
Abstract
Biosecurity measures are traditionally applied to laboratories, but they may also be usefully applied in highly specialized clinical settings, such as the isolation facilities for the management of patients with highly infectious diseases (eg, viral hemorrhagic fevers, SARS, smallpox, potentially severe pandemic flu, and MDR- and XDR-tuberculosis). In 2009 the European Network for Highly Infectious Diseases conducted a survey in 48 isolation facilities in 16 European countries to determine biosecurity measures for access control to the facility. Security personnel are present in 39 facilities (81%). In 35 facilities (73%), entrance to the isolation area is restricted; control methods include electronic keys, a PIN system, closed-circuit TV, and guards at the doors. In 25 facilities (52%), identification and registration of all staff entering and exiting the isolation area are required. Access control is used in most surveyed centers, but specific lacks exist in some facilities. Further data are needed to assess other biosecurity aspects, such as the security measures during the transportation of potentially contaminated materials and measures to address the risk of an “insider attack.”
Biosecurity measures are traditionally applied to laboratories, but they may also be usefully applied in highly specialized clinical settings, such as isolation facilities for patients with highly infectious diseases. In 2009 the European Network for Highly Infectious Diseases conducted a survey in 48 isolation facilities in 16 European countries to determine which biosecurity measures for access control to the facility were being used.
Biosecurity measures are traditionally applied to BSL-3 or -4 laboratory settings. In these settings, the pillars of biosecurity are: (1) the physical security of the facility, such as access control and security services; (2) the security of personnel, including identity verification for those who have access to dangerous materials and the measures taken to prevent the “insider threat”—that is, the possibility that a staff member may steal biological material; and (3) material accountability and security, including the security of potentially infectious agents during handling and transport.1–3 In clinical healthcare facilities, biosecurity issues are generally not considered and are not routinely applied. But in specific, highly specialized clinical settings, such as the isolation facilities used for the management of patients with highly infectious diseases (see sidebar), the application of biosecurity measures could find a useful application, as has been suggested by European and U.S. consensus panels that discussed the construction and management of these units.4–7
The European Network for Highly Infectious Diseases (EuroNHID) project is a 42-month-long project (July 2007 to December 2010), co-funded by the European Commission network, which includes 16 member states: Austria, Bulgaria, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Luxembourg, Malta, Norway, Poland, Slovenia, Spain, and the United Kingdom. Part of the project was a series of surveys, using standardized checklists, that were conducted in 48 isolation facilities identified by national health authorities as referral centers for the management of imported or autochthonous cases of highly infectious diseases. 8 In these surveys, data about infrastructure issues of the facility, staff management, infection control procedures and resources, and the safety of healthcare workers were collected. In this article, we present the collected data about biosecurity measures for access control in these facilities.
Methods
A cross-sectional study was performed to investigate resources and capabilities on biosecurity measures for access control in 48 isolation facilities in 16 countries.
Setting and Participants
National health authorities in all European countries were contacted by the EuroNHID Coordination Team and by the European Commission; each was asked to suggest as a project partner a physician with expertise in the management of highly infectious diseases. This process resulted in the inclusion of facilities in 16 countries. Most partners are clinicians working in isolation facilities designated for referral of patients with highly infectious diseases; they collectively have backgrounds in infectious diseases, intensive care, infection control, pulmonary medicine, occupational health, epidemiology, and public health.
In order to survey only isolation facilities identified by national health authorities for the referral and management of highly infectious diseases, we asked partners to provide official documents in which these hospitals are clearly indicated. This process led to the identification of 48 isolation facilities, which represent all identified centers for all participating countries except Spain, from which only centers from Catalonia were identified (Figure 1).
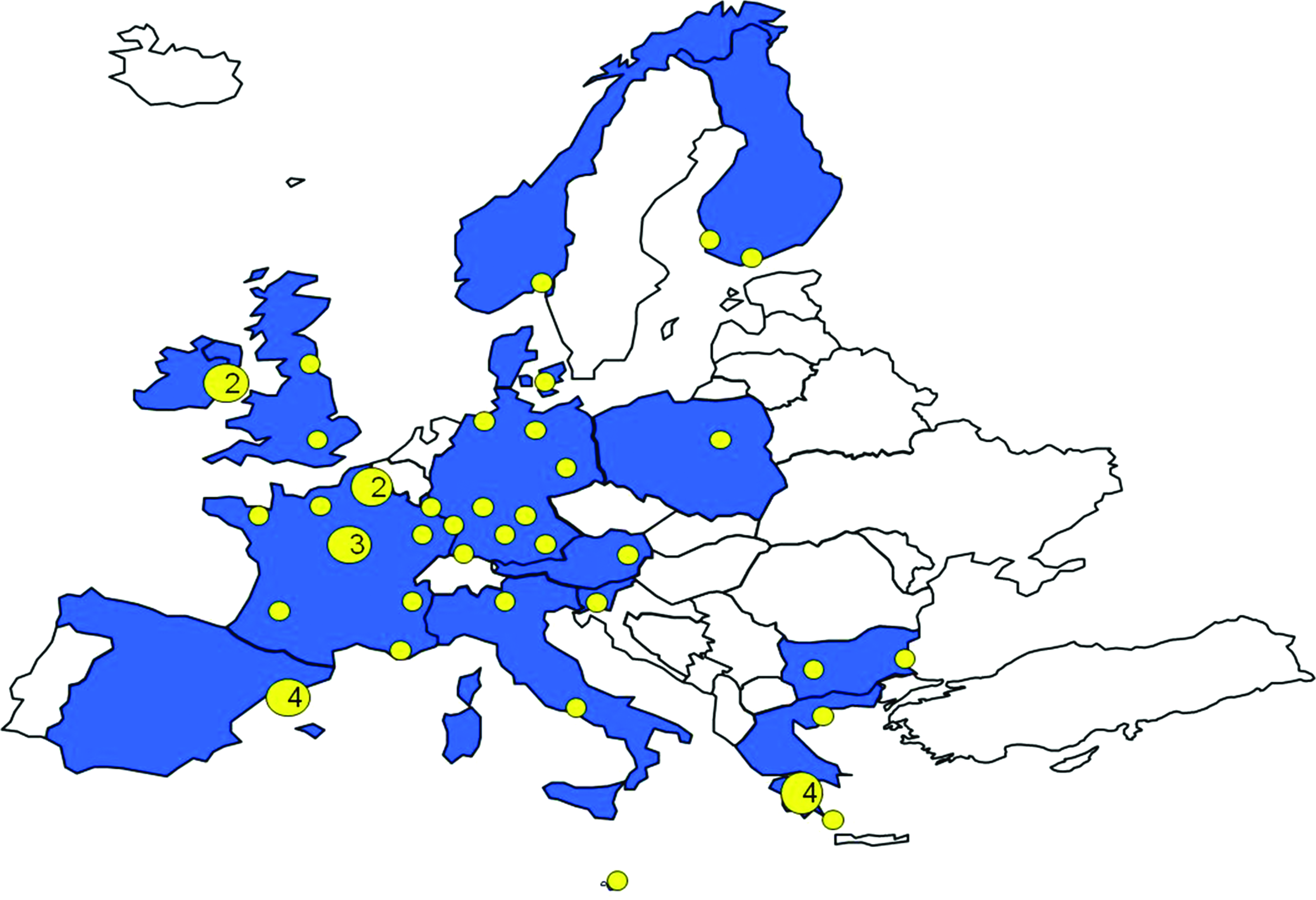
Participating Countries in EuroNHID Project (shaded) and Location of Surveyed Isolation Facilities (dots). Numbers in the dots represent the number of facilities in the same location. Color graphics available online at www.liebertonline.com/bsp
Data Collection
Data were collected during on-site visits, using a set of checklists developed during the first year of project activity. Three checklists were developed, including 16 main topics and 148 specific questions. (The checklists are available on the website www.eunid.eu, after registration, under “Documents.”) Topics that were explored were: infrastructure issues of the isolation facility, technical issues of the isolation facility, staff availability and management, administrative aspects of the isolation facility, management of personal protective equipment, hand hygiene, prevention of needle-stick injuries, transportation of patients, routine hygiene and disinfection, waste management, postmortem procedures, surge capacity, organizational and administrative aspects for healthcare workers' safety, medical aspects for healthcare workers' safety, healthcare workers' education and training, and infection control in emergency departments or medical admission departments.
All on-site visits were performed by the project coordinator together with a representative of the surveyed facility during the period from February to November 2009. The checklists were not designed to collect specific data about biosecurity. Despite that, some collected data were useful to describe the biosecurity measures for the access control to the facilities: existence of a security circuit and/or security personnel, existence of controlled access to the isolation area, methods used to control access to the isolation area, and presence of a register for ingress and egress.
Panel Recommendations
On the basis of a literature review, partners' expert opinions, and data collected during the surveys, EuroNHID developed optimal and minimal indications for biosecurity measures for access control. These indications were discussed with all partners, and a consensus agreement was reached during the final meeting, held in Rome in May 2010.
Results
Among the 48 isolation facilities, 21 reported that they had in the past managed at least 1 confirmed case, while 37 facilities reported having treated at least 1 suspected patient. Specifically, 15 cases of SARS, 6 cases of lassa fever, 4 patients with Crimea-Congo hemorrhagic fever, 3 cases of hantavirus, 2 infections with poxvirus, and 1 case of ebola fever had been managed in these isolation facilities. Moreover, while 12 isolation facilities are activated only for a suspected or confirmed highly infectious disease case, the remaining facilities routinely operate, on a daily basis, to manage other patients requiring isolation, such as those with M. tuberculosis, including multidrug resistant (MDR) and extensively drug resistant (XDR) tuberculosis cases.
We summarized available data on access control in: (1) measures for the security of the facility (ie, presence of security personnel and/or security circuit); (2) measures for assuring restricted access to the isolation area (ie, restricted entrance with any strategy of control); and (3) measures for the identification of personnel (ie, restricted entrance with appropriate strategy of control and/or presence of a registry). The distribution of these measures among the 48 isolation facilities are reported in Figure 2. All measures are in place in 14 facilities (29%), at least 2 types of measures are in place in 21 facilities (44%), and only 1 type of measure is present in 12 facilities (25%). In the remaining facility, no biosecurity measures are available.
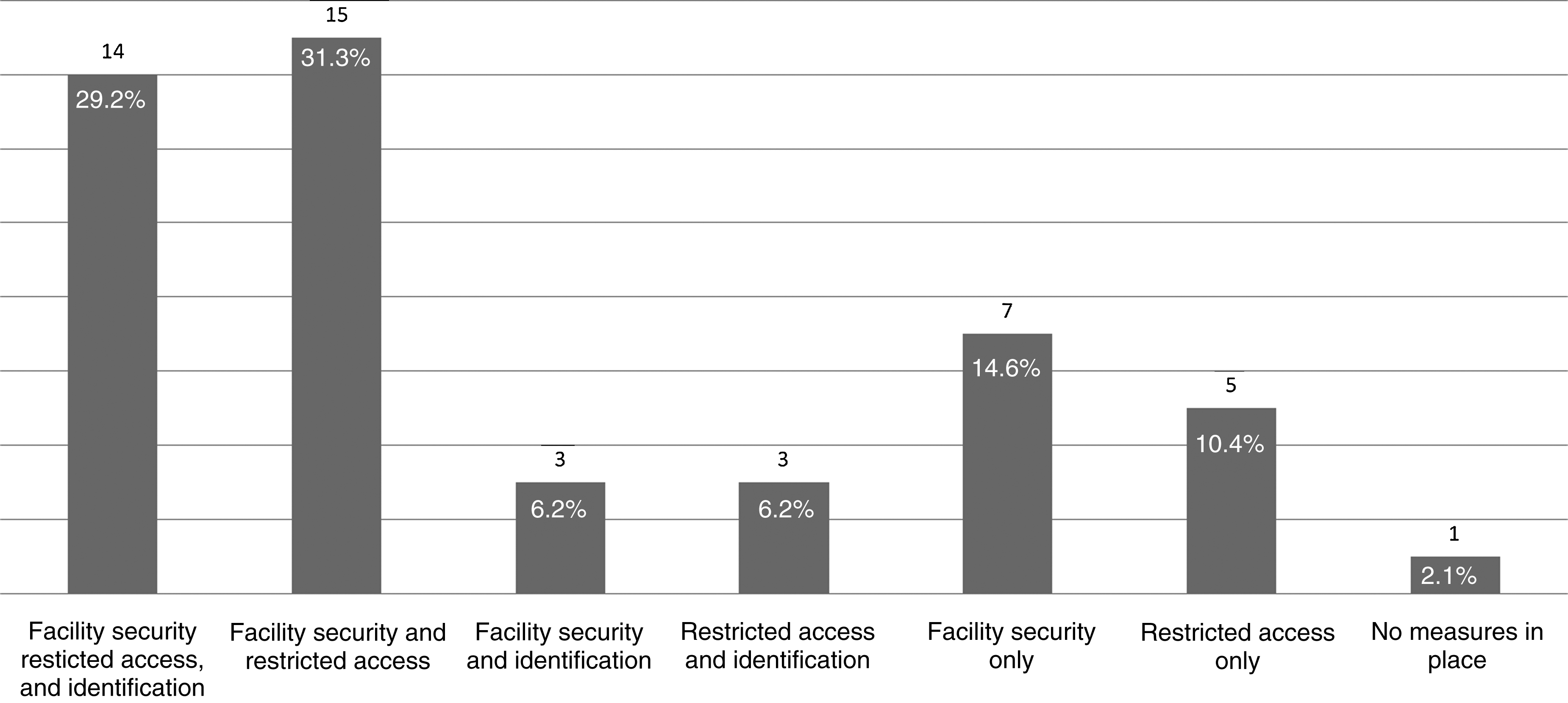
Biosecurity Measures for Access Control (Facility Security, Restricted Access, Identification) in 48 Isolation Facilities for HIDs in 16 European Countries. Facility security: presence of security personnel and/or security circuit; restricted access: restricted entrance to isolation area with any strategy of control; identification: restricted entrance with appropriate strategy (CCTV or guard) and/or presence of a registry.
Regarding measures for the security of the facility, security personnel are present in 39 facilities (81%): private, hospital-employed security guards in 29 facilities, public police officials in 5, and both private, hospital-employed guards and public policemen in the remaining facilities. No information was collected on how security personnel were recruited and selected. In 10 (21%) isolation facilities, mainly in those located in a stand-alone building, security circuits, reinforced by a permanent gate or by mobile, nonpermanent fences, are also available.
Thirty-five facilities (73%) restricted access to the isolation area by use of a separate, dedicated entrance. Different methods are in place for the control of entrance to the isolation area, and in some facilities more than 1 strategy is used: electronic keys are used in 22 facilities, a PIN (personal identification number) system is in place in 6, a closed-circuit TV (CCTV) for the control of the identity of people entering is in place in 4, while 3 have guards at the doors. Some of these measures (such as CCTV and guards at the doors) may also prevent the patient being kept in isolation from spontaneously leaving the facility, although specific data about this point have been not collected.
In 25 facilities (52%), it is possible to identify people entering the isolation area. This is done through a registry for ingress and egress in 18 facilities, or through CCTV or guards at the door in 3 facilities; 4 facilities use both systems.
No data were collected to address the “insider threat.” As a “proxy,” 10 facilities (21%) reported that they perform a psychological attitude interview with all healthcare workers when they are selected for being part of the group working in the isolation area, even if this interview is more targeted to identify team working attitude and ability to work under stressful conditions, rather than the intent of the healthcare worker to commit a malevolent act.
Infectious material, in particular diagnostic specimens, may be stolen during storage, or during transport within or outside of the isolation area. Indeed, the majority of surveyed facilities use external facilities for diagnostic procedures. Only 1 facility (2%) reports having a BSL-4 laboratory in the same center, while 24 facilities (50%) report having a BSL-4 laboratory in the country or having an agreement with a BSL-4 in another country, with transport distance ranging from 0.5 to 800 kilometers. The picture regarding the availability of BSL-3 laboratory facilities is similar: 32 facilities (67%) need to transport specimens from 0.5 to 600 kilometers away. Also specimens for microbiological and routine tests are mostly transported to the central hospital laboratory, while these tests are performed within the isolation area in only 13 facilities. Data about who performs the transport are available from 44 facilities: hospital staff has this duty in 24 facilities, a private courier is used by 10 facilities, and a government body by 1 facility; in the remaining 9, different solutions are used according to risk assessment or regional/national regulations. Specific data about biosecurity measures in place during transport are lacking.
Discussion
Need for Biosecurity Measures
Biosecurity measures are usually applied in laboratory settings where BSL-3 and -4 agents, which could be used for bioterrorism attacks, are handled. Indeed, it is assumed that a person (or a group of people) with intent to harm, having stolen biological material from a laboratory, may have the technological capability to transport, store, replicate, and finally to transform it into a biological weapon.1,2 Thus, this process is possible also starting from blood or other body fluids or tissues of hospitalized patients with highly infectious diseases such as ebola or Marburg virus.
Biosecurity resources and capabilities in high-level laboratories have been surveyed and assessed, 9 but specific studies have not been conducted in clinical isolation facilities, nor do specific international mandatory standards exist, despite the fact that special attention and specific measures dedicated to biosecurity are currently advocated in all recommendations for the construction and management of high-level isolation facilities.4–7
Biosecurity measures should find an application in these highly specialized clinical settings, especially in the isolation facilities identified by National Health Authorities for referring patients with highly infectious diseases: the event of a real patient with a highly infectious disease had occurred in about half of these facilities. Specimens from these patients may contain a high concentration of agents that could potentially be used as a biological weapon. Moreover, despite the fact that usually samples and cultures are not stored in the clinical isolation area but are sent to BSL-3 or -4 laboratories, the samples may be stored for some hours, or even days, in the facilities where some tests are available at bedside, during the management of the patient. This represents a further reason for effective access control.
Biosecurity measures for access control may contribute to reducing the risk of material theft from the facility. Moreover, these measures may be useful in these special settings to avoid allowing access to anyone other than authorized staff (eg, visitors, patients' relatives, journalists) in the isolation area. In real life, cases of highly infectious disease usually stimulate a great interest in the general public; thus, mass media reporters may be interested in entering an isolation area, even if they are not authorized to do so.10–12
Limits of Our Study
Our study did not collect complete data about the effective continuum of measures essential for adequate biosecurity. In particular, our article focuses on measures for access control to the isolation area, whereas an effective biosecurity approach should also include other aspects, such as specific training, implementation of standard operating procedures, periodic inspections, laboratory/facility records and inventories for acquisition and destruction of highly infectious pathogens, and measures taken during the handling and transportation of these agents. Moreover, specific strategies should be developed to address the threat of an “insider attack,” in which a member of the staff may misuse the infectious material. Further studies are needed to assess these other aspects.
Interpretation of Our Results
Despite these limits, some comments are possible. The vast majority of facilities have some security measures for access control, while in only 1 facility these measures are not in place. Most of these measures are probably in place mainly for reasons other than biosafety—for example, to limit the number of potentially exposed personnel—but they may easily be applied for biosecurity purposes. A significant proportion of facilities have the capacity to identify individuals who enter and leave the unit, which would assist in deterring theft from the clinical and laboratory areas. The explored measures would also contribute to reducing the risk of an “insider attack.”
Indications for Biosecurity Measures for Access Control
Biosecurity measures should be based on comprehensive protocols, including the security of the infrastructure itself, the restriction of access, the identification of personnel authorized to have access, the inclusion of biosecurity issues into healthcare worker training, external audits and exercises, a documentation of internal and external storage and movements of specimens and all potentially contaminated items, and strategies for preventing malevolent acts by staff members themselves.
Most of these measures are expensive and time-consuming, but they may be activated only when a patient with a suspected or confirmed highly infectious disease is admitted. However, the construction and the maintenance of an isolation facility itself is expensive. The choice to have a such specialized unit should rest on its strategic relevance and on the existence of strategies for its day-to-day use.
Currently, no widely accepted standards for biosecurity measures in clinical facilities have been produced by an international regulatory body, despite the fact that such a guideline is needed. In order to contribute to the development of complete recommendations about biosecurity in clinical facilities, the EuroNHID group produced a set of indications for adequate measures for access control.
In particular, to control access, several methods are useful, and the most used are electronic keys and PIN access code at the doors. However, for biosecurity purposes, these methods are not optimal, because electronic keys may be stolen or lost, and PIN numbers may be communicated to or extorted by an unauthorized person. Optimal methods include retina or fingerprint scanning devices, or the presence of a CCTV or guard at the doors. People responsible for biosecurity should be clearly identified, and the involvement and roles and responsibilities of public health and security authorities in the event of a security infraction should be clearly defined.
Basic biosecurity training, together with biosafety and infection control training, should be provided to all personnel on a regular basis and should include periodic exercises; such training should help personnel understand the need for protection of such materials and the rationale for specific biosecurity measures. Procedures describing security roles, staff responsibilities, and consequences in the event of a security infraction should also be presented during training.
Detailed strategies, including procedures for a rapid alarm, should be applied during the transport of contaminated material containing highly infectious agents, such as diagnostic specimens. According to our results, the vast majority of facilities need to transport specimens elsewhere, in some cases hundreds of kilometers away, for diagnosis.
It has been observed that the “insider threat” is a major component of biosecurity risk, so biosecurity measures should also take into account the possibility of an attack from a member of the staff. 13 No “magic bullet” exists to identify this threat, but a psychological and attitude pre-employment interview and brief research about personal background may reduce the risks. Another element of prevention is for laboratory workers to always work in pairs; this is more common in clinical settings than in the laboratory. Indeed, this practice has been discussed and criticized in laboratories,14,15 but we believe that, in isolation facilities, at least 2 healthcare workers should always be present in the isolation area, for both biosafety and biosecurity reasons.
Detailed EuroNHID indications for appropriate biosecurity measures for access control in isolation facilities are summarized in Figure 3.
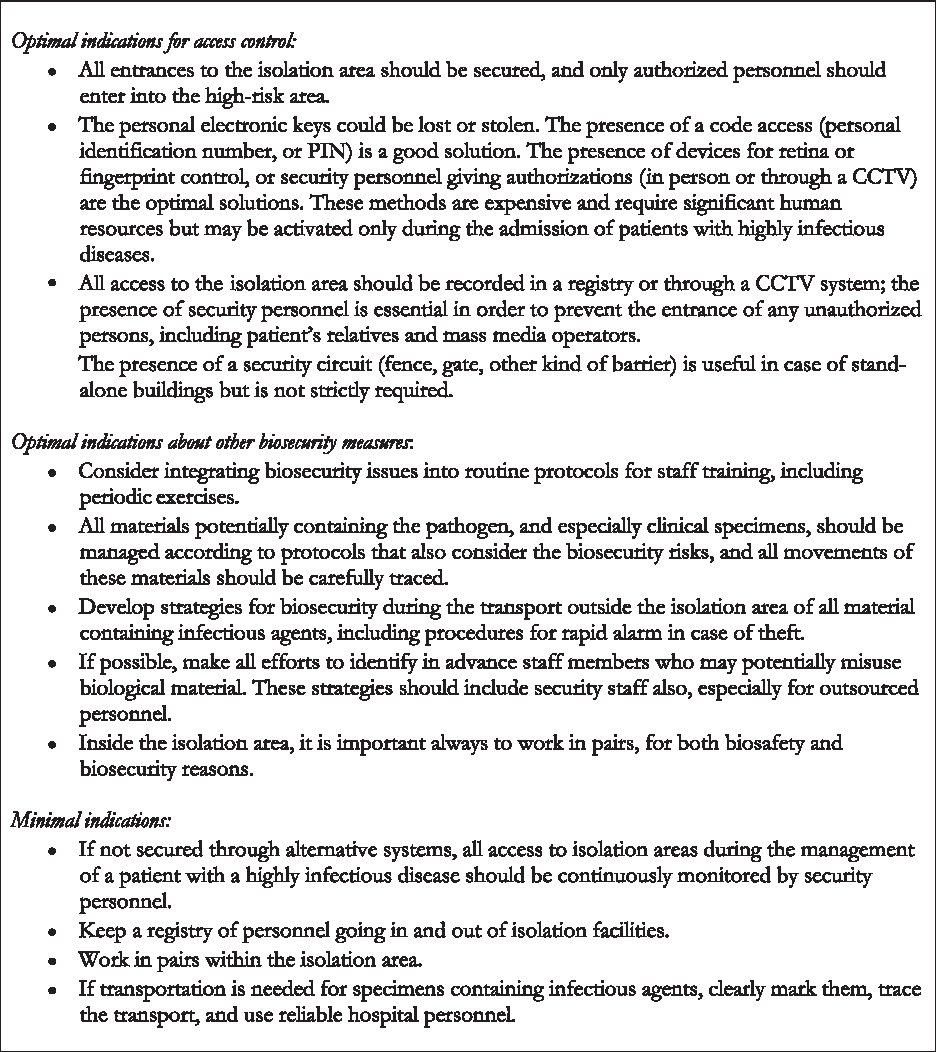
EuroNHID Indications for Appropriate Biosecurity Measures for Access Control
Footnotes
Acknowledgments
We acknowledge Ms. Ramona Iacovino for her administrative support during the project. Additional members of EuroNHID Working Group who contributed to data are Norbert Vetter (Austria), Mira Kojouharova (Bulgaria), Kremena Parmakova (Bulgaria), Peter Skinhoej (Denmark), Heli Siikamaki (Finland), Christian Perronne (France), Olga Adrami (Greece), John Lambert (Republic of Ireland), Simone Lanini (Italy), Robert Hemmer (Luxembourg), Michael Borg (Malta), Anne Lise Fjellet (Norway), Arne Broch Brantsæter (Norway), Andrzej Horban (Poland), Franc Strle (Slovenia), and Antoni Trilla (Spain). This work was supported by the EC grant EuroNHID (2006205) and by the Ministero della Salute, Italia-Ricerca Corrente, Istituti di Ricovero e Cura a Carattere Scientifico.