
Abstract
Objective:
Previous studies suggest that the combination of robot-assisted training with other concurrent tasks may promote the functional recovery and improvement better than the single task. It is well-established that robot-assisted rehabilitation training is effective. This study aims to characterize the neural mechanisms and inter-regional connectivity changes associated with robot-assisted parallel interactive training tasks.
Methods:
Twenty-five healthy young adults (12 females and 13 males) participated in three number-related cognitive-motor parallel interactive training tasks categorized by difficulty: low difficulty (LD), medium difficulty (MD), and high difficulty (HD). Functional near-infrared spectroscopy was used to measure neural responses in the primary sensorimotor cortex (SM1), supplementary motor area (SMA), and prefrontal cortex (PFC). Activation maps and functional connectivity (FC) correlation matrix maps were applied to assess cortical response and connectivity among channels and regions of interest.
Results:
Significant differences were observed in both activation and connectivity results across the three training conditions. Stronger activation (p < 0.01) in oxy-hemoglobin was found in the MD conditions, with activation in the HD condition being stronger than in the LD condition. The FC in the PFC increased linearly with rising training difficulty. Trends in FC for SM1 and SMA were consistent with the activation results.
Conclusions:
In parallel training tasks of varying difficulty, MD stimulates more neural activity and promotes stronger network connections in the brain. This study enhances the understanding of the neurological processes involved in robot-assisted parallel interactive tasks and may inform more effective robot-assisted rehabilitation therapies.
Impact Statement
This study aims to characterize the neural mechanisms and inter-regional connectivity changes of robot-assisted parallel interactive training tasks when coping with changes in task difficulty. It presented an initial increase in activation and connectivity, but a decreasing trend when the excessive load was involved. Moderate difficulty training may stimulate more neural activity and network connections of the brain because it is challenging and acceptable. Our results suggest a relatively optimal condition for the implementation of robot-assisted rehabilitation in terms of training difficulty. It may provide a reference for more effective robot-assisted rehabilitation therapy.
Introduction
The motor, sensory, language, cognitive, emotional, and other dysfunctions are caused by central nervous system (CNS) injury, of which motor and cognitive dysfunctions are the most common (You et al., 2023). These impairments can lead to reduced quality of life as patients are unable to self-care and their ability to participate in social and community activities is severely limited. The human CNS is plastic, and patients can stimulate their cerebral cortex to undergo functional reconstruction and reorganization of their damaged nerves with extensive and reasonably correct rehabilitation training after a nerve injury (Brigadoi et al., 2014). Movement recovery can be enhanced by the intensive, repetitive, and variable motor tasks of functional practice (Turner et al. (2013). Recovery of cognitive function is equally important. Activities of daily living involve cognitive planning and motor execution (Metzger et al., 2017). Cognitive training can improve executive function and task performance. Currently, most rehabilitation training in hospitals relies on physical therapists to provide long-term one-on-one assistance to patients (Dybvik & Steinert, 2021). The duration of traditional rehabilitation training is often shorter than the time required for optimal treatment outcomes, and treatment methods are based on relevant theory and therapist experience (Siddiquee et al., 2020). Manual-assisted training lacks objective measures of the patient’s condition and the reproducibility of the rehabilitation process. At the same time, the patient’s cognitive dysfunction leads to difficulties in communication and feedback, and cognitive function is not improved by training.
Compared with traditional therapy methods, robot-assisted training is a modern rehabilitation therapy technology based on the principle of neuroplasticity and the functional remodeling mechanism (Terranova et al., 2021), which can provide intensive, highly repetitive, task-oriented, and task-specific training with high precision and endurance (Hwang et al., 2012). It also increases a higher patient throughput by allowing multiple patients to be treated in parallel by a single therapist. To date, researchers have developed a variety of robotic devices for automated training tasks in the functional recovery of patients with CNS injuries (Aisen et al., 1997; Mayr et al., 2008). Robot-assisted rehabilitation is now widely used and clinically accepted (Chen et al., 2020; Mehrholz et al., 2015). A number of targeted, specific robotic devices that facilitate repetitive movements have been used to assist patients in rehabilitation tasks, such as the wrist rehabilitation robot (Bae et al., 2017b), and portable exoskeleton for hand and lower limb rehabilitation (Wang et al., 2018, 2021). Effective rehabilitation training modalities can enhance the activity of the relevant cerebral cortex (Calautti and Baron, 2003).
In recent years, nonimmersive virtual reality (VR) contextual human–computer interaction modalities have been increasingly used in rehabilitation robots. With the exploration of various rehabilitation modes, exergames have been applied in rehabilitation intervention and demonstrated their effectiveness (Reis et al., 2019). Cognitive-motor parallel tasks, namely cognitive-motor interventions, have been defined as dual-task (Bank et al., 2018; Uribe et al., 2022), VR exercises, cognitive exercises, or a combination of these. Cognitive-motor parallel tasks are interventions that combine a cognitive task with a physical rehabilitation task, for example, limb movement exercises together with cognitive exercises or performing dual-task exercises. A 2020 review (Gallou-Guyot et al., 2020) showed that positive effects of cognitive-motor dual-task interventions on cognitive, physical, and dual-task functions were observed in cognitively healthy older adults. VR game-based rehabilitation programs can facilitate the recovery of motor and cognitive function as well as increase the motivation to participate in patients with CNS damage (Arip et al., 2017). A Cochrane review (Laver et al., 2015) reported that a VR intervention to usual care resulted in improvements in upper limb function. VR has shown positive effects on cognitive function, motor function, and rehabilitation in general. The results of these parallel task studies seem to indicate that the combination of robot-assisted training and other simultaneous tasks (such as cognitive tasks or visual tasks) can promote the effect of rehabilitation training better than the single task, which may also explain why almost all rehabilitation robot systems on the market have supporting interactive modules (Park et al., 2020; Saita et al., 2018; Zhang et al., 2022). This may require a neurological explanation, but there has been limited research.
Most functional brain rehabilitation for neurological disorders involves the processing of external stimuli to induce activation of the cerebral cortex and remodeling of neural networks. During the rehabilitation process, it is important to monitor the connectivity and cortical activity in neurologically damaged brain regions because the nerve cells that transmit signals are damaged. When interactions between different regions increase, function can be restored by reorganizing neuroplastic connections and activating specific regions (Lee et al., 2020). Functional connectivity (FC) is defined as the temporal association between spatially distant neurophysiological events and can be detected by brain imaging techniques (Zheng et al., 2021). Functional near-infrared spectroscopy (fNIRS) is a noninvasive optical neuroimaging technique that uses light in the near-infrared spectrum (700–1000 nm) to detect hemodynamic response within the cortex during sensory, motor, or cognitive events. Functional NIRS has higher temporal resolution than functional magnetic resonance imaging (fMRI). In addition, fNIRS devices are portable, unobtrusive and relatively robust to motion artifacts, enabling the delineation of cortical correlates of realistic everyday tasks. Functional NIRS can detect activity in multiple brain regions simultaneously and allows for repeated monitoring over time. Therefore, fNIRS is expected to support the study of neural mechanisms underlying the effects of robot-assisted rehabilitation training (Leff et al., 2011).
The magnitude of the brain hemodynamic response can be modulated by the frequency, intensity, and/or complexity of the stimulation, possibly reflecting the demand for additional neuronal recruitment. However, at the point of supramaximal exertion, hemodynamic responses decline, reflecting CNS fatigue (Leff et al., 2011). Motor task performance and related neural activations may be influenced by the complexity of a concurrent cognitive task. Appropriate training intensity and difficulty contribute to motivation and effectiveness of rehabilitation. The study by Zheng et al. (2021) found that the parallel tasks showed overall stronger activation and connectivity in related cortical areas than the single task when the task was simple, and the diminished trend in activation and connectivity when participants were exposed to excessive demands on task difficulty. This may mean that while parallel training tasks yield better clinical measures, rehabilitation outcomes are not always positively correlated with task difficulty/intensity. Further research in this area is needed.
The brain area for executive function is mainly located in the prefrontal cortex (PFC) (Radel et al., 2017), which is closely related to the dorsolateral PFC. Robot-assisted movement starts in the visual system and transmits signals to the motor region of the cortex. The nerve impulse is generated in the primary sensorimotor cortex (SM1), and the impulse signal is transmitted down to the spinal cord to control the execution of muscle movements in the arm and hand. At the same time, SM1 and the supplementary motor area (SMA) are responsible for sensory and spatial guidance of upper limb movement and coordination of upper limb movement. Shi et al. (2021) found through fNIRS observation that when the upper limb rehabilitation training system was used to perform motor tasks, the activation of the SMA and the SM1 was higher.
Therefore, in this study, we aim to characterize the neural mechanisms and inter-regional connectivity alterations of robot-assisted parallel interactive training tasks when coping with changes in task difficulty. Multiple measures were used, including the extent of brain activation, and interacting networks between multiple regions of interest (ROIs) (the bilateral SM1, the bilateral SMA, and the bilateral PFC) based on measures of FC. We hypothesized that 1) higher difficulty tasks would correspond to more pronounced cortical activation; 2) the cognitive-motor parallel interactive task would enhance connectivity between cognitive and motor cortex areas in the cerebral hemisphere; 3) the PFC would be an important brain region involved in the cognitive-motor parallel tasks. It is hoped that the finding from this study will enhance our understanding of the underlying neural processes involved in cognitive motor interventions of robot-assisted rehabilitation.
Material and Methods
Participants
The sample size was determined by referring to relevant previous studies, that used between 10 and 30 participants when investigating fNIRS measures in response to robot-assisted training (Bae et al., 2017a; Shi et al., 2021; Wang et al., 2023). Twenty-five healthy participants with a mean age of 24.3 ± 1.7 years (12 females and 13 males) were recruited for this study. Further statistical validation was performed using G-power analysis which confirmed that our sample size was adequate based on the experimental parameters set for this study (when α = 0.05, power = 0.8, n = 16). All participants were right-handed as assessed by the Edinburgh Handedness Inventory (Oldfield, 1971). The participants did not take any practice tests before the formal experiment and completed the task for the first time. In addition, all participants met the following criteria: 1) normal vision or corrected-to-normal vision; 2) no limb movement disorder; 3) no neurological disease to exert influence on the experiment; 4) no brain structural abnormalities caused by brain tumors and/or external injuries; and 5) without significant cognitive and verbal dysfunction in Montreal Cognitive Assessment (MoCA) scores (Nasreddine et al., 2005). They were informed of the purpose and safety of the experiment. Written informed consent was obtained before the experiment. The study was conducted with the IRB approval of Shanghai University of Medicine and Health Sciences (2019-ZYXM-04-420300197109053525, 10.07.2019).
Procedure
To characterize the neural mechanisms and inter-regional connectivity alterations for coping with changes in difficulty of robot-assisted parallel training tasks, we conducted an fNIRS study in which participants were involved in three separates hemodynamic response during cognitive-motor tasks of varying difficulty, each consisting of parallel training tasks (VR cognitive and motor).
Referring to previous cognitive tasks, the VR cognitive task consists of three digital training tasks, the VR cognitive task included three numerical training tasks (Borst et al., 2012; Schmiedek et al., 2022; Träff, 2013), namely numerical comparison, numerical cognition, and numerical calculation. The motor task was the upper limb active training, which required participants to manipulate the handle, place the arrow on the correct answer and move to the specified position on the display. The upper limb rehabilitation robot (ArmGuider, ZD MedTech, China) was used to assist in both the upper limb motor and the cognitive parallel training tasks, which provided basic motor function training and multiple modes of VR cognitive function trainings.
The classification of cognitive task difficulty is based on the theory of Bloom’s six cognitive levels, which divides the learning process into six levels, from simple memory to deep creation, each level is based on the development and extension of the previous level, and our tasks correspond to three levels of understanding, application, and analysis. Regardless of cognitive processing or motion trajectory planning and operation, the workload of these three parallel training tasks gradually increased, so these three training tasks were successively designated as low difficulty (LD), medium difficulty (MD), and high difficulty (HD) according to the task category, operation time, and complexity. LD corresponds to the comprehension task in cognitive stratification theory, MD corresponds to the application task, and HD corresponds to the synthesis task. Participants were required to select the largest or smallest number from the five numbers within 100 according to the requirements on the display screen when performing the LD task, to count the number of given objects when performing the MD task, and to complete the calculation questions within 100 including four arithmetic operations of addition, subtraction, multiplication, and division when performing HD task. The motor trajectories of the three tasks were similar, ensuring that there was no difference between the motion tasks, but not exactly the same, because the sequence and direction of motion paths is random.
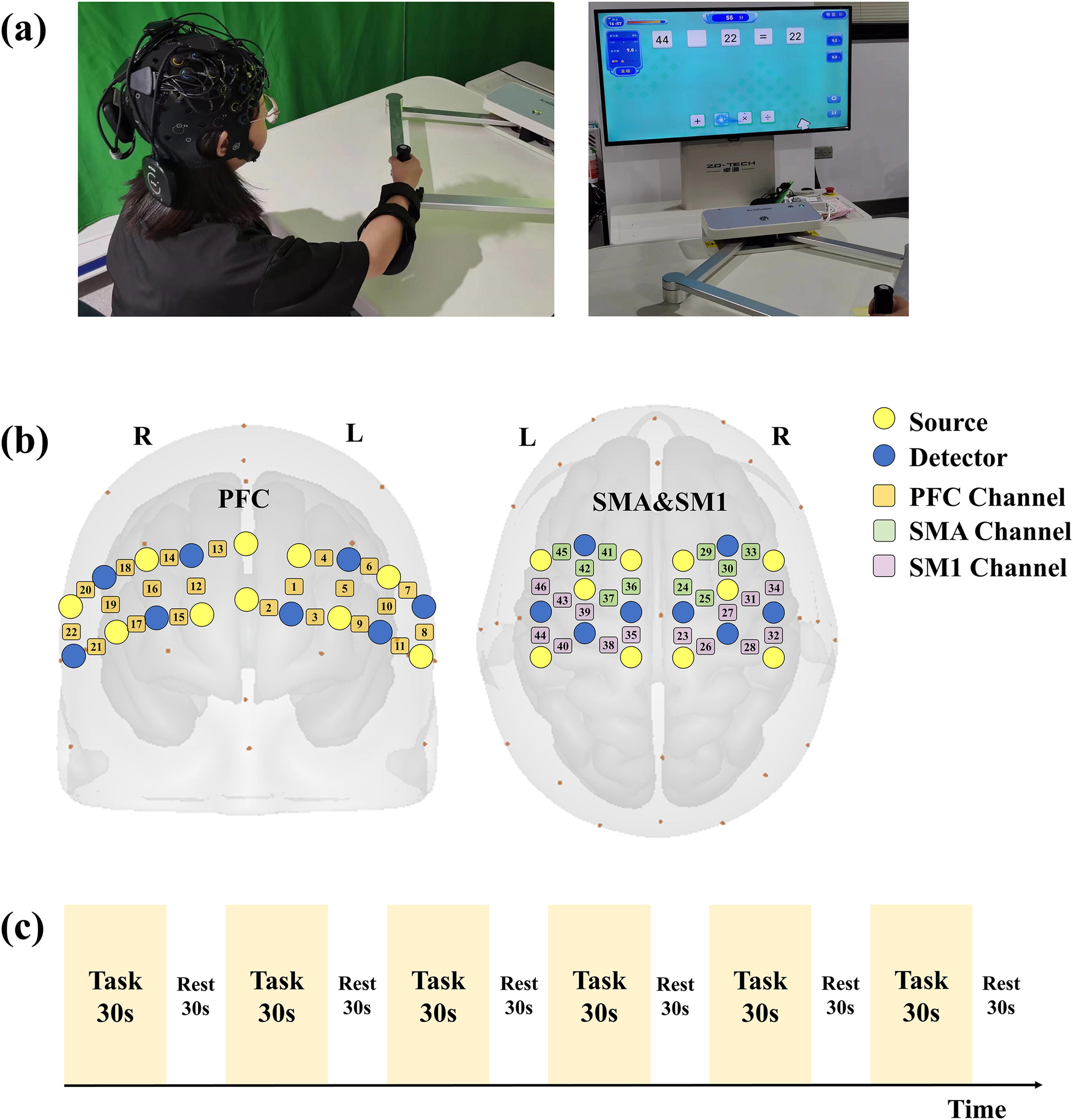
The experiment was conducted in a quiet and dimly lit room at a comfortable temperature. Each participant received about 10 min of training prior to the experiment to familiarize them with the experimental procedure, without covering the specifics of the experiment. Meanwhile, they were told some experimental attentions, including relaxing their body as well as avoiding physical activity other than their right arm, facial activity, frequent blinking, and looking around. During the experiment, the participants sat in a chair facing the upper limb rehabilitation robot display screen. The height of the work platform and the chair were adjusted to a comfortable position. The participants held the upper limb exercise training handle with their right hand, and the forearm was fixed to the support plate, as shown in Figure 1(a).
Experimental protocol.
An illustration describing the experimental protocol is presented in Figure 1(c). Each participant performed the LD, MD, and HD tasks in random order, and participants were not informed of the difficulty level of the tasks prior to the experiment. The experimental paradigm was organized in a block design. Each task consisted of six cycles after an adequate rest period. Each cycle was composed of a 30-sec task period and a 30-sec rest period. The staff gave verbal prompts in the experiment such as “start” and “rest.” During the task period, participants answered the questions on the display screen and manipulated the handle to move the answer to the correct position. Note that the participants remained in motion throughout the task. Although cognitively processing the on-screen questions, participants moved randomly within the movable area. During the rest period, participants rested with their eyes closed to avoid visual interference. They had to select the correct answer from several numbers on the screen. When an incorrect answer was moved to the specified position, a prompt appeared on the screen and that answer disappeared; participants had to continue selecting until the correct answer was moved to the specified position. A score of 5 was awarded for completing a question, and the total score for the corresponding training task was recorded after each completed training session.
Data acquisition and processing
Measurements
In this study, we used two identical continuous-wave fNIRS systems (Brite24, Artinis, the Netherlands) simultaneously. This product allows the use of two identical devices to form an extended system, which allows the coverage of more brain regions and is also more suitable for this study. The systems with a wavelength of 760 and 850 nm were used to record cortical activity from 46 measurement channels (CH) at 10 Hz. In total, 36 optodes with 20 sources and 16 detectors were arranged 3 cm apart to cover the ROIs. Figure 1(b) illustrates the selection of ROIs, cognitive and motor areas of the brain associated with the parallel training task were selected for this research, including the bilateral primary sensorimotor cortex (SM1) in the parietal cortex Brodmann area (BA) (BA1, 2, 3), the bilateral SMA in the frontal cortex (BA4, 6, 8), and the bilateral prefrontal cortex (PFC) in the prefrontal cortex (BA9, 10, 11, 45, 46) with respect to the Cz position of the international 10–20 system (Okamoto et al., 2004), were divided into six regions, the left PFC (lPFC, CH: #1–11), right PFC (rPFC, CH: #12–22), left SMA (lSMA, CH: #36, 37, 41, 42, 45), right SMA (rSMA, CH: #24, 25, 29, 30, 33), left SM1 (lSM1, CH: #35, 38, 39, 40, 43, 44, 46), and right SM1 (rSM1, CH: #23, 26, 27, 28, 31, 32, 34). The location of the optodes was marked with a 3D digitizer. The location information was then registered to the brain coordinates of the Montreal Neurological Institute to eliminate the differences in the shape and anatomy of the different brains.
Functional NIRS data processing
The fNIRS signals were obtained by converting the optical density changes into the relative concentrations of oxy-hemoglobin (HbO) and deoxy-hemoglobin (Hb) using the modified Beer-Lambert law and the age-dependent differential path length factor, which corrects the path length of light during the measurement (Delpy et al., 1988). Because Hb data are unstable, showing the opposite trend of HbO data in some studies (Schroeter et al., 2002), and some studies show that the results of Hb are not significant, we chose the HbO level as a marker of cortical activity during fNIRS data analysis. HbO is a more physiologically accurate notation. HbO is the most sensitive indicator of changes in regional cerebral blood flow and has the highest signal-to-noise ratio (SNR) (Lloyd-Fox et al., 2010). The direction of the HbO change was the most consistent and similar to other studies (Leff et al., 2011; Wagshul et al., 2019).
The NIRS-SPM software package (KAIST, Daejeon, South Korea) (Ye et al., 2009) was used to analyze the fNIRS data in the MATLAB environment (The MathWorks, USA). The coefficients of variation (CV, in %) was used to evaluate signal-to-noise performance of each channels, which is a common procedure for multi-channel fNIRS measurements (Piper et al., 2014). A CV is defined as 100 times the standard deviation divided by the mean value, where the standard deviation and mean are calculated from all the unfiltered raw data. Measurement channels with a CV exceeding 15% were removed (Kenville et al., 2017). Unknown global trends exist in the measured data due to respiratory, cardiac, vascular motion, or other experimental errors. At the same time, cross-talk may introduce additional noise, increasing the volatility of the signal and thereby reducing the correlation between signals. By using data filtering techniques to remove noise and outliers, the interference of cross-talk on correlation analysis can be reduced. To eliminate the global trend and improve the SNR, the hemodynamic response function (HRF) and the wavelet-minimum description length were employed (Jang et al., 2009; Tak et al., 2011). The canonical HRF is preferred to smooth the time-series data because the transfer function of the HRF lies in the frequencies of the modeled neural signals. A low-pass filter based on a typical HRF is used to remove high-frequency noise, and an algorithm based on wavelet transform is used to remove motion artifacts. The general linear model (GLM) was used to analyze the changes in the relative concentration of HbO in the cerebral cortex under the training condition (Ye et al., 2009). GLM is a statistical linear model that explains fNIRS data as a linear combination of an explanatory variable (i.e., regression coefficients) plus an error term. It can be formulated as:
Functional connectivity
The Pearson correlation coefficient was used for FC analysis. The HbO data of all participants during the task epochs were arranged by channel or ROI, and the Pearson correlation coefficient matrix between channels or ROIs was calculated. To calculate the Pearson correlation coefficient, the time series is randomly shuffled. By calculating the correlation of variables at different points in time it is possible to determine whether there is a lagged relationship between them and, based on time series data, it is possible to reveal the causal relationship between time variables. In this case, the maximum relevant time delay and the magnitude of the correlation can provide information about the flow of information between brain regions. These interactions have the greatest impact at a particular time delay, and all have significant values in the lag, indicating that a complex bidirectional interaction occurs. Zero-lag refers to two signals being perfectly aligned in time, with no time delay. However, in the case of zero-lag, it can be used to assess the linear correlation between two time series at the same point in time. Zero-lag correlation analysis can be seen as a special case of the Pearson correlation coefficient in time series analysis. We also applied AR filtering to the data, which can eliminate autocorrelation in the time series, thereby removing zero-lag and ensuring the accuracy of the data. Fisher’s z transformation was used to convert the correlation coefficients into a normally distributed variable for parametric statistical analysis. The formula is as follows:
Statistical analysis
The relative concentrations of HbO during the task period were calculated across three training conditions and six ROIs. Statistical analysis was performed using SPSS 26.0 software. The Shapiro–Wilk test was applied to test the normality of the data, and Leven’s Test was employed to verified the homogeneity of variance. And when normal distribution was detected, then it was analyzed by one-way ANOVA. The β value of the corresponding channel in each ROI represented the degree of activation of each channel. According to the previous ROI division, one-way ANOVA was applied to determine whether there was a statistically significant difference among the three conditions (p < 0.05). To address the issue of multiple comparisons, the least significant difference method was applied, rejecting the null hypotheses of no difference when p values were less than 0.05.
Results
We recorded the performance scores of 25 participants under three training conditions. The average scores were 129.5 for LD, 86.5 for MD, and 79.25 for HD. As the difficulty increased, the participants’ performance scores decreased significantly. As shown in Figure 2, the blood oxygen response curves were different for different task conditions. The oxygen response curves for LD are shown in Figure 2(a), the oxygen changes for MD are shown in Figure 2(b), and Figure 2(c) shows the oxygen changes for HD. Each task lasts a total of 360 sec. The average HbO relative concentrations during the task period under three training conditions and six ROIs are shown in Figure 3. The average response amplitude of the relative concentration of HbO showed an inverted U-shaped relationship with task difficulty, that is, as the task difficulty increased in, the HbO concentration had an initial tendency to rise, but as the task difficulty increased to HD, the HbO concentration had a tendency to fall. The result of the group analysis of the cortical activation levels is shown in Figure 4. The different activation levels of the cerebral cortex were observed when the participants trained along with three different conditions. In the MD training mode, the rPFC, rSMA, lSM1, and rSM1 showed relative maximum activation. The lPFC showed no significant activation in all three training conditions. In the LD training mode, the rPFC and lSM1 were more active, whereas in the HD training mode, there was a greater degree of activation in the right motor area and rPFC, and there was almost no activation in the lPFC. In combination with Figure 2, there is a significant difference in HbO relative concentrations between LD and MD, reflected mainly in lSMA.
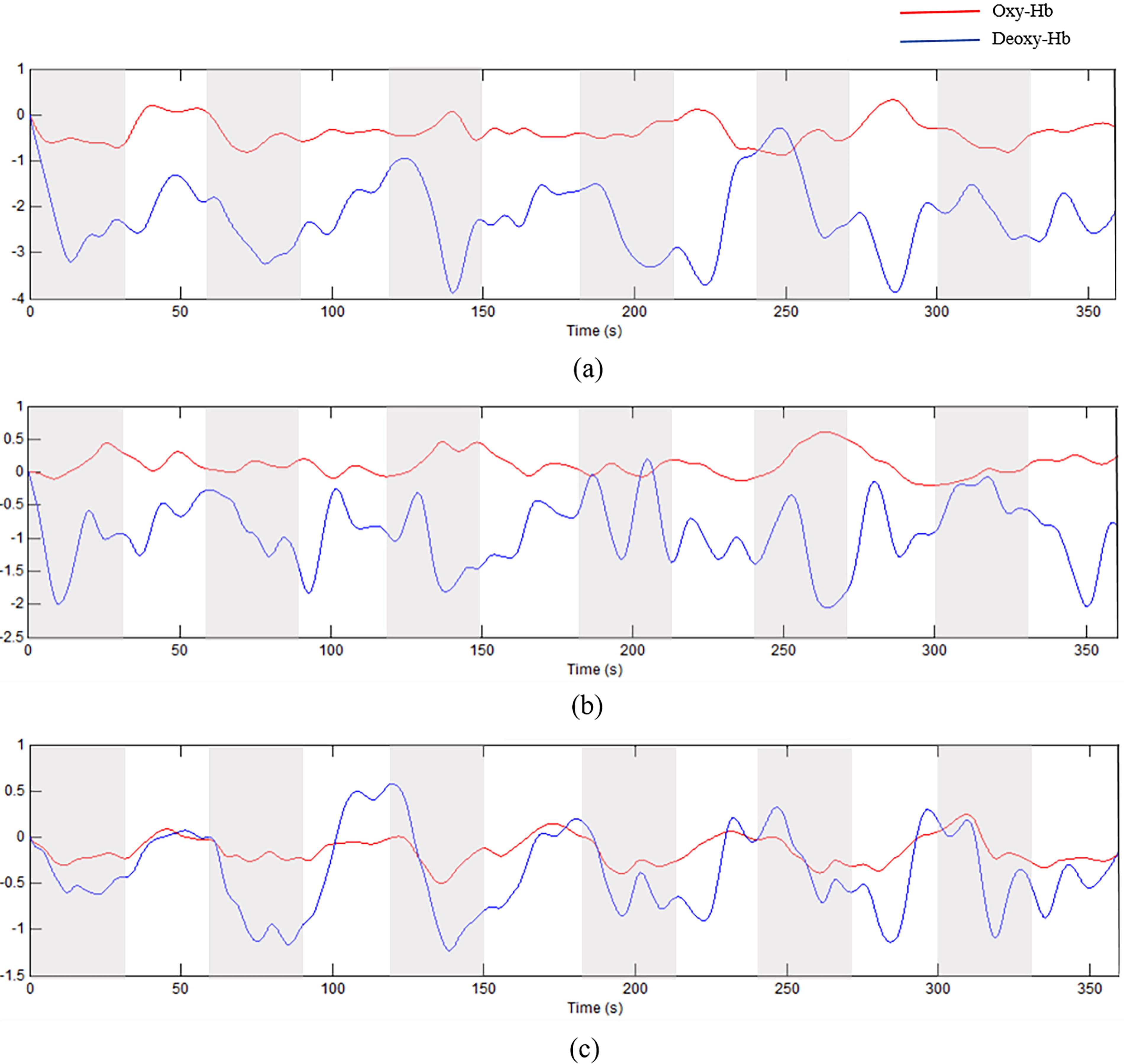
The oxygen response curves in relation to different task difficulties. Red lines represent HbO concentration, blue lines represent Hb concentration, and each block consists of a 30 sec task state and a 30 sec rest state, with gray representing the task state and white the rest state, and a duration of 360 sec.

The average changes of the relative oxy-hemoglobin concentrations (ΔHbO) during the task period in three training conditions and six regions of interest (ROIs). The “∗” indicates a significant difference. ∗p < 0.05.
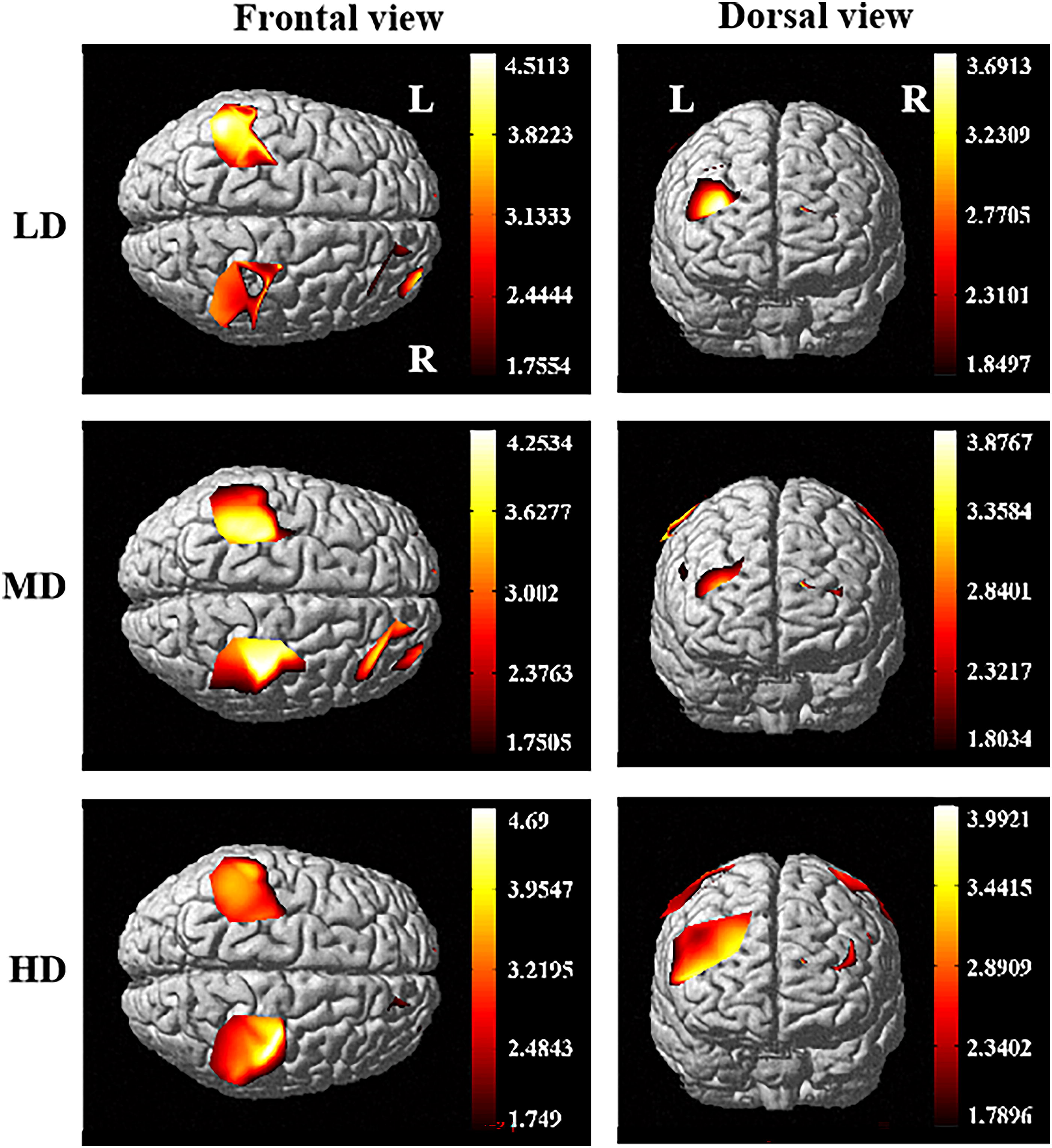
The group analysis result of the cortical activation levels shown from dorsal and frontal view. In the medium difficulty (MD) training mode, the rPFC, rSMA, lSM1, and rSM1 showed relative maximum activation. In the low difficulty (LD) training mode, rPFC and lSM1 were more active, whereas in the high difficulty (HD) training mode, there was a greater degree of activation in the right motor area and rPFC, and there was almost no activation in the lPFC.
The β values as regression coefficients, reflecting the response intensity of the blood oxygen signal of the whole time series, were collected and statistically analyzed. Each channel corresponds to one β value representing the activation level of the channel. The one-way ANOVA results of the β under three training conditions (LD, MD, HD) are shown in Figure 5. It can be seen intuitively that the fitting response intensity of the blood oxygen signal is the strongest in the MD condition. There were significant differences between LD and MD (F(7,193) = 1.188, p = 0.0017) and between MD and HD (p < 0.001). The comparison of the β values for each ROI across the three training conditions is shown in Figure 6. There were significant differences between LD and MD in lPFC (F(1,196) = 1.266, p = 0.023), rSMA (F(1,312) = 1.199, p = 0.004), whereas significant differences between MD and HD were observed in lPFC, rPFC, lSMA (lPFC: F(1,215) = 1.027, p = 0.003; rPFC: F(2,022) = 1.250, p = 0.001; lSMA: F(2, 652) = 1.475, p = 0.037) . The activation intensity of bilateral SM1 showed no significant difference between the three training conditions.
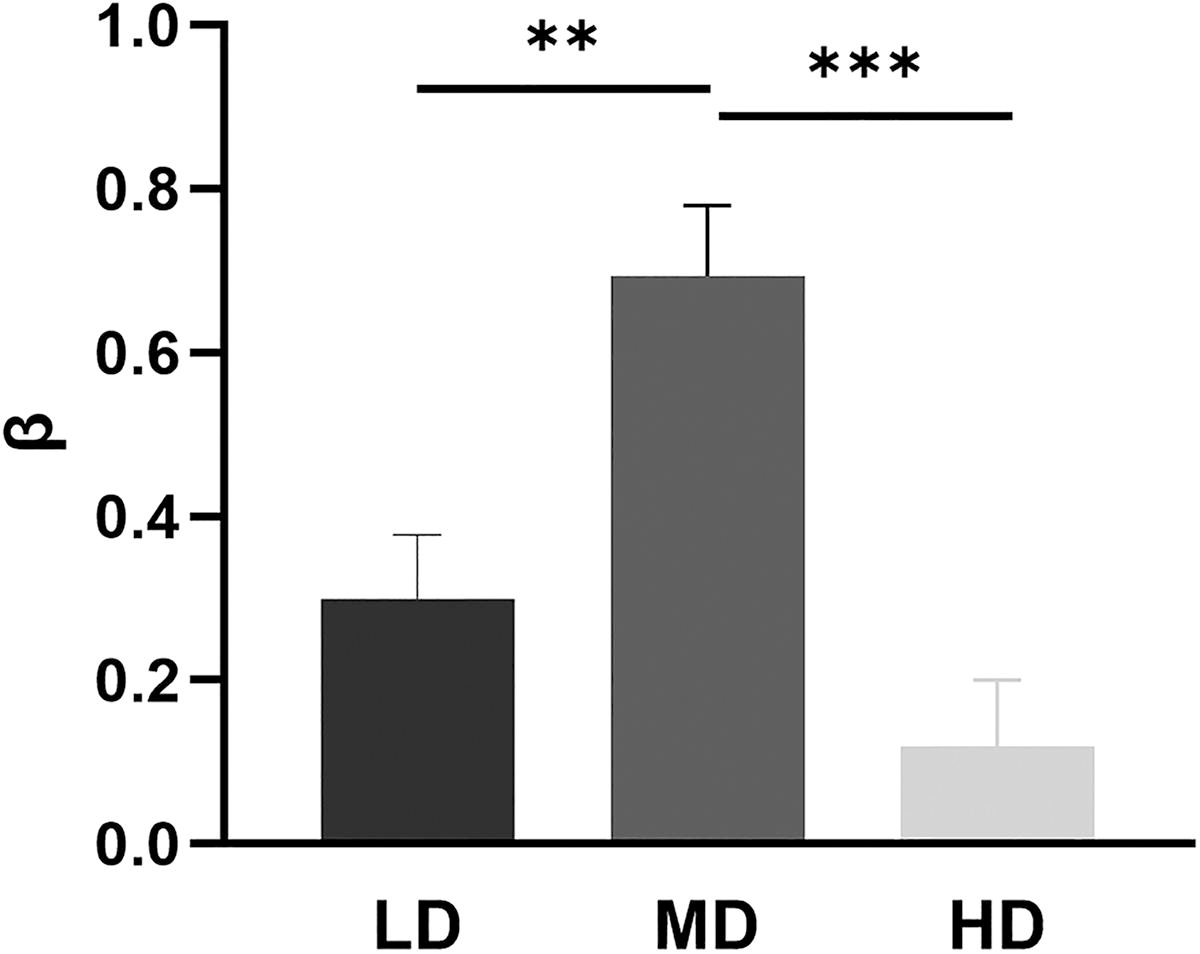
The cortical activation level of the β values under three training conditions (LD, MD, HD). There were significant differences between LD and MD and between MD and HD. The error bar in the figure represents the standard error of the mean. The “∗” indicates a significant difference. ∗∗p < 0.01, ∗∗∗p < 0.001.

The cortical activation level of the β values for each ROI in three training conditions. The “∗” indicates a significant difference. ∗p < 0.05. ∗∗p < 0.01.
Furthermore, we analyzed the temporal correlation between all detection channels and ROIs according to the HbO concentration of the processed time series, and the results are shown in Figure 7. The arrangement of the channels in the matrix follows the distribution of the ROIs. Each pixel value in the 46 × 46 matrix corresponds to a z-score value, which represents the correlation between two measurement channels. It can be concluded that the correlations between the channels were quite different in the three training conditions. With increasing difficulty from LD to MD conditions, there was a stronger correlation between channels and six ROIs. However, in the HD condition, the connectivity was lower than in MD, but still higher than in LD. ANOVA showed that the connectivity indices between channels and ROIs were significantly different in the three conditions (channels: F (2, 135) = 18.94, p = 0.0047; ROIs: F (2, 15) = 8.972, p = 0.0021).

The z-score map of functional connectivity (FC) analysis under the three levels of training difficulty.
Discussion
The present study focuses on investigating the performance of the cortical activation level and FC during robot-assisted parallel training tasks and aims to elucidate how neural activity changes with the variations in training difficulty. To this end, we used fNIRS to reveal the neural responses of healthy individuals during three number-related cognitive-motor parallel interaction training tasks by modulating the understanding and application of numbers at different levels of difficulty. The score performance result showed that the participant’s performance in the LD training was better than in the MD and HD training, and the performance in the MD training was also better than in the HD training. During the experiment, the performance in upper limb motor training slowed down with the rise in cognitive load and thinking time which led to the highest level of participants’ score performance in the LD training, and decreased with the increase in difficulty. However, the fNIRS response trend was not completely consistent with the task performance of the participants.
Cortical activation
The average changes in relative HbO concentrations in Figure 2 indicate higher hemodynamic responses induced by MD and HD training than by LD training. This is similar to the results of previous studies that tasks with higher difficulty levels correspond to more evident cortical activation (Lucas et al., 2020). However, in our study, the average HbO concentration was the highest in the MD condition rather than in the LD or HD conditions, especially in the PFC. According to the cognitive resource theory, task difficulty is related to mental workload and effort investment (Shuggi et al., 2017). When the stimulus or the task is more complicated, it will consume more cognitive resources, resulting in a stronger neural response in the task-specific brain region. Some studies have suggested that increased task difficulty may lead to greater recruitment of executive functions that are conducive to performing a more difficult task (Zheng et al., 2023); namely, a more challenging cognitive workload task evoked significantly greater hemodynamic responses (Csipo et al., 2021; Lucas et al., 2020). Nevertheless, when the individual’s cognitive load level is overloaded, cortical activity would show a lower activation pattern.
The different activation levels and varying degrees of fNIRS response may be related to the workload. The SM1 and PFC regions have been associated with task complexity and attentional resources of autonomous movement (Mandrick et al., 2013; Mirelman et al., 2014). The SM1 is implicated in information processing for the planning and execution of motor tasks (Grafton et al., 1998). The PFC, which is involved in motor learning and numerous cognitive functions (Ishikuro et al., 2014), has been strongly associated with executive functions such as working memory (WM) (Lucas et al., 2020). WM, as an executive function, consists of holding and processing information in the mind. Doing any kind of mental arithmetic requires WM. There are different degrees of complex cognitive processing prior to decision-making under different task difficulties. Thus, the activation and connectivity of PFC, SMA, and SM1 regions can effectively reflect the effect of parallel training tasks from the neural dimension (Zhang et al., 2023).
According to the compensation-related utilization of neural circuits hypothesis (CRUNCH), healthy adults use more brain regions to participate in activities with increased workload (mainly in the PFC) (Reuter-Lorenz and Cappell, 2008). However, the cognitive resource theory suggests that cognitive training gains may be abolished by cognitive overload and mental fatigue. Our activation results supported this theory and showed an inverted U-shaped relationship between task difficulty and hemodynamic responses, as represented by an initial increase in HbO concentration and a lower active level at higher demands on the cognitive resources (Sevcenko et al., 2022; Zheng et al., 2021). Since the tasks were performed by the right arm, the inverted U-shaped effect was more pronounced in the contralateral left hemisphere. Figures 3 and 4 show that activation and average HbO concentration were the highest under MD conditions. And according to the statistical results in Figures 5 and 6, the β values in the MD condition are higher than those in the LD and HD conditions. The low activation mode under LD training in the PFC can be explained by the fact that cognitive resources were not fully utilized. However, the high activation mode under MD training did not mean that cognitive resources were fully utilized. It should be noted that only three levels of difficulty training were used in the experiment, and the most favorable level of difficulty may not have been discovered in parallel training.
Figure 4 illustrated that SM1 and SMA were significantly activated during the cognitive-motor interaction parallel training tasks at three difficulty levels. The activation of PFC showed a significant right hemisphere laterality, the activation of the PFC, which is one of the key parts of higher cognitive function and is the main part of the human brain primarily responsible for thinking and computing, showed significant right-hemisphere laterality. A meta-analysis reported that cognitive training increased neural activation and had broad effects on brain activation, whereas some findings already indicated that numbers could activate a widespread right neural network (Yeo et al., 2017). The bilateral inferior parietal regions, the right-lateralized network of superior parietal, and the superior and inferior frontal regions were involved in functional specialization for processing visually presented numbers (Dai et al., 2023; Yeo et al., 2017). The similar activation network and the apparent right lateralization of the PFC were observed in three training conditions in our activation map.
The fNIRS responses under the three training conditions generally showed positive activation, whereas the β results observed the negative activation of the PFC in the Figure 6, which may be due to increased deoxyhemoglobin and decreased oxyhemoglobin during the task period in part of the time series (Sato et al., 2005). This inverse oxygenation response is generally related to the task mode and task complexity (Abdalmalak et al., 2020; Holper et al., 2011). It has been observed more frequently during simple versus complex tasks, whereas the more complex task would produce a stronger negativity of the oxygenation response. In our study, there was a higher degree of inverse oxygenation in the lPFC region during the HD task than the LD task. However, the inverse oxygenation occurs mainly in the PFC region under the three training conditions, without task specificity. As a technical reason, anatomical individual variability and the limitation of the usually limited fNIRS sample volume (Holper et al., 2011) may have led to differences in the exact location of the sampled tissue from subject to subject when relying on a 10–20 template to define probe locations. Another explanation is that, as a mental task, the cognitive process of motor planning and inhibition may cause changes in heart rate and respiratory rate, so the vascular response caused by the autonomic nervous system during rest periods may affect the task-related signal changes. In addition, one study has shown that a likely cause of the inverse oxygenation detected by fNIRS during motor imagery is due to participants’ unintentional movement during rest periods (Abdalmalak et al., 2020), which may explain the unexpected response signals in the individual cycles.
Brain functional connectivity
Spontaneous neuronal activity causes fluctuations in blood oxygenation. Similarities in fluctuations between anatomically distinct cortical areas have been postulated to reveal FC. Changes in task-related networks may have functional relevance to dynamic cognitive processes (Cole et al., 2021). The FC of the brain has been considered as the temporal correlation between fNIRS measurement channels or between ROIs. Pearson correlation has been widely applied in fNIRS and fMRI studies to estimate FC at the resting state and to reveal how FC changes during specific cognitive processes (Tambini et al., 2010; White et al., 2009). It has been demonstrated that the strength of the FC between brain regions is sensitive to both the cognitive task load and state (Fishburn et al., 2014). From the results of the FC matrix of each channel, the channel connectivity of cerebral intrahemispheres is significantly stronger than that of inter-hemispheres. It indicates that the cognitive-motor parallel interactive task enhances the connection between the cognitive and motor cortex areas in the cerebral hemisphere, and may contribute to the neural reorganization of the brain functional areas. However, the FC of inter-hemispheres in SMA and SM1 is stronger than the FC of intra-hemispheres, which may be due to the SMA involved in motor control, learning and planning and motor activation of the hand with SM1. This conduce to support the research of healthy limb training to promote the recovery and connection of the affected side nerves (Huo et al., 2019).
Some studies have found that with the increase of task complexity and difficulty, the FC of the brain increases linearly with the growth of cognitive load (Fishburn et al., 2014; O’Connell and Basak, 2018). The executive function processes, including enriched environments, that provide physical activities with decision-making opportunities and is able to facilitate the development of both motor performance and brain functions. The FC change of bilateral PFC was consistent with the previous study at the ROI level. At the channel level, the FC of PFC in HD condition represents weaker but more extensive than in MD. Moreover, in the motor cortex, it showed stronger connectivity in the MD experimental tasks, whereas it was lower in the cases of LD and HD. The FC was stronger in the HD training condition than that in LD. As mentioned above, the reduction of the FC performance may be caused by excessive cognitive load and lower motor frequency.
The inverse activation observed in Figure 7 is generally related to task mode and task complexity (Abdalmalak et al., 2020; Holper et al., 2011). It was observed more frequently in simpler or more complex tasks, and more complex tasks produced stronger negativity of the oxygenation response, which is consistent with the findings of this experiment. In the lPFC, the HD task elicited a higher degree of inverse activation than the LD task. Across the three training conditions, reverse activation occurred primarily in the PFC region, with LD and HD eliciting stronger reverse activation and MD maintaining positive activation in the rPFC. As a technical reason, anatomical individual differences and the constraints of the usually limited fNIRS sample size may have led to errors in sampling positions across subjects when relying on the international 10–20 template to define optode positions (Holper et al., 2011; Steinmetz et al., 1989). An alternative explanation is that, as a parallel motor-cognitive task, the cognitive processes of motor planning and inhibition may induce changes in heart rate and respiratory rate, and thus, during rest, the vascular responses elicited by the autonomic nervous system may influence task-related signaling changes (Kempny et al., 2016).
A few limitations of this study should be noted. The experiment participants are a limited number of young and healthy people, which makes the sample size slightly small. The results may provide a reference for the brain activation and connectivity pattern of patients with nerve damage, but they may not be completely consistent. The experimental task involved visual guidance, although cognitive planning and motor execution played more of a role in the task. Since there is an interaction between visual information processing and motor control, we may be able to gain valuable information in the visual cortex. In the future, more cortical areas need to be recruited to better understand neural reorganization (Zheng et al., 2022). Another limitation is that we did not explore and analyze the effect of sex as a biological variable, and further studies should be conducted to reveal it. In addition, the difficulty range from LD training to MD training to HD training may be unbalanced; randomized task sequences may be necessary to further eliminate any potential biases. For clinical applications, it is necessary to investigate the optimal training conditions for cortical activation and FC of brain networks to improve the efficiency of robot-assisted rehabilitation based on the concept of brain plasticity. Future studies could further increase the complexity still further and use fNIRS to explore the activation and FC patterns of the cerebral cortex under more classified conditions.
Conclusion
Taken together, in exploring the better condition about difficulty of robot-assisted rehabilitation with parallel interaction training task, the stronger activation and connectivity were observed at a moderate difficulty training. It presented an initial increase in activation and connectivity, but a decreasing trend when the excessive load was involved. The training of moderate difficulty can stimulate more neural activities and network connections of the brain because it is challenging and acceptable. Our results suggest a relatively optimal condition for the implementation of the robot-assisted rehabilitation in terms of training difficulty. It might provide a reference for more effective robot-assisted rehabilitation therapy.
Footnotes
Acknowledgments
The authors gratefully acknowledge the financial supports by National Key R&D Program of China (No.
Authors’ Contributions
D.W.: Conceived and designed this experimental study. J.Z.: Collected and processed experimental data and summarized the experimental results. Y.H.: Analyzed the functional connection results. D.W.: Drafted and finalized the article. D.W. and Q.M.: Eventually approved publication. All authors agree to take responsibility for all aspects of the work.
Ethical Approval
This research will not cause any mental or physical harm to the subjects, and will not compromise their safety and rights. Written informed consent was obtained from all participants for this experiment, always observing the human subject’s right to privacy. The study was conducted with the IRB approval of Shanghai University of Medicine and Health Sciences (2019-ZYXM-04-420300197109053525, 10.07.2019).
Availability of Data and Materials
The data that support the findings of this study are available from
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose. The authors alone are responsible for the content and writing of this article.
Funding Information
The research was supported by National Key R&D Program of China (No. 2023YFC3604800).