
Abstract
In the early stages of the 2009 H1N1 influenza pandemic, Mexican nationals and Mexican commodities were shunned as being the source of the disease. The authors investigated instances in which Latino migrant and seasonal farmworkers were stigmatized and developed guidance for officials to combat this. They also looked at social factors that make farmworkers more vulnerable to influenza infection and its complications, including high rates of underlying medical conditions and limited access to health care.
At the outset of the 2009 H1N1 influenza (“swine flu”) pandemic, Mexican nationals and Mexican commodities were shunned globally, and, in the United States, some media personalities characterized Mexican immigrants as disease vectors who were a danger to the country. We investigated instances in the U.S. of stigmatization of Latino migrant and seasonal farmworkers (MSFWs) and developed guidance for officials in curtailing its effects. At the same time, we explored social factors that make farmworkers more vulnerable to influenza infection and its complications, including high rates of underlying medical conditions, limited access to health care, and certain circumstances that interfere with the ability to implement community mitigation measures. This article reviews study findings and concludes with advice to policymakers and practitioners on the need to mitigate stigmatization in future outbreaks, to create public health preparedness systems that better protect migrant and seasonal farmworkers, and to undertake larger reforms to reduce institutional conditions that render farmworkers at greater risk for morbidity and mortality during health emergencies.
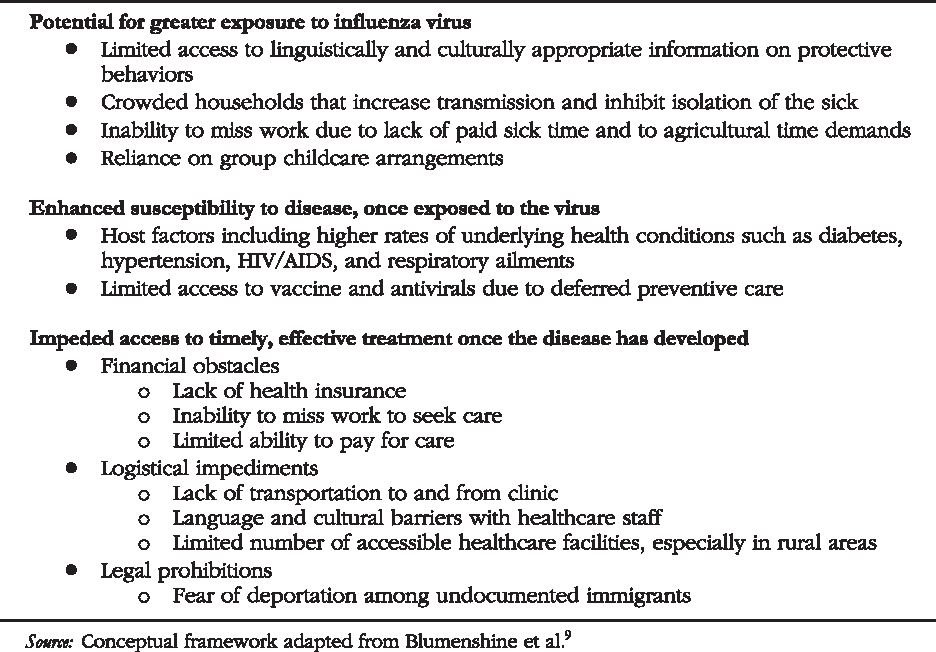
Our group also sought to examine additional factors that contribute to higher risk for 2009 H1N1 influenza and its complications among migrant and seasonal farmworkers (see Figure 1)—a population anticipated to be more vulnerable to the effects of pandemic influenza. 4 These extremely low-paid employees have high rates of underlying medical conditions and face complex barriers to health services.5,6 Disadvantaged groups—including low-income groups and racial and ethnic minorities—often suffer disproportionately high losses during natural disasters and epidemics.7-9 Thus, many analysts have argued for public health preparedness planning to address the unique requirements of vulnerable populations and to reduce differential impacts.10-14
Health Disparities Placing Migrant and Seasonal Farmworkers at Greater Risk of Morbidity and Mortality During the 2009 H1N1 Influenza Pandemic
This article provides some background facts on farmworkers in the U.S. and the 2009 H1N1 influenza pandemic and reviews migrant and seasonal farmworkers' experiences with scapegoating, living conditions that inhibited community mitigation measures, and barriers to care that likely delayed or prevented vaccination and/or treatment for 2009 H1N1 influenza. Following these observations are recommendations to policymakers and practitioners on ways to remedy stigmatization in future outbreaks, to create preparedness and response systems that better protect migrant and seasonal farmworkers, and to reform underlying conditions that expose farmworkers to greater risk during health emergencies (see Figure 2).

Federal Actions to Mitigate the Impact of an Influenza Pandemic on Migrant and Seasonal Farmworkers and Their Host Communities. Interventions span from immediate refinements to preparedness and response systems to increasingly comprehensive reforms that help reduce those societal conditions that put farmworkers at greater risk in health emergencies.
Background
Migrant and Seasonal Farmworkers in the U.S.
An estimated 3 million migrant and seasonal farmworkers reside in the U.S., although it is difficult to establish an accurate number because of population mobility and the lack of a standard definition.15,16 Migrant farmworkers leave their permanent residences in the southern U.S., Mexico, Central America, and the Caribbean to pursue agricultural jobs. In general, they migrate northward in sync with growing and harvesting seasons. Some migrants relocate several times over the course of a year, while others remain at the same farm for an entire season before returning to their home base. Seasonal farmworkers, in contrast, work close enough to farm activities to commute from home. 17
Migrant and seasonal farmworkers plant, cultivate, harvest, process, and pack food for shipment and consumption; they also work in the fishing, poultry, ranching, dairy, nursery, and timber industries. In the U.S., 85% of fruit and vegetable crops are hand harvested and/or hand cultivated; without the timely influx of migrant labor during peak periods, production in this $39 billion industry would falter.18,19 Migrant and seasonal farmworkers work in at least 42 of 50 states; 5 states that host the largest numbers of migrant and seasonal farmworkers are California, Colorado, Florida, Georgia, Idaho, Illinois, Michigan, North Carolina, New York, Oregon, Texas, and Washington.15,20
Most crop workers are young, poorly paid, Hispanic men who are living apart from family, according to the FY2001-2002 National Agricultural Workers Survey (NAWS) 21 (see Table 1). About half lack authorization to work in the U.S. 21 Almost a third of crop workers have total family incomes below the poverty line; most are not covered by health insurance or unemployment insurance. 21 The vast majority report Spanish as their native language, with almost half unable to speak English “at all.” 21 Increasingly, indigenous farmworkers from Mexico and Central America are migrating to the U.S. for work.16,22,23
Farmworker Population Characteristics from the National Agricultural Workers Survey (NAWS), FY2001-2002 21
Note: NAWS participants represent farmworkers in crop agriculture but not poultry, livestock, and fishery settings. 16
Occupational and Lifestyle Exposures
Agriculture is one of the most dangerous work environments in the U.S. Among its health effects are musculoskeletal disorders, traumatic injuries, eye damage, respiratory conditions, heat stress, and skin reactions.5,6,24,25 Pesticides permeate the workplace and can cause acute and chronic poisoning. Different crops present a wide spectrum of hazards: for example, picking orchard fruit presents a danger of falling or injuring an eye, while harvesting mushrooms in humid environments exposes workers to high mold levels.16,24
Farmworkers are vulnerable to certain infectious diseases and intestinal disorders at rates much higher than the general population, in part because of inadequate and crowded housing, poor sanitation, and lack of clean water. 24 Some farmworkers live in dormitories and barracks; many crowd single-family homes and apartments to reduce the impact of rent on their low incomes. 26 Nearly a quarter of migrant and seasonal farmworkers' housing units have serious structural defects and lack basic amenities such as a stove, a refrigerator, a bathtub, and a toilet.26,27
Migrant and seasonal farmworkers are also at increased risk for developing certain chronic diseases, such as diabetes and heart disease, because of high rates of obesity, elevated serum cholesterol, and high blood pressure—conditions that may have some roots in “food insecurity” and the diet choices made by people with limited incomes.5,6,24 Diabetes, tuberculosis, HIV/AIDS, and other illnesses that require active monitoring present special challenges to migrant and seasonal farmworkers, who often lack follow-up care or a stable, ongoing relationship with a single provider or clinic. 25
As we discuss in greater depth later, migrant and seasonal farmworkers face multifaceted barriers to health services and tend to seek out healthcare services only when absolutely necessary.5,6
2009 H1N1 Influenza Pandemic
On March 18, 2009, the first cases of an influenzalike illness were reported in Mexico. These were later attributed to H1N1, a novel influenza virus that then spread around the globe. On April 17, the U.S. Centers for Disease Control and Prevention (CDC) confirmed the first 2 cases of H1N1 in the U.S. On April 25, the World Health Organization's (WHO) director-general called the novel influenza outbreak “a public health emergency of international concern.” 28 The next day, the U.S. Department of Health and Human Services (HHS) declared a national public health emergency. 29 On June 11, WHO declared a global pandemic of H1N1 infection around the world.
Throughout the spring and early summer, several countries, including the U.S., enacted a variety of community mitigation measures to slow down spread of the disease.30,31 Officials in Mexico City temporarily opted to close all schools, restaurants, movie theaters, gyms, swimming pools, nightclubs, museums, and zoos; school closures were eventually extended throughout Mexico. 32 In the U.S., the CDC, lacking good data on pandemic severity during the initial April outbreaks, recommended closure of schools or childcare facilities under certain conditions. 33 Once the virus was recognized as being mild and spreading communitywide, the CDC reversed its guidance on preemptive school closures and advised keeping sick children at home for the duration of their infection.34,35 The CDC also issued recommendations for antiviral drug treatment of people with H1N1 influenza. 36
HHS placed its first order for 2009 H1N1 vaccine on May 22, 2009, with the goal of eventually buying enough for the entire U.S. population. 37 On July 29, 2009, the CDC's Advisory Committee on Immunization Practices met to consider priority groups for receiving the vaccine when it became available. 38 Because of production delays, most states did not begin receiving significant quantities of vaccine until November and December 2009. 37 H1N1 cases, hospitalizations, and deaths in the U.S. first peaked in May (spring wave), declined over the summer, and then peaked again in November during a fall wave of illness. 39
Stigmatization
With reports first emerging from Mexico of a novel disease outbreak with presumed high death rates, conditions were ripe for people and places that were linked in individuals' minds to the illness to be stigmatized. Diseases that are perceived as lethal, contagious, and outside scientific understanding tend to evoke a social stigma.40,41 To distance themselves from the threat, people sometimes point a finger at a presumed “cause”; fixing blame helps turn a mysterious and frightening illness into something that feels familiar and thus more controllable. 40
Some people may see the world as made up of the “infected” and the “uninfected,” but these categories obscure the complex ecologies that give rise to infectious diseases and their spread. 2 At the same time, this binary thinking can lead to scapegoating when a whole region or group of people is singled out as the source of contagion.2,40,42 Stigmatization, scapegoating, and discrimination are fueled by the fear of disease as well as preexisting social hierarchies and political biases.
As news broke of the H1N1 outbreak, some countries around the world began to shun Mexican citizens and products. Haitian officials turned back a Mexican ship carrying humanitarian food aid because of H1N1 fears. 43 Several countries banned Mexican pork and pork products, and China sequestered Mexican travelers on the basis of their nationality as they entered the country, even if they did not show symptoms of influenzalike illness or have an occasion for possible exposure. 44
On April 29, 2009, the first H1N1 fatality in the U.S. was reported: a Mexican child who was visiting Houston, Texas. The report sparked media debates over how the disease was entering the U.S. and what containment measures were needed, including closing the border with Mexico.45,46 In the U.S., some Mexican restaurants reported a drop in business during the spring wave of the disease, 47 and 17% of respondents to a national survey conducted at the end of April reported “avoiding Mexican restaurants or stores” out of concern over swine flu. 48
Stigmatization, however, was not limited to shunning behavior directed at Mexican nationals and commodities, nor was it unknown within Mexico itself. Residents of Mexico City, which was hit hard by the H1N1 epidemic, were unwelcome by some in other parts of their own country. A crowd in the Mexican state of Guerrero, for instance, hurled stones at cars that had license plates from the capital city. 49 In Egypt, minority Christians asserted that religious prejudice by a Muslim majority, and not matters of public health, drove officials to order the slaughter of the country's pigs as a precaution against swine flu. 50
Given the anti-immigrant rhetoric targeted at Mexicans, some U.S. government and nongovernment leaders feared that the H1N1 outbreak would fuel hostility against Latinos. 47 U.S. history is replete with examples of immigrant populations being characterized as a threat to the health, character, and stability of the nation and of immigration policies being influenced by racist and nativist ideologies. 51 Indeed, some media personalities dubbed the H1N1 outbreak “Mexican flu” and “fajita flu,” and they seized on the growing number of flu cases as evidence that the uncontrolled flow of “illegal aliens” across the southern U.S. border and their purported unhygienic practices were a danger to the country.47,52,53
A number of government officials, Latino advocacy organizations, and public health groups moved to denounce the racist anti-immigrant rhetoric, to propose interventions to reduce stigmatization, and to assure that the needs of Hispanics were met during the epidemic.47,54 On April 29, for example, the National Association of Hispanic Journalists made a formal plea to their industry peers to counter the “inflammatory rhetoric” and “breathless” reporting of “talking heads,” and the scapegoating it incited, with fact-driven, balanced news stories. 55 On May 6, the CDC released guidance for communication specialists and response officials on actions to counter stigma. 56 President Obama held a town hall–style meeting on May 8, 2009, with approximately 130 Latino public health professionals and grassroots leaders, promising that the nation's response to the flu outbreak would protect against discrimination and seek to include Hispanic communities. 54
Study Methods and Limitations
Over 11 weeks, from July to October 2009, we conducted semistructured, 45-minute telephone interviews with 31 executives from community clinics (n = 18), government agencies (n = 6), and advocacy groups (n = 7) serving migrant and seasonal farmworkers. We contacted both national organizations and local providers, using purposive sampling to cover diverse regions with large numbers of Latino residents and migrant and seasonal farmworkers. In addition, we spoke with industry and academic contacts (n = 2) familiar with the health challenges of migrant and seasonal farmworkers. We asked about the organization's interaction with migrant and seasonal farmworkers, the timing and extent of the farmworkers' presence in local or regional communities, instances of stigmatization during the first H1N1 wave, the behavior of migrant and seasonal farmworkers in seeking health care, living conditions and other factors influencing compliance with H1N1 containment measures, and advice on protecting farmworkers during the anticipated fall wave of the pandemic.
We prepared summary reports for each interview that combined audiotapes and handwritten notes. At least 2 members of the research team were present for each interview, and, in some instances, all team members participated. Interview questions and data analysis were informed by a literature review of materials on farmworker health issues, on preparedness challenges for vulnerable populations, and on stigma in the epidemic context. Each investigator read the full set of interview reports; audiotapes were consulted to confirm relevant quotes and data points. In November 2009, we published preliminary findings with recommendations intended to assist care providers and health officials in vaccinating migrant and seasonal farmworkers. 57
Topics in this report could benefit from additional, retrospective data that encompass the complete life cycle of the pandemic, as well as first-person accounts from farmworkers. Given limited time and resources to discern a national perspective, we did not directly survey farmworkers but instead spoke to organizational intermediaries. Interviews took place between the spring and fall waves, as the pandemic was evolving; as a result, interviewees provided real-time observations early in the pandemic and speculated about challenges yet to emerge for migrant and seasonal farmworkers. Due to seasonal migration patterns, farmworkers were more numerous in some regions than others at the time of the interview.
Study Observations
At the outset of the epidemic, some community health centers felt that news reporters were characterizing their clinics as swine flu “hot spots” based simply on the fact that the facilities served migrant farmworkers. These local providers reached out to a national farmworker health organization for assistance in correcting misinformation about migrant and seasonal farmworkers, including the perception that they had higher rates of influenza infection than the larger U.S. population. A few healthcare providers, however, were not exempt from thinking automatically of Latino migrant and seasonal farmworkers as carriers of disease. As one interviewee recounted:
I remember talking to one of our providers at the time, and her comment to me was just—it kind of floored me—and she just said, ‘You know, we need to be telling people that especially in [this town], “Little Mexico,” that we have all these people coming from Mexico and they're bringing in the swine flu.’
In some areas interviewees related no known instances of migrant and seasonal farmworkers being stigmatized; one explanation for this was that the region's majority population was Hispanic and not likely to blame others who shared a common cultural and ethnic background. Another explanation offered was the fact that H1N1 had emerged in late April, when migrant and seasonal farmworkers had yet to arrive. Thus, there was no reason to blame Latino farmworkers for introducing the flu. One interviewee also noted that, while H1N1 did not give rise to any “new” instances of prejudice against Latino farmworkers, there was a constant level of anti-immigrant sentiment in the community.
Some migrant workers are not aware of the availability of services at migrant health clinics or other Federally Qualified Health Centers (FQHCs). Mobile populations that are not well integrated into their surrounding communities are difficult to reach and to educate regarding available services. Lack of sick leave prevents many from seeking care, because they fear losing their jobs, and clinics may be open only during work hours. As one subject noted, “In the farm industry … when the crops are ready, the crops are ready, and they [employers] expect them [farmworkers] to be there.”
Because this population tends to reside in isolated rural communities, transportation to and from health clinics remains a major obstacle to obtaining care. Healthcare costs discourage farmworkers from interacting with the medical establishment. Very few employers in agriculture provide health insurance, and various legal and administrative restrictions inhibit many migrant and seasonal farmworkers from gaining access to public assistance. Migrant workers typically cannot afford health services, even at the reduced rates of a community health clinic. In addition, federally subsidized public health care in Mexico and lack of familiarity with the American system create confusion over payment for healthcare services.
Whether documented or not, migrant and seasonal farmworkers hesitate to seek care in communities where federal Immigration and Customs Enforcement (ICE) officials are present and, in some instances, are staking out health clinics, according to interviewees. Migrant and seasonal farmworkers avoid “unessential” road travel, lest they be pulled over by ICE or other law enforcement officers, so they are reluctant to go to a clinic. One facility interviewed for the study reached a verbal agreement with ICE to prevent officials from coming onto clinic property; this measure was intended to build trust and to encourage farmworkers to seek care.
A healthcare provider warned of the compounding effects of fear of deportation during the H1N1 epidemic:
If you already have that concern about seeking care anyway because you don't have proper documentation, … then if you're sick with something and people are stigmatizing you because you are from Mexico, that even makes you more reluctant to seek care.
We've talked to guys who puke their guts out every day from green tobacco sickness. You think a little flu is going to keep them from going to work? … They're afraid of losing their jobs if they don't show up. … They only get paid when they work. They don't have sick leave. … So if they're sick, they're going to work because they have to feed themselves, and there are people back in Mexico expecting money to be sent to them so often.
School closures also create hardships for farmworker parents, just as they do for other working class families. When schools close—as they did in the spring as a preventive measure and during the fall due to absenteeism—farmworker parents are often unable to stay home to care for their children. Even if schools remained open, interviewees recounted, sick children who were “staying home” may have had to accompany their parents to work or be sent to a neighbor's home for group childcare. Inability to isolate and care for these children could contribute to the spread of H1N1 influenza. Lack of adequate childcare when parents are sick may also increase H1N1 transmission risk.
Finally, when migrant and seasonal farmworkers are able to stay home when sick with flu, public health guidance on H1N1 containment recommends isolation from family or other household members. Several farmworker families or many individuals may share a single household, preventing isolation of the sick and increasing the chances of influenza transmission among inhabitants. Study interviewees in a western state, for instance, related that in one labor camp 10 to 12 men or 2 to 3 families would share a small cabin. According to a recent national survey, almost 52% of all migrant housing units are crowded, and among crowded units, 74% have children. 26
During the spring wave of the pandemic, community and migrant health centers helped transmit CDC public health messages and bilingual patient education materials to farmworkers aided by national groups including the Migrant Clinicians Network, the National Association of Community Health Centers, and the National Center for Farmworker Health. 60 Building on prior relationships and knowledge of the populations they serve, many of the health centers interviewed provided H1N1-specific information in multiple languages and low literacy formats. They engaged with community partners, including local health departments and radio and TV stations to communicate the risks of H1N1 to the migrant and seasonal farmworker population. In addition, the health centers provided mobile healthcare services and vaccination. Some health centers remained open beyond normal hours and focused on mobile outreach.
Like other healthcare entities, however, community and migrant health centers faced limitations during the pandemic. Some centers were limited in their ability to develop Spanish or low literacy information, and one commented that, although they had Spanish materials, many workers in their region were of indigenous background and did not speak Spanish. The health centers coordinated with states to obtain antiviral medications from the Strategic National Stockpile and then distribute them to farmworkers. But study interviewees noted that only small amounts of antivirals were available and that they were slow to arrive. Some community clinics felt unprepared to meet the increased demand for services during the pandemic. An interviewee noted that state authorities directed people to community health centers during the spring wave, and these clinics were quickly overwhelmed. They began seeing patients in addition to their normal patients, and staff worked many overtime hours.
Early in the epidemic, anecdotal reports and preliminary data from around the country suggested that the 2009 H1N1 virus had a heightened impact on Latinos and other minority communities. The Chicago Department of Public Health reported that hospitalization rates were 4 times higher among Hispanics than non-Hispanic whites, and it speculated that the disparity may have been partially due to a higher prevalence of asthma, diabetes, and other underlying conditions. 62 Preliminary data from the California Department of Public Health showed that Latinos were twice as likely as whites to die and twice as likely to be hospitalized due to H1N1. A California state epidemiologist pointed to the higher prevalence of diabetes and obesity as the potential reasons for increased mortality and hospitalization rates. 63
The Boston Public Health Commission reported disproportionately high rates of H1N1 in Hispanic populations. 64 The Texas Department of State Health Services noted that Hispanics, who comprise 37% of Texas's population and who have high rates of chronic illness, represented 52% of H1N1 deaths in the first 6 months of the pandemic. In addition, the true death rate among Hispanics may have been higher because ethnicity/race was unrecorded in 17% of the Texas deaths. Hispanics also accounted for about two-thirds of hospital ICU admissions in Texas for H1N1. 65 On February 24, 2010, the CDC published data that corroborated early reports of a higher impact of flu among Latinos, showing that they were hospitalized at a higher rate than whites consistently throughout the fall wave of the pandemic and into January 2010. 66
Study Implications
There is a need in future outbreaks to mitigate stigmatization, create preparedness systems that better protect migrant and seasonal farmworkers, and reduce societal conditions that put them at greater risk in health emergencies. In the event of a communicable disease, benefits accrue not only for stigmatized groups, but also for the larger population. People who are scapegoats are often reluctant to seek medical care when they are sick and go “underground,” putting themselves and others at risk. From a herd immunity perspective, raising the level of farmworkers' access to basic prevention and treatment services may reduce the opportunity for disease transmission within the larger population. 67 As one physician we interviewed put it, “It's not in the public health interest not to educate, immunize, protect, [and] give treatment to everyone.”
Planning for future health emergencies involving communicable disease should incorporate CDC guidance to reduce the potential for stigmatization and counter it when it occurs.
56
Recommendations for officials and communication specialists include:
Use diverse ethnic groups in visual materials; Avoid the use of geographic names when discussing past outbreaks; use dates instead (eg, “1918 influenza pandemic” rather than “Spanish influenza pandemic”); Try out materials with staff members or trusted partners from diverse backgrounds to ensure that culturally insensitive materials are detected and deleted; Monitor traditional and new media for stigmatizing items as well as misinformation that can lead to stigmatization (eg, clarify real risk versus imagined risk); Counter incidents of stigmatization with appeals for fairness, compassion, and sound science; leaders should serve as models, ensuring that their words and actions are consistent with their exhortations to others; and Develop mechanisms to ensure that those who feel stigmatized can report it and receive assistance.
Officials and respected community leaders can fight stigma against minority communities by publicly recognizing special achievements, visiting businesses owned by minorities, and reaching out directly to at-risk communities. Such actions can mitigate negative stereotypes and prejudice and create an environment in which minority communities are more likely to report incidents of harassment.
Some issues can be anticipated in advance: Health emergency communications, for instance, should address the need for low-literacy materials; take advantage of ethnic media outlets (especially radio); build on existing, trusted outreach channels such as lay health educators affiliated with migrant health centers; and deliver messages in Spanish as well as indigenous languages. Mass prophylaxis campaigns must recognize the barriers that keep migrant and seasonal farmworkers from coming to clinics and consider innovations that bring health services to the community, such as using mobile clinics that reach workers in the fields and establishing vaccination or drug distribution at trusted locations such as Migrant and Seasonal Head Start centers.
Employers, with incentives from state and federal governments, should more broadly provide sick leave benefits, paid personal time, and health insurance for workers. Health authorities should educate employers on the financial effects on their business of having sick workers. In addition, more employers should partner with community health clinics to extend their reach to the workforce, such as by hosting mobile clinics in the fields.
Housing problems faced by farmworkers during noncrisis periods put this population at greater risk during health emergencies. 26 Crowding prevents isolation of infected household members, and poor quality housing contributes to greater susceptibility to disease as well as a higher risk of medical complications. The U.S. Department of Housing and Urban Development, with employers and nonprofits engaged with the community, should establish priority housing needs for migrant and seasonal farmworkers.
Recent health reform legislation designates $11 billion in new funding for Federally Qualified Health Centers—money that will permit them to double the number of patients they now see each year. 70 This is a welcome development, but undocumented immigrants still face significant hurdles to receiving care. Health reform explicitly left undocumented immigrants out of the uninsured groups given access to coverage; moreover, they are not eligible to buy insurance in the newly created purchasing pools or “exchanges,” even if they pay entirely out of their own pockets. 70 Migrant and seasonal farmworkers will now be competing with the “newly” insured, who are expected to turn to the federal centers for their primary care.70,71
Clearly differentiating immigration enforcement from emergency response and relief efforts is necessary to encourage farmworker cooperation with directives essential to population health and safety.4,75 Recognizing this, federal health officials sought to quell fears among the undocumented that they would need to prove their immigration status to get an H1N1 vaccine at a public health clinic or mass vaccination site. The CDC communicated this position by working with Hispanic media and with nonprofit and religious groups that routinely interact with immigrants. 76 Earlier in the year, the CDC also clarified for state and local health officials that undocumented immigrants were legally eligible for Strategic National Stockpile assets (antivirals in the case of H1N1); to withhold them would compromise the effectiveness of the public health emergency response. 77
Trust between farmworkers and the health system during normal times is a basic ingredient to ensuring farmworker adherence to public health directives in outbreaks and other extreme events. The presence of immigration officials near migrant and community health centers undermines such relationships. The Department of Homeland Security should make it routine practice not to position ICE personnel near health facilities at any time.
Some have argued that the measure that goes the farthest to ensuring farmworkers' access to health care and protections for the larger population—by reducing the constant fear of deportation—is to expand opportunities for legal residency and citizenship for undocumented immigrants already in the U.S. 78 and to create a workable system for admitting temporary workers. Research also suggests that legal residency, specifically through the H-2A program, which allows U.S. employers to hire foreign nationals for temporary agricultural jobs, corresponds with better living conditions and improved access to job safety training. 79 These provisions are now being considered as part of a larger plan to reform U.S. immigration laws. 80 One interviewee predicts, “Unless we take care of [immigration reform] … , in any outbreak, it can be worse. … I think perhaps we will have more sick people and people that are less willing to be seen.”
Conclusion
Migrant and seasonal farmworkers are highly vulnerable to pandemic influenza because of their overall health status and because they are economically and socially marginalized. Protecting this population in future health emergencies will entail both immediate improvements to preparedness and response practices and a series of more fundamental reforms. These changes—better access to health care, improved housing, expanded work benefits, and established pathways to legal residence—will enable farmworkers to engage in protective behaviors that also benefit their host communities during epidemics to come. Moreover, these changes may also help mitigate underlying health conditions and thus improve population resilience to large-scale outbreaks.