
Abstract
Rapid public health response to a large-scale anthrax attack would reduce overall morbidity and mortality. However, there is uncertainty about the optimal cost-effective response strategy based on timing of intervention, public health resources, and critical care facilities. We conducted a decision analytic study to compare response strategies to a theoretical large-scale anthrax attack on the Chicago metropolitan area beginning either Day 2 or Day 5 after the attack. These strategies correspond to the policy options set forth by the Anthrax Modeling Working Group for population-wide responses to a large-scale anthrax attack: (1) postattack antibiotic prophylaxis, (2) postattack antibiotic prophylaxis and vaccination, (3) preattack vaccination with postattack antibiotic prophylaxis, and (4) preattack vaccination with postattack antibiotic prophylaxis and vaccination. Outcomes were measured in costs, lives saved, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratios (ICERs). We estimated that postattack antibiotic prophylaxis of all 1,390,000 anthrax-exposed people beginning on Day 2 after attack would result in 205,835 infected victims, 35,049 fulminant victims, and 28,612 deaths. Only 6,437 (18.5%) of the fulminant victims could be saved with the existing critical care facilities in the Chicago metropolitan area. Mortality would increase to 69,136 if the response strategy began on Day 5. Including postattack vaccination with antibiotic prophylaxis of all exposed people reduces mortality and is cost-effective for both Day 2 (ICER=$182/QALY) and Day 5 (ICER=$1,088/QALY) response strategies. Increasing ICU bed availability significantly reduces mortality for all response strategies. We conclude that postattack antibiotic prophylaxis and vaccination of all exposed people is the optimal cost-effective response strategy for a large-scale anthrax attack. Our findings support the US government's plan to provide antibiotic prophylaxis and vaccination for all exposed people within 48 hours of the recognition of a large-scale anthrax attack. Future policies should consider expanding critical care capacity to allow for the rescue of more victims.
Rapid public health response to a large-scale anthrax attack would reduce overall morbidity and mortality, but what is the optimal cost-effective response strategy for timing of intervention, public health resources, and critical care facilities? Using a hypothetical large-scale anthrax attack on the Chicago metropolitan area, this study compared response strategies that would begin either 2 days or 5 days after the attack and would consist of administering prophylaxis and vaccine in various combinations. The findings support the government's plan to provide antibiotic prophylaxis and vaccination for all exposed people within 48 hours of the recognition of a large-scale anthrax attack.
Because of the lack of empirical information from actual large-scale anthrax attacks, both CDC and the Institute of Medicine have recommended computational modeling and simulation studies to assess several public health response strategies for mitigating the effects of an anthrax attack.9,10 Prior modeling and simulation studies have indicated that rapid response to an anthrax attack significantly reduces morbidity and mortality, with estimated effects of various strategies dependent on model parameters and timing of the response.11–15 For example, Wein et al estimated that 1 kilogram of anthrax spores released upwind of 11.5 million persons would result in 123,400 deaths if the public health response began on Day 2 after an attack, but the number of deaths would more than double if the response was delayed until Day 5. 11 Other studies evaluated the comparative cost-effectiveness of various response strategies and found important advantages in responding rapidly and combining postattack vaccination with antibiotic prophylaxis for anthrax exposed victims.16–20 Unfortunately, none of these prior studies simultaneously evaluated the costs and effects of response strategies to a large-scale anthrax attack based on (1) timing of the public health intervention, (2) numbers of emergency staff and clinics needed for mass postexposure prophylaxis, and (3) the impact of available critical care facilities. Consequently, it is not clear how mass postexposure prophylaxis and critical care facilities should be used to develop the optimal cost-effective public health response strategy to a large-scale anthrax attack.
We conducted this study to evaluate the comparative cost-effectiveness of time-varying public health response strategies for a large-scale anthrax attack perpetrated on the Chicago metropolitan area. Four strategies were evaluated with response beginning either Day 2 or Day 5 after an attack: (1) postattack antibiotic prophylaxis, (2) postattack antibiotic prophylaxis and vaccination, (3) preattack vaccination with postattack antibiotic prophylaxis, and (4) preattack vaccination with postattack antibiotic prophylaxis and vaccination. We used the attack scenario of the Anthrax Modeling Working Group developed by researchers from Sandia National Laboratory to determine CDC's Strategic National Stockpile requirements.14,15 To enhance the validity of our findings, we simulated the effects of a theoretical large-scale anthrax attack on an actual population and included specific numbers exposed to anthrax, current information on population size and dynamics, available facilities for treating critically ill victims, and the numbers of emergency staff and clinics required to implement each public health response strategy.
Methods
Study Design and Markov Models
We used Markov decision analytic models to quantitatively estimate and compare the cost-effectiveness of various time-varying public health response strategies to a large-scale anthrax attack on the Chicago metropolitan area. Decision trees for the Markov models were created based on information from the following sources: (1) a previously developed attack scenario, (2) an inhalational anthrax disease progression model, and (3) mass postexposure prophylaxis models. These sources are described in detail below.
Following the recommendations of the Panel on Cost-Effectiveness in Health Care, we adopted a societal perspective with 3% annual discount for outcome costs. We also incorporated a 1% yearly probability of a large-scale anthrax attack with specific annual birth, death, in-migration, and out-migration rates per year over 10 years. 21 The analyses were conducted using TreeAge Pro 2005 (Williamstown, MA) and were based on best available evidence on model parameters (Table 1).22–45 Findings were expressed as costs in 2008 US dollars, lives saved, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratios (ICERs) calculated as the incremental cost per QALY. The willingness-to-pay threshold was set at $100,000/QALY gained.
Model Parameters for Cost-Effectiveness Analysis of Response Strategies for a Large-Scale Anthrax Attack on the Chicago Metropolitan Area
Attack Scenario
Scenario development is used by the Department of Health and Human Services (HHS) to assess response strategies for potential bioterrorism attacks. 46 To estimate the probabilities of morbidity and mortality based on various response strategies to a large-scale anthrax attack on the Chicago metropolitan area, we used the attack scenario of the Anthrax Modeling Working Group, which postulates an atmospheric dispersal of 1 kilogram of B. anthracis spores over a large metropolitan city exposing 1.39 million persons to various amounts of spores. The resultant model had the following parameters: (1) approximately 1014 spores are released with 50% dissemination efficiency, (2) a probit dose-response of 0.7, (3) a building protective factor of 50, and (4) 85% of people are indoors and inhale only 2% as many spores as the 15% of people outdoors.
We also incorporated information on population dynamics and hospital facilities of the Chicago metropolitan area (ie, Cook, Dekalb, Dupage, Grundy, Kane, Kankakee, Kendall, Lake, McHenry, and Will counties in Illinois and Lake County, Indiana) to more accurately estimate measures of morbidity, mortality, and costs (Table 1).
Disease Progression Model
We developed a mathematical disease transition state model using Microsoft Excel Version 2003 software programming to estimate numbers of victims progressing through discrete clinical states of inhalational anthrax at various time points after anthrax spore exposure.47–49 The disease progression and sensitivity analyses were constructed in Excel using standard logical operators. No macros or customized programming were used. The model also included states for victims removed from disease progression because of insufficient spore inhalation, antibiotic prophylaxis, vaccination, or critical care. The disease progression model, with definitions and descriptions of the transition states, is presented in Figure 1. Transitions along the states were determined by time course probability estimates of progression or resolution of clinical manifestations of inhalational anthrax from published studies.50–53 This disease progression model also was the basis for the decision trees incorporated in our Markov model analyses.

Inhalational Anthrax Disease Transition State Model, with both progression and resolution states from base-case estimates from a large-scale attack on the Chicago metropolitan area. Estimates consider a public health response of postattack antibiotic prophylaxis only that begins on Day 2 after an attack and is completed within 48 hours with 50% of the 2,655 ICU beds available to provide critical care. Estimates of victims in the disease transition states vary depending on timing of response, type of strategy, and available ICU beds.
Calculations assumed a large group of exposed people who inhaled sufficient spores to cause progression through the clinical disease states based on the availability of vaccination and antibiotic prophylaxis or treatment. Victims could progress only 1 state per day and could not return to a previous state. This model is based on econometric methods of assessing cascade movement through tiered processes. 54 For each disease state, the proportion of the victims progressing to the next state was determined by probabilities selected to match disease progression estimates of the Anthrax Modeling Working Group attack scenario.14,15 Other clinical manifestations of anthrax (eg, cutaneous anthrax) were not considered in our analyses because they do not occur as rapidly as inhalational anthrax and would nevertheless be treated with antibiotics.
The programmed model also assessed response strategies beginning any postattack day with changes in the probabilities of disease progression states (ie, infected, prodromal, fulminant, and dead) or resolution states (ie, cleared, recovered, or rescued), described in Figure 1. For the infected and prodromal states, probability of resolution increased linearly as determined by input days to maximum efficacy of each response strategy. For all fulminant victims, the programmed model limited access to critical care based on available intensive care unit (ICU) beds in the Chicago metropolitan area and estimates of hospital preparedness and surge capacity.55–59 Because no published information exists on ICU bed availability under the assumption of large-scale mass anthrax attack circumstances, we assumed 50% of the 2,655 ICU beds in the Chicago metropolitan area would be available to provide critical care to fulminant victims based on our clinical and administrative experience. Remaining ICU beds would continue to provide critical care for patients with other serious medical conditions. After an attack, ICU beds would be filled with inflows of only fulminant victims who would either be rescued or die in the following 2.5 days (estimated average duration of critical care). Newly available ICU beds would be immediately filled by victims entering the fulminant state. If all ICU beds are filled, fulminant victims do not receive critical care and they progress to death. Fulminant victims receiving critical care would be rescued based on the survival rate (58.3%) of recent inhalational anthrax cases.36–38 Rescued ICU victims would then receive 10 days of non-ICU inpatient care.
Our estimates of the number of ICU and non-ICU hospital days are less than those received by the inhalational anthrax victims from 2001 because we believe clinicians and administrators would hasten the movement of patients through limited healthcare facilities in disaster situations where large numbers of victims would be awaiting critical care. We assumed that victims in the infected and prodromal states would not require hospitalization because these victims would require only oral antibiotics that could be administered in outpatient settings or at home. In addition, in a large-scale anthrax attack, it is unlikely hospitals could provide care for victims who could be cared for as outpatients.
Response Strategies
Four public health response strategies, corresponding to the policy options set forth by the Anthrax Modeling Working Group for a large-scale anthrax attack,14,15 were evaluated for comparative cost-effectiveness: (1) postattack antibiotic prophylaxis of all exposed people, (2) postattack antibiotic prophylaxis and vaccination of all exposed people, (3) preattack vaccination of the Chicago metropolitan area population with postattack antibiotic prophylaxis of all exposed people, and (4) preattack vaccination of the Chicago metropolitan area population with postattack antibiotic prophylaxis and vaccination of all exposed people. We also evaluated the cost-effectiveness of these response strategies beginning either on Day 2 (requiring 2 days to complete) or Day 5 (requiring 6 days to complete).
The 2 strategies with preattack vaccination used anthrax vaccine adsorbed (AVA) given in a series of 3 doses by primary care physicians over a 6-month period followed by yearly booster inoculations for 10 years. We assumed the preattack vaccination program would cover 30% of the Chicago metropolitan area population and would be 92.5% effective (estimated from the only human field trial of anthrax vaccine effectiveness). 60 Postattack antibiotic prophylaxis, vaccination, or both would be provided to all exposed people (including those infected or clinically prodromal) by emergency dispensing clinics over a 2-day period starting on Day 2 or over a 6-day period starting on Day 5 to match calculations of Anthrax Modeling Working Group scenarios. Response strategies using vaccination also include a second postattack clinic visit after 2 weeks to revaccinate all exposed people.
As part of the Anthrax Modeling Working Group calculations, the postattack vaccination program employs 2 inoculations of AVA given to 100% of exposed victims and was considered to be 90% effective in preventing death if given before the development of fulminant inhalational anthrax. 14 The postattack antibiotic prophylaxis program employs 60 days of oral ciprofloxacin to be dispensed to all exposed people. We assumed postattack antibiotic adherence would be 25% for 60 days, 25% for 45 days, 25% for 30 days, 15% for 15 days, and 10% for no days according to the Anthrax Modeling Working Group model.14,15 Notwithstanding this limited compliance, the costs for a 60-day supply of ciprofloxacin to be dispensed to all exposed people were included in the analyses. All victims in the fulminant stage at the time of available postattack prophylaxis would not receive either antibiotics or vaccination, but would instead receive ICU care if available as described above.
Mass Prophylaxis Staff and Clinic Requirements
CDC plans for mass prophylaxis of all exposed victims from a large-scale anthrax attack through the rapid dispensing of antibiotics and vaccinations using emergency point-of-dispensing (POD) clinics.8,61 Staff and number of POD clinics required to implement such a program can be estimated using computer simulations. 62 We estimated these numbers for the 4 response strategies using the Bioterrorism and Epidemic Outbreak Model (BERM Version 2.0) software program developed by the Agency for Healthcare Research and Quality (AHRQ) and recommended by CDC to formulate realistic mass antibiotic prophylaxis and vaccination dispensing plans.63,64 BERM predicts the number of staff and POD clinics needed to respond to a major disease outbreak or bioterrorism attack on a given population based on specific input parameters. Our estimates incorporated parameters on population size, duration of intervention, hours of POD clinic operation, number of work shifts per day, number of briefing and treatment rooms, room capacities, and lengths of briefing and treatment. Postattack antibiotic prophylaxis, vaccination, or both would be provided to all noncritically ill (ie, exposed, infected, and prodromal) people over a 2-day period starting on Day 2 or a 6-day period starting on Day 5 after the attack. Fulminant and dead people were excluded from estimates requiring mass postexposure prophylaxis. The second postattack clinic visit would occur 2 weeks after the first clinic visit, but the second vaccination dose would be given only to noncritically ill people over 6 days for both Day 2 and Day 5 response strategies.
Antibiotic, Vaccination, and Medical Treatment Costs
Medical costs were estimated in 2008 US dollars and adjusted as needed using the medical care component of the Consumer Price Index. 65 Hospital and ICU costs were based on mean daily hospitalization costs for adults, derived from the AHRQ Cost and Utilization Project—Nationwide Inpatient Sample. 39 Outpatient visit costs were based on 2008 Medicare physician charges for an established patient visit using the Current Procedural Terminology (CPT) code 99214. 34 Costs for postexposure ciprofloxacin prophylaxis were based on Bayer's current average wholesale price. 35 Vaccination dosage costs are $24.50 each for the initial 3-dose series and for the annual booster for 10 years. 33 Costs for POD staff for distribution of antibiotic prophylaxis and vaccinations were calculated at $14.20/person-hour. 40 A summary of all modeled costs is presented in Table 1.
Vaccination Adverse Effects
Mild side effects from preattack vaccination were defined as those treated with 1 physician visit in an outpatient setting; severe side effects were those treated with inpatient care. The models assumed that mild and severe vaccine side effects occurred in less than 0.05% of the population as estimated from reports of adverse events in the US military. 66 In a large-scale anthrax attack, it is unlikely that side effects from postattack antibiotic prophylaxis or vaccination would receive treatment in a healthcare system overwhelmed by the patients with inhalational anthrax. Therefore, assessments for postexposure antibiotic prophylaxis and vaccination side effects were not included in the models.
Quality-of-Life Adjustments
Short-term adjustments in quality of life (QOL) were made for the mild side effects of preattack vaccination based on utilities reported for similar health states.31,32 A quality-of-life adjustment was also made for patients with fulminant inhalational anthrax. Using published standardized estimates, we selected a value 1 standard deviation below the mean utility reported for acute illness to capture the impact on quality of life of having an illness with a high probability of fatality. 31 Long-term adjustments were based on reports from inhalational anthrax survivors 1 year after their infection who reported a quality of life that was 60% of the norm value. 32 Utility for the postfulminant inhalational anthrax state was estimated to be 0.6 and assumed in the base-case analysis to persist at this level for a 10-year period. The QALY and ICER estimates included losses from the inhalational anthrax–related deaths but were not age-adjusted.
Sensitivity Analyses
Sensitivity analyses were conducted to assess changes in the cost-effectiveness estimates by varying probability of attacks, costs, utilities, side effects, ICU days, and hospital days. Monte Carlo simulations of 1,000 randomly selected observations were conducted by varying these variables simultaneously under the Day 2 and Day 5 response strategies to assess the sensitivity of the results over a range of possible parameter values. Uniform distributions were assumed for each variable. Cost-effectiveness acceptability curves were then constructed to calculate the percentages of simulated anthrax attack responses that would be cost-effective for preattack vaccination of the Chicago metropolitan area over a willingness to pay range of $0 to $300,000, using Monte Carlo simulations with annual probabilities of attack of the Chicago metropolitan area of 0.1%, 1%, and 10%.67,68 We also estimated the effects of increasing the number of ICU beds available for treatment of fulminant cases on the number of deaths from inhalational anthrax for the Day 2 and Day 5 postattack response strategies. In addition, we compared the effects of varying the numbers of available ICU beds for the Day 2 and Day 5 postattack response strategies over a wide range of initial anthrax-infected victims.
Results
The base-case scenario describes a large-scale bioterrorist anthrax attack on the Chicago metropolitan area population of 9,296,847, with a public health response strategy that incorporates postattack antibiotic prophylaxis (without vaccination) of 1,390,000 exposed persons starting on Day 2 postattack and taking 2 days to complete (Figure 1). This scenario would result in 205,835 infected victims, 35,049 victims developing fulminant inhalational anthrax, 28,612 deaths, and only 6,437 (18.5%) of the fulminant victims rescued if 50% of the 2,655 ICU beds in the Chicago metropolitan area were available to provide critical care. The number of rescued victims would increase only to 9,895 (28.2%) if 90% of ICU beds in the Chicago metropolitan area were available.
Transition state morbidity and mortality estimates for all 4 strategies are presented in Table 2. Delaying initiation and completion of the public health response from Day 2 (with 2 days to complete) to Day 5 (with 6 days to complete) would significantly increase overall morbidity and mortality estimates for all 4 response strategies. However, including postattack vaccination with antibiotic prophylaxis of all 1.39 million exposed persons would significantly reduce mortality estimates for all response strategies starting at either Day 2 or Day 5. We also estimated that morbidity and mortality would be lower for all response strategies if 30% of the Chicago metropolitan area population were vaccinated for anthrax before a large-scale attack.
Disease Progression Transition State Estimates for a Large-Scale Anthrax Attack on the Chicago Metropolitan Area Based on Response Strategies and Timing of Intervention
Note. Attack would result in 1.39 million persons exposed among the Chicago metropolitan area population of 9,296,847. Preattack vaccination would cover 30% of the population and would be 92.5% effective. Postattack antibiotic prophylaxis, vaccination, or both would be provided to all exposed people by point-of-dispensing (POD) clinics over a 2-day period starting on Day 2 or over a 6-day period starting on Day 5. Estimations also assume 50% of the 2,655 intensive care unit (ICU) beds in the Chicago metropolitan area would be available to provide critical care to fulminant victims.
Estimates of staff and POD clinics required to implement the various response strategies were based on the number of exposed victims who have yet to develop fulminant manifestations or die before public health interventions are initiated (Table 3). Response strategies beginning on Day 2 would require significantly more dispensing clinics than strategies beginning on Day 5 in order to provide mass postexposure prophylaxis to a similar number of victims over a shorter period (ie, 2 versus 6 days). In addition, response strategies that include postattack vaccination of exposed people would require more staff person-hours because of the added time needed to provide vaccination with antibiotic prophylaxis during the first clinic visit and the necessity for a second clinic visit for revaccination of these victims.
Year 1 Estimates of Staff and Point of Dispensing (POD) Clinics Required for a Large-Scale Anthrax Attack on the Chicago Metropolitan Area Based on Response Strategies and Timing of Intervention
Note. The first postattack intervention would provide antibiotic prophylaxis or antibiotic prophylaxis and vaccination to all surviving exposed victims by emergency point-of-dispensing (POD) clinics over a 2-day period starting on Day 2 or over a 6-day period starting on Day 5. The second postattack intervention would occur 2 weeks later and provide only vaccinations to all surviving exposed victims over a 6-day period. The Bioterrorism and Epidemic Outbreak Model assumes 24-hour per day POD clinic operation, 2 12-hour work shifts per day, 15% downtime, 10-minute briefing period for either antibiotic prophylaxis or vaccination alone (20 minutes in combination for both), and an average flow rate of 20 patients per minute per POD clinic.
Cost-effectiveness estimates calculated using Markov models for the 4 response strategies beginning either Day 2 or Day 5 are presented in Table 4. We found that postattack antibiotic prophylaxis is overall the least costly strategy, but the addition of postattack vaccination of exposed people is cost-effective when begun either on Day 2 ($182/QALY) or Day 5 ($1,088/QALY) after an attack. We also found the addition of preattack vaccination in the response strategies was not cost-effective (ie, ICER>$100,000/QALY), even with a plausible risk of a large-scale anthrax attack on the Chicago metropolitan area (1%/year over the 10-year study period). More specifically, we estimated that the addition of preattack vaccination to postattack antibiotic prophylaxis and vaccination is cost-effective (ie, ICER<$100,000/QALY) only when the probability of attack is greater than 1.85%/year for Day 2 and greater than 1.30%/year for Day 5 response strategies. Thus, delaying initiation of the response from Day 2 to Day 5 increases the attractiveness of adding the preattack vaccination component to the postattack antibiotic prophylaxis and vaccination response strategy.
Cost-Effectiveness Estimations of Response Strategies Over 10 Years for a Large-Scale Anthrax Attack on the Chicago Metropolitan Area Based on Timing of Intervention
Note. Dominated implies other strategies are less costly and more effective and thus are eliminated from further consideration in a cost-effectiveness analysis. Extended dominated implies more effective strategies have lower incremental cost-effectiveness ratios.
In general, our cost-effectiveness findings were not sensitive to one-way variations in the cost-effectiveness model parameters (Table 5). An important exception was the markedly improved cost-effectiveness of including preattack vaccination in the response strategies with increased probability of an attack. The cost-effectiveness acceptability curves in Figure 2 more clearly illustrate these effects. For the base-case 1% yearly probability of attack, including preattack vaccination with postattack antibiotic prophylaxis and vaccination is only 7.0% likely to be cost-effective at the $100,000/QALY threshold for the Day 2 response strategy and 16.3% likely for the Day 5 response strategy. Both of these probabilities increase slowly for increasing willingness to pay thresholds. At a 0.1% yearly probability of attack, preattack vaccination is not cost-effective in nearly all simulations with either Day 2 or Day 5 response strategies. However, at 10% yearly probability of attack, including preattack vaccination is cost-effective for nearly all simulations with both Day 2 and Day 5 response strategies.
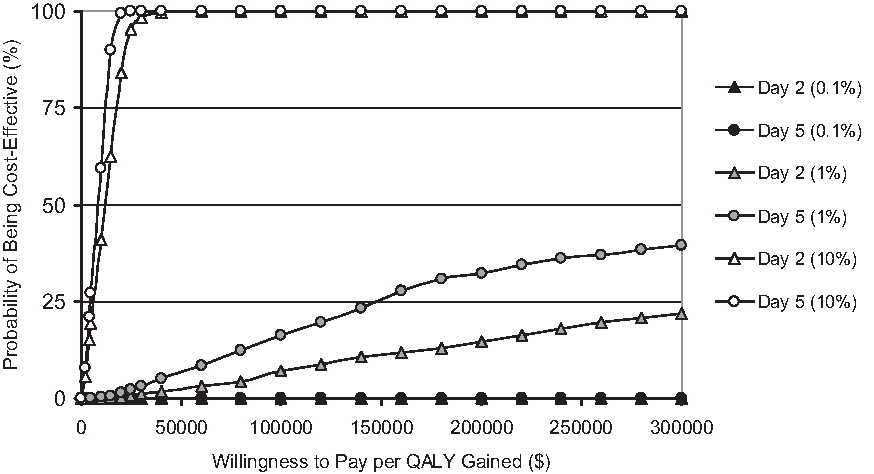
Cost-Effectiveness Acceptability Curves for including preattack vaccination with postattack antibiotic prophylaxis and vaccination strategies based on day of response and probability of attack. For the base-case 1% yearly probability of attack, including preattack vaccination with postattack antibiotic prophylaxis and vaccination has a low probability of being cost-effective that slowly improves for both the Day 2 and Day 5 response strategies as the willingness-to-pay thresholds increase from $0 to $300,000 per QALY gained. At a 0.1% yearly probability of attack, preattack vaccination is not likely to be cost-effective at all willingness-to-pay thresholds for both Day 2 and Day 5 response strategies. However, at 10% yearly probability of attack, including preattack vaccination is likely to be cost-effective for nearly all willingness-to-pay thresholds for both Day 2 and Day 5 response strategies.
One-way Sensitivity Analyses for Day 2 Response Strategies Relative to Base-Case Scenario
Note. Similar proportional changes in the Incremental Cost-Effectiveness Ratio (ICER) estimates for one-way changes in the model parameters were also seen with sensitivity analyses of the Day 5 response strategies. Dominated implies that other strategies are less costly and more effective and thus are eliminated from further consideration in a cost-effectiveness analysis.
Sensitivity analyses of ICU bed availability indicated that increasing the number of available ICU beds in the Chicago metropolitan area from 50% to 90% of the total 2,655 existing ICU beds would increase the number of rescued fulminant victims only from 6,437 (18.5%) to 9,895 (28.2%) in the base-case scenario that includes only postattack antibiotic prophylaxis. However, increasing available ICU beds from 0 to 10,000 would significantly decrease total deaths from inhalational anthrax for either the postattack antibiotics prophylaxis only or postattack antibiotics prophylaxis with vaccination response strategies (Figure 3). For example, increasing the ICU bed availability from 1,000 to 10,000 beds for the Day 2 response strategy with postattack antibiotic prophylaxis would reduce inhalational anthrax deaths from 29,867 to 14,604. This significant reduction in mortality was illustrated for both the Day 2 and Day 5 response strategies.

Effects of Increasing the Number of Intensive Care Unit (ICU) Beds Available to provide critical care therapy for fulminant victims on the overall number of deaths from inhalational anthrax. Estimates are based on the different postattack public health intervention strategies (ie, antibiotic prophylaxis compared with antibiotic prophylaxis and vaccination) and timing of the response strategy (ie, Day 2 compared to Day 5) to a large-scale attack on the Chicago metropolitan area.
We also analyzed the effects of varying levels of ICU bed availability over a wide range (ie, 0 to 500,000) of initially infected cases of inhalational anthrax (Figure 4) on the number of deaths from anthrax for both Day 2 and Day 5 postattack response strategies. This analysis was conducted for 1,000, 5,000, and 10,000 potentially available ICU beds in the Chicago metropolitan area. In general, delaying the response strategy from Day 2 to Day 5 significantly increases mortality regardless of the number of available ICU beds (ie, 1,000, 5,000, or 10,000 beds). Of particular note, increasing the number of available ICU beds to 10,000 for the Day 5 response strategy was not as effective as implementing the Day 2 response strategy with only 1,000 available ICU beds.
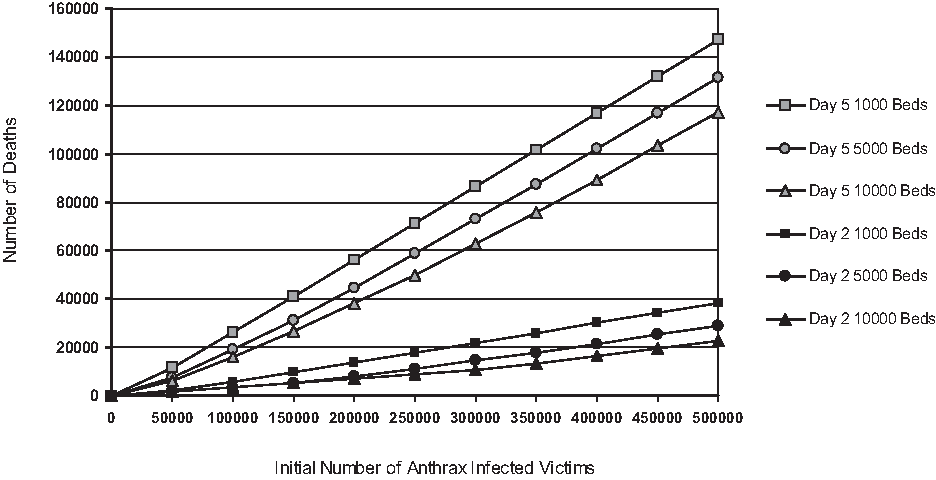
Effects of Varying the Number of Intensive Care Unit (ICU) Bed Availability over a wide range (ie, 0 to 500,000) of initially infected cases of inhalational anthrax on the total number of deaths from inhalational anthrax. These analyses were conducted for both the Day 2 and Day 5 response strategies using postattack antibiotic prophylaxis and vaccination with 1,000, 5,000, or 10,000 potentially available ICU beds in the Chicago metropolitan area.
Discussion
Despite several studies illustrating the importance of rapid response to a large-scale anthrax attack, there is still uncertainty about the optimal cost-effective public health response strategy based on timing of the intervention and availability of critical care resources. Our findings indicate that postattack antibiotic prophylaxis of all exposed victims would be the least costly response strategy for a large-scale anthrax attack on the Chicago metropolitan area, but combining postattack vaccination with antibiotic prophylaxis saves significantly more lives and is cost-effective for both the Day 2 and Day 5 response strategies. In addition, it seems that preattack vaccination of the Chicago metropolitan area is only cost-effective if the probability of an attack on this area is greater than 1% per year or if the public health response is significantly delayed after an attack.
Our findings also indicate that only a limited number of fulminant anthrax victims could be rescued by the existing ICU beds, but that further reductions in the number of deaths could be achieved by expanding critical care capacity in the Chicago metropolitan area or by transporting fulminant victims to healthcare facilities with available ICU beds outside the Chicago metropolitan area. However, increasing the number of available ICU beds has a modest effect in reducing mortality compared with implementing a more rapid response strategy.
Earlier studies evaluating the cost-effectiveness of response strategies to an anthrax attack were limited by (1) assuming relatively small exposed populations (eg, 100,000 exposed persons), (2) the use of simple cost and utility measures, or (3) not considering the option of vaccination of exposed victims.16–19,69,70 One exception was a recent study by Fowler et al that analyzed a theoretical large-scale anthrax attack on 5 million people with derived probabilities of anthrax exposure, prophylaxis characteristics, costs, and clinical outcomes. 20 They found postattack antibiotic prophylaxis combined with vaccination of all exposed victims to be the most effective (0.33 life-year gained per person) and least costly ($355 saved per person) response strategy, but they compared this strategy to postattack vaccination alone as the base-case reference. We do not believe this is a valid or realistic comparison of strategies, because postattack vaccination alone would not adequately protect infected victims until several days after vaccine administration. In fact, postattack vaccination alone of anthrax-exposed victims was not considered a policy option in the Anthrax Modeling Working Group attack scenario commissioned by HHS.
We used the Anthrax Modeling Working Group attack scenario to extrapolate the cost-effectiveness of its 4 policy options. This scenario accounts for several factors affecting numbers of people exposed to anthrax spores, thus facilitating cost-effectiveness estimates based on timing of the public health interventions. We enhanced the validity of our analyses by supplementing the Anthrax Modeling Working Group's policy options with several parameters from a real metropolitan population: (1) size and dynamics; (2) numbers of victims progressing through the disease states of inhalational anthrax at various times; (3) numbers of staff and POD clinics needed to distribute antibiotics and vaccinations; (4) available ICU facilities that could provide critical care to victims with fulminant inhalational anthrax; and (5) variable costs of preexposure and postexposure inhalational anthrax antibiotic prophylaxis, vaccination, and critical care for the 4 response strategies.
Unlike many previous modeling and simulation studies, we did not assume that all people who developed fulminant inhalational anthrax would die. Instead, we assumed that some fulminant victims would receive critical care and survive based on the case fatality rate of recent cases in the US.36–38 However, it is probable that only a limited number of fulminant victims of a large-scale anthrax attack would receive this type of care because individual hospital surge capacity for severely ill patients is limited.55–59 For example, on average there are only 17.7 mechanical ventilators and 28.9 critical care beds per urban hospital in the US. 56 In addition, most hospitals (93.6%) have a surge capacity of fewer than 11 patients who would require mechanical ventilation. 57 Our analyses did not include initial treatment in non-ICU beds, because treatment of prodromal victims would require only oral antibiotics that could be administered in outpatient settings. Although non-ICU beds could be upgraded to provide some level of critical care, most fulminant victims would still need specialized medical care and invasive procedures to manage multiple organ complications; this care can be provided only by trained personnel with particular materials and equipment.
Policy Implications
Our findings indicate that postattack antibiotic prophylaxis and vaccination of all exposed people is the optimal cost-effective public health response strategy for a large-scale anthrax attack on the Chicago metropolitan area. The scientific rationale for this strategy is based on the pathophysiology of inhalational anthrax. In exposed people, B. anthracis spores are phagocytized by alveolar macrophages and transported to mediastinal lymph nodes. 71 Surviving spores germinate into vegetative pathogens that replicate rapidly and release toxins that cause severe mediastinitis, septic shock, and death in a few days.1,7,71,72 Because vaccination takes at least several days to induce immunity,73,74 immediate postexposure antibiotic prophylaxis is needed to prevent toxin production by rapidly multiplying B. anthracis bacteria.
Conversely, because B. anthracis spores can remain dormant in mediastinal lymph nodes for several months before complete clearance, vaccination enhances protection against delayed development of inhalational anthrax. Vaccination also reduces potential problems of noncompliance and adverse drug events related to prolonged antibiotic treatment. For example, in a study involving people from the 6 US sites where B. anthracis exposures occurred in 2001, overall adherence to the recommended 60-day course of antimicrobial prophylaxis was only 44%. 30 In addition, vaccination is especially important if the strain of B. anthracis used in an attack is developed to be resistant to certain antibiotics to enhance its virulence. Furthermore, vaccination provides long-term protection from recurrent exposure to victims who remain in anthrax spore–contaminated areas. 75
Although no human studies have directly compared the overall protective effects of antibiotic prophylaxis versus vaccination, several experiments have found that rhesus monkeys receiving both antibiotic prophylaxis and vaccination after exposure to anthrax spores had significantly greater survival rates compared with either antibiotic prophylaxis or vaccination alone.76–79 These primate studies were individually relatively small, but they support the policy of combining antibiotic prophylaxis with vaccination of all exposed people in response to a large-scale anthrax attack. Because of these potential benefits, the HHS Advisory Committee on Immunization Practices (ACIP) has endorsed CDC's using this combination for postexposure prophylaxis for people at risk for inhalational anthrax. 80
From a societal perspective, the most effective strategy for mitigating the effects of a large-scale anthrax attack would be to vaccinate a significant proportion of the general population before an attack. However, we found that a preattack vaccination program would be cost-effective only if there were a plausible risk for a large-scale attack or a significant delay in the public health intervention. In addition, our assumption that 30% of the Chicago metropolitan area population could be vaccinated before an attack may be too optimistic given the resistance of even high-risk populations to obtaining vaccinations against anthrax. 81 It is unlikely that a significant proportion of the Chicago metropolitan area population would comply with recommendations for preexposure vaccination unless a threat of anthrax exposure was imminent or highly probable. In addition, ACIP does not recommend preexposure vaccination for the general public. 80 However, certain people, such as healthcare workers and government employees, may benefit from preexposure prophylaxis to ensure performance of critical societal functions in an attack.
Currently, the Strategic National Stockpile (SNS) stores medical supplies to send to a major disease outbreak anywhere in the United States within 12 hours. This stockpile contains large transportable “push packages” of antibiotics, antidotes, antitoxins, life-support medications, intravenous supplies, airway maintenance supplies, and surgical items.8,61 In addition, specific “vendor managed inventory” supplies can be shipped within 24 to 36 hours. 61 CDC has also developed the Cities Readiness Initiative program to prepare major metropolitan areas to respond to a large-scale bioterrorist attack by dispensing antibiotics to their entire populations within 48 hours. 8 During a national emergency, state, local, and private stocks of medical materiel will be depleted quickly. State and local first responders and health officials can use the SNS to bolster their response to a national emergency, with a 12-hour push package, vendor managed inventory, or both, depending on the situation. 61
Despite these efforts, the ability to dispense antibiotics or vaccinations to large populations within 48 hours of a bioterrorist attack has not been empirically assessed and remains unknown. In addition, response strategies should include significant augmentation of the number of ICU beds and the personnel to provide critical care to large numbers of severely ill victims. 59 However, our findings clearly indicate that expanding critical care capacity is not as effective as instituting a more rapid public health intervention. For example, even increasing the number of available ICU beds to 10,000 for the Day 5 response strategy was not as effective as implementing the Day 2 response strategy with only 1,000 available ICU beds.
Limitations
Our analyses used multiple simulation models to incorporate the detailed and sophisticated costs and effects of various time-varying response strategies. The principal limitations of our study, therefore, arise from potential misspecifications of key model parameters. To address these limitations, we conducted sensitivity analyses by varying several parameters and found no important changes in our main results except for those seen with increasing the probability of attack. We did not, however, vary the number of victims exposed to anthrax spores who would receive postexposure prophylaxis as this was specified in the original Anthrax Modeling Working Group model.
We also recognize that, during a large-scale anthrax attack, it would not be possible to accurately distinguish exposed victims from unexposed victims, and the number of people requesting postexposure prophylaxis could vary widely. Nevertheless, we deliberately excluded people without postattack exposure to anthrax spores in the Chicago metropolitan area for 3 reasons. First, we used the same number of people treated with postexposure prophylaxis as was specified in the original Anthrax Modeling Working Group model for all our analyses. Second, increasing the number of people receiving postexposure prophylaxis to include a large number of unexposed people would not significantly change our relative cost-effectiveness estimates of the response strategies or the interpretation of our findings. Last, we believe it is unlikely that policymakers would decide to expand the provision of postexposure prophylaxis to a large proportion of people who have exceedingly low risk of anthrax exposure as this would delay the delivery of critical resources to actual anthrax-exposed victims.
In addition, the Anthrax Modeling Working Group attack scenario assumed only 1 kilogram dispersal of anthrax spores. A larger dispersal would probably result in significantly more injured and dead victims.4,5 Moreover, our analyses did not consider overall societal costs for recovering from a large-scale anthrax attack that could potentially dwarf healthcare costs. We also did not vary the percentage of ICU bed availability in our cost-effectiveness sensitivity analyses because we found that few fulminant victims would be saved even if 90% of ICU beds were available. Furthermore, we did not account for additional morbidity and mortality from non–anthrax-related illnesses among patients unable to receive critical care during the postattack period. Including these effects in our analyses would probably widen the cost-effectiveness differences among the response strategies but not significantly change our findings. Finally, we did not assess potential variations in the effectiveness of either antibiotic prophylaxis or vaccination as these were determined by the Anthrax Modeling Working Group estimates.
Conclusions
Postattack antibiotic prophylaxis and vaccination of exposed people is the optimal cost-effective response strategy for a large-scale bioterrorist anthrax attack on the Chicago metropolitan area. The addition of preattack vaccination to the response strategies does not seem to be cost-effective in most reasonable scenarios. Because of the insensitivity to variations in most model parameters, we believe our findings can be generalized to other large US metropolitan areas. In addition, our findings support the US government's current plan to provide antibiotic prophylaxis and vaccination of all exposed people within 48 hours of the recognition of a large-scale anthrax attack. These treatment modalities should be supplied in sufficient quantities from the SNS to accommodate mass casualties. Even with a rapid response, however, only a limited number of fulminant victims could be rescued with available ICU facilities in the Chicago metropolitan area. Thus, future policy considerations should include plans to significantly expand critical care capacity (in hospital and nonhospital settings) and potentially to transport critically ill victims to healthcare facilities beyond the Chicago metropolitan area. Fortunately, a large-scale anthrax attack has yet to be perpetrated in the United States, but the lack of empirical knowledge limits certainty of cost-effectiveness comparisons of response strategies.
Footnotes
Acknowledgments
This study was funded by a grant from the US Department of Veterans Affairs (VA IIR 02-080-1). Dr. Bennett's effort was also supported by funding from the National Cancer Institute (1R01CA 102713-01), the Doris Levkoff Meddin Program on Medication Safety, and the South Carolina Smart State Center for Medication Safety and Efficacy. The funding agencies had no role in the conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript. All authors declare that they have no financial or other conflicts of interest. The authors acknowledge Dr. Robert M. Golub for helping secure VA grant funding for this project and developing the initial Markov models that were further elaborated for this study.