
Abstract
Effective communication and coordination are critical when investigating a possible drinking water contamination incident. A contamination warning system is designed to detect water contamination by initiating a coordinated, effective response to mitigate significant public health and economic consequences. This article describes historical communication barriers during water contamination incidents and discusses how these barriers were overcome through the public health surveillance component of the Cincinnati Drinking Water Contamination Warning System, referred to as the “Cincinnati Pilot.” By enhancing partnerships in the public health surveillance component of the Cincinnati Pilot, information silos that existed in each organization were replaced with interagency information depots that facilitated effective decision making.
This article describes how historical communication barriers during water contamination incidents were overcome through the public health surveillance component of the Cincinnati Drinking Water Contamination Warning System. Information silos that existed in each organization were replaced with interagency information depots, which facilitated effective decision making.
While regulations are in place to manage risk from the threat of contamination incidents, exposure to contaminated drinking water has resulted in widespread illness in historical contamination incidents in North America. 2 A key to detecting water contamination incidents is effective communication among water utilities and public health agencies. Water utilities and public health officials must actively work together to communicate each entity's knowledge in response to potential and actual water contamination incidents. 3 This is important because the water utility may identify contamination sooner (through automated monitoring systems) than it would be identified through traditional disease monitoring of clinical signs and symptoms by public health professionals. In circumstances when a possible water contamination incident is first detected by public health officials, it is still necessary to involve the local water utility to validate and determine the potential source of contamination and its propagation in the distribution system.
The U.S. Environmental Protection Agency (EPA) designed a program, known as the “Water Security Initiative,” to pilot multicomponent contamination warning systems. The program was established in response to Homeland Security Presidential Directive 9 (HSPD-9), which charges EPA to “develop robust, comprehensive, and fully coordinated surveillance and monitoring systems, including international information, for…water quality that provides early detection and awareness of disease, pest, or poisonous agents.” 4 The first pilot was deployed and evaluated in Cincinnati, Ohio. The objective of the EPA's Water Security Initiative is to demonstrate the feasibility and benefits of implementing a CWS, both for detecting contamination incidents as well as improving the day-to-day operation. 5 This system integrates information from multiple sources and is designed to improve detection of contamination incidents, decision making, and day-to-day operations.
This article focuses on communication and coordination protocols implemented between the local drinking water utility, the Greater Cincinnati Water Works (GCWW), and public health partners. Partnerships between the water utility and response partners supporting the public health surveillance component were strengthened with the objective of reducing “information silos” and building “information depots.” Experience derived from this pilot has shown that open communication channels and protocols are necessary to investigate and respond to possible water contamination incidents in a timely and effective manner. One of the most important outcomes of implementation of the public health surveillance component in the Cincinnati Pilot was an effective information exchange protocol to facilitate communication between relevant agencies (referred to as an “information depot” in this article) that can be used during investigation of possible water contamination incidents and during public health events.
Communication Challenges
Historically, communication between water utilities and public health officials has varied widely in providing quick response during disease outbreaks associated with drinking water. In an outbreak situation, exposure to contaminated food is often the initial assumption rather than possible drinking water contamination, and this may lead to a delayed response.
During the 1993 Cryptosporidium outbreak in Milwaukee, Wisconsin, the absence of a standard protocol for sharing information between key agencies involved in the outbreak impeded timely awareness of the evolving incident. Because data were not shared effectively, information silos occurred that prevented a full understanding of the developing outbreak. While evidence of the outbreak was mounting, it was received and investigated by the separate agencies involved in the incident. For example, the city's water plants had been receiving complaints of foul-tasting water, while the health department was receiving complaints about stomach illnesses. It was not until an infectious disease specialist identified Cryptosporidium in an immunocompromised patient that the health department considered the possibility of contaminated drinking water. At the time of this outbreak, the health department had no public health surveillance system in place, and therefore a standard protocol for integrating information from multiple agencies had not been implemented. When contaminated drinking water was identified as the source of the outbreak, the public health response was still delayed: 2 days elapsed before the city issued a boil-water advisory.6–8
In another incident, water in Walkerton, Ontario, was contaminated by Escherichia coli 0157:H7 and Campylobacter jejuni in May 2000. In response to the contamination, public health officials in Walkerton recommended that utility customers boil their water despite utility officials' claims that the water was “fine.” 9 The absence of a coordinated communication plan caused confusion and delayed the incident response process. One conclusion drawn from an inquiry into the Walkerton outbreak was that support is necessary at all levels of government to research waterborne outbreak responses. 10
In April 2008, Alamosa, Colorado, public health officials suspected drinking water as the source of a Salmonella outbreak based on an epidemiologic investigation, although laboratory test results for the presence of the organism were not yet available. Routine water quality monitoring from 2 weeks prior tested negative for coliform bacteria, but a more recent quick screening test conducted by the health department for total coliform bacteria produced positive results. In this case, the chief medical officer of the Colorado Department of Public Health and the Environment assumed responsibility for making the decision to issue a bottled water advisory. As the health department proceeded toward communicating the decision, city officials were reluctant to believe that water was the source of the contamination. 11 Those responsible for making the decision wanted additional data before committing to a course of action.
Although the above examples vary widely in factors such as the source of the contamination and number of people affected, each demonstrates how the lack of standardized communication protocols between water utility and public health officials can cause delays in the public health response. These incidents also emphasize the challenge that these agencies often encounter in the absence of tested communication and decision-making protocols: Who has the authority to call an advisory, and under what circumstances? While the focus of this article is on drinking water security, public health surveillance communication protocols can be effective in any number of events where the quality of the drinking water has been compromised and could be applied during a turbidity event or even a known contamination.
Public Health Surveillance
The main function of a drinking water contamination warning system is to detect water contamination and initiate a coordinated, effective response to mitigate significant public health and economic consequences. The development of the contamination warning system involved, in addition to GCWW, key organizations including area health departments and numerous emergency response agencies. The Cincinnati Pilot program is a collection of several monitoring and surveillance components, including online water quality monitoring, sampling, and analysis; public health surveillance; enhanced security monitoring; and customer complaint surveillance, as depicted in Figure 1. A brief description of each component is provided below:
• Online water quality monitoring involves monitoring for typical water quality parameters throughout the distribution system and comparison with an established baseline to detect possible contamination incidents. • Sampling and analysis involves the collection of distribution system samples that are analyzed for various contaminants and contaminant classes to establish a baseline of contaminant occurrence (contaminants detected, levels detected, and frequency of detections) and method performance, and for investigating suspected incidents. • Enhanced security monitoring includes the equipment and procedures that detect and respond to security breaches at distribution system facilities. • Consumer complaint surveillance enhances and automates the collection and analysis of calls by consumers reporting unusual water quality concerns and compares trends against an established baseline to detect possible contamination incidents. • Public health surveillance involves the analysis of health-related data sources to identify disease events that may stem from drinking water contamination.
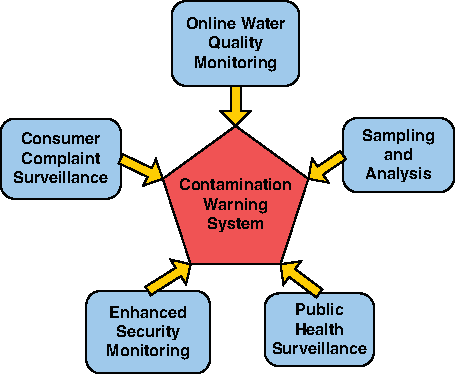
The Monitoring and Surveillance Components of a Drinking Water Contamination Warning System. Color images available online at www.liebertonline.com/bsp
GCWW designated a lead manager (referred to here as the “utility lead”) who functions as a recipient of information from all components when water contamination cannot be ruled out, and who will take additional steps to determine whether contamination is credible. The utility lead also serves as the liaison between GCWW and public health officials during investigation of possible water contamination and in non-water-related public health events. More information on the Cincinnati Pilot, including the supporting components, can be found in the Water Security Initiative: Cincinnati Pilot Post-Implementation System Status. 12
The Cincinnati Pilot used various public health surveillance tools, since information from one data stream can support findings from another. 13 For the pilot, a public health surveillance alert was triggered any time monitored data streams detected an anomaly from any of the public health data sources described below. These tools included automated monitoring systems and astute clinician disease reporting. The public health surveillance component monitored the following data streams: 911 calls, emergency medical service logs (EMS), calls from the local poison control center, (the Cincinnati Drug and Poison Information Center [DPIC]), emergency department (ED) data, and infectious disease reporting. Table 1 describes each of the surveillance tools used in the Cincinnati Pilot.
PHS Component Surveillance Tools
Information in each public health surveillance tool was analyzed spatially and temporally against established baselines for the community. Deviations from the baseline triggered an alert, which was subject to an initial evaluation by the public health partners to determine if it was a valid alert with an unexplained cause. Valid alerts are data anomalies generated by surveillance tools that are due either to water contamination or public health events. If the alert was determined to be valid, then members of the users' group (described below) conducted a collaborative investigation to determine if the public health alert was related to possible drinking water contamination. When a water contamination incident could not be ruled out, the water utility's consequence management plan was activated to assess the credibility of an alert. Information on the Consequence Management Plan can be found in Water Security Initiative: Interim Guidance on Developing Consequence Management Plans for Drinking Water Utilities. 14
Formation of the Users' Group
Several key strategies were implemented to improve communication and coordination protocols for the public health surveillance component. A users' group was formed as a starting point for the component's development and operation. The purpose of the users' group was to create and expand the knowledge base that was formed by the intersection of each agency's expertise relevant to investigation of possible water contamination. Specifically, the users' group functioned to:
• • •
One of the first steps in building the users' group was to identify key agencies and personnel and request their participation. The local public health partners included representatives from the Cincinnati health, fire, and police departments; the Hamilton County Public Health Department (HCPH); the local poison control center (DPIC); and the local field office of the Federal Bureau of Investigation.
The city of Cincinnati is located in Hamilton County, so both health departments participated. The key participant from the water utility was the utility lead, who played an active role in each contamination warning system component. The utility lead had the responsibility and authority for managing certain aspects of the utility's response to an emergency (eg, a contamination threat), particularly during the initial stages of the investigation and response.
The Cincinnati public health surveillance users' group initially met bimonthly. Once the pilot had ended, the group began meeting quarterly or as needed. Benefits of the routine meetings included not only discussion of each entity's role in investigating a possible drinking water contamination incident, but also the opportunity for information exchange among the agencies involved.
Tiers of Communication and Coordination
Three tiers of involvement were identified based on lessons learned about the interactions among participating members of the users' group (Table 2). In Table 2, Tier 1 represents the core partners of the public health surveillance component, including the utility lead, local public health partners, and the poison control center. Representatives from these agencies engaged in the public health surveillance component on a regular basis and interacted directly with other Tier 1 members during regular users' group meetings, alert investigations, and drills and exercises.
Cincinnati Pilot Users' Group
Members in Tier 2 consisted of front-line data providers who regularly evaluated the data and information used by the public health surveillance component. The Tier 2 agencies provided support and data for interpretation by Tier 1 members during the investigation of a public health surveillance alert.
Tier 3 members were not involved in the day-to-day contamination warning system–related communications but provided direction to Tier 1 members regarding their role in routine operations. Tier 3 members also acted as final decision makers during response to a credible contamination incident. Water contamination is characterized as credible if there is evidence of water contamination from more than 1 independent source—for example, an unusual spike in emergency department cases with similar symptoms and a water quality monitoring alert signaling anomalous water quality conditions such as increased turbidity. Other evidence that could lead to a credible determination may include unusual water quality field test results or laboratory results. The contributing factors and resulting decisions that lead to a credible determination will be utility-specific and unique to each investigation.
Understanding the responsibilities of participant agencies and integrating them into a collective group improved the confidence and efficiency in decision making during alert investigations. Prior to the inception of the users' group in the Cincinnati Pilot, each agency was investigating anomalies based on the information readily available to that entity and was not aware of the full array of resources available at other agencies. Consequently, the breadth of the investigation and resulting decisions were limited by information resources contained at 1 agency.
The Communicator Protocol
Collaboration does not happen automatically; it must be managed. 15 Early in the evaluation phase of the Cincinnati Pilot, communication challenges between the drinking water utility and the public health response partners were identified during several drills and exercises.
During a full-scale exercise of the contamination warning system, exercise participants followed an established public health surveillance alert investigation communication protocol. This exercise highlighted issues with the existing communication protocol and demonstrated information flow limitations among partners. A major lesson learned from this exercise was the need for a better mechanism to share information between GCWW and public health partners, and the exercise demonstrated that every agency with pertinent information should have the ability to participate in a central conversation. It also became clear that all members of this group needed to be involved in deciding whether water contamination was a possible cause of a valid public health alert.
Shortly after the full-scale exercise, follow-on discussions were initiated at users' group meetings about the communication challenges experienced during the exercise. Participants agreed that a new protocol to use a central conference line, later referred to as the communicator protocol, should be established to facilitate more efficient information exchanges during investigation of possible water contamination incidents. The communicator protocol served as an information exchange via use of a pre-set emergency contact notification phone system. The Cincinnati Fire Department offered the use of, and agreed to maintain, their auto-dialer system as a mechanism to notify members of the users' group during the investigation of a public health surveillance alert. A summary of the communicator protocol is provided below:
1. Once a participant determines that a public health surveillance alert is valid and contaminated water cannot be ruled out as a possible cause, that individual can initiate the communicator protocol by calling the fire department dispatch line and providing pertinent information. 2. A designated individual at the fire department dispatch records a voice message, which is automatically sent via phone, then follow-up e-mail, to a preestablished contact list (consisting of members of the users' group). The communicator notification includes a number to call to listen to the recorded message. 3. All participants listen to the recorded message and receive further information on when and how to call in to the conference line to discuss the investigation of the public health surveillance alert.
The communicator protocol, as depicted in Figure 2 (using a generic public health surveillance alert as an example), was fully implemented in May 2009. An added benefit is that utility and public health officials may also activate the protocol for investigation of other non-water-related public health events that affect multiple agencies.
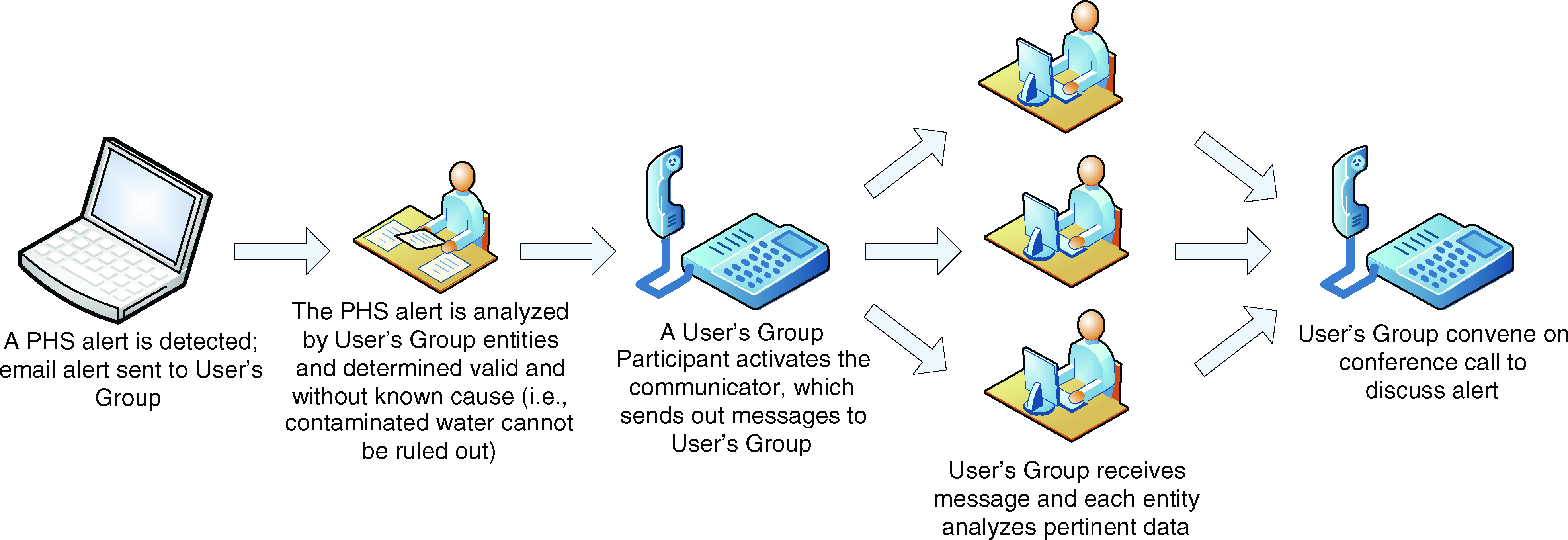
The Public Health Communicator Protocol. Color images available online at www.liebertonline.com/bsp
A Drill to Test the Communicator Protocol
The communicator protocol was tested during a public health surveillance drill in July 2009. Participants from several agencies listed in Tiers 1 and 2 in Table 2 were involved in the drill, including the utility lead, epidemiologists from the local health departments, toxicologists from the Drug and Poison Information Center, the lead project liaison from the Cincinnati Fire Department, and a representative from the local field office of the FBI. During this drill, a simulated call from a daycare center to DPIC reported that several children were exhibiting symptoms that could be related to exposure to contaminated drinking water. Since DPIC needed further information from the users' group to reach any conclusions, DPIC activated the communicator protocol to engage utility and public health partners in the public health surveillance alert investigation.
After the initial collaborative phone discussion, a follow-on discussion was scheduled to allow time for each of the participants to gather relevant information. The local public health departments and DPIC gathered information from emergency departments and infectious disease practitioners. The fire department contacted EMS units in the area. GCWW examined water quality data and customer complaint data from the affected area. During the follow-on discussion, the group concluded that the public health surveillance alerts indicated possible water contamination. Additionally, based on the case information from the simulated emergency departments, DPIC determined that the possible contaminant was likely a metal. Consequently, GCWW modified laboratory analysis protocols to prioritize testing for metals. The time that elapsed from the simulated call to DPIC to group consensus on possible water contamination was less than 90 minutes.
During postdrill discussion, participants agreed that activating the communicator protocol during the alert investigation resulted in more efficient information sharing. In addition, it allowed for those who were responsible for monitoring the data to present their findings firsthand to the overall group, which eliminated information silos that occurred when using previous communication protocols.
Implementation of the communicator protocol demonstrated the benefit of each agency's gaining familiarity with the relative expertise that participating members of the users' group could offer, and it increased confidence in the decision-making process. In this case, collective discussions allowed for more efficient resolution of alert investigations in the public health surveillance component, and no single agency was solely responsible for making the determination about possible water contamination.
Benefits of Enhanced Communication
The effectiveness of new communication and coordination strategies implemented in the Cincinnati Pilot were evaluated using several techniques once the system was fully operational and included:
• Timeline tracking during public health surveillance component drills and exercises (eg, was the investigation and response process expedited through use of new communication protocols?); • Evaluation of utility/public health partner interactions during investigations of public health surveillance alerts when the communicator protocol was activated; • Assessment of user feedback on the effectiveness of regular users' group meetings as an information-sharing forum and documentation of dual-use applications; and • Documentation of feedback provided by utility/public health participants during meetings or lessons learned workshops.
Information derived from this pilot project underscores the importance of efficient communication between the utility and public health agencies, which reinforces lessons learned from historical drinking water contamination incidents in which this link was not well established. One of the most important communication enhancements in the public health surveillance component was collaboration that occurred during joint investigations into possible water contamination when the communicator protocol was used. This provided benefits such as:
• A broadened knowledge base through interagency discussion; • Increased confidence in selection of appropriate response procedures; • Timely decision making; and • Availability of a communication tool for use during non-water-related public health events.
One other highly useful communication enhancement was the users' group, which required only the investment of staff hours to participate in meetings, drills, and exercises. Furthermore, continued collaboration during users' group meetings fostered consistency in interactions between personnel from different agencies, which can apply to investigation of water contamination or to other public health events. While the use of public health surveillance tools is effective in detecting a possible water contamination, they are of little value in the absence of effective communication protocols. Conversely, efficient and effective communication protocols between the utility and public health agencies provide benefits even in the absence of sophisticated, automated surveillance tools.
Throughout the duration of the pilot, the benefits of enhanced communication were observed. Perhaps the best example of an improved understanding of the expertise offered by one agency supporting the Cincinnati Pilot was the knowledge base demonstrated by senior toxicologists from DPIC. Although group participants were aware of DPIC's core mission as a poison control center, the utility and public health partners learned that DPIC's senior toxicologists offered an astute understanding of the symptoms caused by exposure to toxicological agents, and they possessed great skill in determining the causative agent during a hypothetical water contamination incident based on reported symptoms. In realizing the capacity of participant agencies and the roles of specific personnel in those agencies, communication protocols were tailored specifically to the strengths and functions of all participants.
Another example of enhanced communication is the relationship formed between DPIC and one of the local health departments, Hamilton County Public Health. Epidemiologists at the health department initiated a partnership with DPIC to enhance the interpretation of findings uncovered in the Hamilton County Injury Surveillance System—namely, data pertaining to unintentional poisonings. The health department began attending roundtable discussions at DPIC as a forum for sharing local injury data and soliciting feedback about trends and the most effective method(s) for presenting the data. In return, DPIC was able to use Hamilton County injury data summaries and epidemiologic expertise. Leveraging these relationships for purposes beyond the primary objective of identifying and responding to possible water contamination incidents improved the overall value of the contamination warning system to its users.
Conclusions
The sharing of technical knowledge, practical experiences, and communication strategies helped to bolster the confidence and expedite the decision-making capabilities of the users' group as a whole. Results from the pilot have shown that instead of a water utility manager becoming a quasi-expert in epidemiology, or a public health commissioner trying to use novice understanding of water quality monitoring to make important and farreaching decisions (such as issuance of a boil water advisory), the development and use of communication protocols facilitate integration of expert knowledge and joint decision making during response to an incident. This premise can be found in other scenarios, such as Boston's bioterrorism system, which focuses on collaboration at the local level and building on existing relationships for effective bioterrorism response. 16 The usefulness of these protocols is not limited to detecting water contamination or bioterrorism events and can be expanded to improve the efficacy of other projects and services administered by participating agencies.
Improved communication was a key element necessary for increasing the timeliness and effectiveness of decision making during possible water contamination incidents among the partners supporting the public health surveillance component of the Cincinnati Pilot. As demonstrated in the literature, several examples of communication challenges between utilities and public health officials have occurred during water contamination incidents, which delayed response actions. The Cincinnati Pilot provided examples of how separate organizations with a stake in drinking water quality and safety collaborated to solve potential public health problems, including possible contamination of the drinking water distribution system. The strategies described here have illustrated how an information depot has enhanced the communication protocols in the public health surveillance component of the Cincinnati Pilot.
Footnotes
Acknowledgments
We acknowledge the Greater Cincinnati Water Works and the Cincinnati Fire Department for their role in granting access to the data used for this study, and the Cincinnati Health Department, Hamilton County Public Health, the Cincinnati Drug and Poison Information Center, and the Federal Bureau of Investigation for their contributions and support during this study.