
Abstract
Background:
With an aging population, the prevalence of neurological disorders is increasing, leading to a rise in lower limb movement disorders and, in turn, a growing need for rehabilitation training. Previous neuroimaging studies have shown a growing scientific interest in the study of brain mechanisms in robot-assisted lower limb rehabilitation (RALLR).
Objective:
This review aimed to determine differences in neural activity patterns during different RALLR tasks and the impact on neurofunctional plasticity.
Methods:
Sixty-five articles in the field of RALLR were selected and tested using three brain function detection technologies.
Results:
Most studies have focused on changes in activity in various regions of the cerebral cortex during different lower limb rehabilitation tasks but have also increasingly focused on functional changes in other cortical and deep subcortical structures. Our analysis also revealed a neglect of certain task types.
Conclusion:
We identify and discuss future research directions that may contribute to a clear understanding of neural functional plasticity under different RALLR tasks.
Impact Statement
The evaluation of robot-assisted lower limb rehabilitation based on brain function detection technology can assess the neurological changes of patients in the rehabilitation process by monitoring brain activities and can also provide more accurate guidance for robot-assisted lower limb rehabilitation. By monitoring the patient’s brain activity, the robot can adjust according to the real-time status of the patient to achieve more effective rehabilitation training. This has potential impact on improving the rehabilitation effect and speeding up the rehabilitation process of patients.
Introduction
Walking, a fundamental human activity, requires intricate coordination between multiple regions of the brain and the musculoskeletal system (Mehrholz et al., 2020). Neurological conditions such as stroke, spinal cord injury (SCI), and traumatic brain injury can impair gait and balance, significantly affecting independence and quality of life (Schmidt et al., 2007). Effective lower limb rehabilitation is crucial for enhancing mobility in patients with these conditions.
Current research indicates that robotic intervention in lower limb rehabilitation (RALLR) not only shortens recovery times and improve motor function but also reduce the burden on therapists (Shi et al., 2019). RALLR uses advanced bionic devices to help patients restore normal lower limb movements through targeted exercises. These devices combine insights from multiple fields including rehabilitation medicine, mechanics, robotics, and artificial intelligence.
RALLR is designed to promote neuroplasticity through exercise and neurostimulation strategies (Vaida et al., 2019). Monitoring brain activity during rehabilitation allows for a better understanding of its effects on neural networks and helps optimize treatment outcomes. This assessment provides real-time feedback to patients and therapists on the progress of rehabilitation and informs adjustments to therapy to increase effectiveness (Hobbs and Artemiadis, 2020; Hu et al., 2017). In addition, understanding brain activity can shed light on the underlying mechanisms of RALLR, potentially leading to improvements in rehabilitation technologies and practices (Campagnini et al., 2022).
In recent years, brain function detection technologies (BFDTs) have been increasingly used to assess the effectiveness of RALLR. These technologies include stationary methods such as functional magnetic resonance imaging (fMRI) (Bonanno et al., 2023) and mobile methods such as electroencephalography (EEG) (He et al., 2018) and functional near-infrared spectroscopy (fNIRS) (Bonanno et al., 2023). Despite the growing focus on BFDT-based RALLR, there is a lack of comprehensive reviews of recent studies in the field.
This article reviews neuroimaging studies of RALLR to better understand the cerebral mechanisms involved in assisted rehabilitation and to explore the potential of BFDTs in the quantitative assessment of RALLR (Berger et al., 2019).
The performance differences between the three BFDTs, EEG, fMRI, and fNIRS are compared in Table 1. EEG is valuable for its high temporal resolution, low cost, noninvasiveness, and ease of use across all age groups to reflect the electrical activity of the central nervous system. However, its low spatial resolution introduces uncertainties in the interpretation of EEG data.fMRI provides direct signals of neural brain activity and offers high spatial resolution for precise localization and parameter adjustment. It is noninvasive and suitable for all age groups. Disadvantages include sensitivity to head motion, high operating costs, inapplicability for claustrophobic patients, and susceptibility to noise interference.fNIRS, a newer brain imaging technique, uses near-infrared light in the 600–1000 nm range to measure brain activity (Hong et al., 2020). It is portable, less expensive than fMRI, and more tolerant of motion artifacts, making it suitable for a variety of settings, including clinical applications (Doherty et al., 2023) and naturalistic environments (Gossé et al., 2022). fNIRS has higher tolerance to motion artifacts compared with EEG and fMRI, allowing for more robust monitoring in real-world scenarios (Chen et al., 2020).
Comparison of the Performance of the Three Brain Function Detection Technologies of fNIRS, fMRI, and EEG.
EEG, electroencephalography; fMRI, functional magnetic resonance imaging; fNIRS, functional near-infrared spectroscopy.
Other technologies, such as transcranial magnetic stimulation (TMS), have limited application in RALLR because they only affect localized brain areas and do not modulate deeper neural circuits (Tsuboyama et al., 2020). Although side effects such as mild dizziness or scalp discomfort and rare seizures are a concern, they are generally mild and carefully managed (Tsuboyama et al., 2020). Therefore, TMS was not included in our analysis of BFDTs for RALLR.
Materials and Methods
We obtained 481 research works from an initial search of the Web of Science, PubMed, and Scopus database using the following query string for the article title, keywords, and abstract, on articles published in the past 22 years (between January 1, 2000, and January 1, 2023):
(“robot-assisted rehabilitation” OR “robotic rehabilitation” OR robot OR “assistive *” OR “* orthosis”) AND (walking* OR training* OR task* OR exercise*) AND (fMRI OR MRI OR “* magnetic resonance imaging” OR EEG OR electroencephalography OR fNIRS OR “functional near-infrared spectroscopy” OR NIRS OR “near-infrared spectroscopy” OR “optical topography”) AND (leg* OR “lower extremit*” OR “lower limb*”)
After reviewing titles and abstracts, we excluded duplicate publications and those that met one or more of the following exclusion criteria: reviews, meetings, book chapters, dissertations; studies focusing on non-lower limb approaches; studies using measures other than fMRI, EEG, or fNIRS; studies with nonrelevant primary outcomes. After a full-text review, a total of 68 articles met our inclusion criteria and were considered for the study. The detailed selection process is illustrated in Figure 1.

PRISMA flow diagram of literature search.
After statistics, we can find that among the 68 articles finally screened, 53 of them used the neuroimaging method of EEG, 10 used fMRI, and only five fNIRS.
We classified the articles using a twofold taxonomy consisting of brain regions and lower limb task categories, as shown in Figure 2. According to the anatomy of the cerebral cortex, the brain regions involved in this study were grouped into the following eight categories:

Taxonomic overview of the reviewed studies.
Frontal cortex (FC), which is represented in the FC including primary motor cortex (M1), premotor cortex (PMC), supplementary motor area (SMA), frontal eye fields (FEF), middle frontal gyrus (MFG), the superior frontal gyrus (SFG), and dorsolateral prefrontal cortex (DLPFC).
Parietal cortex (PC), represented in the PC including primary somatosensory cortices (S1), secondary somatosensory cortices (S2), the superior parietal lobe (SPL), inferior parietal lobe (IPL), and precuneus (PCUN).
Occipital cortex (OC), which is represented in the OC, including primary visual cortex (PVC), and occipital gyrus/sulci occipitalis laterals (OG/SOL).
Temporal cortex (TC), which is represented in the TC, including primary auditory cortex (PAC), the superior temporal gyrus, middle temporal gyrus (MTG), and fusiform gyrus (FG).
Limbic system (LS), represented in the LS including ventral anterior cingulate cortex (VACC), dorsal anterior cingulate cortex (DACC), ventral posterior cingulate cortex (VPCC), dorsal posterior cingulate cortex (DPCC), hippocampus, and amygdala (AMY).
Insula is part of the LS of the brain.
Thalamus (Thal).
Basal ganglia (BG).
Based on the types involved in all publications, the lower limb tasks were clustered into: Single task, which divided into motor task (MT) and motor-imagery task (MIT). MIT, which included lower limb rehabilitation tasks with walking/running, cycling, sit-to-stand/stand-to-sit, climbing, left/right turning, tapping, stepping, and extending and flexing. MT include other categories of tasks in addition to those mentioned above. Dual task, which included lower limb rehabilitation tasks with MT-Auditory tasks (AT), MT/MIT-Visual tasks (VT), MT/MIT-Cognition tasks (CT). Multi task, which included the MT/MIT-VT-AT.
In addition, we further analyzed these articles based on different data sources. Considering that in dual task and multi task, MT and MIT are arranged the same lower limb task in the same article, so they are combined.
Results
As shown in Figure 3, we find that the total number of published articles for three BFDTs has increased over the years. The number of publications for EEG has grown in recent years, although it has declined since 2018. The decline in the number of EEG publications since 2018 may involve a number of factors. The most important factor is the continued development of technology; while EEG has an advantage in terms of temporal resolution, other neuroimaging techniques are more favorable in terms of spatial resolution and depth. Researchers may prefer to use these techniques. Since fMRI has relevant articles published since 2011, we started the prediction analysis from 2011, and its studies have risen polynomially. fMRI-related data sources have a total of 10 published articles, 5 of which were published in the year 2014. Since fMRI is excellent at detecting activity in deep cortical and subcortical areas. Researchers have attempted an innovative adaptation of fMRI with the addition of fMRI-compatible robotic-like stepping actuators to provide active and passive gait movements to patients without compromising image quality. As an emerging BFDT, fNIRS has been less used in RALLR, and related articles have only been published since 2017, but they also show a growing trend.
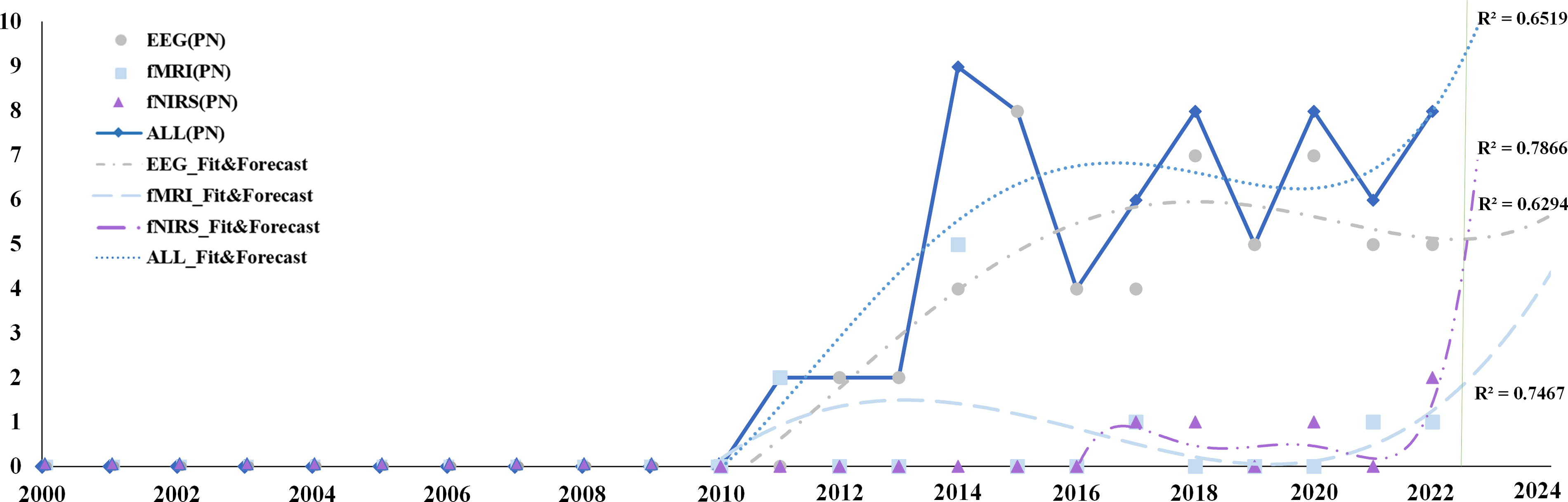
Number of EEG, fMRI, fNIRS, and ALL publications and forecasts over time. EEG, electroencephalography; fMRI, functional magnetic resonance imaging; fNIRS, functional near-infrared spectroscopy.
As shown in Figure 4, the sunburst chart can not only show the proportion of the total number of published articles in each country but also clarify the proportion of the number of published articles in each country each year. As can be seen from the above figure, China has done a lot of research on brain function detection technology in RALLR, and the number of published articles is also increasing year by year. This is followed by the USA and then Switzerland.
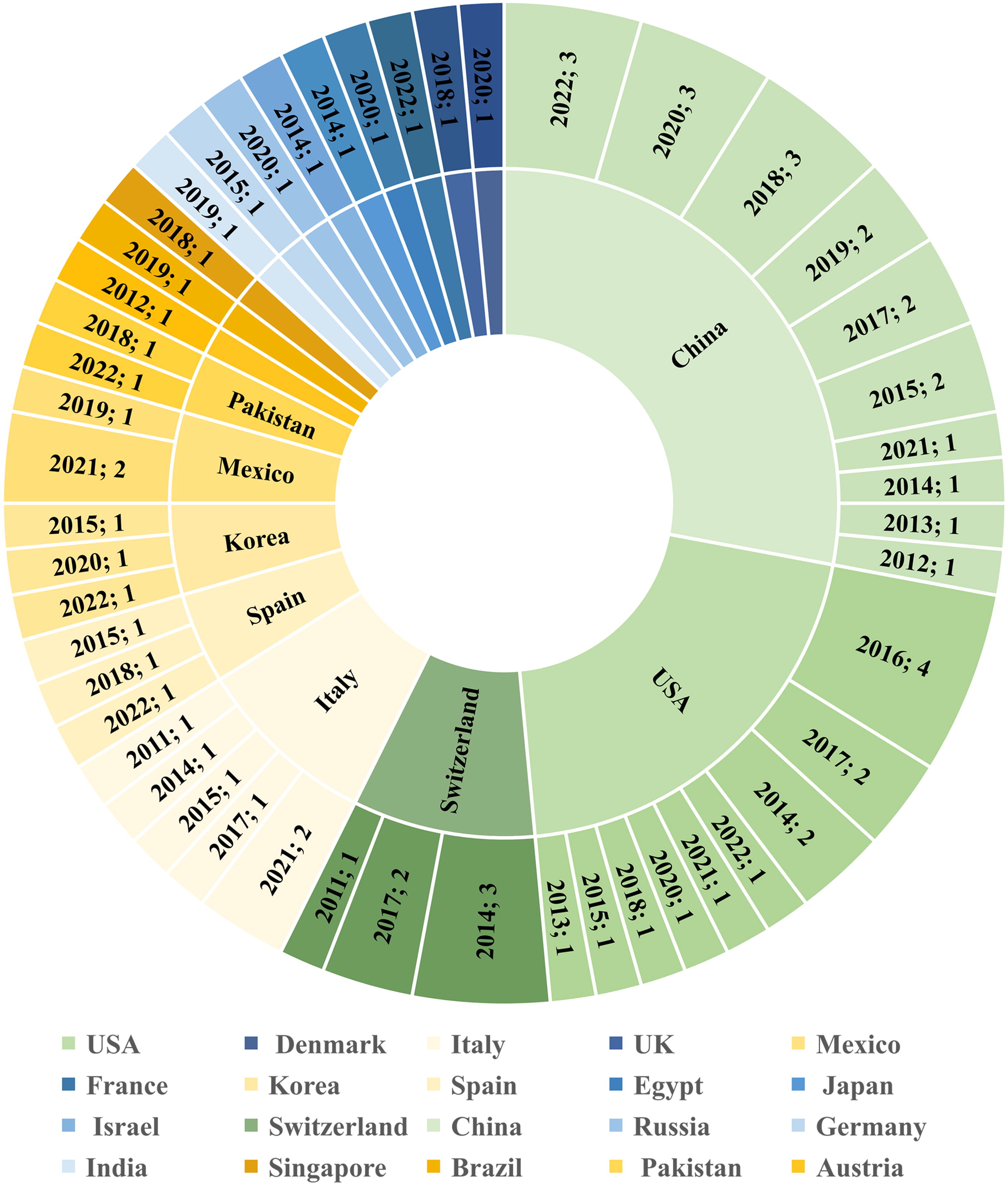
Sunburst of active country in number of each country publications over time.
The size of each circle indicates the number of articles covering a given lower limb task (row) and the distribution of brain regions (column) (Pinto-Fernandez et al., 2020). Bars on the right indicate the total number of publications covering the corresponding lower limb task. Bars at the bottom indicate the number of publications covering the corresponding brain region. The colors of the bars represent the three main categories of lower limb tasks (single task, dual task, and multi task). The numbers in the last column indicate the number of brain regions covered by each lower limb task, and vice versa for the numbers in the last row. The size of the color dot represents the number of reviewed studies. In general, as shown in Figure 3, the number of publications has increased slowly over the years. However, for lower limb rehabilitation training, different brain areas have different research emphases.
Brain regions
As shown in Figure 2 and Table 2, we classify the existing research according to the Brodmann area system, which divides the cerebral cortex into a series of anatomical regions based on cellular structure. Owing to the different optical plate positioning rules for different brain imaging detection techniques, based on the international 10–20 reference system, we unified these different placement rules to find the approximate brain atlas partition (Brodmann partition) label.
Classification of Lower Limb Tasks Corresponding to Different Brain Regions
AG, angular gyrus; BG, basal ganglia; MC, motor cortex; ACC, anterior cingulate cortex; OG/SOL, occipital gyrus/sulci occipitalis laterals; SMG, supramarginal gyrus; DACC, dorsal anterior cingulate cortex; DPCC, dorsal posterior cingulate cortex; DLPFC, dorsolateral prefrontal cortex; FEF, frontal eye fields; INSL, insula; IPL, inferior parietal lobe; MFG, middle frontal gyrus; MTG, middle temporal gyrus; PAC, primary auditory cortex; PHG, hippocampus; PMC, premotor cortex; PVC, primary visual cortex; SFG, superior frontal gyrus; SMA, supplementary motor area; SPL, superior parietal lobe; STG, superior temporal gyrus; VACC, ventral anterior cingulate cortex; VPCC, ventral posterior cingulate cortex.
Lower limb task
Single Task-MT-walking/running: This type is often used in lower limb rehabilitation training and rehabilitation programs for various lower limb disorders. This is the most frequent lower limb task in the literature, with 23 publications (Bonnal et al., 2022; Contreras-Vidal et al., 2018; Di Marco et al., 2021; Do et al., 2013a; Garcia-Cossio et al., 2015; Hasan et al., 2020; Hasan et al., 2021; He et al., 2014; Jochumsen and Niazi, 2020; Lee et al., 2017; Li et al., 2020; Li et al., 2021; Li et al., 2018; Li et al., 2019a; Lisi et al., 2014; Liu et al., 2017b; Liu et al., 2015; Marchal-Crespo et al., 2011; Marchal-Crespo et al., 2014a; McCrimmon et al., 2015; Saleh et al., 2022; Sczesny-Kaiser et al., 2015; Shin et al., 2022).
Single Task-MT-cycling: This task type has also been involved in only two (Delisle-Rodriguez et al., 2019; Dong et al., 2022) articles, the subjects (Delisle-Rodriguez et al., 2019) were asked to pedal on a monocycle, the patient’s foot was fastened on the pedal (Dong et al., 2022) to achieve planar movement, and the two degree-of-freedom plane motion of the pedal can be realized.
Single Task-MT-sit-to-stand/stand-to-sit: We found four publications (Bulea et al., 2014; Jochumsen and Niazi, 2020; Shin, 2020; Wang et al., 2018) involved in the lower limb task category, spanning eleven different brain types, which improve lower limb neuroprocessing and rehabilitation techniques by distinguishing early detection of motor intent.
Single Task-MT-climbing: Only two articles (Li et al., 2019b; Winslow et al., 2016) covered this lower limb task, with three different brain types. Subjects climbing stairs or crawling on slopes with the assistance of powered exoskeletons can effectively enhance human mobility and promote lower limb rehabilitation.
Single Task-MT-right/left turning: We found two publications (Lee et al., 2017; Vinoj et al., 2019), covered this category, with five brain region types: M1, PMC, SMA, S1, and S2.
Single Task-MT-tapping: Only one article (Batula et al., 2017), covered this category, with three brain region types: M1, PMC, SMA, all in FC. Subjects tapped their right and left feet during RALLR.
Single Task-MT-stepping: We found three publications (Jochumsen and Niazi, 2020; Marchal-Crespo et al., 2014b; Mercado et al., 2021) evaluating lower limb tasks, which include three movement tasks: step up, side step, and back step.
Single Task-MT-extending and flexing: We found two articles (Formaggio et al., 2017; Heng et al., 2020) that considered this scenario, with thirteen brain region types, including foot active or passive dorsi-plantar extending and flexing and single-joint cyclic ankle motor.
Single Task-MT-others: We found four publications (Attallah et al., 2020; Sui et al., 2014; Yi et al., 2013; Zhang et al., 2015), covering the difficult to define RALLR training, with five brain region types.
Single Task-MIT-walking/running: We found four publications (Cohen et al., 2014; Donati et al., 2016; Kun et al., 2020; Liu et al., 2017b). MI was used to control the robotic motions of walking or performing gait in a neurorehabilitation paradigm aimed at restoring locomotion.
Single Task-MIT-cycling: There are two publications (Delisle-Rodriguez et al., 2019; Dong et al., 2022), in which the subjects were asked to mentally pedal on a cycle, thinking of a real situation, such as going to the beach or home, among others.
Single Task-MIT-sit-to-stand/stand-to-sit: This lower limb task has been involved in only one article (Wang et al., 2018), spanning seven different brain region types.
Single Task-MIT-climbing: We only found one publication (Li et al., 2019b) assessing this task type, with three different brain region types: M1, S1, and S2.
Single Task-MIT-turning right/left: We only found one publication (Lee et al., 2017) with six different brain region types, using MI to distinguish the intention of turning left and right.
Single Task-MIT-tapping: Only one publication (Batula et al., 2017), covered these motor types, which focused on MI for tapping.
Single Task-MIT-stepping: One article (Jochumsen and Niazi, 2020) covered this category, with twelve brain region types, including three MITs: step up, side step, and back step.
Single Task-MIT-extending and flexing: We found only one publication (Formaggio et al., 2017), which mentioned movement imagination of foot passive dorsi-plantar flexion in the text.
Dual Task-MT and AT: There are two publications (Jaeger et al., 2014; Zhang et al., 2017). The participants responded accordingly to the sound (the auditory stimulation), the corresponding cerebral cortex also responded, especially the PAC.
Dual Task-MT/MIT and VT: We found eight publications (Andreu-Perez et al., 2018; Gordleeva et al., 2020; Kwak et al., 2015; Lisi et al., 2014; Liu et al., 2018; Trieu Phat et al., 2016; Youssofzadeh et al., 2016; Zhang et al., 2018). This is the second most considered task category in this review. When processing MT and visual task at the same time, it refers to the lower limb task using screen or VR (Virtual Reality) as an aid to bring participants into a virtual scene in order to enhance visual stimulation. Data in (Zhang et al., 2018) refer to visual stimulation with a flashing light bulb.
Dual Task-MT/MIT and CT: Three articles (Ferrero et al., 2022; Marchal-Crespo et al., 2017; Sacco et al., 2011) were found covering this aspect. These studies concentrated on the default mode network in the resting state. CTs such as subtraction cycle calculation and learning predefined gait-like patterns in advance were used while MT or MIT performed in the meantime. This situation increased interference with the brain, and it is critical to choose the matching dual-task type in relation to the cognitive ability of the patient, for better improving the evaluation and training effects.
Multi Task-MT/MIT and VT and AT: We found six publications (Cui et al., 2022; Gaxiola-Tirado et al., 2019; Liu et al., 2017a; Maggio et al., 2021; Zhang et al., 2015; Zhou et al., 2022a), ranking in third place among the covered lower limb task category. It is enough to see that the lower limb training under multimodal stimuli has attracted the attention of researchers.
Analysis of subject selection conditions
In Table 3, we discuss various aspects of sample size, male/female ratio, age, patient status, region, and ethnicity, considering demographic factors.
Experimental Scale Design
AB, able bodied; F, female; H, healthy; P, patients; LH, left-handed; M, males; RH, right-handed; RF, right-footed; NHND, no history of neurological diseases; NLD, no locomotor deficits; NLLP, no lower limb pathology; NV, normal vision; SCI, spinal cord injury; SD, standard deviation.
Ethnicity
Subjects with different skin colors may have different hair densities and scalp colors. Selecting a sample of subjects with different skin colors may provide a more complete picture of the applicability of the various BFDTs. None of the selected literature mentions the use of subjects of different skin color, and the literature (Pinti et al., 2020) reports on a study of infants in Africa that investigated the neurodevelopmental effects on children in a low-resource environment. The literature mentions that fNIRS (Pinti et al., 2020) is a viable method for investigating whether PFC is activated in children, but as fNIRS relies on optical detection, it is not possible to predict whether the use of darker-skinned subjects will affect data collection. This is because of two factors, one of which is technical: there are very few hairs on the front of the skull. The second is that the amount of hair and its scalp color can affect the accuracy of the data collected and increase the complexity of the data collection and processing process. The literature in the table below does not take into account ethnicity in the experimental design, and in order to increase the credibility of the findings, a sample of subjects of different ethnicities could be selected for future research. Cultural differences between races can affect cognitive processing and motor learning (Taylor and Ivry, 2011). Genetic factors related to ethnicity can affect research on brain network mechanisms (Wang et al., 2022).
Patients’ status
In most experiments, only healthy participants were recruited. Only a few trials have used patients as controls, and the limited number of patients provided in these trials is insufficient for drawing meaningful conclusions. With regard to reviewing the implications of the limited use of patient populations in research, we discussed the following aspects: in terms of external validity, the external validity of research findings can be affected by the limited choice of patient populations. If only specific types of patients are used, then the results of the study may not apply to other populations. Therefore, we need to be careful when interpreting the results and be aware of the scope of their applicability. In respect of clinical application: a restrictive patient population may lead to limitations in clinical application. For example, a treatment may be effective in a particular patient group, but whether it is applicable to a wider range of patients requires further study. Clinical decisions should be based on more comprehensive evidence. In view of neuroplasticity and individual differences, limitations in patient populations may affect the understanding of neuroplasticity and individual differences. There may be differences in brain adaptations and responses between patients, which need to be explored in a wider sample. Limitations of the patient population may affect the statistical validity and reliability of the study when considered in terms of study design and sample size selection. Larger sample sizes and diverse patient populations may enhance the scientific value of the study.
In conclusion, when discussing the results of the study, we should carefully consider the limitations of the patient population and encourage a wider and diverse study sample.
Male/female ratio
Gender differences exist in brain activation patterns during lower limb MTs (Hong et al., 2020). In the RALLR, it is not difficult to find that male subjects have more advantages than female subjects to a certain extent. Most experiments, however, allow for an even split between men and women. There is a lack of women, there’s a lot of experiments with only men, and it’s not well thought out. For the following reasons, we chose to recruit only male participants: the customized exoskeleton was designed to fit a specific range of heights and weights in order to provide proper and efficient assistance (Li et al., 2019a); women’s strength might bias data analysis, as they differ from males in strength (Li et al., 2019a). For female subjects, hormonal fluctuations (e.g., menstrual cycle) may affect brain responses. Gender-specific feedback mechanisms could optimize rehabilitation training (Xu et al., 2022).
Age
Age-related changes in brain structure and function can affect BFDT outcomes (Vandewouw et al., 2024) In terms of neuroplasticity, younger individuals may exhibit greater neuroplasticity, allowing for faster adaptation to BFDT systems (Mary et al., 2022). Older adults may experience slower learning curves and reduced motor control. A wide range of age ranges facilitates individualized treatment, and adapting the treatment programmed to different age groups improves the outcome of rehabilitation (Vandewouw et al., 2024). For the sake of experimental convenience, most of the experiments in college and universities in the below table restrict the sample group to college students, which led to the limitations in the sample ranges and means. We divided the subjects into the patient group and the healthy group to analyze the age distribution, respectively, and obtained that the age of the patient group was approximately distributed in the range of 15–46 years old, while the age of the healthy subjects was approximately distributed in the range of 27–52 years old.
Discussion
RALLR has demonstrated significant advantages over traditional rehabilitation methods, as evidenced by significant improvements in clinical outcomes and recovery efficiency (Meng et al., 2015). This article summarizes studies using BFDTs to assess the effectiveness of RALLR, referencing a total of 68 studies. As shown in Figure 3, there is a consistent increase in research activity in this area. Table 4 provides a summary of the “Results” section of the reviewed studies, categorizing the main findings. In the following sections, we will explore in more detail the potential reasons for this growing interest in RALLR and the use of BFDTs to study its impact.
An Overview of the Section “Result” Found on the Reviewed Studies Engaged in the Main Categories
AMY, amygdala; AT, auditory tasks; BG, basal ganglia; CT, Ccognition tasks; DACC, dorsal anterior cingulate cortex; DLPFC, dorsolateral prefrontal cortex; DPCC, dorsal posterior cingulate cortex; FEF, frontal eye fields; FG, fusiform gyrus; INSL, insula; IPL; inferior parietal lobe; MFG, middle frontal gyrus; MIT, motor-imagery task; MT, motor task; MTG, middle temporal gyrus; OG/SOL, occipital gyrus/sulci occipitalis laterals; PAC, primary auditory cortex; PCUN, precuneus; PHG, hippocampus; PMC, premotor cortex; PVC, primary visual cortex; SFG, superior frontal gyrus; SMA, supplementary motor area; SPL, superior parietal lobe; STG, superior temporal gyrus; Thal, Thalamus; VACC, ventral anterior cingulate cortex; VPCC, ventral posterior cingulate cortex; VT, visual tasks.
Brain region
The categorization map shows that a significant amount of studies on lower limb tasks have focused primarily on the motor cortex in the FC and the sensory cortex in the PC. The motor cortex, which is responsible for controlling movement in the lower limbs, includes three main areas: M1, SMA, and PMC. These areas not only receive input from almost all of the cortical areas involved in motor control but also represent the category with the most articles on lower limb tasks, as shown in Figure 2.
The FEF, which controls eye movement, accounts for 15% of the total studies. The PFC plays a key role in the planning and execution of lower limb rehabilitation exercises. The DLPFC is key to cognitive processes and integrates prefrontal association. It is connected to several other brain areas, such as the Thal, HPC, PC, and TC, and handles functions such as working memory and executive processes that are essential for thought and action. Studies involving DLPFC-related tasks account for 12% of the total.
On the other hand, the MFG is crucial for training postural control and is involved in other movements, including visual and cognitive tasks, although only two articles focus on this region. The SFG is involved in a variety of functions, including motor skills, working memory, resting state, and cognitive control, but remains understudied.
The PC, which is central to sensory perception and processing, contains the S1 and S2 somatosensory cortices, which process body sensations related to temperature, pain, touch, weight, and proprioception. Other PC subdivisions such as the SPL, IPL, and PCUN also support lower limb training by integrating various sensory and motor feedback to facilitate information processing and decision making.
The PVC, located in the OC, is responsible for the initial processing of visual information and accounts for 24% of the total. The VACC, VPCC, DACC, and DPCC are the main components of the LS involved in emotion, learning, and memory. Related tasks have also been included in cortical studies, accounting for 20% of the total.
Similarly, studies on the HPC are beginning to gain more attention, and in the subcortical areas such as the AMY, functional connectivity has been found to increase with training, but only one article has been published, probably because of the limitations of certain BFDTs in detecting and accurately measuring subcortical regions.
Lower limb task
Figure 2 shows that the number of studies focusing on walking far exceeds those investigating other lower limb rehabilitation tasks, confirming its importance. Walking not only strengthens the leg muscles, increasing strength and flexibility, but also improves balance and coordination. These improvements are critical for rehabilitation patients, especially those recovering from conditions such as stroke or SCI. Since walking is both a fundamental daily function and the primary focus of lower limb exoskeletons and stationary rehabilitation robots, its experimental design is relatively simple, making it a popular choice among researchers (Pinto-Fernandez et al., 2020).
Despite the focus on walking, other tasks in lower limb rehabilitation such as cycling, squatting, stepping, climbing, right/left turning, and sit-to-stand/stand-to-sit provide varied challenges and enjoyment for both patients or healthy participants during RALLR. In addition, motor imagery has gained attention for its ability to activate sensorimotor regions similar to actual task performance and induce brain plasticity, improving task evaluation accuracy and reducing experimental risk for patients (Teo and Chew, 2014).
Dual tasks involving motor-visual functions are well suited for assessment with all three BFDTs. Studies using motor-AT show clear cerebral responses to auditory stimuli, particularly in the PAC (Jaeger et al., 2014; Zhang et al., 2017). Such studies suggest that auditory stimulation can enhance cognitive, social-emotional, and motor functional connectivity (Haslbeck et al., 2020).
The experimental paradigm of motor-cognitive tasks has matured, and there are three articles involving this experimental paradigm (Ferrero et al., 2022; Marchal-Crespo et al., 2017; Sacco et al., 2011). Studies in this area mainly focus on cognitive challenges such as subtraction or learning walking patterns during MTs. Selecting tasks that match the subject’s cognitive abilities is crucial for improving the quality of both assessment and training.
There are six literatures related to Multi Task (Cui et al., 2022; Gaxiola-Tirado et al., 2019; Liu et al., 2017a; Maggio et al., 2021; Zhou et al., 2022a; Zhou et al., 2022b), ranking third in the category of lower limb tasks covered. This indicates a growing research focus on RALLR under multimodal stimuli, assessed using BFDT.
Data source
The limitations of nonwearable fMRI technology limit its applicability to training tasks in RALLR, resulting in a paucity of relevant literature. However, four fMRI evaluation studies have used the MRI-compatible robotic gait actuator MARCOS (Jaeger et al., 2014; Marchal-Crespo et al., 2014a; Marchal-Crespo et al., 2014b; Marchal-Crespo et al., 2017). MARCOS, a single-degree-of-freedom robot, allows both active (machine-controlled) and passive (subject- controlled) gait-like movements during fMRI scans without compromising image quality.
Among the portable BFDTs, EEG and fNIRS are prominent. EEG, which measures electrical potential changes from the scalp, is widely used because of its high temporal resolution, noninvasiveness, portability, and low cost, resulting in numerous EEG-based studies in this review.
It is important to note that both fMRI and EEG are sensitive to subjects’ head movements, which can affect the accuracy of brain response recordings. Conversely, fNIRS offers a promising alternative. This relatively new technology provides faster temporal resolution than fMRI and better spatial resolution than EEG. Its higher portability and lower susceptibility to artifact interference make fNIRS less sensitive to head motion. This allows data acquisition in a variety of settings and positions, facilitating support for more complex and challenging RALLR tasks. Despite these advantages, as shown in Figure 3, the number of studies using fNIRS in RALLR remains limited, although interest is gradually increasing (Berger et al., 2019).
Experimental design
This study identified several common limitations of the studies reviewed. First, the majority of research had small sample sizes, typically less than 20 participants, and included only healthy subjects. This is a significant limitation to the generalizability of the findings. Second, there was a notable lack of diversity in the selection of participants. Many experiments restricted their participant pool to male subjects only, and none of the studies reviewed included black subjects or considered racial factors in their analyses. In addition, while there is a growing trend to combine BFDTs with other techniques to obtain more accurate data-for example, incorporating physiological signals such as myoelectricity to assess brain activation levels-such integration was lacking in the studies selected for this review.
Regarding brain network connectivity, only four articles were identified that addressed this aspect, focusing solely on functional connectivity. Important types of connectivity, such as effective connectivity and structural connectivity, were not investigated. Understanding these aspects is essential to elucidate the brain’s information processing mechanisms during different lower limb tasks, which would help determine the degree of activation and connectivity within the corresponding brain networks. Future research addressing these limitations could significantly improve our understanding and application of BFDTs in robotic lower limb rehabilitation.
Limitations
This article does not provide an in-depth summary of the data analysis methods used in the reviewed studies. Although common data analysis techniques were mentioned, emerging methods that could potentially enhance understanding, such as deep learning, brain rhythm analysis, and complexity analysis, were not explored. Highlighting and integrating these innovative analysis methods could lead to significant advances in the field. In addition, the research considered only three standard BFDTs. There are additional BFDTs that could provide meaningful insights, but were not included because of their limited mention in the selected articles. Furthermore, this article focused only on lower limb rehabilitation because of its direct relevance to walking. Inclusion of a broader range of BFDTs, and perhaps a broader range of MTs, could provide a more comprehensive understanding of neurorehabilitation processes.
Conclusion
The increasing use of robotics in lower limb rehabilitation is becoming a widespread trend. Despite this, there is an ongoing debate within the scientific community about its effectiveness (Rodgers et al., 2019), highlighting the need for more comprehensive studies to draw reliable conclusions about its effectiveness.
Rooted in the theory of neuroplasticity (Nahum et al., 2013), modern rehabilitation medicine relies heavily on understanding and influencing the brain’s ability to reorganize itself. Since direct visualization of the brain’s intricate activities is not possible, BFDTs serve as critical tools for assessment studies. BFDTs primarily assess the activation state of the cerebral cortex and the dynamics of brain network connectivity during cognitive activities, making them indispensable for studying the effects of RALLR.
This review found a polynomial increase in publications investigating the effectiveness of RALLR, which indicates a burgeoning interest in understanding the associated brain mechanisms. Despite this growing interest, there is considerable heterogeneity in the areas of focus within the cerebral cortex. Research has predominantly focused on the motor areas in the FC, the somatosensory cortex in the PC, and the vision-related cortex in the OC. In contrast, other regions such as the MTG, FG, and other deep subcortical nuclei such as the AMY, BG, and Thal have been less studied, with only a few publications in the past two decades.
In terms of task types in rehabilitation, walking tasks continue to be the most widely studied because of established experimental paradigms such as n-back tasks. However, there is growing interest in more complex task types that combine motor functions with cognitive challenges, such as AT and decision making, although these areas are not as robustly developed. We believe that performing different types of lower limb rehabilitation tasks to discover the corresponding level of brain activation is important for understanding information processing in the brain.
The findings of this review may provide a clear understanding of where BFDT-based RALLR evaluation research has been neglected over the past two decades. The study of brain mechanisms in RALLR training contributes to the development of neurorehabilitation therapies to promote neuroplasticity. Although the advantages of robotics are clear, it is too early to conclude that all RALLR is superior to traditional manual therapy. In order to evaluate the clinical effectiveness of rehabilitation robots, further studies with larger patient populations should be conducted in the future. It is hoped that in the near future, researchers will be able to study more efficient RALLR training protocols and analyze the level of cortical activation and connectivity during lower limb training in a more rigorous and scientific manner.
Footnotes
Acknowledgment
The authors would like to thank the reviewers for the constructive comments regarding this article and all those who have helped us finish this article.
Authors’ Contributions
Conceptualization, Y.W. & D.W.; methodology, Y.W. & D.W.; software, Y.W.; validation, D.W.; formal analysis, Y.W.; investigation, Y.W..; resources, Y.W.; data curation, Y.W..; writing—original draft preparation, Y.W. & D.W.; writing—review and editing, D.W.; visualization, Y.W.; supervision, D.W. & H.Y.; project administration, D.W.; funding acquisition, D.W.
Author Disclosure Statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding Information
The authors gratefully acknowledge the financial supports by National Key R&D Program of China (No. 2023YFC3604800).