
Abstract
Introduction:
Essential tremor (ET) comprises motor and non-motor-related features, whereas the current neuro-pathogenetic basis is still insufficient to explain the etiologies of ET. Although cerebellum-associated circuits have been discovered, the large-scale cerebral network connectivity in ET remains unclear. This study aimed to characterize the ET in terms of functional connectivity as well as network. We hypothesized that the resting-state network (RSN) within cerebrum could be altered in patients with ET.
Methods:
Resting-state functional magnetic resonance imaging (fMRI) was used to evaluate the inter- and intra-network connectivity as well as the functional activity in ET and normal control. Correlation analysis was performed to explore the relationship between RSN metrics and tremor features.
Results:
Comparison of inter-network connectivity indicated a decreased connectivity between default mode network and ventral attention network in the ET group (p < 0.05). Differences in functional activity (assessed by amplitude of low-frequency fluctuation, ALFF) were found in several brain regions participating in various RSNs (p < 0.05). The ET group generally has higher degree centrality over normal control. Correlation analysis has revealed that tremor features are associated with inter-network connectivity (|r| = 0.135–0.506), ALFF (|r| = 0.313–0.766), and degree centrality (|r| = 0.523–0.710).
Conclusion:
Alterations in the cerebral network of ET were detected by using resting-state fMRI, demonstrating a potentially useful approach to explore the cerebral alterations in ET.
Impact Statement
This study explores the alteration of functional connectivity and characteristics of resting-state networks in patients with essential tremor (ET), specifically investigating our hypothesis that the network within cerebrum could be altered in patients with ET. The results demonstrate several differences between normal control and ET subjects, indicating that cerebral network of ET could be of importance in addition to the cerebellum. Such finding also shows the potential of resting-state functional magnetic resonance imaging in exploring the cerebral basis in ET.
Introduction
Essential tremor (ET) is a neurological disorder with a wide spectrum of clinical characteristics (Bhatia et al., 2018). In addition to motor-related symptoms such as involuntary and rhythmic shaking of hands, legs, and head, non-motor features had been mentioned in several studies including mild cognitive function deficit in memory and executive function (Benito-Leon et al., 2013, Chandran and Pal, 2012). The older adults with ET onset after 65 years of age were 70% more likely to exhibit dementia (Benito-Leon et al., 2006). The cerebello-thalamo-cortical circuit has been regarded of importance in the pathology of ET. The olivo-cerebellar model was first proposed in 1970s (Llinas and Volkind, 1973), and the cerebellar degeneration model emerged in these years (Louis and Faust, 2020). However, these models cannot fully explain the pathogenesis of ET. Environmental epidemiology of ET has been discussed (Louis, 2008). A recent study demonstrated that the synaptic pruning deficits of climbing fiber to Purkinje cell synapses caused by insufficiency in glutamate receptor delta 2 (GluRδ2) protein would lead to excessive cerebellar oscillations, which might be responsible for tremor (Pan et al., 2020). Although many efforts have been done on investigating ET in these decades, the origins and causes are not well recognized (Louis and Faust, 2020).
Neuroimaging modalities such as magnetic resonance imaging (MRI), positron emission tomography, and single-photon emission computed tomography have been used in studying ET (Holtbernd and Shah, 2021), offering robust noninvasive approaches in discovering the pathophysiology of ET. A variety of MRI techniques including diffusion MRI, functional MRI (fMRI), MR spectroscopy, and quantitative MRI have been used in investigating ET. Among these MR techniques, fMRI possesses a feasible approach in exploring the brain function of patients with tremor. Both of task-based fMRI and resting-state fMRI (rs-fMRI) have been used in investigating tremor. In task-based fMRI, it has been reported that involuntary tremor of patients with ET was related with significantly higher activation in the cerebellar hemispheres and the red nucleus (Bucher et al., 1997), and another study suggested that ET is associated with the dysfunction of cerebello-thalamo-cortical circuit (Nicoletti et al., 2015).
Different to task-based fMRI, rs-fMRI monitors the intrinsic neuronal activity in the brain under rest condition (Biswal et al., 1995). The functional connectivity (FC) can be evaluated by calculating the correlation of the time-varying signals in two spatially remote regions. Altered FC has been described in patients with ET comparing to healthy controls, particularly the increased connectivity in default mode network (DMN) and frontoparietal networks. The severity and duration of ET were also shown to be related with the network integrity (Benito-Leon et al., 2015). Graph theoretical analysis has been used to evaluate the functional network organization, indicating the disruption of the efficiency in brain functional networks (Benito-Leon et al., 2019). It has been suggested that the intrinsic functional activity, which characterized by the amplitude of low-frequency fluctuation (ALFF), reflects the abnormality in bilateral posterior lobe of the cerebellum of patients with ET (Wang et al., 2018).
As a movement disorder, tremor-related studies had focused on the abnormal function of cerebellum and cerebellar-associated circuits. As the possibility of cognitive change and psychological alterations in ET has been suggested (Chandran and Pal, 2012), we aimed to extend the scope from cerebellum to cerebrum and to explore tremor from network aspect. We hypothesized that the resting-state network (RSN) within the cerebrum could be altered in patients with ET. To our knowledge, although the intra-network and inter-network resting-state FC have been used in investigating Alzheimer’s disease (Brier et al., 2012) and Parkinson’s disease (Zeng et al., 2022), a limited number of studies have emphasized on the connectivity within and between various RSNs of tremor. A previous study has used group-independent component analyses to identify several RSNs, showing decreased FC between DMN, cerebellar network, and somatosensory cortex network (Fang et al., 2015).
In this study, we aimed to characterize the common RSNs with the cerebral hubs summarized by Power et al. (Power et al., 2011), providing a more comprehensive analysis on the network connectivity between normal control and patients with ET. The inter-network connectivity, intra-network connectivity, and intrinsic functional activity were evaluated to portray the network organization, together with its correlation to tremor features.
Materials and Methods
Participants
All participants gave their written informed consent, all procedures were performed in compliance with institutional guidelines and have been approved by local ethics committee (EC1090504-E). Initially, a total of 27 patients with ET were recruited in this cohort. Diagnosis of ET was based on the Consensus Statement on the classification of tremors (Bhatia et al., 2018). Assessment of tremor severity was based on the Washington Heights-Inwood Genetic Study of Essential Tremor (WHIGET) rating score by an experienced neurologist. In addition, all subjects have completed information of their disease history as well as the family history. All the patients were drug naïve at the time of MRI scan. In addition, the clinical neurological examination was conducted three times to fulfill the ET clinical features. The laboratory and physical examinations were inspected to exclude other medical conditions. Subjects with incomplete tremor test examinations were not included. Subjects with severe head motion during MRI scan were not included because of image artifact. A total of 17 patients with ET (10 females) fulfill all study criteria and 19 healthy volunteers (12 females) were analyzed. Demographics of the final eligible participants were summarized in Table 1. There was no significant difference in age (Mann–Whitney U test p = 0.06) and sex (Pearson Chi-square p = 0.79) between patients and normal controls.
Demographics of Participants
Mann–Whitney U test.
Chi-squared (χ2) test.
Magnetic resonance imaging
MRI datasets were acquired on a Philips Ingenia 1.5T system (Philips Healthcare, Best, the Netherlands) with a 20-channel head coil for signal receiving. T1-weighted image was acquired by 3-dimensional gradient echo scanning with the following parameters: field of view (FOV) = 25.6 cm × 25.6 cm × 16.5 cm, matrix size (MTX) = 400 × 400 × 150, repetition time (TR)/echo time (TE)/flip angle (FA) = 7.51 ms/3.49 ms/8°. Resting-state fMRI images were obtained by gradient echo echo-planar imaging in an interleaved manner with 26 transversal slices covering the brain. Scanning parameters were: FOV = 19.2 cm × 19.2 cm, MTX = 64 × 64, TR/TE/FA = 2.5 s/40 ms/90°. Each subject was asked to stay relaxed but keep awake with eye closed during rs-fMRI scanning. A total of 156 consecutive volumes were acquired in 6.5 min.
Data processing
All MRI images in DICOM format were pre-processed by using CONN toolbox version 19.c (www.nitrc.org/projects/conn) (Whitfield-Gabrieli and Nieto-Castanon, 2012). Standard pre-processing steps including realignment, slice-timing correction, outlier identification, direct segmentation, normalization to MNI space, and spatial smoothing (6-mm Gaussian kernel) were performed using the default setting in CONN. The first five and last five volumes of the rs-fMRI time series were discarded to avoid unsteady signals. After spatial processing, the nuisance signal components derived from white matter and CSF regions, estimated subject-motion parameters, and the outlier identified by CONN’s artifact detection tool were used as the temporal confounding factors and were removed separately using ordinary least squares regression. Linear detrend and despike were consequently performed, followed by a band-pass filter of 0.01–0.08 Hz. Finally, all of the denoised functional data were in MNI space and ready for network analysis.
Analysis of functional network
A functional network atlas with 264 regions of interest (ROIs) proposed by Power et al. (Power et al., 2011) was utilized in this study. Among these ROIs, regions engaged in the following 11 common functional networks were selected: sensory-motor network (SMN), cingulo-opercular task control network (COTC), auditory, DMN, memory retrieval (MEM), visual network (VIS), fronto-parietal task control network (FPTC), salience network (SAN), subcortical, ventral attention network (VAN), and dorsal attention network (DAN). A total of 232 spherical ROIs (10-mm diameter) were used to extract the rs-fMRI time courses and to evaluate the Pearson correlation coefficient matrix by using DPARSF toolbox (http://rfmri.org/DPARSF) (Yan and Zhang, 2010). The intra-network connectivity and inter-network connectivity were then calculated based on the Fisher’s z transformed correlation coefficient, as used in a previous study by Brier et al. (Brier et al., 2012). Specifically, the intra-network connectivity of network
For visualizing the 11 common RSNs, several sphere seeds in 12-mm diameter were used to generate the voxel-wise correlation maps. Seeding locations and its rationales were described in Supplementary Table S1. The seed-based correlation maps (in Fisher z) were averaged and subjected to one sample t-test against zero, where the voxels with |t| > 3.1 were shown on the map, as shown in Supplementary Figure S1. The seed-based correlation analysis was performed by using DPARSF toolbox.
Statistical assessment
Statistical assessment was performed using SPSS 12 (IBM, Armonk, New York). Analysis of covariance (ANCOVA) with age and sex as the covariates was used to detect the significance in network measurements. Mean value of age was compared using Mann–Whitney U test, and the difference in sex distribution was compared via Chi-squared (χ2) test.
Results
The selected 232 ROIs formed the averaged correlation matrices of normal control and tremor groups, as shown in Figure 1(a). The distinct squared blocks in the correlation matrix were the ROI pairs of RSNs. Difference between the two groups were depicted in Figure 1(b) by one-way ANCOVA with age and sex as covariates. Although several differences between ROI pairs were found (p < 0.001 uncorrected), there was no significance after considering multiple comparison (FDR corrected).
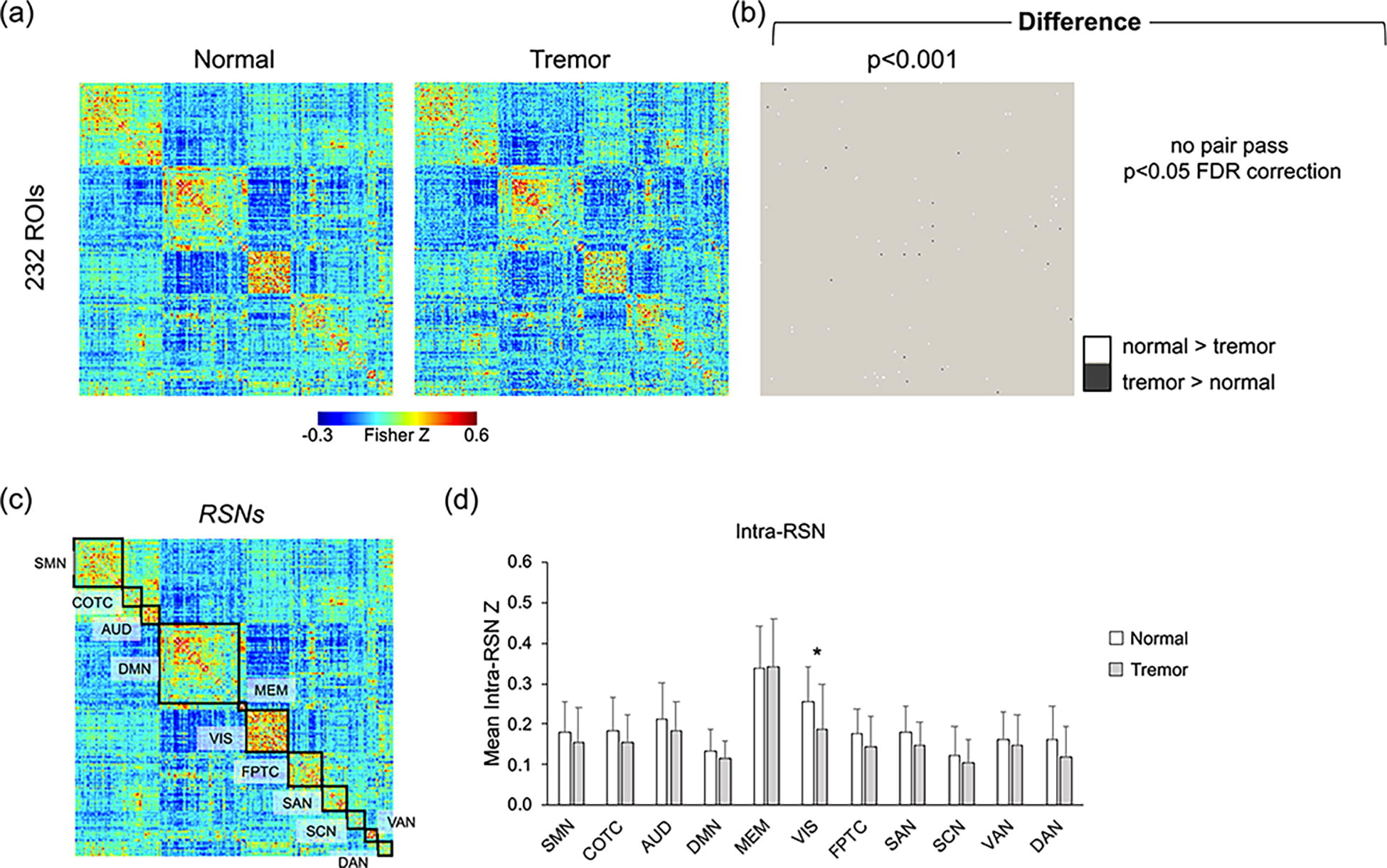
Comparison of the functional connectivity between normal and essential tremor groups.
The ROI-wise FC matrices were then merged into the 11 common RSNs to facilitate the analysis in network level. Figure 1(c) illustrates the RSN blocks, where the intra-network correlation pairs were averaged to generate the mean intra-RSN Z value, as shown in Figure 1(d). Generally, the intra-network connectivity in normal control group tends to be higher than that in the ET group. Significance can be found in VIS with a p value of 0.042 (student’s t-test). Nevertheless, there was no significance (p = 0.267) after controlling age and sex.
The inter-network connectivity among 11 RSNs was depicted in matrix, as shown in Figure 2(a). The ROI correlation pairs between each two RSNs were averaged to generate the inter-network connectivity values. Calculation details can be found in Methods. Specifically, decreased inter-network connectivity in AUD–FPTC, MEM–VAN, and DMN–VAN was found in the ET group comparing to normal control. The difference in DMN–VAN connectivity is significant after FDR correction.

Comparison of the inter-network connectivity.
Regional comparison of the ALFF and degree centrality between the two groups were also performed. Schematic labels are shown in Figure 3, indicating the difference between normal control and ET subjects. The ET group presented higher ALFF in regions, which are involved in DMN (left superior frontal gyrus, right superior temporal gyrus, and left parahippocampal gyrus), AUD, VIS (right fusiform gyrus), and COTC, and presented decreased ALFF in regions which are involved in DMN (left medial frontal gyrus, left fusiform gyrus, and left middle temporal gyrus), VIS (left cuneus and left middle occipital gyrus), DAN, and SAN. As to the degree of centrality, the tremor group generally has higher value over normal control. Complete list of the regions that show significant difference between normal and tremor groups can be found in Supplementary Table S2.

Illustration of the regions showing differences in ALFF and centrality. Anatomical regions corresponding to each RSN showing significant statistical differences in ALFF (left Fig.) and degree centrality (right Fig.) between normal control and ET groups. The between-group ALFF and degree centrality were compared by using one-way analysis of covariance with age and sex as the covariates. ALFF, amplitude of low-frequency fluctuation; ET, essential tremor; FusG, fusiform gyrus; IPL, inferior parietal lobe; LingualG, lingual gyrus; MedFG, medial frontal gyrus; MedTG, medial temporal gyrus; MidTG, middle temporal gyrus; MidOG, middle occipital gyrus; ParaCG, paracentral gyrus; ParaHip, parahippocampus; PreCG, precentral gyrus; PostCG, postcentral gyrus; ROI, region of interest; SFG, superior frontal gyrus; STG, superior temporal gyrus; SupraG, supramarginal gyrus.
In order to address the relationship between network characteristics and clinical assessment of tremor, a correlation analysis was conducted. Figure 4 shows the correlations with p value < 0.05. For the correlation with WHIGET score, statistical results are reported after controlling age, sex, and disease period. For the correlation with disease period, statistical results are reported after controlling age, sex, and WHIGET score. The mean ALFF within MEM network showed a negative correlation with WHIGET score (r = −0.601). Inter-RSN connectivity of MEM–DAN and DMN–SCN were negatively correlated with WHIGET score (r = −0.601 and −0.135, respectively). As to disease period, a negative correlation was found between period and the inter-RSN connectivity of DMN–SCN (r = −0.224). Intra-RSN connectivity showed no significant correlation to either WHIGET score or disease period. Besides, there was no significant correlation between WHIGET score and disease period (r = −0.032, p = 0.488; Supplementary Fig. S2). In addition to network-level analysis, the correlation between tremor rating and regional indices (ALFF and degree centrality) was also evaluated and tabulated in Supplementary Table S3.
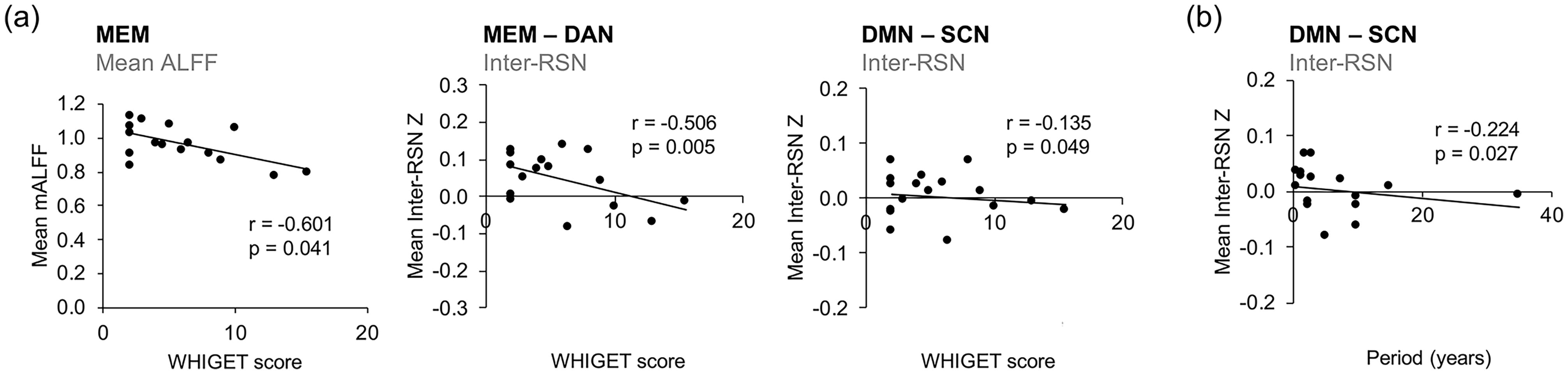
Correlations between rs-fMRI indices and tremor features.
Discussion
This study aimed to explore the alteration of FC and characteristics of RSNs in patients with ET. A total of 11 RSNs have been characterized in both normal control and patients with ET. Inter-RSN connectivity, intra-RSN connectivity, ALFF, and degree centrality have been calculated in assessing the network organization of patients with ET. Several regions with significant differences between normal control and tremor subjects have been found, including the inter-RSN connectivity, regional ALFF, and regional degree centrality. The RSN metrics were also shown to be correlated with WHIGET score. Here, we discussed the findings in this study as below.
Inter-network and intra-network connectivity
Among the inter-network connectivity comparisons, DMN–VAN connectivity was shown to be significantly reduced in patients with ET, which have not been reported before. The role of DMN and its interaction with other networks is vital in the regulation of brain function (Buckner et al., 2008, Buckner and DiNicola, 2019). It has been reported that patients with ET have worse cognitive performance than healthy controls, including attention, executive function, and language (Benito-Leon et al., 2015). Alterations in DMN and DMN-related connectivity can be related to the disturbance in self-referential processing, cognition process, and proper transition to attention-demanding task (Raichle, 2015). As DMN is involved in several cognitive functions and disrupted DMN is often observed in neuropsychological diseases, altered DMN-related connectivity in patients with ET may also imply the issues in cognitive function. Indeed, a previous study has indicated increased connectivity between DMN and frontoparietal networks (Benito-Leon et al., 2015), which was shown to related to several cognitive domains and depressive symptoms. Although the cognitive performances were not assessed in our cohort, the altered DMN–VAN connectivity may be associated with the dysregulation of attention, or the abnormality between the transition from default mode to attention-demanded task. The attention system can be triggered by sensory processing as well as internal-based information (Pessoa et al., 2003, Vossel et al., 2014). We speculate that the involuntary and rhythmic movement would draw excessive attention in patients with ET, leading to the potential abnormality of the attention network. Future studies with thorough cognitive evaluations will be beneficial to elucidate the underpinnings.
Neuroanatomically, a previous study in volumetric MRI also indicates the reduction of gray matter volume of the ET group in superior temporal gyrus and inferior frontal gyrus (Cameron et al., 2018), which are engaged in the VAN network. Other studies also suggested altered gray matter volume in precuneus (Cao et al., 2018, Pelzer et al., 2017, Qi et al., 2020), which is one of the hubs of DMN. This evidence may provide the structural basis of the disruption in DMN–VAN connectivity.
Our results show no significant difference between normal control and patients with ET in intra-network evaluations. Indeed, a previous study using voxel-based analysis has reported that patients with ET presented elevated FC in DMN and bilateral frontoparietal network and decreased FC in VIS (Benito-Leon et al., 2015). This may be caused by different evaluation approaches which were used, as the literature presented the comparison between the voxel-based connectivity maps. In contrast, the intra-network connectivity in this study was calculated by averaging out the value within predefined ROIs that are engaged in the network, representing the main contribution from the hubs in each network.
Alteration of regional ALFF
The evaluations of regional ALFF and degree centrality indicated several significant differences, distributing among several ROIs engaged in various RSNs. Differences in ALFF were found within COTC, AUD, DMN, VIS, SAN, and DAN. The changes in regional ALFF values among DMN subregions were complicated. The ALFF values were found to be increased in some of DMN subregions, including the L’t parahippocampus, R’t superior temporal gyrus, and L’t superior frontal gyrus of the ET group. On the contrary, the ET group showed decreased ALFF in R't middle temporal gyrus, L’t medial frontal gyrus, L’t fusiform gyrus, and L’t middle temporal gyrus. It has been suggested that there was an increased ALFF in R't middle temporal gyrus in patients with hand tremor but not head tremor (Wang et al., 2018), which seems to be dissimilar to the findings in this study. As the MNI coordinate of the altered ALFF in R't middle temporal gyrus in our study (x = 43, y = −72, z = 28) was a great distance to that in the abovementioned literature (x = 51, y = −36, z = 3), the intrinsic functional activity could be different.
A recent study using meta-analysis has identified several regions related to the resting-state activity changes of the ET group, including the increase in R’t postcentral gyrus, R’t superior frontal gyrus, and L’t precentral gyrus and the decrease in bilateral insula (Lan et al., 2021). Although our results indicated elevated ALFF in L't superior frontal gyrus, the coordinates were quite different. As the findings in literatures regarding to the ALFF of tremor were also varying (Li et al., 2021, Wang et al., 2018, Yin et al., 2016), our results again imply the complexity of tremor pathophysiology, especially in the cerebrum.
Alteration of regional degree centrality
The degree centrality indicates how the importance of the given ROI within a network is (Wang et al., 2015). Brain regions that possess important roles often interconnect with many other regions and contribute to functional integration (Rubinov and Sporns, 2010). Changes in degree centrality may imply the alteration on individual nodes and the reorganization of brain networks. In our result, increased degree centrality was found within SMN, AUD, DMN, VIS, SAN, and SCN. Although the ROIs found in our result were different to that in a previous study (Benito-Leon et al., 2019), both our work and the previous study have shown that the ET group generally manifests higher degree centrality among several regions. The elevated degree centrality in SMN (right postcentral gyrus and right paracentral gyrus) and SCN (left thalamus and right caudate) may indicate the abnormality of thalamo-cortical circuit, which is one of the common focuses in literatures (Holtbernd and Shah, 2021, Sharifi et al., 2014).
Alterations in DMN and SAN could be of importance to the brain function. DMN, FPTC, and SAN are regarded as the three core neurocognitive networks, which is called triple network model (Menon, 2011). The SAN plays a critical role in switching between DMN and FPTC (Sridharan et al., 2008), and dysfunction in these networks has been related to the disturbance of cognition, as seen in psychological disorders such as Alzheimer’s disease, Schizophrenia, and depression (Bolton et al., 2020, Menon, 2011). As reported in previous literatures, altered cognitive functions were also observed in patients with ET (Benito-Leon et al., 2015, Benito-Leon et al., 2019, Fang et al., 2015). Although the cognitive scores were not evaluated in the present study, our results indicate the potential of these networks and the need for cognitive evaluation in future studies.
Correlation between tremor features and rs-fMRI indices
Correlations between resting-state indices and tremor features were assessed in both network and regional level. In literature, the total B score of the Fahn–Tolosa–Marin tremor rating scale (motor impairment) has been demonstrated to be negatively correlated with the ALFF in precentral gyrus and supplementary motor area proper (Gallea et al., 2015). Consistent with literature, our results also showed negative correlation between WHIGET score and the ALFF in several SMN regions, including L't postcentral gyrus, L’t precentral gyrus, and R’t medial frontal gyrus. This evidence suggests that the resting-state activity in SMN decreased with motor impairment. In addition to SMN, several regions in DMN, VIS, and DAN also showed negative correlations between its ALFF and WHIGET score. On the contrary, it should be noted that the regions in AUD and SAN presented positive correlations between its ALFF and WHIGET score. These findings denote that the intrinsic functional activity within AUD and SAN could intensify with declined activity in other networks of patients with ET, in which the underlying causal relationship and mechanism remain to be explored in the future.
From the network aspect, our analysis showed that the inter-network connectivity of MEM–DAN and DMN–SCN were negatively correlated with the WHIGET score. In particular, a moderate correlation was found in MEM–DAN. The mean ALFF within MEM regions (cingulate gyrus and precuneus) was also negatively correlated with the WHIGET score. As DAN- and DMN-affiliated regions are important in MEM (Stawarczyk et al., 2018), these evidences may imply the disturbance in memory-associated networks. On the contrary, DMN–SCN connectivity was shown to be negatively correlated with both the WHIGET score and disease period. Although the correlation was mild, these findings might also imply the altered thalamo-cortical circuit.
The value in exploring cerebral networks
Our findings demonstrate the altered RSN connectivity and activity within the cerebrum of patients with ET, suggesting the importance of cerebral network in the disease. The interconnection and harmonization between cerebral and cerebellar networks have been highlighted in recent years (Bostan et al., 2013, Boven et al., 2023), particularly the neuroanatomical and functional relations to cognitive tasks. As the normal brain RSNs are speculated to interact and harmonize in a balanced manner, the disturbance to such dynamic equilibrium, for example, the altered motor control in patients with ET, could also lead to the interference on other networks. From our results, the observed alteration in DMN, VAN, and SAN implies the hindrance in proper switching between networks. We believe that it would be helpful to characterize these networks with thorough cognitive tests in the future. Overall, our findings indicate the worth in exploring cerebral networks. In addition to motor-related features, more attention on other cerebral functions may be required in clinical setting.
Limitations
Despite the findings that have been identified in this study, several limitations should be noted. First, the cognitive performance in this cohort was not assessed. As the non-motor features have been evidenced in literature and the target RSNs cover whole cerebrum, cognitive evaluation will be of great assistance in elucidating tremor. Second, because the original MR images in this study did not cover the whole cerebellum, cerebellum-associated regions and networks were not taken into analysis. Future studies including cerebellar circuits are believed to introduce a more comprehensive insight into the brain of tremor, both in motor and non-motor circuits. Third, only the straightforward analysis of centrality was used in this study. Other graph-theory evaluations such as betweenness centrality, participation coefficient, and modularity could help in understanding the interconnections of functional hubs and modules. In addition, sophisticated rs-fMRI indices such as dynamic effective connectivity may provide a novel aspect to the causal relationship of various brain networks. It should also be noted that, as a nature of the cross-sectional study, the casual relationship between the disease and network change is hard to be determined. The reported network changes generally reflect the condition of ET and healthy subjects during the scan. Nevertheless, our results showed mild-to-moderate correlations between specific networks and tremor severity, suggesting that these networks may be associated with the disease progress to a certain extent.
Conclusions
Resting-state fMRI was used to investigate our hypothesis that the RSN within cerebrum could be altered in patients with ET. The results indicate alterations in several cerebral network of ET, showing the potential of resting-state fMRI in exploring the cerebral basis in ET.
Footnotes
Acknowledgments
The authors gratefully thank all volunteers and their family for their participation to this research.
Authors’ Contributions
S.-M.H.: Investigation, methodology, software, visualization, writing—original draft, and writing—review and editing; C.-T.O.: Data curation, formal analysis, investigation, writing—original draft, writing—review and editing; Y.-C.H.: Conceptualization, data curation, formal analysis, funding acquisition, resources, and writing—review and editing; N.-H.C.: Formal analysis, methodology, software, and writing—review and editing; T.-K.L.: Resources and writing—review and editing; C.-Y.S.: Data curation, investigation, writing—review and editing; L.-W.K.: Conceptualization, funding acquisition, resources, methodology, supervision, writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.