
Abstract
Introduction:
Improved understanding of multiple sclerosis (MS) symptomatology, disease mechanisms, and clinical effectiveness can be achieved by investigating microstructural damage. The aim was to gain deeper insights into changes in white matter (WM) tracts in MS patients.
Methods:
Diffusion magnetic resonance imaging-based tractography was utilized to segment WM tracts into regions of interest for further quantitative analysis. However, tractography is susceptible to false-positive findings, reducing its specificity and clinical feasibility. To address these limitations, the Convex Optimization Modeling for Microstructure Informed Tractography (COMMIT) technique was used. COMMIT was used to derive measures of intracellular compartment (IC) and isotropic compartments from multishell diffusion data of 40 healthy controls (HCs) and 40 MS patients.
Results:
The analysis revealed a widespread pattern of significantly decreased IC values in MS patients compared with HCs across 61,581 voxels (p FWE < 0.05, threshold-free cluster enhancement [TFCE] corrected). Similar WM structures studied using the fractional anisotropy (FA) value also showed a reduction in FA among MS patients compared with HCs across 57,304 voxels (p FWE < 0.05, TFCE corrected). Out of the 61,581 voxels exhibiting lower IC, a substantial overlap of 47,251 voxels (76.72%) also demonstrated lower FA in MS patients compared with HCs.
Discussion:
The data suggested that lower IC values contributed to the explanation of FA reductions. In addition, IC showed promising potential for evaluating microstructural abnormalities in WM in MS, potentially being more sensitive than the frequently used FA value.
Impact statement
In the last decade, numerous neuroimaging studies have shown that multiple sclerosis (MS) promotes changes in structural connectivity. Advanced techniques for identifying the origin and location of white matter (WM) abnormalities might result from integrating diffusion magnetic resonance imaging measures with connectivity-based evaluation and new image analysis methods. In this study, the Convex Optimization Modeling for Microstructure Informed Tractography (COMMIT) framework with the ball-and-sticks forward model was used to eliminate false-positive brain connections. Then we applied a whole-brain and regional tract-based spatial statistical analysis approach to test its potential in detecting microstructural alterations in isotropic compartment and intracellular compartment signal fraction maps produced from the COMMIT global fitting between healthy controls (HCs) and MS patients utilizing multishell diffusion data.
The analysis revealed a widespread pattern of significantly decreased IC values in MS patients compared with HCs. Similar WM structures studied using the fractional anisotropy value also showed a substantial trend toward statistical significance.
Introduction
Multiple sclerosis (MS) stands as the most prevalent nontraumatic impairment in young and middle-aged individuals (Cameron and Nilsagard, 2018). This chronic condition entails inflammation, demyelination, and neurodegeneration in the central nervous system (Bruck, 2005). The pathological features of MS include the dispersion of demyelinated plaques throughout this system (Ge et al., 2005). A more precise localization of white matter (WM) and an assessment of microstructural damage along specific tracts could greatly enhance our understanding of symptomatology, disease processes, and clinical efficacy (Lipp et al., 2020). Utilizing diffusion magnetic resonance imaging (MRI)-based tractography, WM tracts are divided into regions of interest (ROIs) for further quantitative investigation (Jeurissen et al., 2019).
Diffusion-derived metrics are crucial for identifying microstructural abnormalities. Complex fiber configurations can alter the interpretation of changes in diffusion metrics derived from tensors and make it difficult to model regions with complex and crossing fiber populations. These regions are found in 60–90% of the WM voxel (Vos et al., 2012). To overcome tensor model limitations, constrained spherical deconvolution (CSD) as a higher order diffusion model that is used to improve the accuracy of WM fiber orientation estimates in the presence of multiple fiber populations was developed (Jeurissen et al., 2014). This model uses high-angular diffusion-weighted imaging (HARDI) data, which allows for more detailed information about the diffusion properties of WM than traditional diffusion tensor imaging (DTI). These approaches allow for the resolution of multiple fiber orientations within a single voxel, enhancing the accuracy of fiber tractography (Jeurissen et al., 2014).
One challenge of probabilistic tractography algorithm is the high number of false-positive streamlines, and to improve the accuracy of the reconstructed whole-brain probabilistic tractography and filter implausible brain connections, the framework named Convex Optimization Modeling for Microstructure Informed Tractography (COMMIT) was used (Daducci et al., 2015). COMMIT is based on the ball-and-stick model, which involves assigning weights to individual streamlines to estimate their contributions to the signal. In accordance with the ball-and-stick model, the signal undergoes decomposition into intra-axonal, extra-axonal, and isotropic (ISO) compartments within every voxel (Alexander et al., 2010). This framework enhances tractography specificity without compromising sensitivity by integrating tractography with brain microstructural features. COMMIT facilitates the removal of inexplicable streamlines, thereby mitigating false-positive connections (Schiavi et al., 2019).
By using COMMIT, significant differences in neuronal density between MS patients and healthy controls (HCs) have been revealed, even in the presence of lesions, utilizing multishell data and the tractography algorithm (Jeurissen et al., 2014). This model estimates parameters for the intracellular compartment (IC) and ISO compartments (Stampfli et al., 2019).
Despite methodological progress, the implementation of COMMIT has been limited in some studies, including chronic adult cocaine users (Michels et al., 2022), individuals with schizophrenia (Stampfli et al., 2019), and prematurely born adults (Menegaux et al., 2020). In this study, we used the COMMIT framework, utilizing the ball-and-stick forward model to eliminate false-positive brain connections. Subsequently, a whole-brain and regional tract-based spatial statistics (TBSS) analysis was applied to assess the potential of ISO and IC signal fraction maps, derived from COMMIT global fitting, in detecting microstructural alterations between HCs and MS patients using multishell diffusion data.
Materials and Methods
Participants
Forty HCs were included in this study (mean age ± standard deviation [SD] = 36.25 ± 12.36 years; 8 males), as well as 40 patients with MS (mean age ± SD = 35.43 ± 9.29 years; 7 males). The clinical condition of the patients was assessed using the Expanded Disability Status Scale (EDSS) at the onset of the trial, and the diagnosis of MS was established based on McDonald's criteria (Thompson et al., 2018). Patients exhibiting relapses and stable neurological impairment between episodes were classified as having relapsing-remitting MS (Thompson et al., 2018). Individuals with severe neurological or neuropsychiatric conditions that could influence the brain structure were excluded from the patient group.
The exclusion criteria for patients also included organic brain disorders, history of head trauma resulting in unconsciousness lasting more than 5 min, MS patients displaying symptoms of depression or undergoing antidepressant treatment, and contraindications for an MRI. A general medical assessment checklist was administered to assess the health status of the control group (history of head trauma, seizures, and neuropsychological disorders). The subjects did not use any medications, alcohol, or other substances.
Image acquisition
Diffusion MRI data were collected on a 3T MRI scanner equipped with a 64-channel head and neck coil using a multishell DTI acquisition (SIEMENS Magnetom Prisma Fit Scanner) with the following parameters: 94 diffusion-encoding directions (b values: 700 [30 directions] and 2000 [64 directions] s/mm2; repetition time [TR]/echo time [TE]: 11,000/105 ms; flip-angle = 90°; field of view (FOV) = 256 × 256 mm2, matrix: 128 × 128 mm2; voxel size 2.0 × 2.0 mm) and 2 nondiffusion weighting (b = 0 s/mm2) images with opposing phase encode directions. Accelerated sagittal T1-weighted anatomical images were obtained using a 3D magnetization-prepared rapid acquisition gradient echo (MPRAGE) sequence with the following acquisition parameters: TR/TE = 2250/3.5 ms; acquisition flip angle = 7°, FOV = 256 × 256 mm2, matrix = 256 × 256 mm2; voxel size = 1 × 1 × 0.6 mm3; 225 contiguous sagittal slices providing complete brain coverage.
In addition, T2 fluid-attenuated inversion recovery (FLAIR) and 3D-FAST spin-echo techniques were used to acquire another image. These techniques, closely related to fast (turbo) spin-echo methods, offer a flexible and robust approach for 3D spin-echo-based imaging with wide clinical applications. Whole-brain coverage was obtained using an isotropic 3D image with voxel size = 0.9 × 0.9 × 0.9 mm3, TR/TE = 5000/225 ms, FOV = 256 × 256 mm2, matrix = 320 × 320 mm2, and 176 continuous sagittal slices.
Image processing
Lesion segmentation
The open-source Lesion Segmentation Tool (LST) version 3.0.0 (https://www.statistical-modeling.de/lst.html) for SPM12 was utilized for lesion segmentation. LST is designed to facilitate the segmentation of MS lesions (Schmidt and Wink, 2017). T2-hyperintense lesions were segmented using the FLAIR images' lesion prediction algorithm (LPA). This approach uses a binary classifier as a logistic regression model, which was trained on data from 53 MS patients with pronounced lesion patterns for the LPA. The model incorporated a lesion probability map utilized in the lesion growth algorithm and a spatial covariate accounting for voxel-specific variations in lesion probability. The parameters of this model were applied to segment lesions in new images by estimating the probability of each voxel containing a lesion. The default threshold value for lesion probability (0.65) was used. Lesion probability maps were generated and used to fill lesions in T1-hypointense MRI images.
Local information was utilized in the filling algorithm, eschewing global intensity distributions. This approach enabled accurate lesion filling even in images affected by field biases. Lesion filling on T1-weighted MRI images was performed before postprocessing to mitigate segmentation errors.
Processing of DTI data
We utilized dcm2nii to convert all images into NIFTI format, and then applied preprocessing steps using MRtrix3,* FSL, † and the Advanced Normalization Tool (ANTs ‡ ) (Avants et al., 2009) to prepare the diffusion MRI images. The preprocessing included the following: denoising the data using MRtrix3, correction of EPI distortions, motion and eddy-current distortions using FSL, and bias field correction using ANTs. A quality check was conducted on the diffusion data to assess the reliability. Slices with signal loss due to subject movement during diffusion encoding were identified and replaced using Gaussian process predictions. The b0 images were processed with dwi2mask (MRtrix3) to extract the brain region. We estimated response functions using dwi2response with the msmt 5tt algorithm (MRtrix3). The fiber orientation distribution (FOD) was computed using dwi2fod with the msmt CSD algorithm (MRtrix3). Whole-brain probabilistic tractography was performed through second-order integration over FOD.
To create a whole-brain tractogram using the anatomically constrained tractography algorithm, tissue classification for five different tissue types (cortical gray matter, subcortical gray matter, WM, cerebrospinal fluid [CSF], and pathological tissue) was generated from the anatomical data. Next, anatomical images were coregistered to averaged b0 using the FLIRT toolbox of FSL.
We adopted the spherical deconvolution informed filtering of the tractogram model for dynamic seeding of tractography points (tckgen seed-dynamic option in Mrtrix3). This strategy mitigated intrinsic tractography biases across the whole WM. Tractograms were filtered using the COMMIT method with bundle sparsity constraints. The ball-and-stick model was used for constructing signal fraction maps of the ISO and IC compartments using the COMMIT algorithm. This model assumes distinct components related to the local fiber structure within each voxel. The IC component can be considered sticks with water restrictions (purely anisotropic Gaussian motion). In contrast, the ISO are modeled as a purely (Gaussian) isotropic diffusion. Finally, the FSL software package's DTIFIT tool (Version 6.0.5; FMRIB, Oxford, United Kingdom) was utilized to calculate fractional anisotropy (FA) maps.
Voxel-wise statistical analysis using TBSS
We applied the TBSS method (Smith et al., 2006) using the PANDA pipeline toolbox (https://www.nitrc.org/projects/panda/) for voxel-wise statistical analysis. This process involved aligning the masked FA images for each subject, generating the mean FA map, extracting the FA skeleton, and projecting each subject's FA image onto the skeleton. We extended the same methods to create data on IC and ISO. Voxel-wise analysis was performed using the FSL Randomize tool (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/Randomise) with a general linear model (GLM), including a 5000-repetition permutation test to compare the MS and HC groups. The obtained p-value maps were family-wise error corrected (FWE) at the threshold-free cluster enhancement (TFCE) level of p < 0.05. The ICBM-DTI-81 WM atlas aided in identifying significant clusters within specific fiber tracts.
We also compared IC changes with FA alterations by calculating the Dice coefficient to measure overlap in significant areas. The Dice coefficient calculates agreement between any two sets. The Dice coefficient is determined if A and B are the two sets by the following:
No overlap is shown by a value of 0, whereas a value of 1 shows perfect agreement. We conducted voxel-wise correlation studies between IC and ISO metrics with EDSS, disease duration, age of disease onset, and lesion volume and number. Regarding the group comparison method, 5000 permutations were run, and covariates of no interest, including sex and age, were added. After applying TFCE and FWE correction, statistical significance was determined at p < 0.05. The nifti-snapshot tool (GitHub—pnlbwh/nifti-snapshot) was used to visualize all significant clusters.
ROI-wise statistical analysis
The selection of ROIs was based on the TBSS results, and an analysis of covariance (ANCOVA) was used to compare the diffusion measurements between the MS and HC groups, while accounting for age and sex as covariates. Multiple comparisons were addressed through Bonferroni correction. Furthermore, post hoc analyses were conducted to assess group differences. Correlations between clinical variables and intergroup ROI-based data were evaluated using age and sex as covariates (p = 0.05).
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistics (version 23.0; IBM, Armonk, NY). Differences in sex were tested using chi-squared tests, and two-sample t-tests were conducted for age.
Results
Demographic findings
Table 1 presents the demographic and clinical characteristics of MS patients and HC groups. There were no significant differences in age and sex between MS patients and controls.
Demographic and Clinical Variables According to Multiple Sclerosis Group
The conducted statistical tests were chi-squared tests of independence for sex and handedness; unpaired two-tailed t-tests for age.
EDSS, Expanded Disability Status Scale; HC, healthy control; MS, multiple sclerosis.
Voxel-based analysis of intracellular and isotropic maps
As depicted in Figure 1A, our analysis revealed a widespread reduction in FA among MS patients compared with HCs across 57,304 voxels (p FWE < 0.05, TFCE corrected). These differences in FA were observed across regions such as the genu, body, and splenium of the corpus callosum, bilateral internal capsule (anterior and posterior portions), bilateral corona radiata (anterior, posterior, and superior segments), as well as the bilateral longitudinal fasciculus (inferior and superior segments). As shown in Figure 1B, a significant decrease in IC was observed in MS patients compared with HC subjects across 61,581 voxels (p FWE < 0.05, TFCE corrected), while controlling for sex and age. Lower IC values (Fig. 1B) were particularly prominent in the genu, body, and splenium of the corpus callosum, left inferior fronto-occipital fasciculus, bilateral internal capsule (anterior and posterior parts), bilateral corona radiata (anterior, superior, and posterior parts), bilateral longitudinal fasciculus (inferior and superior parts), and fornix.

Voxel-wise TBSS analysis results of images among the MS and HC groups with a significant t-test statistical difference (p < 0.05, TFCE-based FWE corrected).
Conversely, higher ISO values (Fig. 1D) were primarily observed in the splenium of the corpus callosum, right corona radiata (superior and posterior parts), and right superior longitudinal fasciculus.
Overlapping lower IC with lower FA in MS
To gain a deeper understanding of the observed lower IC in MS patients and its relation to typical FA changes, we conducted a comparative analysis between group differences in IC and FA. Upon comparing the IC and FA group difference maps, a noteworthy observation emerged. Out of the 61,581 voxels exhibiting lower IC, a substantial overlap of 47,251 voxels (76.72%) also demonstrated lower FA in MS patients compared with HCs (Fig. 1C). This overlap primarily manifested in the body, genu, and splenium part of the corpus callosum, bilateral corona radiata (anterior, posterior, superior parts), bilateral internal capsule (anterior and posterior parts), and bilateral longitudinal fasciculus (inferior and superior parts) (Table 2).
Significant Clusters for Intracellular Compartment and Isotropic Compartment with Family-Wise Error Corrected <0.05
Brain location where clusters of significant differences between groups were found. All results are shown for p < 0.05 (FWE corrected). Percent columns indicate the percent volume of the cluster inside the corresponding area. Only clusters with lower IC in MS patients than HCs were observed.
FA, fractional anisotropy; FWE, family-wise error corrected; ISO, isotropic compartment; IC, intracellular compartment.
ROI analysis
We segmented the whole brain's IC skeleton using the “JHU White-Matter Tractography Atlas” WM partition map, and selected 17 fiber bundles as ROIs due to their significant differences in TBSS voxel-level analyses. Both the TBSS voxel-level analysis results and the post hoc Bonferroni-corrected ROI analyses consistently demonstrated significant alterations in FA, IC, and ISO values (p < 0.05). Within the ROI analysis, the right anterior and posterior limb internal capsules, as well as the bilateral posterior corona radiata, did not exhibit any changes related to FA (Table 3). The ISO evaluation further revealed a substantial portion of fibers with significant between-group differences.
Region-of-Interest Level Analysis Fractional Anisotropy, Intracellular Compartment, and Isotropic Compartment Results of White Matter Skeleton Partition
Indicates statistical significance (p < 0.05, Bonferroni-corrected).
Altered IC and its association with clinical variables
Figure 2 illustrates the correlation between IC and clinical variables, specifically lesion volume and disease duration, using a voxel-based Spearman's correlation approach. We identified critical clusters correlating with lesion volume, including portions of the genu of the corpus callosum, bilateral internal capsule (anterior and posterior segments), the left corona radiata (anterior, posterior, and superior segments), the left superior longitudinal fasciculus, and the left fronto-occipital fasciculus. Similarly, clusters correlated with disease duration covered parts of the splenium of the corpus callosum, the left posterior superior of the corona radiata, the left longitudinal fasciculus (inferior and superior segments), as well as the left inferior fronto-occipital fasciculus. There was no correlation between the ISO metric and the clinical variables.
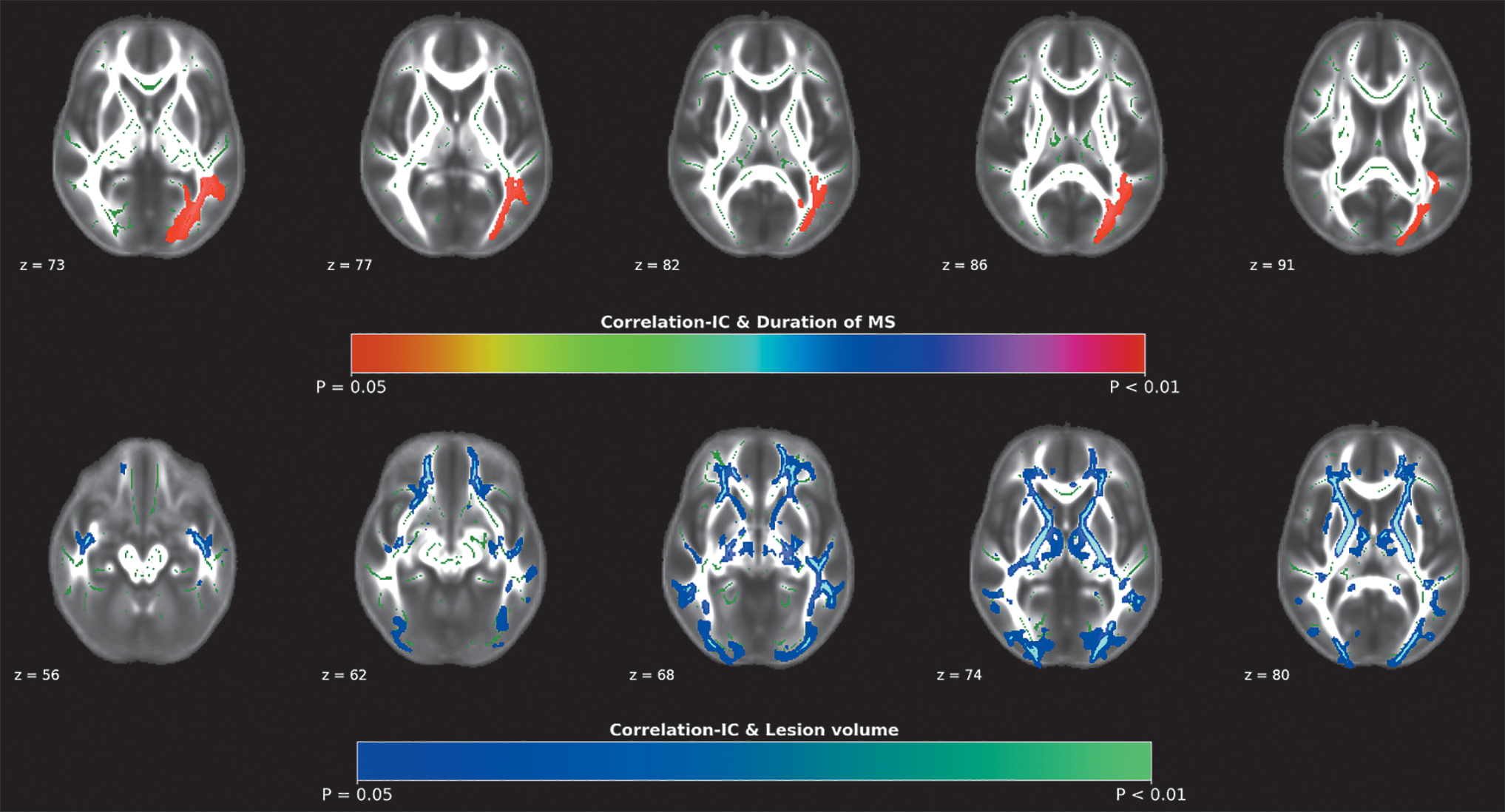
Significant voxel-wise spearman correlations were found between IC and lesion volume and disease duration in MS patients.
Within the 17 WM fiber bundles, we investigated the correlation between the mean value of the diffusion metrics and clinical variables. The results revealed no significant correlation between the diffusion metrics of any fiber bundles and clinical variables, except for the IC value of the right posterior corona radiata and the EDSS score (p = 0.04, r = −0.0325).
Discussion
Advanced techniques for identifying the origin and location of WM abnormalities may emerge through the integration of diffusion MRI measures with connectivity-based assessments and novel image analysis methods. The tractography approach used in this study, utilizing COMMIT filtering, indicated microstructural alterations in WM associated with MS. By comparing the restricted and ISO using the ball-and-stick diffusion model in both HCs and MS, we observed an increase in the ISO and a decrease in the restricted compartment in MS. Diffusion measurements derived from MRI may be sensitive to alterations associated with MS. Increased MD and decreased FA consistently characterize MS-related changes.
Conventional tractography methods are susceptible to producing false-positive connections that do not correspond to real anatomical pathways, thereby reducing the specificity of the estimated brain networks. Studies have demonstrated that the presence of false-positive connections in reconstructions can substantially impact the accuracy of tractography in mapping the brain connectome (Drakesmith et al., 2015; Maier-Hein et al., 2017; Zalesky et al., 2016). To overcome these limitations, robust diffusion analysis frameworks, including COMMIT, have been developed. The COMMIT framework enhances probabilistic FOD-based tractography by incorporating anatomically and microstructurally informed filtering. Notably, this framework enhances the specificity of estimated brain networks without compromising their sensitivity (Obaid et al., 2021). The COMMIT approach utilizes a forward model rooted in biological motivation and the measured diffusion signal to optimize weight for each streamline. The IC volume is derived by multiplying the contribution of each streamline (fiber weight) with the streamline length (Sommer et al., 2017).
The restricted compartment, known as IC or fiber density (FD), has been a subject of numerous theories based on diffusion-weighted imaging (Calamante et al., 2015; Raffelt et al., 2012). Notably, voxels derived from the COMMIT model with lower FD values exhibited overlap with those showing lower FA, indicating its potential as a reliable predictor of WM microstructure (Menegaux et al., 2020; Stampfli et al., 2019). Previous studies utilizing fixel-based analyses indicated reduced FD in MS patients (Carandini et al., 2021; Gajamange et al., 2018). Compared with HC, our findings indicated a reduction in IC among MS patients. The alterations notably distributed across the brain, particularly evident in tracts such as the inferior fronto-occipital fasciculus, internal capsule, corona radiata, and longitudinal fasciculus. These results align with prior research using different diffusion metrics (Gharaylou et al., 2021; Hagiwara et al., 2019).
We also examined changes in FA to support our findings of reduced IC. We noted a noteworthy reduction in FA within tracts that corresponded with the decreased IC. Although the majority of tracts exhibiting lower IC also displayed decreased FA, there were instances where lower IC was observed without alterations in FA. Differences in the angle or ratio of crossing fibers in these voxels might offer a plausible explanation. Moreover, our study revealed that the IC pattern varied based on tissue type, suggesting increased sensitivity compared with FA. Notably, areas in early MS patients exhibited lower FD compared with HCs (Gajamange et al., 2018). Unlike FA, which struggles with evaluating voxels containing crossing fibers, IC benefits from enhanced tractography algorithms and advancements in higher order diffusion models, making it a reliable assessment tool for voxels with crossing fibers.
In addition, we revealed an association between lower IC, lesion volume, and disease duration within specific tracts characterized by lower FA. Moreover, correlations were identified between FA and clinical variables such as EDSS scores, disease durations, and WM lesion loads in similar WM tracts (Liu et al., 2012). Previous in vivo studies using tractography in MS patients showed changes in diffusion measures across fibers affected by MS lesions, indicating that these changes extend beyond the effects of a single lesion (Kolasinski et al., 2012). Supporting this, postmortem histology and MRI studies demonstrated that focal MS lesions could trigger diffuse WM damage. This WM abnormality correlated with histological assessments of myelin integrity (Droby et al., 2015; Rocca et al., 2013). Our findings complement the growing body of evidence that the focal inflammatory MS plaque impacts more distant networks than anticipated.
In contrast to previous studies that often relied on applying a single shell to optimize the intracellular compartment percentage in diffusion data, our investigation used multishell diffusion data. This approach revealed an association between mild cognitive impairment and lower IC alongside higher ISO values (Obaid et al., 2021). The multishell strategy facilitated precise differentiation of various ISO characterized by different diffusion coefficients, including gray matter and CSF.
Considering MS within the context of histological, genetic, immunochemical, and imaging findings, there emerge two potential pathologies: axonal degeneration and neuroinflammation (Bjelobaba et al., 2017; Di Bari et al., 2017). In chronic neuroinflammation, the surrounding tissue is secondarily impacted by cellular damage. A critical element in MS etiology is inflammation initiated by an initial lesion, affecting oligodendrocytes, myelin sheaths, and ultimately axons and neurons (Weiner and Selkoe, 2002). Neuroinflammation is projected to influence the interstitial intraneuronal space, leading to increased isotropic diffusion of extracellular water (Schwartz et al., 2006). An increase in ISO could potentially identify subvoxel neurodegeneration, which shows the proportion of the diffusion signal also explained by tissue with isotropic diffusion.
Our data predominantly highlighted higher ISO values in regions such as the splenium of the corpus callosum, corona radiata (superior and posterior parts), and superior longitudinal fasciculus. Notably, this increase aligns with studies using neurite orientation dispersion and density imaging (NODDI) analysis for MS patients with normal-appearing WM (Hagiwara et al., 2019).
Conclusions
This study found substantial variations in WM microstructural integrity between MS patients and HCs, using IC and ISO measurements. Locally, decreases in the intracellular compartment were observed across WM tracts in MS, indicating reduced WM integrity. Conversely, increased intracellular compartment fractions suggest neurodegeneration, which also manifests in MS. Future research should explore diverse approaches in the context of neurodegeneration, with validation remaining crucial for a conclusive interpretation of these findings. Each method carries distinct benefits and drawbacks.
Confirmation Statement
All authors confirm that the research is supported by Kermanshah University of Medical Sciences that is primarily involved in education or research.
Footnotes
Acknowledgments
The authors gratefully appreciate the volunteers for participating in this study.
Data Availability
The data sets used during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The Ethics Committee of Iran University of Medical Sciences reviewed and approved the study protocol (![]() ). The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
). The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Authors' Contributions
Z.G. and M.R. contributed to the study design, method definition, data analysis, statistics, and article writing. F.S. contributed to data interpretation and article writing and editing. M.K. contributed to the study design and article editing. F.A. recruited the subjects. P.K. contributed to the study design and recruitment, and supervised the study and article editing. All authors contributed to the article and approved the submitted version.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.