
Abstract
Background:
Brain tumors are associated with impaired cognitive functioning, which may result from disruptions in brain structural connectivity. Estimating structural disconnections is a more advantageous representation of tumor impact and can be performed indirectly through normative brain atlases.
Materials and Methods:
Using a publicly available dataset of glioma and meningioma patient MRI scans and tumor masks, latent correlations were estimated between measures of structural disconnection and attention-based cognitive functioning. These measures included gray matter (GM) parcel damage, white matter tract damage, GM parcel-to-parcel disconnections, and reaction time (RTI) as part of the Cambridge Neuropsychological Test Automated Battery to assess attention.
Results:
Preprocessing pipelines with two different methods of minimizing the pathology impact on MRI normalization were utilized: cost-function masking and lesion filling. The results across both pipelines were nearly consistent, with significant correlations mainly found between RTI measures and the damage to the left inferior fronto-occipital and uncinate fasciculus, as well as the left prefrontal–visual disconnections.
Conclusions:
This alludes to the importance of left-hemispheric prefrontal–visual coupling in attention-based tasks, particularly those involving object- and feature-based attention.
Impact Statement
Using a publicly available dataset of glioma and meningioma patient MRI scans and tumor masks, atlas-based normative modeling and latent correlations were used to estimate the association between measures of structural disconnection and attention-based cognitive functioning. Our findings underscore the critical role of left-hemispheric prefrontal–visual coupling in attention-based tasks. Moreover, our comparison of preprocessing methods highlights the robustness of our results, affirming the significance of our approach in understanding the cognitive consequences of brain tumors.
Introduction
Meningiomas and gliomas are the two most common primary brain tumors in adults (Wang et al., 2023; Weller et al., 2015). While meningiomas are generally benign and associated with a better prognosis than gliomas (Lee and Wee, 2022; Maggio et al., 2021; Weller et al., 2015), both conditions are accompanied by neurological symptoms that greatly affect daily activities (Lee and Wee, 2022; Ogasawara et al., 2021). Research on brain tumor outcomes now recognizes cognitive functioning as an important metric because of its significant impact on patient quality of life (Kirkman et al., 2022; Meskal et al., 2016). Three-quarters of patients with glioma experience cognitive deficits prior to treatment (Spina et al., 2023). Meningiomas are understudied compared to gliomas, although presurgical cognitive impairment was also found in this group of patients (Meskal et al., 2016; Rijnen et al., 2019).
Behavioral and cognitive assessments can be studied in relation to tumor location using lesion-symptom mapping (LSM) (van Grinsven et al., 2023). Traditional LSM using a voxel-wise representation of lesions fails to capture the impact of damage on structures spanning across various areas of the brain, such as white matter tracts (WMT). This limitation has prompted the exploration of alternative methods capable of capturing such structural disconnections (Griffis et al., 2021).
Diffusion tensor imaging (DTI) can be used to visualize the WMT course, allowing for direct assessment of lesion-inflicted damage (Mandal et al., 2023). Using this method, the brain can be represented as a network of gray matter (GM) regional nodes and WMT connectivity as graph edges (Fekonja et al., 2022). In fact, an increasing number of studies have shown that brain tumors lead to widespread functional and structural brain network reorganization (Falcó-Roget et al., 2024; Silvestri et al., 2022), with significant consequences on cognitive abilities. This suggests that patients’ cognitive functioning is dependent on the complex interplay and connectivity between brain regions rather than isolated GM areas or WMT pathways (Maas and Douw, 2023; Mandal et al., 2023; Wei et al., 2023).
Alternatively, structural disconnections can be estimated indirectly by mapping the patients’ lesion masks to the reference space or a normative atlas aggregated from healthy individuals. More specifically, the locations of lesions are used to calculate damage to lesion-associated brain networks or the probability of structural disconnection caused by the intersection of lesions and WMTs estimated from healthy subject data (Foulon et al., 2018; Griffis et al., 2021). This approach has the benefit of allowing the analysis of historical routine patient data, even when patient-specific DTI is lacking, and it minimizes intersubject variability caused by low-quality estimates of noisy MRI data (Germann et al., 2022; Sperber et al., 2022) (Fig. 1).
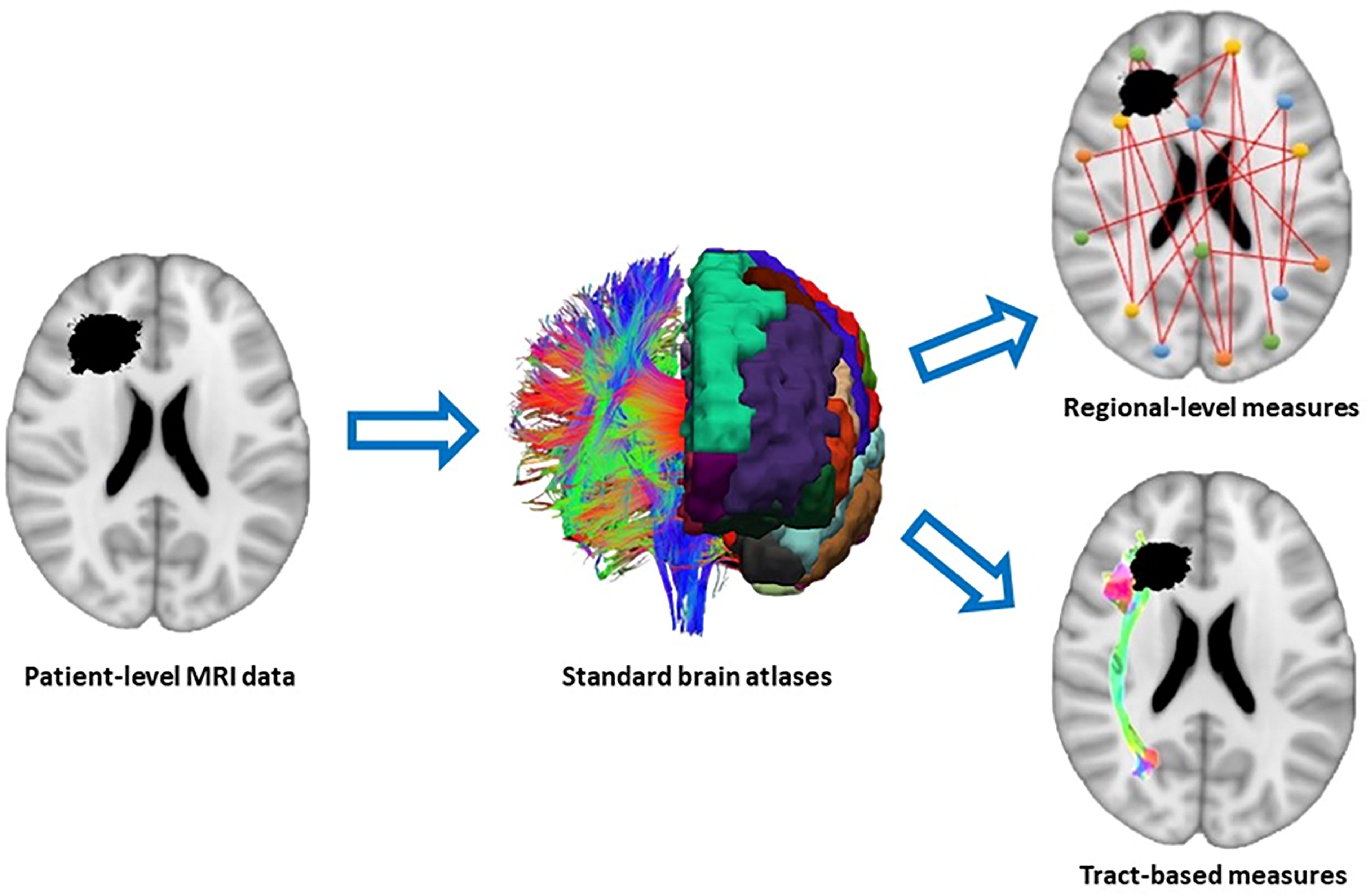
Normative atlas-based representation of brain lesions. Rather than representing lesions as binary voxels, lesions can be represented as measures of damage to GM parcels, WMT damage, and GM parcel disconnections. Adapted from Schiffler et al. (2017). GM, gray matter; WMT, white matter tract damage.
Indirect mapping of structural disconnections has been studied in numerous neurological and psychiatric disorders (Bertagnoli et al., 2022; Cotovio et al., 2022; Pan et al., 2022; Talozzi et al., 2023), but is still largely underexplored in neuro-oncology research (Burkhardt et al., 2023; Silvestri et al., 2022).
Therefore, this study aimed to estimate the relationship between tumor-related structural alterations and cognitive performance using normative brain atlases. This was performed using two custom preprocessing pipelines designed to mitigate the impact of tumor pathology on MRI normalization, and the results from each pipeline were compared and discussed.
Methods
Data
Preoperative data of 11 glioma patients (mean age = 47.5 years; standard deviation [SD] = 11.3) and 14 meningioma patients (mean age = 60.4 years; SD = 12.3) were obtained from the OpenNeuro database (Aerts and Marinazzo, 2022). Patients were recruited on the day before surgery and were eligible if they (1) were at least 18 years old, (2) had a supratentorial meningioma (WHO grade I or II) or glioma (WHO grade II or III), (3) were able to complete neuropsychological testing, and (4) were medically approved to undergo MRI scanning (Aerts et al., 2022).
The dataset contained T1-weighted MRIs (T1w) and corresponding probabilistic tumor masks segmented by a combination of manual and automated delineation. Demographic and clinical information, including age, sex, smoking status, alcohol intake index (current and lifetime), tumor location and size, and handedness, as measured by the Edinburgh Handedness Inventory (Oldfield, 1971), are also provided (Aerts et al., 2022).
Cognitive performance was assessed in all patients in the dataset using the Cambridge Neuropsychological Test Automated Battery (CANTAB) (Aerts et al., 2022). The CANTAB is a computerized test battery for assessing various aspects of cognition, including information processing speed, attention, executive function, and working memory (Fried et al., 2021; Talebi et al., 2020). Before administering the main tasks, the motor screening task was employed to identify any sensorimotor or comprehension difficulties that might compromise the validity of data collection. Following this, the main tasks were conducted in a random order to prevent sequence bias (Aerts et al., 2022). Reaction time (RTI) is a subtask of CANTAB measuring attention and consists of simple (sim-RTI) and 5-choice RTI (5-RTI). The task required participants to react to the appearance of a yellow dot on the test screen and touch its location. The outcome measures of sim-RTI and 5-RTI were reaction time (RTI) and movement time (MT), respectively (Fujii et al., 2020; Kaser et al., 2022). For each of these four outcomes, the median (Mdn) and SD were computed over repeated testing. Subsequently, the eight RTI outcome measures were as follows: simple RTI Mdn and SD (sim-RTI-Mdn, sim-RTI-SD), simple MT Mdn and SD (sim-MT-Mdn, sim-MT-SD), 5-choice RTI Mdn and SD (5-RTI-Mdn, 5-RTI-SD), and 5-choice MT Mdn and SD (5-MT-Mdn, 5-MT-SD).
MRI and tumor mask preprocessing
From all participants, T1w structural MRI scans (160 slices, TR = 1750 ms, TE = 4.18 ms, field of view = 256 mm, flip angle = 9°, voxel size 1 × 1 × 1mm), were acquired with a Siemens 3T Magnetom Trio MRI scanner with a 32-channel head coil. The steps for preprocessing the T1w images and tumor masks for each patient are illustrated in Figure 2. For T1w, denoising and N4 bias field correction (Tustison et al., 2010) were performed using Advanced Normalization Tools (ANTs) (Avants et al., 2011), and brain extraction was performed using the HD-BET algorithm (Isensee et al., 2019). HD-BET was developed using MRI data from a large multicentric clinical trial in adult brain tumor patients and was thus designed to be robust with respect to brain tumors, lesions, and resection cavities across different MRI scanners and acquisition parameters (Isensee et al., 2019). According to Aerts et al. (2022), tumors were manually delineated based on the T1w images, and further automatically optimized using the Unified Segmentation with Lesion toolbox. First, thresholding and binarization were performed to transform the probabilistic tumor masks into binary masks suitable for subsequent analysis. A threshold of 0.5 was implemented. T1w was then normalized to MNI152 space through three-stage registration, beginning with affine and rigid linear transformations, followed by nonlinear SyN registration as performed by ANTs. To reduce registration errors introduced by the presence of tumors, two mitigation strategies were implemented: (1) cost-function masking (CFM) (Brett et al., 2001), which masked tumor areas during registration using the inverse of the tumor mask to limit registration to non-lesioned brain tissue, and (2) virtual brain grafting (VBG) (Radwan et al., 2021), which was used to generate lesion-free T1w for registration. The advantage of VBG is that it enables lesion filling in the presence of large or bilateral lesions or damage. This was achieved by generating a synthetic donor image that matched the input brain image to ensure that the filling tissue did not contain concomitant pathologies from the relatively non-lesioned side (Radwan et al., 2021).
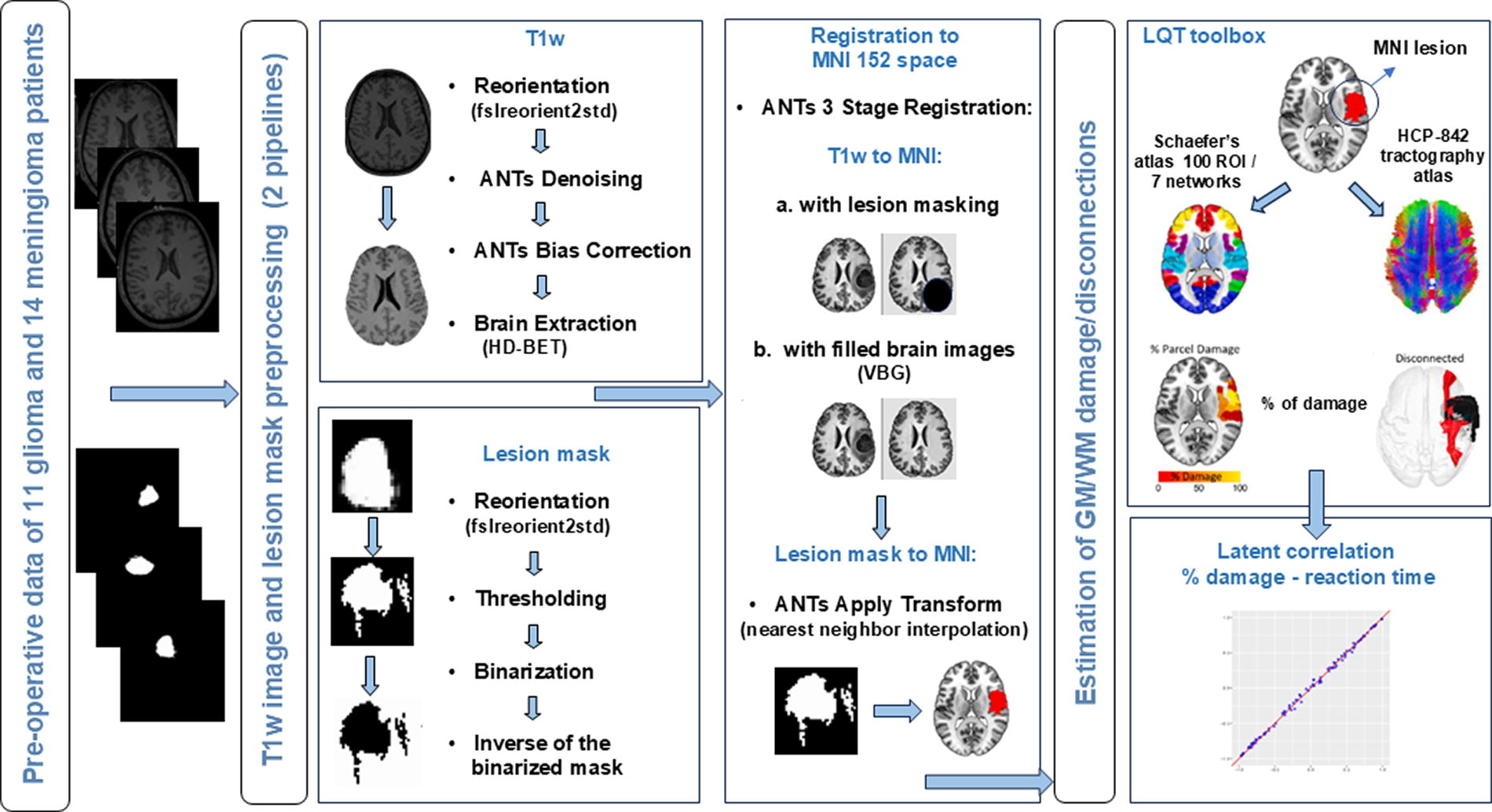
Pipelines for preprocessing and computing GM and WMT damage/disconnections.
Quantification of tumor damage
The structural impact of tumors was quantified with the Lesion Quantification Toolkit (LQT) (Griffis et al., 2021) using normative atlas-based metrics to estimate: (1) parcel-level GM damage, also referred to as lesion load, computed as the percentage of voxels within each GM parcel that overlapped with the lesion; (2) WMT-level damage or disconnection severity, calculated as the percentage of the total number of streamlines per given tract that intersects the volume occupied by the lesion (i.e., disconnected streamlines); and (3) parcel-wise disconnections, computed as the percentage of the total number of streamlines connecting each GM parcel pair whose trajectories intersect the lesion volume.
Reference atlases included Schaefer’s atlas (100 parcels, 7 networks) for the GM regions of interest (Schaefer et al., 2018) and the HCP-842 tractography atlas (Yeh et al., 2018) for the 70 canonical white matter fiber tracts (Fig. 2).
Statistical analysis
Correlations were computed between the estimated structural damage and RTI tasks. Parcel damage, WMT damage, and parcel-wise disconnection matrices generated by LQT were highly sparse because many brain regions within the corresponding atlases remained unaffected by individual tumors. Pearson’s correlation analysis is unsuitable for handling zero-inflated data because it violates the normality assumption (Yoon et al., 2021). Instead, latent correlations were estimated using the “latencor” R package, which can handle mixed data types through latent Gaussian copula models (Huang et al., 2021). The statistical significance of the computed correlations was estimated using permutation testing (1000 permutations). The false discovery rate (FDR) was used to adjust for multiple comparisons. p values below 0.05 were considered significant. Spearman correlations were also computed between RTI measurements and potential confounding factors, including age, tumor size (cm3), and current alcohol intake index.
Results
In the study, the average age of the participants was 55.9 years, with a SD of 12.5 years. The sample consisted of 60% females and 40% males. The cohort included 14 subjects with meningiomas and 11 with gliomas. A detailed breakdown of each group and individual participant information can be found in Tables 1 and 2, respectively.
Demographics and Clinical Characteristics
SD, standard deviation.
Tumor Location and Laterization for Each Participant
Handedness score is calculated using Edinburgh Handedness Inventory: –1, left-handed; 0, ambidextrous; +1, right-handed.
Among the 25 patients studied, 12 (48%) had tumors localized to the left hemisphere, 10 (40%) in the right hemisphere, and 3 (12%) exhibited bilateral involvement. The most common region affected was the frontal lobe (60%). The majority of patients (22 out of 25) were right-handed, as indicated by a handedness score closer to 1 (two patients had a score of 0.9, while one had 0.6). Two patients exhibited left-handedness or mixed-handedness, with handedness scores of −0.68 and −0.16. Left-sided tumors were predominantly found in right-handed individuals (44%), with a single left-handed individual having a same-side tumor (4%). Right-sided tumors exclusively occurred in right-handed individuals (40%). Bilateral tumors were less common but were observed in both right-handed (8%) and left-handed (4%) individuals.
The results obtained from the correlation analysis of the CFM and VBG pipelines are presented in Tables 3–5. Overall, both mitigation strategies produced similar results. The RTI measures were not significantly correlated with any of the measures of lesion damage. Furthermore, all significant results obtained were within the SD measures of MT for both sim-RTI and 5-RTI. No significant correlations were found between any RTI measures and age, tumor size, or alcohol index, as shown in Figure 3. An example of the results obtained from the LQT is shown in Figure 4.

Spearman correlations between potential confounding factors and RTI measures. The crossed-out values refer to correlation coefficients that were not significant. The alcohol index refers to the current alcohol intake. RTI, reaction time.
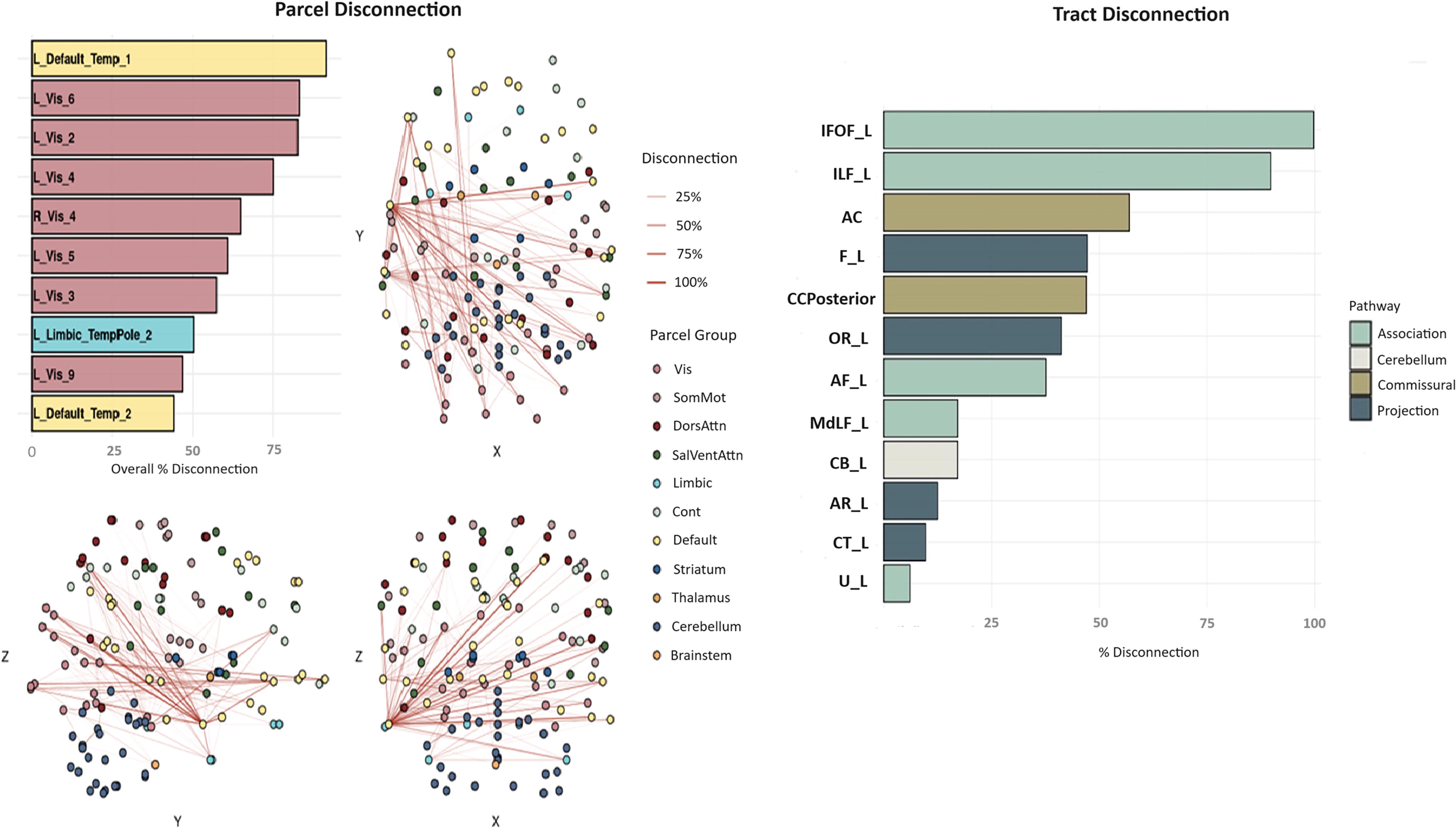
Illustrative example of percentage of parcel-to-parcel disconnection (left) and WMT damage (right) as computed by LQT. The barplot and brain network plots on the left illustrate the extent of disconnection at the parcel level for regions defined by the Schaefer’s atlas. The thickness of the lines between regions represents the percentage of disconnection between those regions. On the right, the barplot displays the percentage of tract-level disconnection for selected white matter fiber tracts as defined in the HCP-842 tractography atlas. LQT, Lesion Quantification Toolkit.
Significant Results of Latent Correlation Testing Between RTI and WMT Damage
p values were corrected across RTI measures for each tract.
CFM, cost-function masking; FDR, false discovery rate; IFOF-L, left inferior fronto-occipital fasciculus; UF-L, left uncinate fasciculus; U-L, left U-fibers; VBG, virtual brain grafting; WMT, white matter tract damage.
WMT disconnection and RTI
Damage to the left inferior fronto-occipital fasciculus (IFOF-L) and uncinate fasciculus (UF-L) was significantly correlated with RTI 5-MT-SD and sim-MT-SD for both CFM and VBG pipelines. The highest correlation was obtained between UF-L and sim-MT-SD, with a coefficient of 0.697 at a corrected p value of 0.035. The pipelines diverged for the left U-fibers (U_L), which only showed a significant correlation with 5-MT-SD when VBG was utilized for normalization. All significant results for the WMT damage correlations with RTI are shown in Table 3.
GM parcel damage and RTI
For the VBG pipeline, no significant correlations were found between RTI measures and GM parcel damage. For CFM, however, two parcels were significantly correlated with 5-MT-SD, namely, the left-hemispheric default mode network prefrontal cortex 2 (LH_Default_PFC_2) and the left-hemispheric ventral attention network frontal operculum insula 2 (LH_SalVentAttn_FrOperIns_2), as shown in Table 4.
Significant Results of Latent Correlation Testing Between RTI and GM Parcel Damage
p values were corrected across the RTI measures for each parcel.
LH_Default_PFC_2, left-hemispheric default mode network prefrontal cortex 2; LH_SalVentAttn_FrOperIns_2, left-hemispheric ventral attention network frontal operculum insula 2.
Parcel-to-parcel disconnection and RTI
For both pipelines, disconnections between the visual network and prefrontal cortical parcels were significantly correlated with the RTI 5-MT-SD. The strongest correlations for both VBG and CFM were with the left visual network 3 parcel (LH_Vis_3) and LH_Default_PFC_4, with coefficients of 0.778 (FDR-adjusted p value = 0.021) and 0.786 (FDR-adjusted p value = 0.007), respectively. Furthermore, the strong associations were also found with disconnections between the LH_Default_PFC_4 region and other subregions of the visual network, such as LH_Vis_4, LH_Vis_5, and LH_Vis_6, for both pipelines (detailed results are reported in Table 5). The CFM pipeline showed additional significant correlations with LH_Default_PFC_4 disconnections in the left caudate nucleus and left lenticular nucleus pallidum. Another significant correlation was with LH_Default_PFC_2 and the left-hemispheric default mode network temporal area 1 (LH_Default_Temp_1). All the significant results are displayed in Table 5.
Significant Results of Latent Correlation Testing Between RTI and Parcel-to-Parcel Disconnections
p values were corrected across the RTI measures for each parcel-to-parcel connection.
LH_Vis, left-hemispheric visual network.
Discussion
The purpose of this study was to investigate the correlations between measures of structural disconnections and CANTAB RTI in patients with tumors using an indirect atlas-based approach, in addition to comparing the results of two custom preprocessing pipelines designed to mitigate the effects of tumor pathology on MRI normalization. Overall, the CFM and VBG pipelines performed similarly across the LQT-produced measures; however, a greater number of significant correlations were found for the CFM pipeline.
Cognitive dysfunction, particularly attention deficits, is a common consequence of brain tumors in patients with meningioma and glioma (Chieffo et al., 2023; Meskal et al., 2016; Spina et al., 2023). Attention tasks are carried out through synchronous activity in multiple brain areas, with visual attention tasks largely controlled in a top-down fashion by the prefrontal cortex (PFC), including feature-based tasks, such as RTI (Bichot et al., 2019; Martinez-Trujillo, 2022; Paneri and Gregoriou, 2017; Rossi et al., 2009). This synchronized coupling between areas in the PFC and visual cortex enhanced perception through preparatory attention (Paneri and Gregoriou, 2017). Hence, the correlations found between RTI tasks and the disconnections between multiple subareas of the visual cortex and PFC cortex could be explained by this mechanism of control.
Furthermore, the correlations with the SD of the MT and GM damage in various frontal cortex subregions, such as the left-hemispheric default mode network’s (DMN) PFC and the left-hemispheric ventral attention network’s frontal operculum, suggest the frontal cortex’s role in regulating attention (Habets et al., 2019; Quirmbach and Limanowski, 2022). This relationship is evidenced by the observed variability in task performance, as reflected in the increased SDs of MT across repeated tasks.
The DMN, particularly the medial PFC (mPFC), plays a crucial role in modulating attention tasks. In healthy individuals, the DMN typically decreases its activity during attention-demanding tasks (Mancuso et al., 2022), allowing other networks like the visual and salience networks to dominate and focus on external stimuli (Menon, 2023). In brain tumor patients, disruptions in the DMN’s functioning can lead to difficulties in disengaging from internal thoughts, resulting in lapses in attention and reduced cognitive control. This impairment is especially significant as the DMN’s interaction with the visual and salience networks is vital for balancing internal and external stimuli (Bogler et al., 2017). When the DMN fails to adequately interact with these networks, patients may struggle with maintaining focus, experience slower reaction times, and have reduced accuracy in tasks requiring visual attention and salience detection. These deficits highlight the critical importance of intact network dynamics for cognitive function in brain tumor patients (Smolders et al., 2023).
All correlations were found with left-hemispheric structures, which is interesting given that visual attention tasks are typically lateralized to the right hemisphere in right-handed individuals (Serrien and O’Regan, 2022), who represent the majority of the participants in this study. However, there is recent evidence of a left-hemispheric role in attentive selection, specifically for recognizing objects with certain shapes and colors, which is in line with our results (Orlandi and Proverbio, 2019). Additionally, there was no clear pattern in the lateralization of tumors among the sample, as right-handed patients were nearly evenly distributed between having left or right-sided tumors. This suggests that factors other than hemispheric dominance may influence the impact of tumor location on cognitive functions.
Furthermore, a previous study (Arbula et al., 2017) investigated whether inhibitory impairments in brain tumor patients with left or right prefrontal lesions could be explained by associated cognitive processes like response selection and sustained attention. Findings indicated that patients with right prefrontal damage had issues with sustained attention, leading to omissions in Go/No-Go and target detection tasks, while those with left prefrontal damage exhibited both decisional and inhibitory impairments, resulting in high false alarm rates, highlighting the PFC’s role in maintaining cognitive control and the role of both hemispheres in attention-based tasks.
Similar findings were demonstrated (Campanella et al., 2016), in which the left PFC is essential for switching between quick and accurate responses, highlighting its role in cognitive flexibility in brain tumor patients. This finding is consistent with our results, where damage to the left PFC was associated with lower and more variable performance across tasks, emphasizing the importance of this region in managing attentional control and decision-making processes. Moreover, understanding these deficits can have significant clinical implications, as identifying and addressing PFC damage and its disconnection from the visual cortex may improve therapeutic strategies and present new targets for neuromodulation (Hamer and Yeo, 2022).
Correlations were also found with WMT damage, specifically IFOF-L and UF-L damage. The IFOF-L, which connects the occipital, temporal, and frontal lobes, and UF-L, which links the anterior temporal pole with the PFC (Bullock et al., 2022), converge in the inferior frontal lobe (Hau et al., 2016; Kier et al., 2004). The IFOF-L is particularly important for tasks requiring visual concentration and planning visually-guided movement (Debenedictis et al., 2021), such as the Go/No-Go task, where it plays a role in inhibition and controlled responses (Gonzalez Alam et al., 2024). The UF-L plays a key role in emotional regulation and decision-making (Wang et al., 2018), contributing to attentional control by linking the frontal and temporal lobes (Liu et al., 2020; Papagno et al., 2011). Recent studies also suggest its involvement in visual attention span and visual working memory (Zhao et al., 2022). These overlapping functions and anatomical proximity could imply that disruptions in either tract can lead to similar deficits in attention and reaction time (Krogsrud et al., 2018; Von Der Heide et al., 2013), especially in conditions affecting these pathways, such as brain tumors or other neurological disorders.
Owing to the limited number of participants, partial correlations, including potential confounding factors as covariates, were not performed. Performing partial correlations on a small sample size is problematic because it can lead to increased sampling variability and a higher likelihood of Type I and Type II errors, making the results unreliable. Additionally, small samples are more susceptible to the influence of outliers and may not accurately represent the larger population, reducing the generalizability of the finding. Nevertheless, we did investigate the association between RTI measures and several covariates available for this dataset. CANTAB measures have been found to be significantly correlated with age (Buján et al., 2022), and performance decline has also been associated with alcohol consumption (Devenney et al., 2019; Irwin et al., 2013). However, age and current alcohol index were not significantly correlated with any RTI measure in this study. Our results suggest a positive correlation between alcohol intake and brain tumor size, possibly due to alcohol’s impact on brain volume and white matter integrity (Daviet et al., 2022). Alcohol consumption has been linked to brain atrophy and may influence tumor growth through mechanisms like immunosuppression and increased oxidative stress (Anand et al., 2023). This association highlights the potential for alcohol to exacerbate neurological conditions, including increasing the size or aggressiveness of brain tumors. However, the relationship between alcohol consumption and tumor characteristics remains complex, and further research is needed to clarify these associations and understand the underlying biological mechanisms (Cote et al., 2021; Shu et al., 2023).
This study has several limitations. The sample size is small, significantly limiting the statistical power of the findings. Small sample sizes increase the likelihood of Type II errors, where true effects may go undetected due to insufficient statistical power. This limitation can lead to unreliable results and reduced generalizability, as the findings may not accurately represent the broader population. Due to the small sample size, we were unable to include detailed clinical data, such as tumor grade, in our analysis. This limitation prevents a comprehensive understanding of the differential cognitive impacts of low-grade versus high-grade tumors, as these grades can significantly differ in their progression and effects on brain function.
While indirect structural disconnection mapping offers valuable insights, caution is required when interpreting results, especially in patients with brain tumors. Both meningiomas and gliomas can displace surrounding structures during their growth, a factor not fully accounted for by indirect methods (Hanna et al., 2023; Lipková et al., 2022). Gliomas, which originate from glial cells, are often infiltrative and can aggressively invade surrounding brain tissue, rather than completely interrupting it, complicating the assessment of true disconnections. In contrast, meningiomas arise from the meninges and generally grow as well-demarcated masses that displace rather than interrupt WMT, potentially biasing the estimation of neural network integrity and cognitive correlations. Thus, to encapsulate the complex and multifaceted nature of these disruptions, we use the term “disconnectome.” This term reflects the nuanced interplay between structural disconnection and functional impairment caused by both displacement and infiltration of neural structures.
Furthermore, the results of an investigation by Silvestri et al. (2022) showed differences between the direct and indirect mapping of structural disconnections in patients with glioma. Tractography methods have their own shortcomings (Yeh et al., 2021) and thus require further investigation.
In conclusion, these results highlight the importance of investigating structural disconnections occurring in brain tumors and their association with cognitive performance in these patients. While indirect mapping offers certain advantages, future studies should investigate cognitive functioning with respect to both direct and indirect measures to further assess the reliability and consistency of these methods. Moreover, larger study cohorts will allow for more sophisticated statistical modeling, taking into account potential biasing factors.
Footnotes
Authors’ Contributions
B.M.T. designed and directed the project. H.Y. contributed to the design and implementation of the research and performed data analyses. H.Y. and B. M. T. interpreted the results and prepared the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Statement
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.