
Abstract
Purpose:
This study investigated the association between psychological resilience and resting-state network functional connectivity of three major brain networks in pediatric concussion.
Methods:
This was a substudy of a randomized controlled trial, recruiting children with concussion and orthopedic injury. Participants completed the Connor–Davidson Resilience 10 Scale and underwent magnetic resonance imaging at 72 h and 4-weeks postinjury. We explored associations between resilience and connectivity with the default mode network (DMN), central executive network (CEN), and salience network (SN) at both timepoints and also any change that occurred over time. We also explored associations between resilience and connectivity within each network.
Results:
A total of 67 children with a concussion (median age = 12.87 [IQR: 11.79–14.36]; 46% female) and 30 with orthopedic injury (median age = 12.27 [IQR: 11.19–13.94]; 40% female) were included. Seed-to-voxel analyses detected a positive correlation between 72-h resilience and CEN connectivity in the concussion group. Group moderated associations between resilience and SN connectivity at 72 h, as well as resilience and DMN connectivity over time. Regions-of-interest analyses identified group as a moderator of longitudinal resilience and within-DMN connectivity.
Conclusions:
These results suggest that neural recovery from concussion could be reliant on resilience. Resilience was related to functional connectivity with three of the main networks in the brain that are often impacted by concussion. Improving resilience might be investigated as a modifiable variable in children as both a protective and restorative in the context of concussion.
Clinical Trial Registration Identifier: NCT05105802. PedCARE+MRI team (see Supplementary Appendix S1)
Impact Statement
This work contributes to recent evidence suggesting an association between psychological resilience and outcomes following pediatric concussion. Specifically, we identified several significant associations between resilience postconcussion and functional connectivity of major resting state networks in the brain. These results compliment findings reported in the literature that resilience is associated with postconcussion symptomatology, as well as quality of life. This study may serve to support future investigations of resilience-targeted interventions following pediatric concussion and its impact on neural and clinical outcomes.
Introduction
Concussion affects the well-being and quality of life of children (Novak et al., 2016). Children with concussion who are highly resilient, defined as one’s ability to adapt when faced with adversity (Connor and Davidson, 2003), are more likely to report decreased postconcussion symptoms than less resilient children in the chronic phase of injury (Bunt et al., 2021; Durish et al., 2018b; Hassan et al., 2023) and higher scores of quality of life (Durish et al., 2018a). Resilience has been associated with several neurofunctional networks (Iadipaolo et al., 2018, 2017), whereas the same networks have been found to be disrupted postconcussion (Abbas et al., 2015; Borich et al., 2015; Brett et al., 2022; Iyer et al., 2019; Johnson et al., 2012; Mayer et al., 2011; Meier et al., 2017; Newsome et al., 2016; Plourde et al., 2021; Sours et al., 2015, 2013). Limited evidence exists on whether resilience can be protective to the neurophysiological deficits of concussion.
Resilience reflects an individual’s accessible adaptive capacities for the successful coping of trauma or adversity that may otherwise threaten healthy functioning or development (Masten and Barnes, 2018). The most common functional networks associated with measures of resilience in children are the Default Mode Network (DMN; Iadipaolo et al., 2017, 2018), Central Executive Network (CEN; Iadipaolo et al., 2018), and Salience Network (SN; Iadipaolo et al., 2017). The DMN supports self-referential processes, emotional processing, and recollection of past experiences (Raichle, 2015). The CEN plays a role in executive functioning, sustained attention and working memory, response selection, and response suppression (Seeley et al., 2007). The SN is theorized to integrate, identify, and prioritize the most relevant incoming stimuli, as well as switching between activation of the DMN and CEN (Goulden et al., 2014; Seeley et al., 2007). Greater psychological resilience has been associated with decreased within-network DMN functional connectivity (FC) in healthy adults (Hemington et al., 2018). Within- and between-network FCs of the DMN and SN have also been reported as inversely associated with resilience (Altinok et al., 2021; Bolsinger et al., 2018; Hemington et al., 2018; Van der Werff et al., 2013). In healthy children and adolescents, decreased resilience has been associated with increased FC of the DMN to the anterior cingulate cortex, a key node of the SN (Iadipaolo et al., 2017). A negative correlation was also identified in children and adolescents between resilience and a dynamic state of FC between the DMN and CEN (Iadipaolo et al., 2018). Dynamic state describes discrete patterns of FC or time-varying patterns of resting-state FC. These reports indicate evidence of an inverse association between resilience and FC to the DMN, CEN, and SN in healthy individuals. However, the DMN, CEN, and SN FCs have been shown to be altered postconcussion (Abbas et al., 2015; Borich et al., 2015; Iyer et al., 2019; Johnson et al., 2012; Mayer et al., 2011; Meier et al., 2020; Newsome et al., 2016; Plourde et al., 2021; Sours et al., 2015, 2013; van der Horn et al., 2023).
Considering the empirical findings indicating that concussion alters neurofunctional networks associated with resilience, it remains unclear whether the functional correlates of resilience are altered postconcussion. As such, the functional correlates of resilience might be unique to pediatric concussion compared with children without brain injury. Children with orthopedic injuries serve as an appropriate comparison group, as they control over various nonspecific effects of traumatic injury (Wilde et al., 2018). An investigation of the neurofunctional correlates of resilience in pediatric concussion is vital for developing a clear comprehension of resilience’s impact on neural components of recovery following brain injury. The present study investigated cross-sectional and longitudinal associations between resilience and resting-state FC of DMN, SN, and CEN, and whether these associations were moderated by pediatric injury type (concussion or orthopedic injury). Given that resilience can be malleable (Connor and Davidson, 2003), we examined the associations between resilience and FC over time and at each timepoint separately. Secondary objectives were to investigate cross-sectional and longitudinal associations between resilience and patterns of within-network DMN, SN, and CEN FCs. In other words, we examined the association of resilience and clusters of connections between nodes belonging to each network, respectively, or within-network FC.
We hypothesized that changes in resilience are inversely associated with FC to each network within both groups and that these associations are moderated by pediatric injury type. We also hypothesized that resilience is inversely associated with patterns of within-network FC in both groups and that these associations are moderated by pediatric injury type.
Methods
Study design
This is a secondary analysis of a larger randomized clinical trial, Pediatric Concussion Assessment of Rest and Exertion (Ledoux et al., 2019), where a subsample of children with a concussion or orthopedic injury underwent an MRI scan at 72 h (±48 h) and 4-weeks (±5 days) postinjury (Ledoux et al., 2019). This study received approval by the Research Ethics Board and the Children’s Hospital of Eastern Ontario. All eligible children and adolescents capable of consenting on their own behalf provided written informed consent, whereas those unable to consent on their own behalf provided assent and parental consent.
Participants
Children with a concussion or an orthopedic injury (OI) were included in the study if they sustained a concussion or OI < 48 h from their emergency department visit, were 10 to 17.99 years of age, and proficient in English. Concussion participants were excluded from the study if they presented with a Glasgow Coma Scale score of ≤13, had abnormalities on standard imaging, underwent intubation, or had a history of trauma prior to the injury. Children with an orthopedic injury were excluded if their injury was isolated to the lower extremity or if they experienced a concussion within the past year.
Any participants from either group were excluded if they met any of the following criteria: communication difficulties as a result of severe chronic neurological developmental delay; history of neurological disorder; intellectual disability; intoxication at the emergency department or during the imaging session; required sedation at or prior to the emergency department visit; required surgical operation; history of hospitalization for psychiatric illness; incapable of resuming physical activity; incapable of providing consent or assent; absent legal guardian; unavailable for data collection at both timepoints; medical contraindications to the MRI scanner; and equipped with braces or metal implants.
Symptoms were assessed with the validated and reliable Health Behavior Inventory (HBI; Ayr et al., 2009), a 20-item, 4-point Likert self-report scale of symptomatology, with higher total scores indicating increased symptom severity. The validated and reliable Pediatric Quality of Life Inventory (PedsQL) version 4.0, a 23-item, 5-point Likert self-report scale, was used to assess quality of life. Each item is reverse scored and transformed to a linear 0–100 scale, with higher scores reflecting higher quality of life based on the past 7 days. The Connor–Davidson Resilience Scale 10 (CD-RISC 10) is a validated 10-item, 5-point Likert self-report scale of resilience with scores ranging from 0 through 40 (Campbell-Sills and Stein, 2007). The sum of every item on the scale is interpreted as the degree of psychological resilience in the past 30 days, with higher scores indicating increased resilience and lower scores indicating diminished resilience. These assessments and MRI scanning were recorded at 72 h and 4-weeks postinjury.
MRI acquisition
The fMRI acquisition used a 3-Tesla Siemens PET-MRI with a 12-channel head coil. A resting-state fMRI sequence was applied as part of the acquisition protocol. Participants were tasked with fixating on a crosshair and instructed to relax and try not to think of anything specific. The gradient-echo echoplanar pulse sequence parameters were as follows: resolution= 3.6 × 3.6 × 3.6 mm3, slices = 36, FOV= 23 × 23 cm2, TR = 2000 ms, TE = 30 ms, measurement total = 241. The duration of this sequence was 8 min and 10 sec. The high-resolution T1-weighted image acquisition parameters were as follows: TE = 2.21, 4.09, 5.97, and 7.85 ms; TR = 2300 ms; an inversion time of 1.16 s; an 8° flip angle; a slice thickness of 1 mm; a voxel size of 0.9 × 0.9 × 1 mm3; FOV = 230 mm; and a resolution of 230 × 230 × 176 mm. The duration of this sequence was 5 min and 52 sec. These sequences were identical for both scan sessions.
Statistical analyses
Between-group differences in age and resilience were tested using independent samples t-tests. Within-group differences in resilience at both timepoints were tested using paired samples t-tests. Group differences in both proportion of biological sex at birth and history of concussion were computed using a chi-square test. Pearson correlations were conducted to assess correlations between CD-RISC 10 scores and both HBI and PedsQL scores (Bonferroni corrected alpha value at α = 0.013). Outliers were defined as being 2.48 standard deviations from the mean (Cousineau and Chartier, 2010) and were Winsorized to the nearest score within their group. Two cases of 4-week resilience were missing from the concussion group and were imputed using expectation maximization (Dong and Peng, 2013).
Structural image quality checks were conducted based on guidelines proposed by Backhausen et al. (2016). The CONN toolbox, a Matlab-based software, was used for the preprocessing and both seed-to-voxel and ROI-to-ROI analyses of the resting-state data (Whitfield-Gabrieli & Nieto-Castanon, 2012). The default data preprocessing pipeline for volume-based analyses (direct normalization to MNI-space) was used for the data preprocessing, which includes functional realignment and unwarp; slice-timing correction; outlier detection; segmentation and normalization; and smoothing (Gaussian kernel of 8 mm). The CONN toolbox quality assurance plot was used to identify and exclude potential subject outliers based on automated measures of valid scans and average framewise displacement or motion (Morfini et al., 2023). The functional outlier detection threshold was set to 97th percentiles in normative samples. The default denoising pipeline, combining linear regression of confounding effects in blood-oxygen level dependent signal and temporal band-pass filtering, was used for denoising the data. Regarding temporal band-pass filtering, temporal frequencies below 0.008 Hz or above 0.09 Hz were removed. All region labels were based on the CONN toolbox default structural atlas derived from the Harvard-Oxford Cortical atlas (Desikan et al., 2006). The network seeds were based on CONN’s default clustering and ordering procedures applied to Cambridge 1000-connectomes resting state dataset.
A seed-to-voxel approach was used to analyze FC between DMN, SN, and CEN seeds and every voxel of the brain. The seed-based connectivity maps reflect FC between the specified seed and each voxel across the brain. The seed-based connectivity maps were based on the CONN toolbox provided seeds corresponding to the DMN, CEN, and SN. These networks were selected based on significant findings reported in literature pertaining to concussion (Abbas et al., 2015; Borich et al., 2015; Iyer et al., 2019; Johnson et al., 2012; Mayer et al., 2011; Meier et al., 2017; Plourde et al., 2021; Sours et al., 2015, 2013; van der Horn et al., 2023) and resilience (Altinok et al., 2021; Bolsinger et al., 2018; Goulden et al., 2014; Hemington et al., 2018; Iadipaolo et al., 2018, 2017; Seeley et al., 2007; Van der Werff et al., 2013). The DMN seeds included the following: the medial prefrontal cortex, the bilateral parietal cortex, and the posterior cingulate cortex. The CEN seeds included the bilateral prefrontal cortex, as well as the left and right posterior parietal cortex. The SN seeds included the anterior cingulate cortex, the bi-anterior insula, and the left and right rostral prefrontal cortex, as well as the left and right supramarginal gyrus. All significant clusters were defined following the CONN toolbox application of the Random Field Theory (Worsley et al., 1996), using a voxel height threshold of p < 0.001 uncorrected and a cluster height threshold of p < 0.05 corrected for false discovery rate (FDR). The corrected alpha value for analyses concerning seeds of the DMN was Bonferroni corrected at α = 0.013. The alpha value for analyses concerning the seeds of the CEN was corrected at α = 0.013. The alpha value for analyses concerning the seeds of the SN was corrected at α = 0.007.
Based on previous reports suggesting an inverse association between resilience and resting-state FC (Altinok et al., 2021; Bolsinger et al., 2018; Hemington et al., 2018; Iadipaolo et al., 2017; Van der Werff et al., 2013), we pursued a priori region-of-interest (ROI) analyses of within-network DMN, SN, and CEN FC. The ROI connectivity maps measure FC between predetermined pairs of ROIs. The ROIs selected for our analyses included each of the listed CONN toolbox provided DMN, SN, and CEN seeds. We used parametric multivariate statistics for cluster-based inferences. A series of t-statistics for all connections in a matrix of selected ROIs were computed. The selected ROIs were then sorted by a hierarchical clustering procedure based on the CONN toolbox default weight (0.05) for ROI-to-ROI anatomical proximity (1 = proximal) or functional similarity (0 = functional). Significant clusters were defined using a connection threshold of p < 0.05 uncorrected and a cluster threshold of p < 0.05 corrected for FDR among connections across all ROIs included in the analysis. A significant cluster is a similar pattern of FC within a set of connections between ROIs, irrespective of whether the association with individual connections is significant. The within-network analyses of DMN, SN, and CEN FC included only ROIs from their respective network.
Multiple regressions were used to examine interactions between resilience change scores, group, and timepoints when predicting FC (longitudinal). These three-way interactions were analyzed to explore how group moderates the associations between resilience change scores and changes in FC over time. Multiple regressions were also used to examine interactions between resilience and group at each timepoint separately when predicting FC (cross-sectional). Meaning, our regression models measured the associations between resilience and FC across time (from 72 h to 4 weeks) and at each timepoint (72 h and 4 weeks), and whether these associations were dependent on group. Resilience change scores were imported into the CONN toolbox as a second-level covariate, whereas the scans (72 h scans and 4-week scans) were entered as two contrasting conditions into the model. An interaction term between group and resilience change score was created using the CONN toolbox calculator and implemented to investigate whether there was an interaction between group and resilience change scores when predicting changes in FC. The multiple regression model for the longitudinal analyses is represented as follows:
The multiple regression model for cross-sectional analyses is represented similarly, but without the time-related terms:
Analyses using both groups included the following covariates entered jointly across groups: age, sex, handedness, and history of psychiatric illness. Within-group analyses of the concussion group included the following covariates: age (Alarcón et al., 2015; Zemek et al., 2016), sex (Alarcón et al., 2015; Zemek et al., 2016), handedness (Saenger et al., 2012), and history of psychiatric illness (Durish et al., 2018b; Hahn et al., 2011). Meanwhile, due to a smaller group size, within-group analyses of the orthopedic injury group included age and sex as covariates.
Results
Demographics
A total of 67/92 (73%) children with concussion (median age = 12.81 [IQR: 11.79–14.36]; 46% female) and 30/46 (65%) children with orthopedic injury (median age = 12.27 [IQR: 11.18–13.94]; 46% female) were included in this study (Fig. 1). All demographic and clinical data met assumptions for parametric testing, including normality and homogeneity of variance. Sports was identified as the main mechanism of injury for both the concussion (38/67 [57%]) and orthopedic injury (19/30 [63%]) group. There were no significant differences between groups with respect to age, sex, history of concussion, handedness, diagnostic history, 72 h resilience, 4-week resilience, and resilience change scores (Table 1 and Table 2). There were no significant differences between 72 h resilience and 4-week resilience scores within the concussion (t[66] = −1.58, p = 119) and orthopedic injury groups (t[29] = −0.527, p = 0.602).

Participant flow chart. Information regarding participant enrollment and attrition.
Demographic Data
IQR, Interquartile range.
Demographic Data Continued
ED, emergency department; HBI, Health Behavior Inventory; IQR, interquartile range; PedsQL, Pediatric Quality of Life Inventory.
The total emergency department self-reported HBI scores were significantly higher in the concussion group compared with the orthopedic injury group, t(95) = 3.80, p < 0.001. The total 72 h self-reported HBI scores were also significantly higher in the concussion group, t(95) = 5.62, p < 0.001. There was no significant difference in total 4-week HBI scores between groups. There were no significant correlations between HBI and resilience scores at either timepoint.
The total 72 h PedsQL scores were significantly higher in the concussion group compared with the orthopedic injury group, t(95) = 3.21, p = 0.002. There were no significant differences in total 4-week PedsQL scores between groups. The correlation between 72 h CD-RISC 10 scores and 72 h PedsQL scores group did not reach significance after correction for multiple comparisons within both the concussion (r[66] = 0.29, 95% CI: [0.054–0.5], p = 0.017; α = 0.013) and orthopedic injury groups (r[29] = 0.25, 95% CI: [−0.12 to 0.56], p = 0.180). A significant positive correlation was identified between 4 week CD-RISC 10 scores and 4 week PedsQL within the concussion group (r[66] = 0.33, 95% CI: [0.098–0.53], p = 0.006). This correlation did not reach significance within the orthopedic injury group after correction for multiple comparisons (r[29] = 0.37, 95% CI: [0.011–0.64], p = 0.042; α = 0.013).
Seed-to-Voxel analyses
Longitudinal resilience and FC
A significant three-way interaction (group × resilience × time) with the right lateral parietal cortex seed of the DMN was identified along the right cerebellum (cluster size = 237, MNI x y z = +02–72 −34, F[1 89] = 30.69, FDR corrected p = 0.012; Fig. 2). Group was a moderator of longitudinal resilience and DMN FC with the right cerebellum. Within this cluster, the concussion group showed a negative correlation between longitudinal resilience and FC (F[1 89] = 15.59, FDR corrected p = < 0.001, β = −0.003). Meanwhile, orthopedic injury group showed a positive correlation between longitudinal resilience and FC (F[1 89] = 29.41, FDR corrected p = < 0.001β = 0.033).

Group as a moderator between longitudinal resilience and FC. Sagittal slices displaying the significant cluster within the right cerebellum, color-coded by voxel statistic, indicating an interaction between group and changes in resilience when predicting changes in FC to the right lateral parietal cortex of the DMN. Associations between longitudinal resilience and connectivity values within this cluster differed significantly between groups, whereby the concussion group showed a negative correlation, whereas the orthopedic injury group showed a positive correlation. DMN, default-mode network.
Within the orthopedic injury group, longitudinal resilience was positively correlated with FC between the right lateral parietal cortex seed of the DMN and the right cerebellum (cluster size = 327, MNI x y z = +02–76 −28, F[1 26] = 39.92, FDR corrected p < 0.001, β = 0.033). Within the concussion group, no significant associations between longitudinal resilience and FC were detected.
Cross-sectional resilience and FC
A significant two-way interaction (group*resilience) with the left anterior insula seed of the SN was identified along the posterior division of the cingulate gyrus (cluster size = 407, MNI x y z = +02–30 + 28, F[1 89] = 19.33, FDR corrected p < 0.001; Fig. 3). Group was a moderator of 72 h resilience and SN FC with the posterior cingulate gyrus. Within this cluster, the concussion group showed a positive correlation between 72 h resilience and FC (F[1 89] = 9.69, FDR corrected p = < 0.001, β = 0.006). Meanwhile, orthopedic injury group showed a negative correlation between longitudinal resilience and FC (F[1 89] = 15.33, FDR corrected p = < 0.001, β = −0.019).
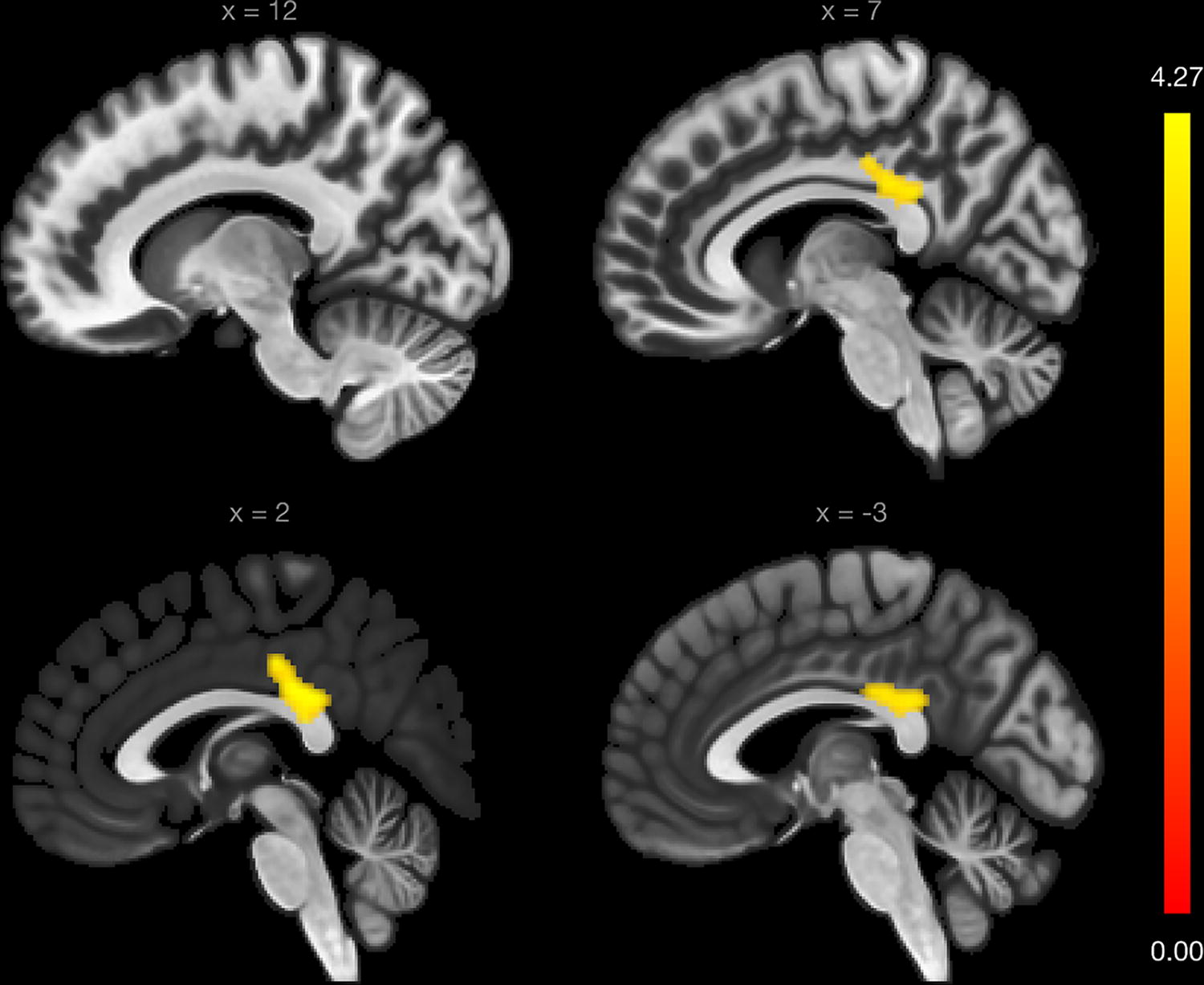
Group as a moderator between 72 h resilience and FC. Sagittal slices displaying the significant cluster within the posterior division of the cingulate gyrus, color-coded by voxel statistic, indicating an interaction between group and 72 h resilience when predicting 72 h FC to the left anterior insula of the SN. Associations between longitudinal resilience and connectivity values within this cluster differed significantly between groups, whereby the concussion group showed a positive correlation, whereas the orthopedic injury group showed a negative correlation. SN, salience network.
Within the concussion group, 72 h resilience was positively correlated with FC between the left lateral prefrontal cortex seed of the CEN and the left lateral occipital cortex (cluster size = 307, MNI x y z = −26–70 + 62, F[1, 61] = 29.92, FDR corrected p = 0.003, β = 0.015; Fig. 4).
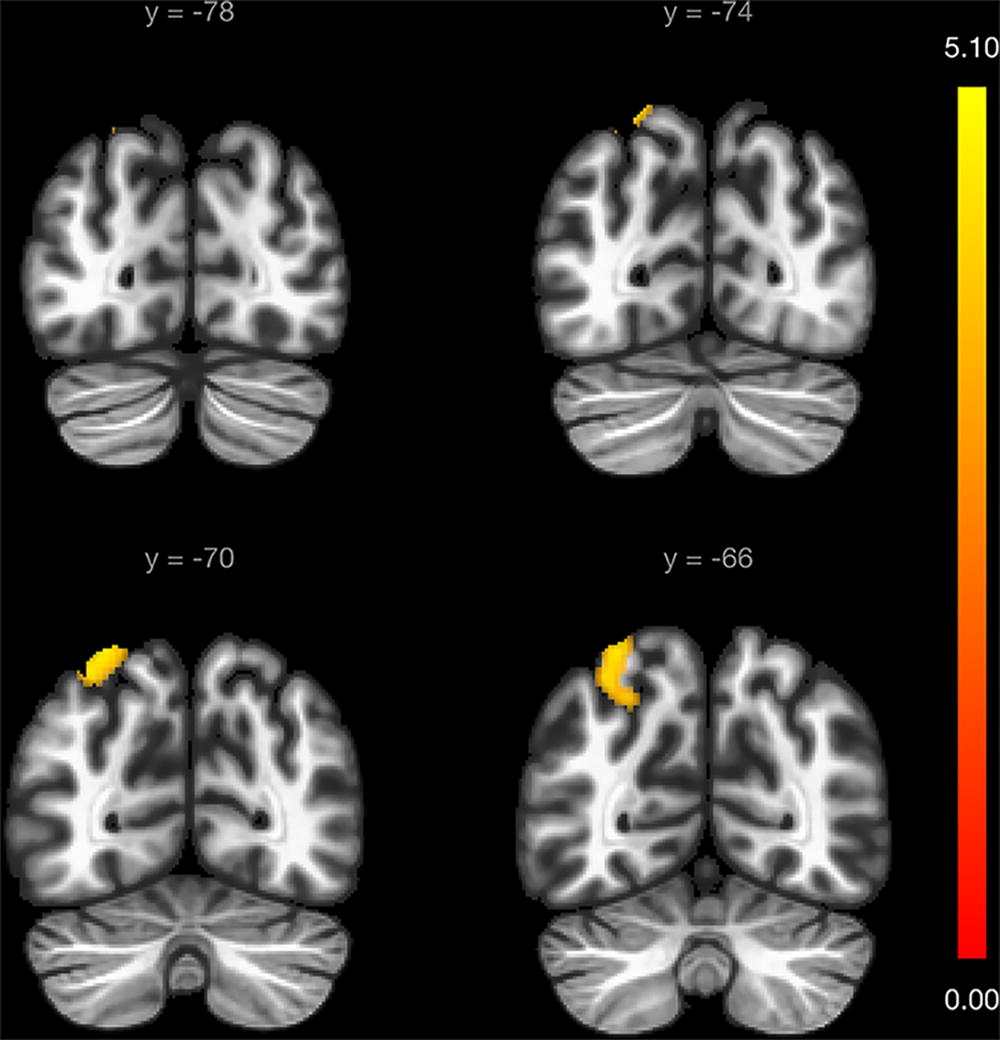
Associations between 72 h resilience and FC within concussion group. Coronal slices displaying the significant cluster within the left lateral occipital cortex, color-coded by voxel statistic, indicating a positive correlation between 72 h resilience and 72 h FC to the left lateral prefrontal cortex of the CEN. CEN, central executive network.
Within the orthopedic injury group, 72 h resilience was positively correlated with FC between the left anterior insula seed of the SN and the right superior parietal lobule (cluster size = 416, MNI x y z = +44 −38 + 54, F[1, 26] = 52.28, FDR corrected p < 0.001, β = 0.018; Fig. 5).

Associations between 72 h resilience and FC within orthopedic injury group. Coronal slices displaying the significant cluster within the right superior parietal lobule, color-coded by voxel statistic, indicating a positive correlation between 72 h resilience and 72 h FC to the left anterior insula of the SN. SN, salience network.
Seed-to-voxel analyses did not detect any significant interactions or associations between 4-week resilience and FC.
ROI-to-ROI analyses
Longitudinal resilience and FC
A significant three-way interaction (group*resilience*time) was identified among connections between DMN seeds (F[2, 88] = 4.56, p-FDR = 0.026; Fig. 6). Group was a moderator of longitudinal resilience and patterns of FC between DMN nodes. The interaction cluster included three ROIs and three connections among them. The first connection between bilateral lateral parietal cortices was a positive correlation in both the concussion group (β = 0.001) and the orthopedic injury group (β = 0.018). The second connection between the right lateral parietal cortex and posterior cingulate cortex was a negative correlation in both the concussion group (β = −0.002) and the orthopedic injury group (β = −0.021). The third connection between the left lateral parietal cortex with the posterior cingulate cortex was a positive correlation in the concussion group (β = 6.80E-05) and a negative correlation in the orthopedic injury group (β = −0.015).

Group as a moderator between longitudinal resilience and within-DMN FC. Ring plot demonstrating the connectivity differences between DMN seeds of the identified cluster, color-coded by connection statistic. The orthopedic injury group had an overall greater effect size relative to the concussion group, suggesting that injury type interacts with longitudinal resilience when predicting within-DMN connectivity. DMN, default-mode network.
Within the orthopedic injury group, longitudinal resilience was associated with longitudinal within-network DMN FC (F[2, 25] = 4.99, p-FDR = 0.030; Fig. 7). The significant cluster comprised of three ROIs and three connections among them: a positive correlation between the right and left lateral parietal cortex (β = 0.018); a negative correlation between the right lateral parietal cortex and posterior cingulate cortex (β = −0.021); as well as a negative correlation between the left lateral parietal cortex and the posterior cingulate cortex (β = −0.015). Within the concussion group, no significant associations between longitudinal resilience and within-network FC were detected.
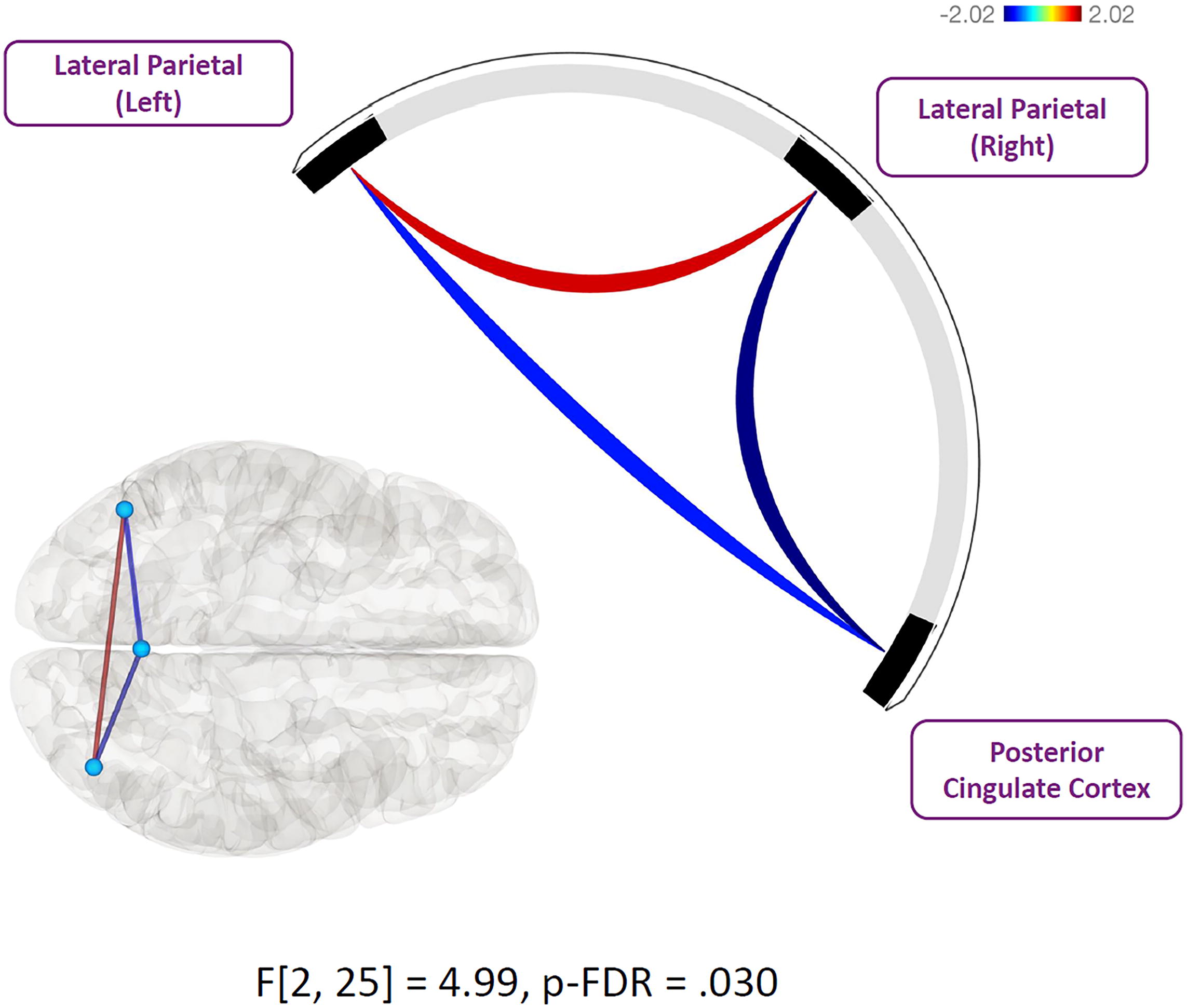
Orthopedic injury associations between longitudinal resilience and within-DMN FC. Ring plot demonstrating the associations between longitudinal resilience and within-DMN connectivity of the identified cluster, color-coded by connection statistic. The orthopedic injury group had a significant association between resilience and patterns of within-DMN cluster-based connectivity over time. DMN, default-mode network.
Cross-sectional resilience and FC
Within the orthopedic injury group, analyses of within-network SN FC identified one significant cluster (F[1, 26] = 8.98, p-FDR = 0.036; Fig. 8). The cluster included three ROIs and three connections among them as follows: a negative correlation between 72 h resilience and FC of the right anterior insula with the anterior cingulate cortex (β = −0.012); a negative correlation between 72 h resilience and FC of the left and right anterior insula (β = −0.016); and a negative correlation between 72 h resilience and FC of the left anterior insula with the anterior cingulate cortex (β = −0.015). No two-way interactions (group*resilience) were detected for within-network FC. Within the concussion group, analyses did not detect any significant associations between 72 h resilience and FC.

Orthopedic injury associations between 72 h resilience and within-SN FC. Ring plot demonstrating the associations between 72 h resilience and within-SN connectivity of the identified cluster, color-coded by connection statistic. The orthopedic injury group had a significant association between resilience and patterns of within-SN cluster-based connectivity at 72 h postinjury. In this study, all identified connections were negatively correlated with resilience scores. SN, salience network.
ROI-to-ROI analyses did not detect any significant interactions or associations between 4-week resilience and FC.
Discussion
Results showed that with higher resilience, there was greater FC with the CEN in children with acute concussion. Heightened resilience over time was related to decreased FC with the DMN in children with concussion, however was related to increased FC in children with orthopedic injury. Resilience over time was also related to differential patterns of within-DMN FC in children with concussion compared with children with orthopedic injury. In addition, highly resilient children had greater quality of life at 4-weeks postconcussion.
Results for our primary objective suggest that pediatric injury type moderates the associations between longitudinal resilience and DMN FC, that is, FC of the right lateral parietal cortex with the right cerebellum. Within the concussion group, there was a negative correlation between longitudinal resilience and FC within the identified cluster in the right cerebellum. Meanwhile, within the orthopedic injury group, there was a positive correlation between longitudinal resilience and FC within the same cluster. The lateral parietal cortex plays a role in various cognitive processes, including attention, working memory, spatial cognition, and social cognition (Cabeza et al., 2012; Desmurget et al., 2009; Humphreys and Lambon Ralph, 2015; Tumati et al., 2019). A recent fMRI study identified the cerebellum and corticocerebellar connections as being integral to episodic memory for emotionally arousing visual information (Fastenrath et al., 2022). Furthermore, this study found a significant positive correlation between longitudinal resilience and FC with the same regions within orthopedic-injured children. As longitudinal resilience did not differ between our samples of concussion and orthopedic injury children, perhaps the difference of associations between groups may be attributed to concussion-related changes to FC. Our secondary analyses indicate that associations between longitudinal resilience and within-DMN FC are also moderated by pediatric injury type. The association within the cluster of ROIs was stronger in the orthopedic injury group compared with the concussion group. Our results similarly found that such associations were significant in orthopedic-injured children. The effects of pediatric concussion might thus contribute toward a diminished association between longitudinal resilience and within-DMN FC.
Moreover, our primary analyses indicate that the associations between 72 h resilience and SN FC are moderated by pediatric injury type. This significant moderation was identified in FC between the left anterior insula of the SN and the posterior division of the cingulate gyrus, a node of the DMN. Within the concussion group, there was a positive correlation between 72 h resilience and FC within the identified cluster. In the orthopedic injury group, there was a negative correlation between 72 h resilience and FC within the same cluster. This finding of differential FC with the DMN is consistent with a recent study that reported an association between pediatric mild traumatic brain injury and decreased time spent in a default mode brain state with altered FC within midline cortical regions (van der Horn et al., 2023). In a study investigating whether damage to white matter tracts of the SN disrupts regulation of associated networks, structural connectivity within the SN was a significant predictor of DMN function (Bonnelle et al., 2012). Specifically, integrity of a tract connecting the right anterior insula to the presupplementary motor area and dorsal anterior cingulate cortex was correlated with abnormal posterior cingulate cortex activation in traumatic brain injury patients. The authors concluded that structural integrity of the SN is imperative for regulation of DMN activity. Pediatric concussion might diminish the association between resilience and SN FC to the DMN, contributing to a deregulation of DMN activity. This might, in turn, partially explain the discrepancy of significant DMN FC associations between our samples of children with concussion and orthopedic injury.
A significant positive correlation was reported between 72 h resilience and FC of the CEN, specifically the left lateral prefrontal cortex, with the left lateral occipital cortex in children with concussion. Interestingly, a recent study identified increased FC between the right lateral prefrontal cortex and right occipital pole in youth with concussion with resolved headache symptoms compared to youth with concussion showing persisting headache symptoms (Lemme et al., 2021). This recent study, however, did not incorporate a measure of resilience. It is possible that their sample of youth with concussion showing resolved headache symptoms had increased resilience relative to those showing persisting headache symptoms. This warrants further investigation into the associations between resilience and CEN FC in concussion. Meanwhile, in orthopedic-injured children, 72 h resilience was positively correlated with SN FC. Secondary analyses found that 72 h resilience was also significantly associated with within-SN FC in orthopedic-injured children. This is consistent with previous reports of negative correlations between resilience and within-SN FC in healthy populations (Altinok et al., 2021; Bolsinger et al., 2018). As suggested by Altinok et al. (2021), highly-resilient individuals might have decreased switching of the SN between networks responsible for processing self-relevant information. Highly-resilient individuals might thus maintain a reasonable emotional response to injury, allowing for an increased capacity to focus on their current mental state and successfully cope without interference from internal and external stressors. Unfortunately, these results were not identified in the concussion group, which might suggest that biomechanical injury to the head contributes to a disruption of this association otherwise identified in nonconcussed individuals. As such, only results from the orthopedic-injury group, as opposed to the concussion group, are largely consistent with the resilience literature using noninjured participants. Additional research is necessary to understand the effects of such associations on clinical symptoms postinjury in both orthopedic injury and concussion groups.
There were no significant results to report with respect to 4-week resilience and FC. Associations between resilience and resting-state FC might thus only be pertinent or detectable within the acute phase of injury. Research using noninjured pediatric samples reported various associations between resilience and resting-state FC of the SN with the DMN and CEN (Iadipaolo et al., 2018). Considering this, the underlying mechanism that may explain the progressive changes in associations between resilience and FC during pediatric concussion recovery remains unclear.
CD-RISC 10 scores were previously identified as being positively correlated with PedsQL in children with concussion in the chronic stage of injury (>4 weeks postinjury; Durish et al., 2018a). Our results are consistent with this finding and demonstrate an association between resilience and quality of life at 4-weeks postconcussion using identical metrics to Durish et al. (2018a). Although the association between resilience and quality of life at 72 h did not reach significance, this may be the result of diminished statistical power and differential report instructions in the acute phase of injury. The computed confidence intervals suggest that the association between resilience and quality of life at 72 h could potentially reach significance after multiple comparisons if statistical power were to be increased. Furthermore, the CD-RISC 10 instructs the participant to complete the report based on the past 30 days, whereas the PedsQL is based on the past 7 days. It remains a possibility that the acute injury event had a greater impact on quality of life scores than resilience scores at the time of reporting (72 h postinjury), consequently altering the association between the two metrics. These findings, along with the reported associations between resilience and functional connectivity, suggest that self-reported resilience may be implicated in both neural and functional outcomes following pediatric concussion. Conversely, our results suggest that resilience is not correlated with symptom burden at any timepoint, contradicting prior research reporting a significant association between resilience and postinjury symptom burden in the chronic phase of concussion (Hassan et al., 2023). Further research of resilience-targeted interventions is needed to assess the effects of such an intervention on the outcomes reported here.
Although this study provides insight as to the associations between resilience and DMN, CEN, and SN FC following pediatric concussion, the identified patterns in resting-state FC might be affected by our selection of spatial seeds in the seed-based correlations. It is known that subtle differences in selection of spatial seed voxel locations for seed-based correlation analyses of resting-state networks can have a significant effect on the variability of resulting associations in network FC (Buckner et al., 2008; Cole et al., 2010; Hayasaka and Laurienti, 2010). Future research of this sort should seek to apply similar spatial seeds as the ones selected for this study to replicate these findings. It is also important to note that this study applied the CONN toolbox default weight for the hierarchical clustering. Although the significant results reported here are based on a combined weighting of function and proximity, a different approach (e.g., modified weight to reflect only functional or only proximal clustering) may influence results. More research comparing the effects of prioritizing either clustering method is required to discuss its implications on cluster-based inferential analyses in this context. Furthermore, the analyses conducted in this study might be constrained by diminished statistical power. Although the sample size may be considered adequate for fMRI research, the complexity of our models (i.e., three-way interaction multiple regressions with the implementation of several covariates) may have limited the power of our statistical analyses. Future studies should seek to mitigate this potential limitation by increasing sample size and constricting the number of predictors and/or covariates of the statistical models.
Conclusions
Our results provide insight of the associations between resilience and FC in the subacute phase of pediatric concussion. Highly resilient children with concussion had heightened FC with the CEN at 72 h postinjury. We report several differences between our samples of children with orthopedic injury and concussion, whereby significant associations between resilience and FC were identified in the former but not the latter. Resilience was also associated with quality of life in the concussion group, whereby highly resilient children reported higher quality of life at 4-weeks postinjury. These findings indicate that resilience might play a role in both the functional neuroimaging results and quality of life following pediatric concussion and should be further examined to determine its potential usefulness in clinical settings as a protective or restorative element after injury. Additional investigations are warranted to determine the potential of resilience as a factor linked to optimal recovery from pediatric concussion.
Footnotes
Acknowledgment
The authors would like to acknowledge and thank the MRI technologists with the Brain Imaging Centre at the Royal Mental Health Centre in Ottawa, Ontario. This work was supported by the OSSU IMPACT Award; PSI Foundation Award; Canada Graduate Scholarships – Master’s (CGSM) competition.
Authors’ Contributions
Author contributors included conception and study design (O.B., A.S., R.Z., A.A.L.), data collection or acquisition (K.H., R.Z.), statistical analysis (O.B., Z.F., A.A.L.), interpretation of results (O.B., A.S., A.A.L.), drafting the article work (O.B., A.S., A.A.L.), and approval of final version to be published (all authors).
Preprint
An earlier draft of this article was posted as a preprint at Research Square (DOI: 10.21203/rs.3.rs-3143238/v1).
Compliance with Ethical Standards
This study received approval by the Research Ethics Board and the Children’s Hospital of Eastern Ontario. All eligible children and adolescents capable of consenting on their own behalf provided written informed consent, whereas those unable to consent on their own behalf provided assent and parental consent.
Author Disclosure Statement
R.Z. has received competitively-funded research grants from Canadian Institutes of Health Research (CIHR), Ontario Neurotrauma Foundation (ONF), Physician Services Incorporated (PSI) Foundation, CHEO Foundation, Ontario Brain Institute (OBI), Ontario SPOR Support Unit (OSSU), and the National Football League (NFL) Scientific Advisory Board, and he is supported by a Clinical Research Chair in Pediatric Concussion from University of Ottawa. He is the cofounder, Scientific Director, and a minority shareholder in 360 Concussion Care, an interdisciplinary concussion clinic. All other coauthors have no conflict of interest.
Data Availability Statement
The data cannot be shared due to legal, ethical, or privacy restrictions.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Appendix S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.