
Abstract
Previous reports have identified the development of healthcare coalitions as the foundation for disaster response across the United States. This survey of acute care hospitals characterizes the current status of participation by US hospitals in healthcare coalitions for emergency preparedness planning and response. The survey results show the nearly universal nature of a coalition approach to disaster response. The results suggest a need for wide stakeholder involvement but also for flexibility in structure and organization. Based on the survey results, the authors make recommendations to guide the further development of healthcare coalitions and to improve local and national response to disasters.
Healthcare coalitions have become the foundation for disaster response across the country. This article surveys acute care hospitals about the current status of their participation in healthcare coalitions for emergency preparedness planning and response. The survey results show that the coalition approach to disaster response is nearly universal.
A subsequent report on the challenge of healthcare preparedness for catastrophic health events concluded that every US hospital should participate in a healthcare coalition that prepares for and responds collaboratively to common medical disasters and catastrophic health events. 2 Links should be established between neighboring healthcare coalitions to enable regional exchange of healthcare information and assets during a catastrophic health event. 2 The HPP, administered by the Office of the Assistant Secretary for Preparedness and Response (ASPR), has placed increasing emphasis on building required partnerships and coalitions during the FY2010 and FY2011 budget periods. The FY2011 ASPR HPP guidance says that this work should build on developing broader-reaching healthcare system partnerships/coalitions that enhance community resilience. 3 This concept is presented in “Comprehensive Coalition Strategies for Optimization of Healthcare,” which is promoted through the FY2009 Pandemic Influenza Healthcare Preparedness Improvements for States Funding Opportunity Announcement, 4 and the new handbook Medical Surge Capacity and Capability: The Healthcare Coalition in Emergency Response and Recovery. 5 The ASPR HPP guidance also points to the “Provisional Criteria for the Assessment of Progress toward Healthcare Preparedness” report, which outlines key functional characteristics and metrics for assessment of progress in the development of healthcare coalitions. 6 FY2012 ASPR guidance further emphasizes development of healthcare coalitions and suggests structural and functional characteristics. 7
A first step in promoting the development of healthcare coalitions was a competitive grant process, the Health Facilities and Emergency Care Partnership Grant Program, which funded 16 successful applications for coalition development programs. Evaluation of this program included descriptions of several new healthcare coalitions and further progress in previously established programs. 8
Although these reports and the ASPR HPP guidance recognize and encourage the development of healthcare coalitions, their methodology does not allow for any conclusions about the “epidemiology” of healthcare coalitions. These coalitions were becoming more common and important in healthcare emergency preparedness. But how many such coalitions exist, how much US hospitals participate in healthcare coalitions, and how effectively these coalitions are integrated with jurisdictional emergency preparedness systems throughout the country could not be determined from these anecdotal reports and case studies. State HPP coordinators who were interviewed may have over- or underreported hospitals' participation in coalitions. Reporting of impressive results from well-established coalitions that were successful in a competitive grant process may not be representative of hospitals throughout the country. An important step toward the goal of development of healthcare coalitions in all communities and jurisdictions is an analysis of where the country is now in hospital participation in healthcare coalitions.
This survey is an effort to characterize the status of participation by US hospitals in healthcare coalitions for emergency preparedness planning and response.
Methods
We surveyed 4,632 acute care hospitals in the US (nonfederal, non–Veterans Affairs hospitals) regarding their participation in collaborative healthcare coalitions for coordination of emergency preparedness and response. We developed the survey questions, which were based on previous research into healthcare coalitions and healthcare system preparedness for mass casualty events. 1 Before the survey was disseminated, it was tested by 3 experts in emergency preparedness healthcare coalitions to ensure that it was easy to understand, that the questions were meaningful, and that all important topics were covered. A list of survey questions can be found at www.liebertonline.com/bsp.
The survey was e-mailed directly to the president, chief executive officer, or designated executive at acute care hospitals, who were asked to forward the survey to appropriate hospital personnel in charge of disaster preparedness. E-mail addresses were obtained from a database provided for 1-time use by the American Hospital Association (AHA). The first e-mail invitation to participate in the survey was sent in early August 2011, and the survey remained open for about 1 month.
A support e-mail account was provided to answer questions about the survey. The survey was also advertised by leaders of the National Hospital Preparedness Program, who e-mailed grantees and stakeholders to encourage hospital participation in the survey. We also announced the survey on a conference call with AHA members.
The survey was designed and data were collected using SurveyMonkey. The data were analyzed using STATA version 11.2. The survey data were tested to measure whether the respondents were representative of the hospitals in the AHA database based on 4 characteristics: urbanicity, bed size, geographic distribution, and teaching hospital status.
The data analysis was carried out in 3 parts: summary statistics, chi-squared analyses, and a conditional scoring test. The chi-squared tests primarily examined responses to the questions of whether hospitals reported that coalitions participated in joint response to mass casualty events and whether coalition members contribute money or in-kind resources to the coalition. The conditional scoring test examined 14 hospital coalition characteristics based on when the survey respondents indicated their coalition began.
Results
A Representative Sample
The survey generated 477 responses from a survey population of 4,632 acute care facilities, a 10.3% response rate. The demographics of the responding hospitals are described in Table 1.
Characteristics of Survey Respondents and AHA Database with 95% Confidence Intervals
To measure geographic distribution, we grouped the HHS regions into 5 groups and measured the survey respondents against the AHA database.
9
The regions were divided as follows:
• Northeast—Regions 1-3 • Southeast—Region 4 • South—Region 6 • Midwest—Regions 5, 7, 8 • Pacific—Regions 9, 10
Table 1 displays each group with 95% confidence intervals. Hospitals in the Midwest group are slightly overrepresented, while hospitals in the Southeast are slightly underrepresented. These mild deviations in geographic distribution are to be expected in a survey that was conducted using a convenience sample. Survey respondents included hospitals from 49 of 50 states.
Compared with the AHA dataset, the survey respondents were statistically representative with regard to urban or rural location, bed size, and teaching hospital status. Percentage of urban hospitals and teaching hospitals and median bed size are shown in Table 1 for both the AHA dataset and the survey respondents. Table 1 shows that the survey respondents for all 3 categories are within the 95% confidence intervals of the AHA data. Urban hospitals may be slightly underrepresented, but not outside the 95% confidence intervals.
According to the most recent data from ASPR, 5,341 hospitals in the 50 states and 4 metropolitan areas participate in the HPP. 10 The California Hospital Association estimates that these hospitals represent over 85% of the more than 6,300 hospitals in the US. 11 About 75% of survey respondents indicated they participate in the HPP. Although this measure was not tested for statistical significance, it is clear that hospitals participating in HPP were not overrepresented. Because HPP guidance supports the development of coalitions, that HPP hospitals are not overrepresented indicates that the data are not skewed toward coalition participation.
Coalition Participation
Nearly all (94.51%) the hospitals that responded to the survey said that they participated in a discrete entity, partnership, organization, coalition, planning group, consortium, or other agreement with other hospitals and community partners for emergency preparedness and response. Nearly 90% of respondents said that more than 75% of their local hospitals participated in their healthcare coalition. Although many coalitions were founded before 2002, more than 60% began after 2002, when federal funds became available to most hospitals to improve their ability to respond to public health emergencies and bioterrorism.
We recognized that several hospitals representing the same coalition would probably respond to the survey. The survey provided the option of entering the name of the healthcare coalition that the hospital participates in. In examining these responses, we identified 314 unique coalitions out of 416 that entered a coalition name, so there were some coalitions represented more than once. Although 7 coalitions were represented 4 or more times, the most hospitals representing the same coalition was 7. This occurred only once. This indicates that a broad range of coalitions was represented in the survey.
Structure and Function of Coalitions
Additional survey results, presented in Table 2, show the diverse structure, leadership, and funding of healthcare coalitions for emergency preparedness and response. Notably, in 88% of respondents, more than 75% of hospitals in a community participated in coalitions and most coalitions began after HPP funding was initiated in 2002. Although most coalitions included a formal linkage, the leading organization was split between a hospital or group of hospitals and a public health or emergency management agency. More than 75% of hospitals said they participate in the HPP, and among those, grant money was distributed in a variety of ways.
Summary Statistics
Stakeholder Involvement in Coalitions
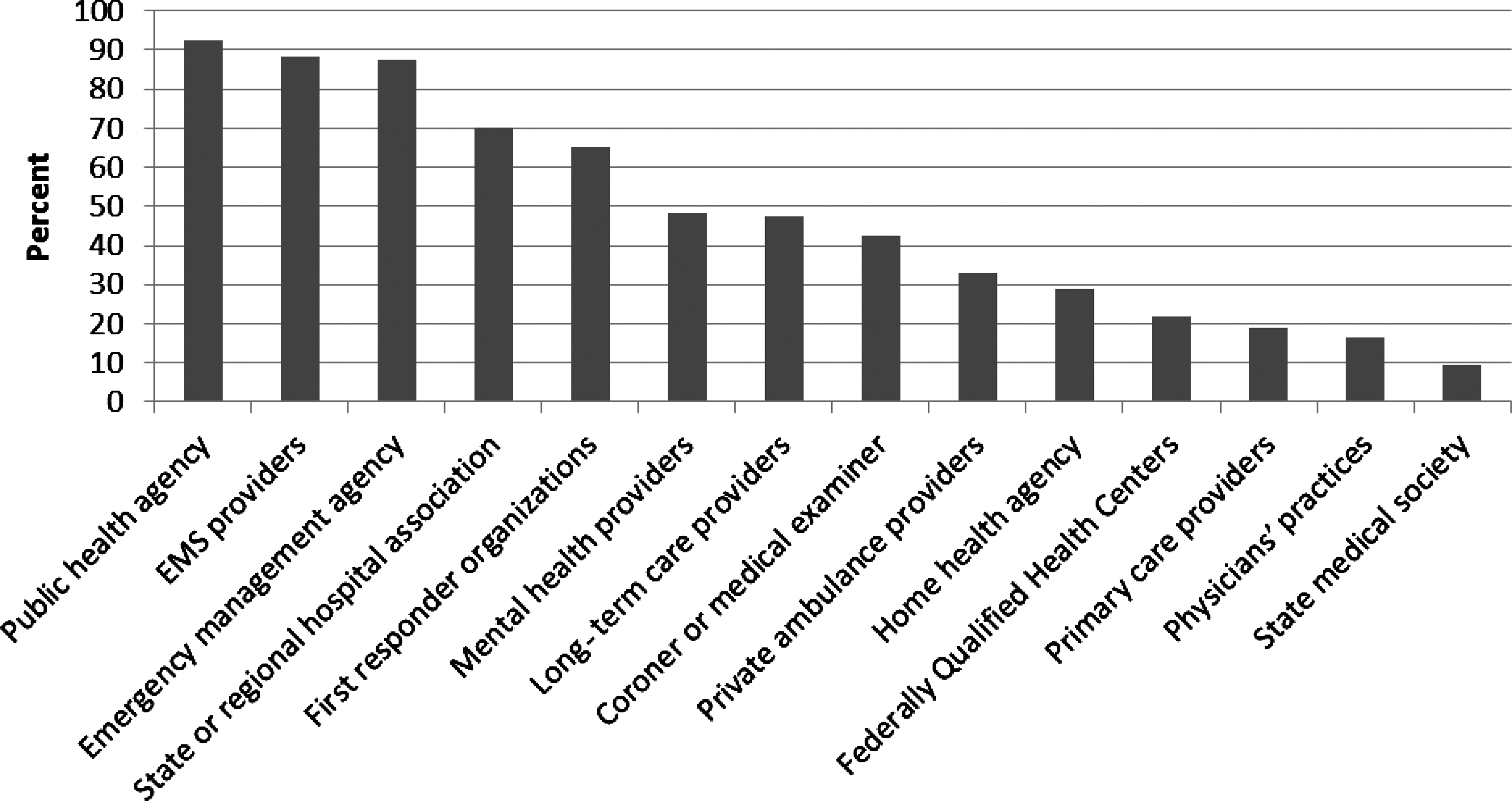
Of the 477 survey respondents, 383 (80%) said they participated in a healthcare coalition with a diverse group of stakeholders, and 12% said that the coalitions in which they participated included only hospitals. Of those 383 that described a diverse group of stakeholders, public health agencies, EMS providers, and emergency management agencies participated at a high rate: about 90% for each (Table 3, Figure 1). Most hospitals reported state or regional hospital associations and first responder organizations also participated in their coalitions. About half the hospitals in this group reported that long-term health providers and mental health providers participated in their coalition. The overall rate of stakeholder participation is high and is in accordance with federal grant guidance and accreditation requirements (such as the Joint Commission's Emergency Management Standards).
Stakeholder Involvement in Coalitions
Percent of Hospitals that Indicated Various Stakeholder Participation in Coalitions
Coalition Activities
Survey respondents were asked to describe activities performed by their coalitions (Table 4, Figure 2). Response rates were highest for participation in planning activities, conducting joint training and drills, and sharing bed availability and surge capability. Overall, respondents said that most coalitions engaged in most of the activities listed in the survey. The one exception was member contribution of money or in-kind resources to support the coalition, to which only 23.7% of hospitals responded positively. These activities are divided into those that are primarily conducted before a disaster (preparedness) and activities primarily conducted during a disaster (response).

Coalition Activities
Percent of Hospitals that Participate in Coalitions that Perform These Activities
Note: The researchers divided these activities into “preparedness” and “response” categories after completion of the survey during the data analysis. The complete survey tool is available online at: www.liebertonline.com/bsp
Preparedness Only Versus Preparedness and Response
There were differences between coalitions that participated in joint response to mass casualty events and those that did not participate in response activities (ie, were largely preparedness-only entities). None of the responding hospitals said that their coalitions were response-only entities. Table 5 shows a comparison of the characteristics reported between coalitions that did or did not jointly respond to mass casualty events and whether there were statistically significant differences. Of note, coalitions were more likely to be involved in a joint response if the local emergency management agency and EMS providers were part of the coalition. They were also more likely to be involved in a disaster response if they contributed resources to the coalition and participated in the local emergency operations center (EOC).
Chi-square Tests: Characteristics of Coalitions Described as Involved in Preparedness and Response Compared to Those Involved in Preparedness Only
However, whether the leading organization of the coalition was a hospital or public health/emergency management agency (EMA) and whether hospitals were required to participate in coalitions were not associated with whether the coalition had a role in response. Likewise, participation in the HPP and the method of distributing HPP funds was not associated with whether joint response was a characteristic of a coalition.
Member Contributions
Similarly, there were differences between coalitions in which members contributed money or in-kind resources to support the coalition and those that did not. Table 6 details these differences as determined by a chi-square analysis. Public health agency participation in the coalition correlated with hospital contribution of funds, as did participation in the local EOC. However, state or regional hospital association, EMS, and EMA involvement was not associated with contribution of funds or resources. The lead organization of the coalition, HPP participation, and required hospital participation in coalitions were not significantly associated with member support of coalitions. But members were more likely to contribute funds or resources to the coalition if HPP funds were sent to the coalition directly for distribution to hospitals. Furthermore, there was an association between joint purchasing or other cost incurring activities such as management of alternative care facilities and members contributing to the coalition. This was also true for sharing data on patient load and available assets.
Chi-square Tests: Characteristics of Coalitions Described as Members Contributing Money or Resources to Support the Coalition Compared to Those in Which Members Do Not
Age of Coalition
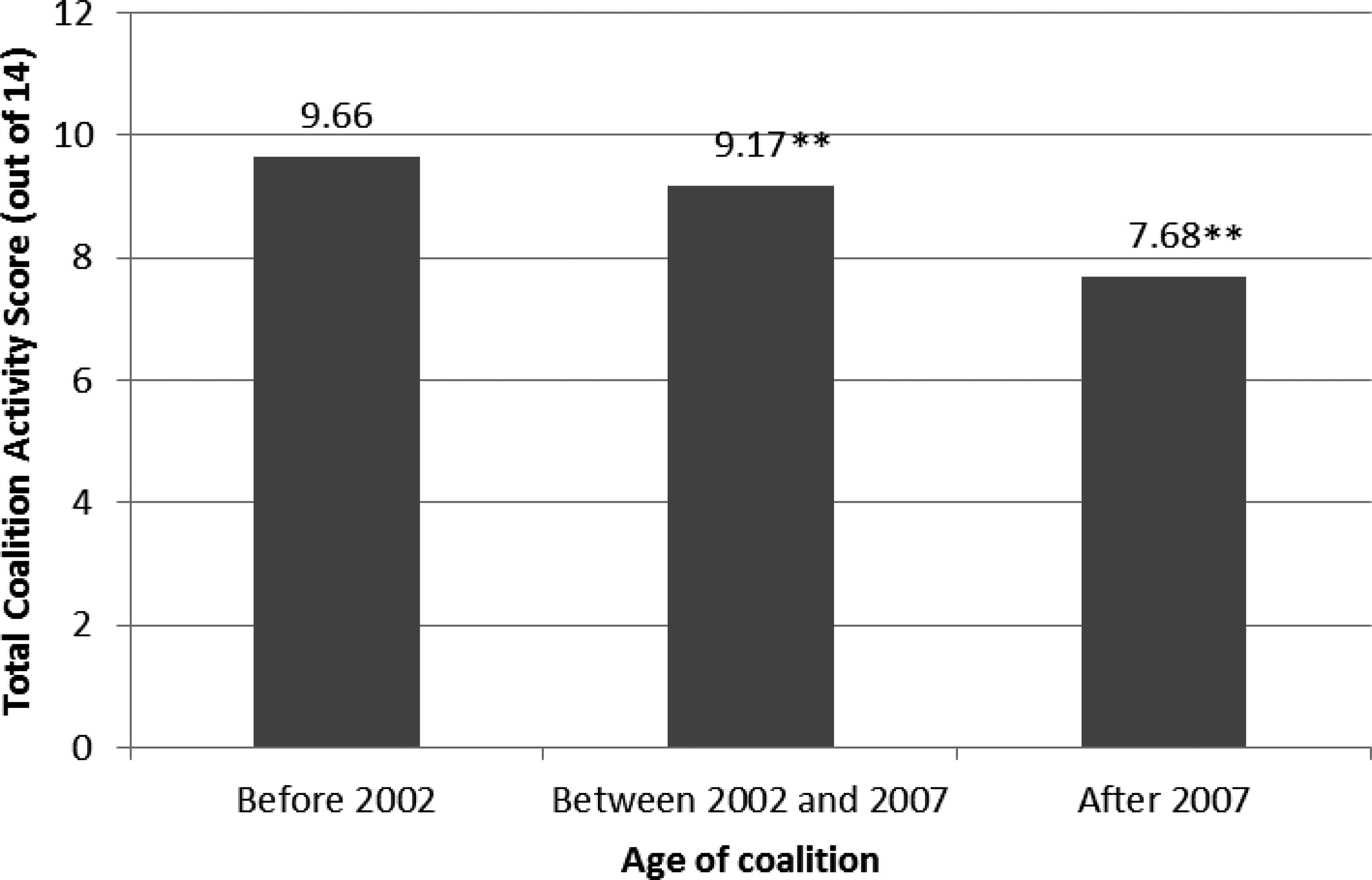
Coalitions also had different qualities based on when they began; we hypothesized that coalitions that have existed for longer are more likely to be more advanced, include more stakeholders, and perform more activities than newer coalitions. As part of the survey, we asked respondents what year their coalition started. In the survey, 3 time periods were given for the question, “When was this entity started?”: before 2002, between 2002 and 2007, and after 2007.
Figure 3 and Table 7 examine 14 characteristics of coalitions taken from the survey. Each of the 3 periods was scored based on positive responses to each of the 14 questions. A positive response was assigned a value of 1, a negative response 0, and the mean numbers of positive responses to the 14 questions per survey respondent in each group were then compared to determine significance. These 14 characteristics were used in the scoring analysis:
1. Joint planning activities 2. Participation in HPP 3. Public health participation 4. Emergency medical services participation 5. Joint response to mass casualty events 6. Alternative care facilities coordination 7. Mental health provider participation 8. Contribution of money or in-kind resources to support coalition 9. Private ambulance provider participation 10. Distribution of HPP funds through coalition 11. Formal linkage through MOU, MOA, or contract 12. Joint purchasing of equipment, supplies, stockpiles 13. Participation in local emergency operations center (EOC) 14. Sharing of bed availability
Characteristic Score by Coalition Age
Scores of Coalition Characteristic by Coalition Age
Indicates a p-value of less than 10%.
Indicates a p-value of less than 5%.
As expected, coalitions that began before 2002 had, on average, more of the 14 characteristics than those coalitions that began later. When the before-2002 group was compared with the other 2 groups, there was statistically significant difference. Figure 3 shows the total coalition activity score in the 3 age ranges. Table 7 shows trends for all 14 characteristics for coalitions that began in 2007 and earlier and after 2007, with statistically significant trends indicated by asterisks.
Limitations
This survey is based on self-reporting, and there is no means to verify the reports. The low response rate of about 10% is also a limitation in interpreting these data broadly across all hospitals in the country. The results of this survey are subject to some bias. Although the sample seems representative by the measures we examined, it may not be a true representation of the spectrum of US hospitals by other measures. High-performing hospitals (ie, those that participate in coalitions) may be overrepresented in the survey respondents. The survey was administered to hospitals, and not directly to healthcare coalitions, which may also introduce bias in addition to multiple hospitals representing a single coalition. Furthermore, the survey could be subject to recall bias of the respondents.
Discussion
This survey of a representative sample of US hospitals revealed that most hospitals identify themselves as participants in healthcare coalitions for emergency preparedness and response. Organized healthcare coalitions have existed for many years and were started by groups of private hospitals, 12 state or local public health agencies, or hospital associations or were built on preexisting emergency response infrastructures, such as Metropolitan Medical Response System (MMRS), or trauma systems. 6 This survey shows that the adoption of this approach to the organization and performance of emergency preparedness and response by US hospitals is nearly universal in this sample and is a fairly recent development. Other surveys have shown similar results by analyzing the extent to which hospitals achieve certain emergency preparedness and response functions. 13 In a previous report on the first 5 years of the HPP program, background interviews of officials in 63 states and municipalities included frequent anecdotal reports of the significance of the development of healthcare coalitions. 6 Several new and established healthcare coalitions received competitive partnership grants, and their progress and development have been described. 8
Because of the methodology of these previous reports, the question left unanswered was whether the importance and prevalence of healthcare coalitions as organizing entities for hospital preparedness and response was over- or underestimated in anecdotal reports. In the current study, 94% of surveyed hospitals identified themselves as healthcare coalition participants, suggesting that these entities are the dominant structures for hospital emergency preparedness and response.
The timing of the start of the healthcare coalitions suggests that HPP funding and guidance significantly affected their growth and development: 60% of coalitions developed after 2002 when HPP funding and guidance became available, and some have developed recently, since 2007, when guidance from the HPP began to emphasize the importance of this type of collaborative organization. 3 The lower coalition activity score for coalitions formed after 2007 suggests that seeking and gaining diverse stakeholder buy-in and participation takes a significant amount of time, as does engaging in response activities and preparedness activities.
The current study provides further details about healthcare coalitions. Respondents noted that more than 75% of hospitals in the surrounding local or regional community participated in the coalitions. Participation also included other stakeholders, such as public health agencies, emergency management agencies, and coalition members that were linked by a formal agreement. This suggests that this is a true coalition and not just a hospital response to grant guidance or accreditation agency requirements. Roughly equal percentages of coalitions were described as being organized by a group of hospitals or a public health agency, which suggests that either structure can be successful from the perspective of participating hospitals. Similarly, a variety of HPP funding distribution methods were described, including direct funding of hospitals, of coalitions, or both, which did not seem to affect the range of functional capabilities of coalitions.
The identification of the breadth of stakeholder participation was also informative. As noted, public health and emergency management agencies, such as EMS and other first responder organizations, and state or regional hospital associations were most frequently mentioned; however, at least 25% of the respondents mentioned home health agencies, long-term care providers, mental health providers, and medical examiners' offices as partners in healthcare coalitions. This inclusion of essential stakeholders in community-wide planning and response also supports the conclusion that these coalitions are more than hospital-based entities.
The coalition functions most frequently reported demonstrate comprehensive efforts toward the development of surge capacity and capability. Although planning and training activities were most commonly reported, 75% of hospitals noted that the coalitions in which they participate were involved in joint response to mass casualty events through formal links to other hospitals and the jurisdictional response agencies, sharing of bed availability and surge capability during response, and participation with the local EOC.
About half the hospitals reported that coalitions coordinated the use of alternative care facilities or volunteers in the healthcare setting during an emergency response. The survey questionnaire was not designed to explore the use of volunteers, either in hospitals or alternative care facilities, in more detail. Further investigation is necessary to understand the way programs such as the Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP), the Medical Reserve Corps (MRC), and the National Disaster Medical System (NDMS) are coordinated with hospitals and healthcare coalitions at the local, state, and regional levels. 14
There were some differences in the characteristics of coalitions that participated in an emergency response compared to those that participated only in preparedness. EMS and EMA were more frequently included in those coalitions that become involved in a response, and these coalitions played a role in the local EOC. Although only 23% of hospitals noted that members contributed money or in-kind resources, coalitions in which those hospitals participated were more likely to be involved in a disaster response, suggesting that member investment may be important for supporting response activity. Resource investment may also play a role in healthcare coalition sustainability and the commitment of members to the mission of the organization, but these possibilities were not investigated in the current report.
Recommendations
The findings of this survey suggest several implications for program guidance, performance measures, and funding strategies to promote further development of healthcare coalitions.
• The survey showed that nearly all hospitals are involved in preparedness activities but fewer are involved in response activities. Federal and state guidance to hospitals and public health agencies should emphasize building response functions of healthcare coalitions. • The survey results indicated a correlation between EMS and EMA participation in a coalition and coalition participation in a local EOC with a coalition coordinating joint response to disasters. Guidance should promote the inclusion of EMS and EMA as stakeholders in coalitions, if they are not already included, and suggest participation in the local EOC. • The survey showed lower participation of certain stakeholders in the coalition. Inclusion of ambulatory facilities, long-term care providers, coroners, medical examiners, federally qualified health centers (FQHCs), primary care practices, physicians' practices, home health agencies, and mental health providers in healthcare coalitions should be encouraged. • The survey indicated that the variability in organization structures and mechanisms for distribution of hospital preparedness funds did not seem to affect hospital participation in coalitions. Therefore, flexibility in these areas should be maintained to allow for differences in historical strengths and weaknesses of potential lead agencies or entities. • The survey showed that in only a few coalitions did members provide financial support or in-kind resources to the coalition. Sustainability planning should be a part of healthcare coalition work and strategy, as it will require funds to maintain current progress. Further studies are needed to determine the impact of financial or in-kind resource contributions by member institutions on the long-term sustainability and effectiveness of healthcare coalitions.
Footnotes
Acknowledgments
The authors thank Roslyne Schulman and Peter Kralovec of the American Hospital Association for their help in disseminating the survey and providing the AHA database of hospitals. The authors thank Robert Scott Dugas and Clare Helminiak of the US Department of Health and Human Services for their support and announcement of this survey. The authors also thank Cynthia Dold of Public Health-Seattle & King County, John Hick of Hennepin County Medical Center and the Minnesota Department of Health, and Dan Hanfling of Inova Health System for their help in review of this survey.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.