
Abstract
Points of dispensing (PODs) are vital for responding to events that require mass chemoprophylaxis, such as bioterrorist attacks or pandemic influenza. This article evaluates the operational success of a large-scale dispensing drill for first responders and first receivers, focusing on differences in functioning of PODs by practice discipline and POD model. PODs were operated by either first responders (EMS, fire, or police) or first receivers (hospitals). Facilities could operate a centralized POD model, a decentralized POD model, or a combination, or “hybrid,” model. Evaluation consisted of having evaluators at every POD, conducting a survey of POD individuals, and reviewing retrospectively the medications dispensed during the drill. Throughput counts, satisfaction with POD functioning, and errors in medication dispensing at each site are reported by practice discipline and facility model. During the drill, 23 PODs successfully processed more than 4,000 individuals. Centralized PODs and first responder facilities had faster throughput times than hybrid and hospital facilities, but hospital facilities had a lower incidence of medication error. Nominal differences in patient satisfaction were found. Assessing a combination of throughput, medical errors, and patient satisfaction with first responders and first receivers as points of dispensing can provide valuable insight into the feasibility of providing chemoprophylaxis to first responders and first receivers in advance of POD operations for the general public.
POD Structure
Points of dispensing, or dispensing/vaccination centers (DVCs), are generally regarded as the most efficient way to rapidly distribute mass vaccinations or mass chemoprophylaxis.7,8 PODs are critical public health assets and are intended to be rapidly functional to distribute chemoprophylaxis in response to a bio-event, whether it be intentional (eg, bioterrorism) or not (eg, influenza pandemic). PODs were opened in New York City to distribute chemoprophylaxis to those exposed following the anthrax attacks in 2001, and they are being used to provide vaccine for the H1N1 influenza virus.
Though all PODs share a common goal of mass distribution of medications or vaccine, the strategies by which individual PODs accomplish these goals vary; however, 1 of 2 POD models is generally used.9-16 Many variations of the 2 model types exist, but generally the first, a decentralized model, is ideally suited for a hospital or other similar setting in which the individuals to receive prophylaxis are already in place. In this model, medications are loaded onto some type of conveyance, such as a cart, and are then taken to the individuals to receive prophylaxis by a trained medical dispenser.
In the second model, a centralized model, individuals who are to receive prophylaxis come from various locales to a centralized, predetermined location, where large numbers of people can receive prophylaxis in a short amount of time. Variations on this model include “drive-through” vaccination operations, in which individuals come to a centralized distribution center but do not get out of their vehicles or wait outside during potentially inclement weather to receive the necessary medications or vaccinations.
Operation RAPID
To exercise POD operations in Nassau County, New York, Operation RAPID (Responder Alert Prophylaxis Initiative Drill) was devised for Nassau County first responders, first receivers, and their families. They were to practice the process of opening and operating PODs at multiple sites. Operation RAPID simulated the airborne release of anthrax in Nassau County, a county with 1.3 million people, all of whom could potentially need chemoprophylaxis were such an event to occur. 17
A release of anthrax over Nassau County would have far-reaching public health implications. It is estimated that an airborne release of 50 kg of Bacillus anthracis over an urban population the size of Nassau County would be capable of infecting 105,000 persons and killing 30,000.18,19 During the 2001 anthrax attacks, the median delay between anthrax exposure and the onset of symptoms was 4 days. It can take from 2 to 6 days for victims of inhalation anthrax to die of the infection, thus affording public health officials, at best, a 6- to 10-day window to respond.20-27 However, the lag time between exposure and symptoms in individuals would make best-case scenarios unlikely, as the initial indication of an anthrax attack would probably not be the release of anthrax itself but individuals seeking treatment as they become symptomatic. Such a scenario would shorten the window of time available to public health officials to mount an effective chemoprophylaxis campaign. 20
If such a release were to occur, the Nassau County Department of Health would first provide chemoprophylaxis to first responders and first receivers, who would need to receive prophylaxis to serve in their official capacity and protect the community. Additionally, chemoprophylaxis would be provided to their families, so that first responders and receivers would be able to continue working, with the assurance that their loved ones were safe.28,29 In Nassau County, this group is made up of an estimated 13,500 first responders, 35,000 first receivers, and 117,000 family members.
As part of Operation RAPID, 23 first responder and first receiver facilities (composed of fire departments, police stations, and hospitals) opened PODs. Each facility participating in Operation RAPID could elect to host centralized PODs, decentralized PODs, or a combination of both POD types (hereafter referred to as “hybrid” facilities) (Figure 1). Hospitals often employed a hybrid model: at least one decentralized POD was used to distribute medication to staff unable to leave their posts, while a centralized POD was simultaneously opened at a central location for other staff in the facility and for off-duty workers and their families. First responder disciplines employed only the centralized model.
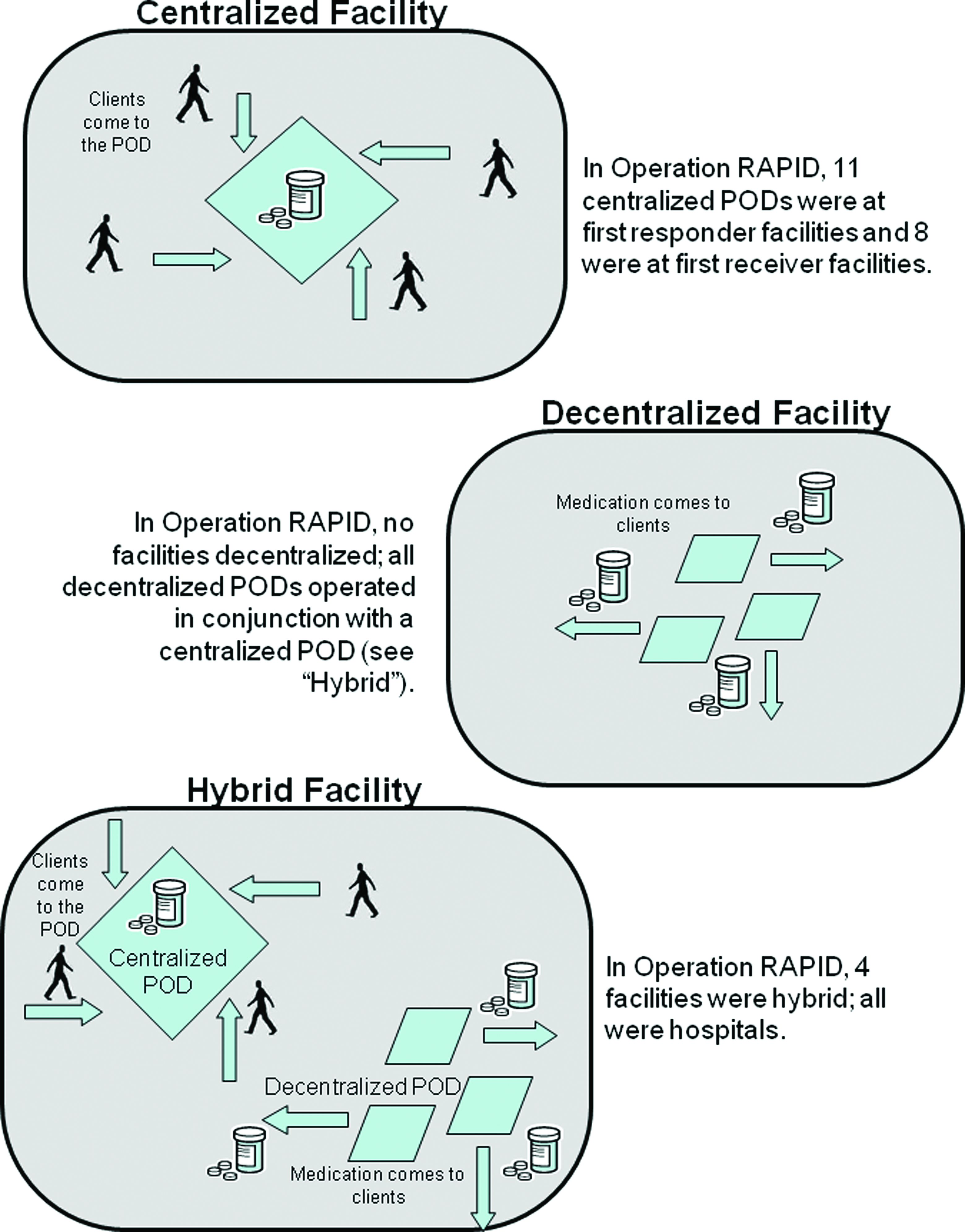
Points of dispensing by type. Color images available online at www.liebertonline.com/bsp.
Because Operation RAPID focused primarily on the process of opening first responder and first receiver PODs, and because it combined different practice disciplines and different POD models, we sought to assess the effectiveness of the different types of dispensing sites available for use in Operation RAPID (hybrid and centralized), as well as to assess differences in POD functioning between the different first responder and first receiver disciplines (ie, fire, police, hospital personnel). Effectiveness was measured through total throughput counts, satisfaction with POD functioning, and errors in medication dispensing at each site. Previous studies of similar POD operations have focused primarily on throughput capabilities,29-33 and none of these studies has systemically quantified medication error rates. We sought to expand on these previous studies by including a quality assurance component, achieved through the evaluation of patient satisfaction and medication errors.
Methods
Drill Development
Operation RAPID was conceived and developed by an interdisciplinary team that included representatives of the Nassau County health department, all 9 fire department battalions in the county, the fire marshal's office, the fire and EMS academies from the vocational education and extension board in Nassau County, the police department and the sheriff's department, the county office of emergency management, all 12 hospitals in the county, and the New York Consortium for Emergency Preparedness Continuing Education (NYCEPCE). Operation RAPID was the culmination of multiple training sessions conducted by the team in advance and just-in-time training. Advance training sessions such as those conducted by the Operation RAPID team have been demonstrated to be a critical element in rapid dispensing of chemoprophylaxis on the day of an actual exercise.29,30,34,35
Drill Implementation
Operation RAPID began with the activation of the county emergency operations center (EOC) and the subsequent call for the opening of the PODs. A total of 23 PODs were opened and operational for the exercise. Nineteen PODs were centralized; of these, 11 were operated by first responders (fire, EMS, or police), and 8 were operated by hospitals. Four PODs were decentralized, all of which were housed in hospital facilities that also employed a centralized POD, resulting in 4 facilities using a hybrid dispensing model (Figure 1).
Each POD placed a request to a central dispensing site for the needed medications and began operating once medications were received. Individual first responders and first receivers and their families were notified to report to their respective PODs (or to expect a visit from the POD medication cart), where they completed the medical dispensing forms and process, based on the real responses they would provide in an actual event.
Since one of the goals of Operation RAPID was to have first responders and receivers become able to operate nearly self-sufficient PODs for themselves and their families, first responders and receivers were used in most roles. In addition, members of the Nassau County Medical Reserve Corps (MRC) were stationed at each POD as medical consultants. PODs were given the option to have MRC members in additional roles, and 1 POD did so.
Exercise Evaluation
To evaluate the exercise, participants were asked to complete a 42-item survey rating various aspects of the entire dispensing process. Two of the survey items focused specifically on throughput, asking individuals to rate how long it took them to complete the sign-in and registration process and how long it took them to complete the rest of the dispensing process once registration was completed.
Trained evaluators also observed the exercise, with several evaluators in place at each POD. The evaluators completed evaluation packets, including time study sheets and observation checklists. The time study sheets did not track individual patient flow but rather charted when individuals began arriving at the PODs and when the last patient left the PODs, and they provided a total count of people who had gone through the PODs throughout the day.
Evaluators with medical backgrounds also conducted a chart review at the completion of the exercise. Based on the responses participants gave on their registration forms (eg, age, gender, weight, pregnancy status, allergies, possible drug interactions), the medical evaluators compared the medication dispensed to individuals to the county health department's protocol to determine if the appropriate medications and amounts had been dispensed.
The exercise was evaluated by evaluators from the University of Kansas School of Medicine–Wichita (KUSM-W). The evaluation tools and overall project were approved by the Human Subjects Committee at KUSM-W.
Results
A 2-tiered approach was used to evaluate the results. First, overall POD functioning was assessed by measuring throughput, patient satisfaction, and medication error rates. These overall POD functionality results were then compared by practice discipline type and by POD model type.
Overall POD Functioning
Operation RAPID began at 9:00
POD Throughput
A total of 4,246 individuals were seen in 23 PODs, with 18 sites reporting (78% site response rate) throughput data on 1,010 individuals. Of these 18 sites that reported throughput data, 11 were first receiver facilities and 7 were first responder facilities. Average processing time of individuals was 0.68 per minute, or 40.62 people per hour (Figure 2). These processing times varied by practice discipline and model type. The 7 first responder facilities reported processing an average of 0.99 individuals per minute (standard deviation 0.488), or 59.60 individuals per hour (standard deviation 29.308). The 11 hospital facilities reported processing an average of 0.47 individuals per minute (standard deviation 0.380), or 28.33 individuals per hour (standard deviation 22.827). On average, facilities using a centralized POD processed 0.75 individuals per minute, or 45.169 individuals per hour. Hybrid facilities processed an average of 0.48 individuals per minute, or an average of 28.805 individuals per hour.
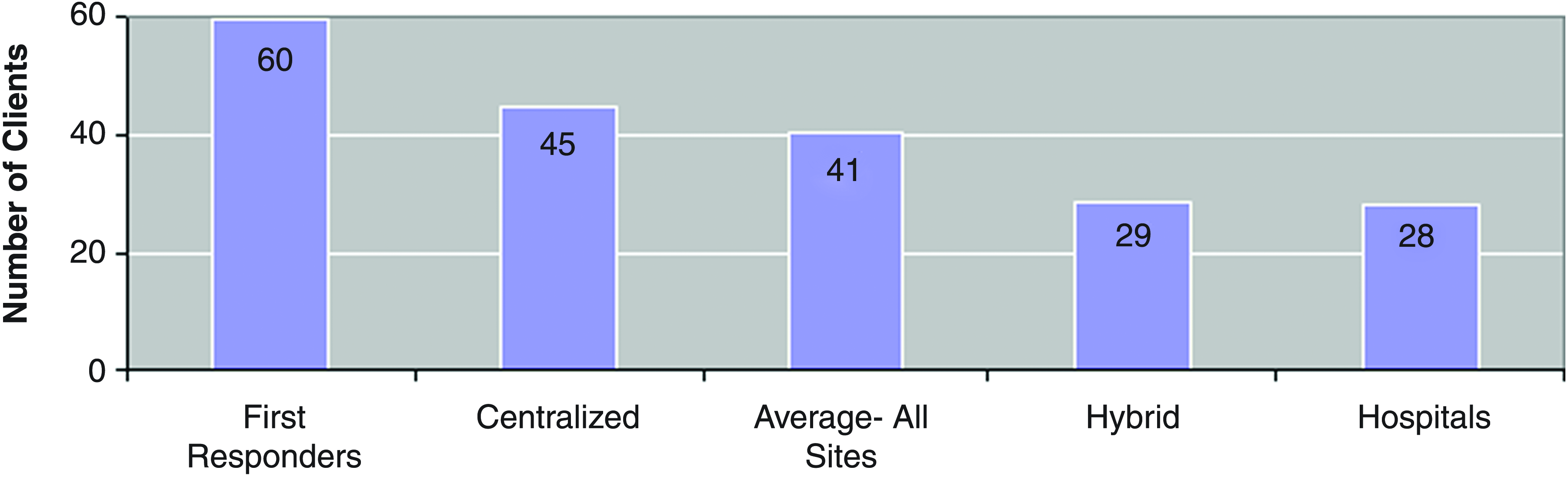
Average number of clients through PODS per hour by subgroup. Color images available online at www.liebertonline.com/bsp.
Of the 4,246 people who participated in the exercise, 1,181 (28%) returned completed postexercise evaluations rating their experiences throughout the dispensing process. Using 5-minute increments, individuals estimated their total time spent completing POD registration and the time required to finish the dispensing process following registration: 36% of individuals reported taking approximately 5 to 10 minutes from arrival at the POD to having completed registration, and 39% reported taking 5 to 10 minutes from completed registration to exiting the POD (Figure 3).
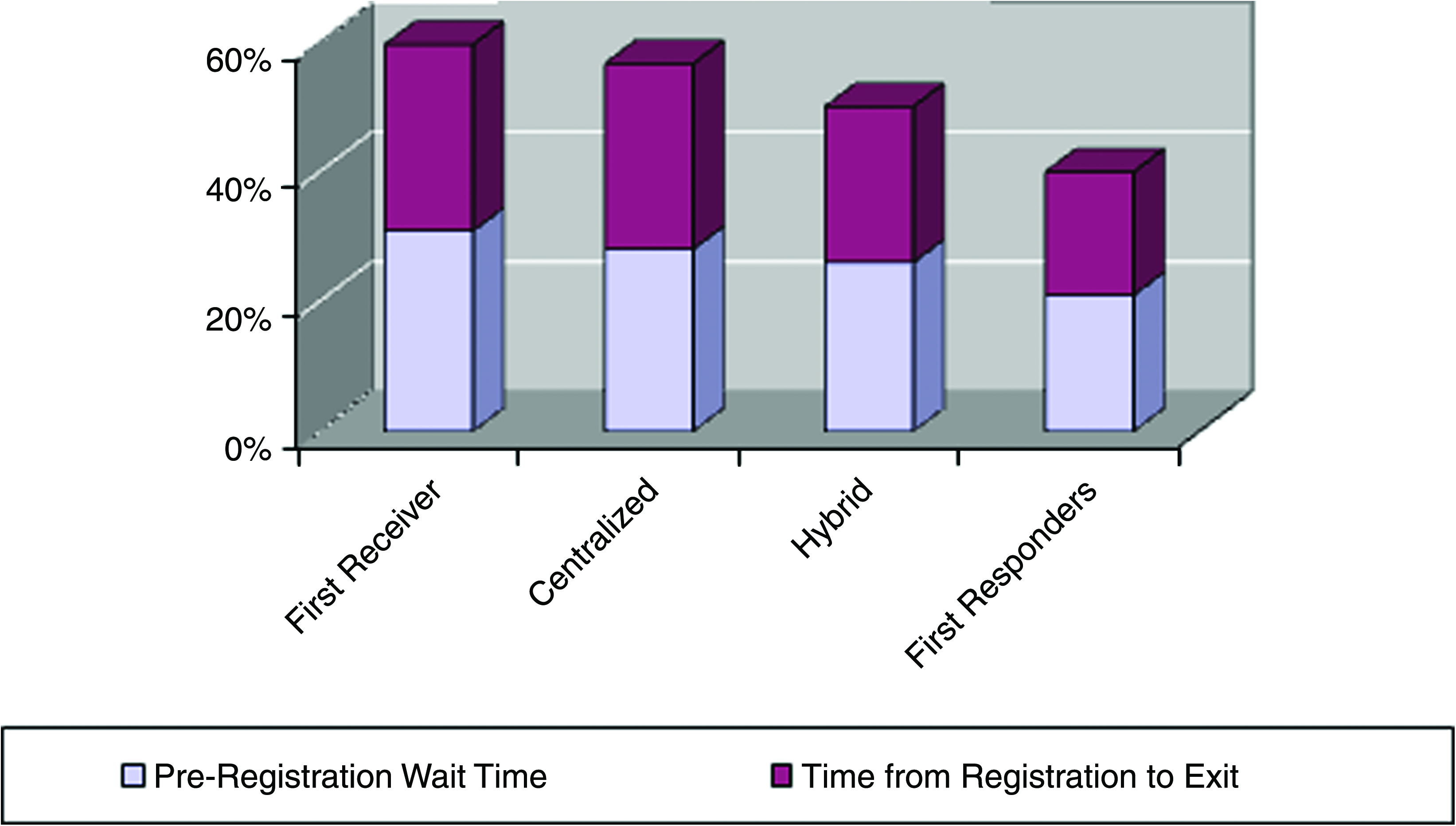
Percent of clients reporting wait of 5 minutes or less. Color images available online at www.liebertonline.com/bsp.
Processing times varied by practice discipline and model type. Regarding practice discipline type, individuals from first responder PODs were significantly less likely than individuals from first receiver PODs to report being processed from arrival to completed registration in less than 5 minutes [χ2(N = 1,064, 3) = 32.249, p < 0.001] and from registration to POD exit in less than 5 minutes [χ2(N = 1,058, 3) = 35.916, p < 0.001]. Regarding facility type, individuals from hybrid facilities were more likely to report the time between arrival to completed registration as less than 5 minutes, and they were less likely to report the time between arrival to completed registration as more than 15 minutes than were individuals from centralized facilities, although this difference was not statistically significant [χ2(N = 1,064, 3) = 5.817, p = 0.121]. There was no difference between individuals' reported times from completed registration to POD exit between hybrid and centralized facilities.
Satisfaction with POD Functioning
Individuals used a 4-point Likert scale to indicate their level of agreement with positive statements about various aspects of the dispensing process. When comparing by practice discipline type, some differences in satisfaction were identified. Of the 1,378 respondents, 509 were from first responder PODs and 869 were from first receiver PODs. A sample of 509 of the 869 first receiver POD individuals was randomly selected for comparison. Of the 7 satisfaction measures, there were no differences in 3 of them: individuals' satisfaction with the effectiveness and efficiency of medication dispensing, POD staffs' ability to fully answer questions, and the organization of the PODs. However, individuals at first receiver PODs were more likely than individuals at first responder PODs to strongly agree that: (a) there were enough staff dispensing medication (95%, 91%), (b) they knew the proper dosage of medication to take (89%, 78%), (c) they knew what to expect after taking the medication (82%, 75%), and (d) participating in the exercise was a valuable experience (97%, 94%).
Of the 1,378 respondents, 955 (69%) were from centralized facilities and 423 (31%) were from hybrid facilities. To conduct appropriate statistical analyses, equal sample sizes were needed, so a sample of 423 individuals from centralized facilities was randomly selected for comparison. There were no differences in 6 of the 7 measures of satisfaction. Individuals from hybrid facilities were more likely to report sufficient numbers of staff to operate the POD than were individuals from centralized facilities (96%, 92%).
Medication Errors
The medication distributed to individuals was reviewed by trained medical evaluators, where “charts” were registration forms that had been collected from people as they left the PODs. This review and analysis was conducted by model type (centralized or hybrid) and the practice discipline type responsible for the POD (first responder or hospital).
Of the 4,246 individuals processed, 3,532 (83%) returned completed registration forms. Medical reviewers completed evaluations of 2,745 (78%) of the 3,532 registration forms. The remaining 787 registration forms, which contained incomplete information on one or more areas, had not been completed in full by the medical evaluators.
Comparisons of POD Functioning
POD Functioning by Practice Discipline
Of the 2,795 charts reviewed, 972 had been processed through a first responder POD, and 1,823 had been processed through a first receiver POD. A random sample of 972 charts from the 1,823 hospital charts was selected for comparison of the 2 practice discipline types. There were no differences between first responders and first receivers in: (a) the number of forms signed by individuals, (b) the number of forms signed and completed by a medical screener, (c) the number of screeners prescribing the correct medication, or (d) the number of distributors who changed medications for properly dispensing.
However, a significantly larger proportion of first responder POD individuals completed all questions than did first receiver individuals [χ2(N = 1,944, 1) = 15.781, p < 0.001]. Yet, first receiver PODs overall had more positive outcomes. Of the 63% of the sampled individuals who had completed forms, more first receivers (54%) than first responders (46%) finished the registration forms in totality [χ2(N = 1,941, 1) = 26.505, p < 0.001]. More first receiver screeners checked medication that was to be distributed [χ2(N = 1,944, 2) = 8.245, p = 0.016]; more first receiver distributors signed and completed forms [χ2(N = 1,942, 1) = 31.171, p < 0.001]; and more first receiver distributors dispensed medication as prescribed [χ2(N = 1,944, 1) = 13.516, p < 0.001]. Moreover, fewer first receiver participants received improper medication than first responder participants [χ2(N = 1,944, 1) = 23.306, p < 0.001] (Table 1).
POD Functioning by Model
Of the 2,795 charts reviewed, 1,879 (67%) were from centralized facilities, and 916 (33%) were from hybrid facilities. A random sample of 916 charts from the 1,879 centralized charts was selected for comparison of the 2 model types. There were no differences between centralized and hybrid facilities in the number of (a) complete forms regarding patient information, (b) forms signed by participants, or (c) distributors changing medication to be properly dispensed. Moreover, there was no difference in the facilities' overall completion of the forms.
However, facilities with hybrids had significantly more forms signed and completed by medical screeners [χ2(N = 1,832, 1) = 4.681, p = 0.030]. The screeners in hybrid facilities checked medication to be distributed more than did those in centralized facilities [χ2(N = 1,832, 1) = 9.807, p = 0.007], and they prescribed the correct medication more often than did screeners in centralized facilities [χ2(N = 1,832, 1) = 12.355, p < 0.001].
Yet, centralized facilities had significantly more forms signed and completed by distributors [χ2(N = 1,832, 1) = 5.202, p = 0.023], and, in these facilities, the distributors dispensed more medication as prescribed [χ2(N = 1,832, 1) = 5.370, p = 0.020]. Moreover, individuals who were processed through centralized facilities were less likely to receive improper medication [χ2(N = 1,832, 1) = 6.825, p = 0.009] (Table 1).
Discussion
Although POD exercises have been previously conducted for individual hospitals and clinics or for use by the general public, Operation RAPID presents an analysis of a large-scale regional exercise featuring POD operations for first responders, first receivers, and their families. Such a large-scale type of event involving different practice disciplines and different POD model types in the same exercise has not been previously presented in peer-reviewed literature.
This analysis is particularly noteworthy in its comparison of POD facility functionality by practice discipline and model type, so that more specific recommendations can be made concerning best practices for POD operations for first responders and first receivers. The police, fire, and EMS workers in Operation RAPID are an integral part of many local plans for emergency response and would be needed in the event of mass dispensing of chemoprophylaxis, making enhanced understanding of efforts to provide this population with mass chemoprophylaxis of paramount importance.
Practice Discipline
Differences in throughput, medication errors, and patient satisfaction were all evident when comparing POD functionality by practice discipline, with the most pronounced differences occurring in throughput and medication errors. In terms of throughput, first responder facilities were markedly faster at processing people than were first receiver facilities. The differences in throughput rates probably related to 2 factors: the total number of people processed and differences in the POD workers' respective work environments.
First, regarding the number of individuals, first receiver facilities handled fewer individuals than did first responder facilities; the median number of individuals processed at first receiver facilities was just 21, whereas the median number of individuals processed at first responder facilities was 67. The larger number of individuals available to first responder facilities may have afforded them greater throughput rates; delays inherent in the initial opening of the clinic and initial “hiccups” were likely evened out as more individuals flowed through and the clinic was operating at maximum efficiency. With a median of just 21 individuals at first receiver facilities, POD workers there would have had less opportunity to function at maximum efficiency before the supply of individuals was exhausted.
Second, regarding the work environment, first receivers may be more accustomed to responding in their facilities to a constant flow of individuals, where they must pace themselves. In contrast, first responders travel to external emergency calls that occur at random intervals throughout their day, requiring sudden expenditures of energy followed by an indeterminate lag time between emergency calls.
Though first responder facilities processed individuals more efficiently, individuals at first receiver facilities reported greater satisfaction with the process than first responder individuals. First responder facilities also exhibited an advantage over first receiver facilities in medication error rates. Based on the responses participants gave on their registration forms (eg, age, gender, weight, pregnancy status, drug allergies), first receiver facilities were more likely than first responder facilities to dispense the proper type and dosage of medication according to health department protocols.
These first receiver successes could be explained by hospital workers' familiarity with medication dispensing and the accompanying processes and paperwork. Furthermore, the attention to detail that enabled fewer medication errors in first receiver facilities may also be directly related to their slower throughput. Although rapid throughput is especially important for PODs designed to provide chemoprophylaxis to first responders and receivers who are needed to return to work quickly, 10 accuracy of medicine dispensing is equally (if not more) important. An excessive number of medication-related adverse events could render the best-laid plans of emergency planners moot and hinder disaster response by leaving first responders and receivers unable to work and in need of medical care themselves. 36
Model Type
Unlike the differences in throughput, patient satisfaction, and medication error rates observed when comparing POD functionality by practice discipline, only nominal differences were observed when analyzing POD functionality by model type. This suggests that discipline is a much more critical factor in assessing POD functionality.
However, there were some differences in POD functionality by model type, particularly in medication error. Unlike the medication error differences by practice discipline, differences in medication error rates by model type were not uniform in direction, with some aspects of medication error favoring centralized facilities and others favoring hybrid facilities.
Centralized POD facilities were minimally more accurate in dispensing medication (according to proper protocols) than hybrid facilities, but hybrid facilities were more likely to follow the individual steps in the protocol designed to reduce medication error (eg, medical screeners at the PODs initially prescribing the correct medication, more medical screeners signing registration forms).
Implications
Further collaboration between first responders and receivers is warranted to increase efficiency and accuracy of POD operations. Practice discipline, rather than POD model type, was consistently the stronger predictor of any differences between PODs. However, since first receiver and first responder facilities had different strengths and weaknesses, interdisciplinary planning, training, and exercising could be beneficial to all practice disciplines that fall under the first receiver and first responder umbrella.
Furthermore, having select hospital workers assist first responder facilities with POD implementation and operation and vice versa must be considered. For example, since hospitals had better medication dispensing, hospital workers could aid in medical screening and drug dispensing at first responder facilities, while first responders could aid hospital workers in registration areas to produce greater throughput.
As a result of the evaluation findings, the Nassau County Department of Health has instituted training that includes an additional focus on assurance of quality in medicine dispensing. The pre-exercise training focused primarily on overall POD operation, without any special emphasis on quality assurance. This overall operational focus was critical, as many of the first responders, first receivers, and their families that were to be participants in Operation RAPID had little or no previous experience with PODs. Also, as a result of the evaluation results of Operation RAPID, the Nassau County fire departments have acknowledged the importance of POD training and have now included POD operations in their yearly training requirements.
In addition to this study's findings, the methodology employed has implications for future studies and POD exercises. Researchers were able to construct a multifaceted measure of POD functionality that extended beyond mere throughput measures because of the ability to measure participant satisfaction and medication error rates. While the addition of participant satisfaction measures is important in their own right, the addition of retroactive chart reviews to assess quality and to correlate it with throughput is seldom done in evaluations of POD exercises.29-33 By combining these metrics, researchers were better able to examine the functionality of these first receiver and first responder PODs. Impressive throughputs achieved without quality control in the dispensing of medication have the potential to do more harm than good. If this focus on accuracy coupled with throughput could become more commonplace, POD operations in general could be improved.
Limitations
Many of the limitations of this evaluation are related to the experiential nature of Operation RAPID for the Nassau County Health Department, hospitals, first responders, and MRC. While experienced evaluators and researchers were a part of the planning process, they could not control events or data collection as they might have had this been solely a research project. For example, the evaluation of various models through Operation RAPID was limited in that no facilities employed only decentralized PODs; however, decentralized PODs were employed at hybrid facilities, which allowed for both models (centralized and hybrid) to be analyzed and compared. Additionally, despite extensive efforts to assure full data collection, not all participants and facilities reported data, although many response rates were in keeping with other emergency preparedness evaluations of this size.37,38
Operation RAPID did not achieve the throughput times suggested by POD modeling, such as BERM, 39 or that of other previously conducted and reported exercises.29-33 This may be due to the fact that PODs had to process only a limited number of individuals and closed as soon as all their individuals were processed. As a result, PODs may not have been operating at their maximum capacity. However, Operation RAPID did process more than 4,000 first responders, receivers, and family members in about 4 hours, with limited need for individuals receiving chemoprophylaxis to travel to an unfamiliar location or to leave work; this is a significant accomplishment and serves as the potential foundation for future exercises. Additionally, Operation RAPID's evaluation provides value to POD modeling in its ability to include quality control in addition to throughput. The combination of these 2 factors is critical for assessing live POD exercises and may produce a more accurate representation of throughput capabilities.
One final project limitation lies in the unique nature of the population in the exercise. Operation RAPID was conducted in Nassau County, New York, and the results may not be applicable to other geographic areas. Compared to Americans in general, New Yorkers are more fearful of being subjected to another terror attack, with this fear being most pronounced among New York City and Long Island residents.40-42 With this higher level of fear and greater self-identification as possible victims, New Yorkers are likely to be more receptive to disaster preparedness exercises such as Operation RAPID than citizens from other locales. However, the results provide an important look at a large, interdisciplinary exercise. Further studies to examine the differences between first responder and first receiver disciplines and model types would be of great benefit to mass chemoprophylaxis preparedness.
Conclusions
Providing emergency chemoprophylaxis to first responders and first receivers would be vitally important in a bioterror event, and it is likely that their assistance would be needed in operating community-wide PODs. Health departments would require assistance in providing chemoprophylaxis to first responders, first receivers, and their families. Thus, cooperative and comprehensive POD operational plans for first responders and first receivers and POD exercises incorporating hospital, police, fire, EMS, and health department personnel are critical. These different practice disciplines must work together in a unified emergency response.
In Operation RAPID, the only substantial differences in POD outcomes were observed by practice discipline, not model type. First responder facilities exhibited better throughput than first receiver facilities, yet first receiver facilities had a lower incidence of medication error. To maximize the strengths of the different practice disciplines, further cooperation between first receivers and first responders in planning and implementing POD sites must be encouraged. The differences observed by discipline in this exercise were pronounced enough to warrant a need for greater cooperation by practice discipline, but they also provide an opportunity for various disciplines to practice and exercise together to maximize their different skill sets and use these differences to enhance future preparedness efforts.
Footnotes
Acknowledgments
Special thanks go to Frank Chester, EMT-CC, Assistant Chief Instructor, Vocational Education and Extension Board of Nassau County, and Kristine Qureshi, RN, CEN, DNSc, Associate Professor, School of Nursing and Dental Hygiene, University of Hawaii at Manoa. This project was funded through an Office of the Assistant Secretary for Preparedness and Response (ASPR) grant (621889815). There are no conflicts of interest to report.