rating, where lower task-based functional connectivity within the precuneus was strongly associated with lower sustained attention in 28 participants (also using an ROI-based approach) (Bonnelle et al., 2011).
Finally, a moderately high-quality study in 50 patients with acute mild TBI found greater resting fc within the right insula or between the DMN and ECN (ROI approach) to be moderately to strongly associated with greater executive attention (Li et al., 2020b).
Greater functional connectivity between DMN and other task-positive networks is associated with greater attention after TBI
A study with a moderately high-quality assessment rating found that in 11 patients with chronic mild to severe TBI, greater connectivity between left/right inferior parietal lobule (IPL) and several regions in the DMN, DAN, ECN, SN, and language network (ROI approach) was moderately to strongly correlated with executive and spatial attention after an attention program, and the opposite trend was seen for anticorrelated connectivity between these areas after the program (Lindsey et al., 2022).
In a moderately high-quality study of 38 adults with chronic mTBI, lower resting alpha band connectivity between left middle temporal gyrus (MTG)/left supramarginal gyrus or left MTG/left angular gyrus (ROI approach) was moderately to strongly associated with lower attentional inhibition, likely reflecting VAN involvement (Liu et al., 2021).
Lower structural connectivity within ECN is associated with lower attention after stroke
In a high-quality study of 49 adults with chronic left or right hemisphere ischemic stroke (basal ganglia and neighboring regions), lower FA between thalamus/prefrontal cortex or caudate/prefrontal cortex (ECN; voxel-wise approach) was strongly associated with lower executive attention (Liu et al., 2018). However, lower FA between thalamus/caudate (ECN), or specifically in left or right brain damage patients alone were not significantly associated with executive attention (Liu et al., 2018).
Similarly, in a high-quality study of 52 children with chronic left or right ischemic stroke, Larsen et al. (2022) found greater mean and axial diffusivity (AD) in the anterior forceps (part of ECN; ROI approach) to be strongly associated with lower executive attention. In a moderate-quality study of 19 adults with subacute right hemisphere ischemic stroke, lower FA within supramarginal gyrus, occipital cortex or parietal areas, or between posterior parietal cortex (PPC)/superior parietal lobule (SPL) or PPC/inferior frontal gyrus (voxel-based approach) was moderately to strongly associated with lower spatial attention (Umarova et al., 2014).
Greater functional connectivity within the DAN is associated with greater attention after stroke
A moderate-quality study in 43 adults with subacute right hemisphere ischemic or hemorrhagic adult stroke (cortical, subcortical, cortico-subcortical, brainstem, cerebellum, cortical white-matter regions; ROI approach) found lower interhemispheric resting fc within the DAN to be strongly associated with lower spatial attention (Baldassarre et al., 2016). Similarly, in a moderately high-quality study of 86 adults with left or right ischemic subcortical stroke, greater resting fc within the left supplementary motor cortex (SMC) or between left SMC/right MFG (ECN, DAN, VAN, and motor network [MN]; voxel-based approach) was moderately to strongly associated with greater executive attention and inhibition (Diao et al., 2020).
In a moderately high-quality study using Granger Causality (Brovelli et al., 2004), greater resting interhemispheric integration in functional networks in 132 patients with right hemisphere stroke was strongly associated with greater spatial attention (Allegra et al., 2021). However, greater interhemispheric integration after subacute left hemisphere ischemic or hemorrhagic stroke was weakly associated with greater sustained attention and attentional shifting (Allegra et al., 2021).
Several other studies in this systematic review reported greater DAN connectivity to be associated with greater attention, although associations were only rated as low or moderate and, therefore, not discussed in the results text (refer to Table 6).
Influence of age
Traumatic brain injury
Due to the large-scale changes occurring in the attention networks during childhood to adulthood development, we considered the effect of age on the association between connectivity and attention. Of the 24 TBI studies included in this review, only 5 studies were conducted in childhood populations: 2 DTI studies (mean age 13.8 [SD 0.07] years) and 3 rs-fMRI studies (mean age 15.1 [SD 1.6] years) (Table 1). Structural connectivity trends in childhood populations differed from adult populations, whereas similar results were seen in functional connectivity.
The two studies examining structural connectivity in childhood populations used a graph theory approach. The overall trend across both studies was that decreases in structural system segregation were associated with greater attention. In a moderate-quality study of 11 children with mild-severe chronic TBI, Yuan et al. (2017) found lower mean local efficiency alongside greater normalized path length to be strongly associated with greater inhibition, executive attention, and sustained attention (after an attention program).
In a moderately high-quality study of 31 children with mild to moderate TBI, Cao et al. (2021b) found greater nodal local efficiency of the parahippocampal gyrus and transverse temporal gyrus (part of the ECN; ROI approach) to be moderately associated with lower executive attention.
Using fc analyses, in a moderately high-quality study of 40 children with mild to moderate chronic TBI, lower nodal efficiency in the left postcentral gyrus or lower nodal degree in the left IPL was associated with lower attention, using a task-fMRI ROI-based approach (Cao et al., 2021a). Paradoxically, Cao et al. (2021a) also found greater clustering coefficient in the right temporal area to be moderately to strongly associated with greater executive attention.
In a high-quality study of 17 children with mild to severe TBI, greater resting fc between left or right caudate and MN (ROI approach) was strongly associated with greater attentional inhibition (Stephens et al., 2017), and resting fc between the DMN and supramarginal gyrus was strongly associated with executive attention. However, in a high-quality study of 11 children with mild-moderate TBI, resting fc between the DMN and supramarginal gyrus (ROI approach) was not associated with executive attention and inhibition (Stephens et al., 2018).
Stroke
Two stroke studies included in this review recruited pediatric participants and showed similar trends to those found in adults. In a high-quality study of 52 children after left or right chronic ischemic stroke, lower executive attention was strongly associated with lower structural integrity in the anterior forceps (part of the ECN) using ROI-based tractography (Larsen et al., 2022). In a high-quality study of 20 children from a similar stroke population, thalamo-DMN and thalamo-ECN fc was strongly associated with inhibition and spatial attention using resting independent component analysis (ICA)-based functional connectivity (Steiner et al., 2022).
Influence of recovery stage
Traumatic brain injury
Four TBI studies recruited participants in the acute stage of injury (defined in this review as <7 days postinjury). Twenty-one studies recruited patients in the chronic phase of injury (>4 weeks postinjury). Two studies examined longitudinal changes in the association between connectivity and attention over time. In a moderate-quality study, Li et al. (2023) found that over time between 6–12 months after mild TBI (n = 109 in the acute stage, and n = 41 in the chronic stage), greater SN-ECN integration alongside reduced SN-DMN coupling (ICA-based approach) was strongly associated with lower executive and spatial attention (reflecting the chronic stage of recovery) (Li et al., 2023).
In a moderately high-quality study, Dall'Acqua et al. (2017) found that from acute to chronic adult mild TBI (n = 49), greater mean sc within a DMN-like subnetwork (NBS) was weakly correlated with greater divided attention, but not inhibition. The same study found that lower resting mean fc within this DMN-related functional subnetwork was moderately correlated with greater divided attention, but not inhibition (Dall'Acqua et al., 2017).
Stroke
In the included stroke studies, seven studies recruited patients in the subacute stage postinjury (defined as >7 days but <4 weeks postinjury). Eight studies recruited patients in the chronic phase of injury (defined as >4 weeks postinjury), and one study did not report the stage of recovery. Ramsey et al. (2016), Siegel et al. (2018), and Pirondini et al. (2022) investigated the relationship between changes in fc and changes in attention longitudinally from the acute to chronic phase (over ∼1 year).
In a low-quality study, from the subacute to chronic phase, greater interhemispheric DAN connectivity alongside lower DAN-DMN connectivity (ROI approach) was moderately to strongly associated with greater spatial attention in 77 patients with left or right hemisphere stroke (predominantly ischemic) (Ramsey et al., 2016). In a moderate-quality study of 107 participants with left or right hemisphere ischemic stroke in the subacute to chronic phase, greater resting modularity on the ipsilesional, but not contralesional stroke site was associated with greater spatial attention over time, where the strength of this correlation increased from moderate to strong. This study used a whole brain (graph theory) approach (Siegel et al., 2018).
In a moderate-quality study of 103 participants with acute to chronic left or right hemisphere adult ischemic stroke, greater network durations in a variety of networks, including the VAN, anterior and posterior DMN, salience and frontoparietal network, as well as visual, precuneus, cerebellar, and hippocampal areas over time (innovation-driven co-activation patterns [iCAP] approach) were weakly correlated with greater spatial attention over time between 1 week, 3 months, and 1 year postinjury (Pirondini et al., 2022).
Discussion
This review investigated the relationship between brain connectivity and attention in adults and children with ABI. We synthesized published literature reporting associations between structural or functional connectivity and attention after ABI, where all studies that met inclusion criteria recruited individuals with TBI or stroke. In these studies, the predominant neuroimaging modalities included DTI and fMRI, with fewer studies utilizing EEG or fNIRS. Sample sizes varied across studies (ranging between n = 11 and n = 173 participants) and a total of n = 974 participants with TBI and n = 1209 with stroke participated.
Nine studies (n = 7 TBI and n = 2 stroke) included children (n = 7 exclusively children, aged 6.6–18.9 years, 59.0% male). The mean age of adults was 45.8 (SD 12.8) years, 56.7% male. Many types of imaging and connectivity analysis techniques were used, where structural analyses involved quantification of FA, AD, MD, and tractography, and functional connectivity modalities included MRI, EEG, and fNIRS. Functional connectivity analyses included not only primarily voxel and ROI-based connectivity, but also NBS, graph theory, voxel-based morphometry, psychophysiological interaction, Granger causality, regional homogeneity, dynamic causal modeling, and iCAP analyses; the latter of which were almost exclusively used in studies published from 2020 onward.
Structural network disruption and attention in focal and diffuse injury models
Brain connectivity disruption in several structural networks was associated with poorer attention after TBI and stroke. After TBI, decreased attention was strongly associated with impaired global efficiency and connectivity between several large-scale task-positive networks (Caeyenberghs et al., 2014). In contrast, after stroke, changes in attention function were strongly associated with connectivity between smaller-scale brain regions primarily in the DAN.
Differences in injury mechanism impact the damage sustained to structural brain networks, resulting in differences in functional outcome. TBI results in diffuse large-scale network disruption (Sharp et al., 2014), whereas stroke is a focal injury causing dysfunction in the immediate region surrounding the insult, as well as in remote network regions (Carter et al., 2012). It is important to consider these differences in injury mechanism when relating structural changes to functional outcomes.
Structural white matter networks have been shown to act as a “scaffold” for functional network activity, where disruptions to white matter impact brain function. This concept, known as “structure-function coupling,” indicates the importance of considering structural and functional networks changes in tandem when assessing cognitive function (Baum et al., 2020). Overall, these results indicate that the type of disruption to network structure after TBI or stroke has a differing effect on attention function, and it is important to consider functional connectivity changes alongside structural connectivity changes.
DMN interference is associated with attention after TBI
Previous literature has repeatedly shown the relationship between the task-positive ECN and task-negative DMN to be impacted after TBI. In this systematic review, deceased structural integrity in several DMN regions (using ROI analyses) was moderately to strongly associated with lower sustained attention after TBI (Bonnelle et al., 2011; Zane et al., 2021), indicating the importance of intact DMN pathways for attention function. However, greater functional connectivity within the DMN during an attention task was associated with greater executive and spatial attention (Bonnelle et al., 2011; Sharp et al., 2011), contradicting the anticorrelated relationship of the DMN and ECN.
The key role of the ECN is to integrate sensory inputs to initiate and maintain cognitive control (Sharp et al., 2011). It comprises core structural regions such as the interhemispheric frontal, frontoparietal, and frontal-striatal connections (Ren et al., 2020), and core functional regions such as the bilateral dorsolateral prefrontal cortex (dlPFC), ventrolateral prefrontal cortex (PFC), dorsomedial PFC, dorsal caudate, and anterior thalamus (Seeley et al., 2007).
In contrast, the DMN is a task-negative network, active during periods of internal focus of attention (e.g., introspection and mind wandering) and relatively inactive during cognitive engagement (Raichle, 2015; Raichle et al., 2001). It comprises the posterior cingulate cortex, precuneus, medial prefrontal cortex, IPL and temporoparietal junction, where the delineation of structural and functional regions is less well understood (Raichle, 2015; Raichle et al., 2001).
In previous literature, a complex relationship has been identified between the DMN and task-positive networks after TBI. The ECN and DMN are anticorrelated in the healthy brain, where task-related activation of the ECN is accompanied by suppression of the DMN (Hellyer et al., 2014; Raichle et al., 2001). However, after TBI, a breakdown in segregation is seen between these networks, resulting in a loss of anticorrelation, termed “DMN interference” (Sharp et al., 2014), as seen in the results of this study.
Previous research has postulated that DMN interference during cognitive load, as well as loss of segregation between the task-negative DMN and task-positive networks, is thought to reflect network-wide compensation to support cognitive function in a less efficiently functioning network after injury (Sharp et al., 2014). As highlighted earlier, evidence for DMN interference was found in several studies in this systematic review (Bonnelle et al., 2011; Sharp et al., 2011). DMN interference was apparent as a loss of segregation between the resting DMN and task-positive networks, where greater connectivity between the DMN and task-positive networks was moderately to strongly associated with greater executive and spatial attention and inhibition (after an attention program) (Lindsey et al., 2022; Liu et al., 2021).
DAN connectivity is related to spatial attention after stroke
Greater DAN fc was strongly and repeatedly shown to relate to greater spatial attention after stroke (Baldassarre et al., 2016; Carter et al., 2010; Diao et al., 2020; Fellrath et al., 2016; Ramsey et al., 2016; Veldsman et al., 2017). The DAN is essential for modulating the top-down control of attention, where it encodes and maintains preparatory signals and coordinates sensory (e.g., visual, auditory, somatosensory, and olfactory) regions, and comprises the middle frontal gyri, intraparietal sulcus (IPS), SPL, and middle temporal gyri (Alves et al., 2022; Suo et al., 2021). The DAN works closely with the VAN, which comprises the central frontal cortex and temporoparietal junction, and coordinates the bottom-up control of spatial attention, that is, to detect new and unexpected stimuli in the visual field (Alves et al., 2022; Corbetta and Shulman, 2002; Corbetta et al., 2008).
In this systematic review, we focused on spatial attention as a deficit in stimulus detection or discrimination, as opposed to visuospatial neglect, where patients show visual neglect or omission of a partial or full visual field or side of the body (Ptak and Schnider, 2011). Here, we define spatial attention deficits as a higher-level attention deficit, arising from dysfunction in attention shifting systems such as the DAN and VAN (Corbetta et al., 2005; Ptak and Schnider, 2011). Where visuospatial neglect has been linked with damage to white matter structures such as the superior longitudinal fasciculus (Kim and Min, 2020), spatial attention deficits can arise from abnormal functional activation of structurally intact regions of the DAN and VAN (Corbetta et al., 2005). The IPS is thought to influence this relationship due to its central role in the convergence of low-level sensory and motivational inputs to create representations of environmental stimuli (Ptak and Schnider, 2011). Supporting this, several studies in this systematic review found a strong association between lower functional connectivity in the IPS and deficits in spatial attention (Baldassarre et al., 2016; Carter et al., 2010; He et al., 2007), or between DAN-related parietal areas more broadly and spatial attention (Umarova et al., 2014). Therefore, deficits in spatial attention may be linked to imbalances between the DAN and VAN, particularly involving structural and functional disruptions to the IPS.
Changes in brain connectivity and attention in childhood TBI and stroke
Distinct patterns of attention-related structural connectivity disruptions were found across pediatric and adult TBI populations. In pediatric TBI, decreases in structural network segregation (i.e., lower mean local efficiency and greater normalized path length) (Latora and Marchiori, 2001; Sporns and Betzel, 2016) were strongly associated with greater attention (Cao et al., 2021b; Yuan et al., 2017). This contrasted with adult TBI findings in this systematic review, where greater structural local network efficiency was strongly associated with greater attention (Caeyenberghs et al., 2014).
Brain network reorganization is dynamic across the lifespan, where large-scale changes are particularly apparent during childhood and early adolescence, as well as the later years of life (Bagarinao et al., 2019; Sherman et al., 2014). Childhood TBI is sustained during a period of considerable developmental change for global brain networks. During childhood, brain networks display lower segregation. As children mature, these structural networks differentiate and display increases in modular segregation (Gu et al., 2015), which has been shown to increase global efficiency and support the development of EF by increasing the efficiency of networks (Baum et al., 2017; Dennis et al., 2013).
Thus, decreased structural network segregation after childhood TBI may reflect disrupted network maturation. The fact that a decrease in structural segregation was seen alongside greater attention may relate to compensatory mechanisms across brain networks to facilitate greater attention function (Caeyenberghs et al., 2009; Gooijers et al., 2016; Meningher et al., 2020). Conversely, in this systematic review, a pediatric stroke study found that poorer structural integrity of the anterior forceps, a white matter tract that supports ECN functional activity, was strongly associated with lower executive attention (Larsen et al., 2022). This may indicate that compensatory changes in networks may be more present across global architecture, rather than disruption to localized tracts. This trend is similar to that seen in adult populations in this systematic review, where poorer white matter integrity was associated with lower attention in across several studies (Bonnelle et al., 2011; Ware et al., 2019; Zane et al., 2021). Therefore, global measures of structural connectivity, such as graph metrics, may provide more information about the interaction between brain injury and childhood development.
Unlike structural connectivity trends, attention-related functional connectivity in children after TBI or stroke was similar to trends seen in adult populations. In children with TBI, decreased nodal efficiency of the postcentral gyrus and IPL was moderately to strongly associated with lower attention, indicating that these regions displayed suboptimal communication with other attention network regions to facilitate attention (Cao et al., 2021a). The postcentral gyrus is part of the MN (Tomasi and Volkow, 2011), and is responsible for communicating tactile information during attention processing (Macaluso et al., 2000), whereas the IPL is important for frontoparietal integration of information during attention (Vincent et al., 2008), and may be part of the DMN (Numssen et al., 2021). A similar MN involvement was seen in another pediatric TBI study in this systematic review, where greater resting fc between the left or right caudate and MN was strongly associated with greater attentional inhibition (Stephens et al., 2017).
Similarly to adults, DMN fc was also related to attention in pediatric stroke, where connectivity between several regions of the thalamus and the DMN showed varying relationships with attention (Steiner et al., 2022). Therefore, attention-related functional DMN and motor connectivity in children after ABI showed similar trends to that seen in adults in this systematic review.
It is unclear why attention-related structural, but not functional, connectivity differed between adults and children after ABI. It is possible that a global connectivity analysis approach is needed to reveal differences in functional connectivity during development. Future long-term follow-up studies using graph theory to examine whole-brain architecture may reveal how changes in network connectivity and efficiency may affect long-term functioning. Understanding these changes may also elucidate an optimal therapeutic window during development (Pearn et al., 2017).
Changes in brain connectivity and attention across recovery phase of TBI and stroke
Recovery over time was associated with changes in attention-related functional connectivity. In particular, recovery from mild TBI was associated with normalization of DMN activity. Using a triple network interaction model, greater SN integration with the ECN alongside dissociation from the DMN between 6–12 months after injury was strongly associated with lower executive and spatial attention (Li et al., 2023). The SN is hypothesized to play a role in moderating the switch between the ECN (external focus of attention) and DMN (internal focus of attention) (Supekar et al., 2019).
In this study, more segregated cross-network interactions between the SN-ECN and SN-DMN systems was associated with poorer attention recovery after TBI. These results may reflect a loss of coupling between the SN and DMN, therefore, decreasing the ability of the SN to “switch off” the DMN during attention, and contributing to DMN interference.
Another longitudinal study included in this systematic review found that lower mean resting fc within a DMN-like subnetwork was moderately correlated with greater attention over the course of 1 year (acute to chronic TBI) (Dall'Acqua et al., 2017). Whereas this finding seems unexpected given that connectivity was measured at rest (when the DMN is most active), previous research has found that cognitive fatigue after sustained visual attention results in upregulation of the DMN. Therefore, reduced resting DMN activity alongside greater attention may indicate reduced cognitive fatigue as a result of general recovery from TBI (Dall'Acqua et al., 2017; Esposito et al., 2014). On the whole, long-term changes in brain networks during recovery from TBI are poorly characterized (Hillary et al., 2011). Further research should be conducted to investigate changes in brain connectivity in association with attention over time during TBI recovery.
Attention-related connectivity over time in stroke showed a similar trend to that in TBI. Over the course of 1 year, greater spatial attention during acute to chronic recovery from stroke was associated with greater functional network modularity, greater connectivity within the DAN, lower connectivity between DAN and DMN, and greater segregation between the DAN and DMN (Pirondini et al., 2022; Ramsey et al., 2016; Siegel et al., 2018). Increased modularity over time reflects functional reorganization of networks after injury, therefore, increasing efficiency of information transfer (Sporns and Betzel, 2016). Interestingly, the association between network modularity and spatial attention in this study was moderate in the subacute phase, but strong in the chronic phase, indicating ongoing changes in network organization (Siegel et al., 2018). Disruption in interhemispheric connectivity of the DAN has been postulated as a cause of spatial attention deficit and, therefore, this finding of greater interhemispheric DAN connectivity over time is in keeping with recovery of spatial attention (Ramsey et al., 2016). This recovery was further supported by findings of DMN normalization, where greater segregation (i.e., anticorrelation) between DAN and DMN was seen alongside attention improvement over time (Ramsey et al., 2016; Sharp et al., 2014).
Limitations
Our review systematically pooled all published literature reporting a correlation between structural or functional brain connectivity and attention tasks to provide insight into how brain connectivity may relate to ongoing cognitive deficits after ABI. This review was limited by the biased nature of published literature, where ROI-based analyses were commonly used, and in most cases, only significant correlations between attention and brain connectivity were reported. Therefore, results are biased toward predetermined brain regions or networks that displayed significant correlations with attention. Although this hypothesis-driven approach is encouraged for robustness and reproducibility in neuroimaging analyses (Song et al., 2016), it provides a biased perspective when compared with a voxel-based approach. Methods of brain connectivity analysis differed across included articles, where several different models were used to estimate structural and functional brain connectivity. The influence of these different analysis techniques on results has been discussed throughout this review. As previously discussed by Olsen et al. (2021) and Nichols et al. (2017), heterogeneity in neuroimaging pipelines and lack of openly accessible data contribute to a lack of replicability in neuroimaging data. This highlights the importance of using robust connectivity pipelines with openly accessible data.
In this review, it was also difficult to assess the impact of injury severity on attention-related connectivity, as the majority of included articles did not include individual patient clinical details. Finally, the numerical score given by the AXIS (Downes et al., 2016) quality assessment tool used in this review prevented traditional quality ratings (e.g., high, moderate, and low).
Clinical perspectives and future recommendations
Considering these limitations, key recommendations for future research are discussed. First, more thorough reporting of patient clinical details such as symptomatology and individual ABI characteristics (e.g., location of injury/infarct for stroke and injury mechanism for TBI) in clinical neuroimaging literature is recommended to allow for better characterization of heterogeneity in clinical populations. Second, we recommend the use of openly accessible data and standardized neuroimaging preprocessing and connectivity analysis pipelines to ensure more robust and reproducible neuroimaging outcomes (Olsen et al., 2021).
Third, assessment of attention after injury should be conducted using a standardized and validated test or battery of tests. As brain connectivity measures are observational in nature, in this review we could only determine a correlational, rather than causational, relationship between changes in connectivity and resulting changes in cognition. To explore causality, functional neuroimaging modalities should be combined with noninvasive brain stimulation to directly perturb brain networks associated with attention. Finally, online stimulation of key networks during attention tasks, recorded using neuroimaging tools, may elucidate important network-level activity and/or ABI-related changes implicated in attention.
This systematic review informs clinical management of ABI by contributing to understanding of the association between brain structure, brain function, and functional outcomes after injury. However, the use of brain connectivity to predict outcome at the point of care continues to be limited by factors such as lengthy and heterogenous data preprocessing and analysis procedures and cost of equipment (Van Diessen et al., 2015). The development of robust standardized brain connectivity analysis pipelines will help to bridge the gap between research and clinical utilization of brain connectivity.
Furthermore, compared with MRI as the standard measure of connectivity, the use of more portable inexpensive tools such as EEG and fNIRS may allow better integration in clinical settings. In this review, a small number of EEG and fNIRS studies found moderate to strong associations between attention and connectivity, indicating the clinical potential for these tools to be used as a prognostic measure, or to track recovery over time. In childhood ABI, this may help to inform a therapeutic window during development (Pearn et al., 2017).
Conclusions
This systematic review summarized published literature that reported a correlation between brain connectivity and attention in adults and children with ABI. We found that after TBI, greater attention was associated with greater structural global and local efficiency within and between the ECN, SN, and DMN; or greater fc between the DMN and other task-positive networks. After stroke, greater attention was associated with greater structural connectivity within the ECN or greater fc within the DAN. Structural connectivity differed across pediatric and adult populations, whereas fc trends were similar across the lifespan. Finally, after TBI, recovery of attention over time was associated with normalization of DMN activity, whereas after stroke, attention recovery was associated with greater network modularity, particularly in the DAN.
To further explore the relationship between brain connectivity and attention after ABI, future research should (1) ensure clear reporting of patient symptomatology; (2) make neuroimaging preprocessing and connectivity analysis pipelines standardized and openly accessible; (3) develop standardized attention assessments; and (4) combine neuroimaging with noninvasive brain stimulation to determine causal relationships between brain networks and attention across the lifespan.
Footnotes
Acknowledgments
We gratefully acknowledge the guidance of Paul Dux, Owen Lloyd, and Roslyn Boyd.
Authors' Contributions
Conceptualization, methodology, software, formal analysis, investigation (screening and data extraction), visualization, writing—original draft, writing—review and editing, and project administration by A.S. Conceptualization, methodology, investigation (screening and data extraction), and writing—review and editing by J.R.T. Investigation (screening and data extraction), validation, and writing—review and editing by J.M.H. Investigation (screening and data extraction), writing—original draft, and writing—review and editing by D.P.A. Writing—review and editing by K.K.I. Conceptualization, methodology, formal analysis, investigation (screening and data extraction), writing—review and editing, and supervision by K.M.B.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.