
Abstract
With the growing recognition of the critical role that risk communication plays in a public health emergency, a number of articles have provided prescriptive best practices to enhance such communication. However, little empirical research has examined perceptions of the quality of communication, the impact of uncertainty on changing communication, use of information sources, and trust in specific government spokespersons. Similarly, although there is significant conceptual focus on trust and communication as important in vaccination intent and acceptance, little research has explored these relationships empirically. We conducted an online survey in late January 2010 with a nationally representative sample (N=2,079) that included Hispanic and African American oversamples. The completion rate was 56%. We found that public health officials were the most trusted spokespersons, with President Obama being the most highly trusted elected official. Demographic variables, including race, accounted for 21% of the variance in trust of the president. Perceptions of the quality of communication were high, including significant understanding of uncertainty and appreciation for officials' openness about evolving information. Other factors that contributed to vaccination acceptance were quality of communication, closely following the news, and confidence in the vaccine because of a role model effect of the Obama daughters' immunizations; these factors significantly increased trust in government actions. Because the challenges of communication often vary over the course of a pandemic, there is a consistent need to pay close attention to both communication content and delivery and prepare public health officials at all levels to be effective communicators.
Clear and consistent communication by public health and government spokespersons about vaccination during the 2009 H1N1 pandemic was important to the public's trust in government actions and increased the likelihood that people sought the vaccine. Public health officials were the most trusted spokespersons, with President Obama indicated as the most highly trusted elected official. Other factors that contributed to vaccination acceptance were the quality of the communication, closely following the news, and confidence in the vaccine because of a role model effect when President Obama had his daughters immunized.
The French writer Alexis de Tocqueville in the 1800s was one of the first to describe what an important role communication played in informing and mobilizing public action in America. 2 As mass media has become more pervasive in America, research has focused on understanding and using the power of communication to achieve social change. 3 This article follows in that tradition by exploring the relationship between perceptions about communication during the pandemic, trust in government actions and spokespersons, and vaccination acceptance and intention.
Emergency situations necessitate different communication activities than are typically employed in public health responses.4-6 High uncertainty, nearly impossible time constraints, and public anxiety are challenges to effective communication during many crises. Literature on crisis and emergency risk communication prescribes a defined set of communication activities scientifically derived from risk communication principles that, when executed, can guide the public, the news media, and others in responding appropriately and complying with public health measures.5-8 Crisis and emergency risk communication that can ameliorate negative outcomes from a pandemic include disseminating accurate information in a timely and transparent way, describing what is known and unknown, and providing concrete recommendations for behavior. Although there was significant uncertainty and public anxiety in the early phases of the pandemic, these lessened as public health knowledge expanded and public perception of the severity of the influenza declined.
Trust and communication are inextricably linked in a pandemic as well as in other public health emergencies.6,9-13 Trust can affect perceptions of communication, and, conversely, communication can either foster or damage trust. The content of an official emergency message will immediately be judged by the public for its timeliness and honesty and the trustworthiness of the messenger.10,14 This trust in the information source may influence the public's judgments of the quality of the communication, as well as their compliance with the recommended actions. For instance, in a survey in the United Kingdom, Rubin et al found that trust in government authorities, the perception that communication was clear, and the lessening of uncertainty early in the pandemic were associated with adopting behaviors to prevent infection with H1N1 influenza. 15
There is growing literature that examines the importance of communication and trust specifically related to vaccination behavior during a pandemic.12,16-18 Freimuth et al 13 found a small association between trust and vaccination, but 2 studies found that communication about vaccines from official government sources was a consistent predictor of higher vaccination rates during the pandemic, resulting in a call for sufficient, clear, and timely communication to “maintain public confidence and trust to increase compliance.”12(pD10) Additional research suggests that people who relied on unofficial sources were less likely to be vaccinated and that, during the H1N1 pandemic in the United States, mistrust and conspiracy theories promulgated by local clergy, the media, and social media sources were potential factors in H1N1 immunization disparities in African Americans.16,19
In general, Americans' trust in government has declined over the past 50 years, reflecting the decrease in public trust in government and political institutions in all advanced industrialized democracies since the mid-1960s. 20 In the US, trust in government varies by race and ethnicity. A 2010 Pew Research Center study reported that 37% of African Americans trust the government always or most of the time compared with just 20% of whites and 26% of Hispanics. 21 The increase in trust in government, particularly by African Americans, is a sharp turnaround from previous years—particularly following Hurricane Katrina in 2005, when just 12% of African Americans said they trusted the government. The election of President Obama may well be a major factor in that improvement. While racial differences and trends must be acknowledged, it is unclear what impact, if any, they will have on adherence to public health recommendations during a pandemic.
Although trust is recognized to play an important role in risk communication and the public's response in an emergency, the literature is still defining exactly what trust means and how it can be operationalized. While there is no generally accepted theory, the Trust Determination Model 22 and others identify elements such as perceived competence, objectivity, fairness, consistency, faith, commitment, and caring as core components of trust.10,23,24 Vaughn and Tinker add accountability and transparency to these components. 6 There is growing consensus that, as Larson and Heymann remind us, “It is not only the ‘what’ that matters [with regard to what is communicated], but ‘who’ is conveying the information or concerns and ‘how’ it is communicated. Concern and care also implies listening.”25(p272) Not only the words but also the actions of government officials matter in modeling desired behavior. 26 Little research has explored the interaction of these elements and their impact on trust.13,14,18 Using components from Meredith et al, 10 as well as elements of the Trust Determination Model, Quinn et al 27 developed a quantitative trust scale that includes questions to assess respondents' level of trust regarding the government's openness, honesty, commitment, caring and concern, and competence in addressing H1N1; the extent to which respondents believe the government's actions in response to H1N1 are in their personal best interest; and how much respondents believe the government will protect them from H1N1. These items were used in the current study to measure levels of trust in the government handling of the H1N1 pandemic.
With a clear need to facilitate trust and credibility in communication, we also looked to include what Meredith et al 10 call credible models for communication. We extended this approach to the concept of role models, which is grounded in social learning theory and social cognitive theory26,28 and holds that observational learning can influence behavior and that the use of credible, trusted role models is an effective tool. Coupled with the clear importance of credible, official spokespersons in communication, 16 role models are suggested as an effective means to increase vaccination intention and behavior. 29
We explored the relationship among communication, trust, and vaccination intention and uptake during the 2009 H1N1 pandemic using a random national survey administered in late January 2010, at the peak of the H1N1 vaccination effort. President Obama had just encouraged all Americans to observe National Influenza Vaccination Week (January 10-16) by getting the 2009 H1N1 flu vaccine and asking families, friends, and coworkers to do the same. We posed these research questions: (1) What information sources did Americans use? (2) What was the level of public trust in government in handling the pandemic and public trust in spokespersons in the midst of the 2009 pandemic? (3) How are perceptions of communication quality associated with trust during the pandemic? (4) How and to what extent do the quality of communication, role modeling, and trust in government affect vaccination intent and acceptance later in the pandemic?
Methods
Sample
The participants were randomly drawn from the Knowledge Networks (KN) online research panel, which is representative of the US population. At the time of the survey, KN used a combination of random-digit dial and address-based probability sampling methods to recruit panel members, with about 96% coverage of the US population. KN provides panelists without access to the internet (including low-income panelists) with hardware and access to ensure a representative sample. Panelists participate in online research studies in return for internet access and hardware or for points redeemable for cash.
The sample randomly selected by KN for this study included oversamples of African Americans and Hispanics (from KN's KnowledgePanel Latino, which represents all strata of the US Hispanic population). Of the 3,689 panel members 18 years old and over who were selected to participate, 2,079 completed the survey, for a completion rate of 56%. For this analysis, the sample was limited to the 2,042 participants comprising 3 race/ethnicity groups: white non-Hispanic, black non-Hispanic, and Hispanic. The survey was administered from January 22, 2010, to February 1, 2010, in both English and Spanish. KN sends email and telephone reminders to panelists to maximize participation. KN provides a weighting variable that includes both a panel base weight and post-stratification weights to demographically adjust the sample to the US population using the most recent current population survey. All analyses reported here are weighted. More information on the KN research panel is available from their website (http://www.knowledgenetworks.com).
Measures
Demographics: Seven variables were used in the analysis: gender, age, race, income, education, political ideology, and party affiliation (see Table 1). Age was categorized into 3 levels, and income was categorized into 4 levels, with roughly equal proportions in each level. We collapsed education into 4 categories: less than high school, high school graduate, some college, and bachelor's degree or higher. Political ideology was measured on a 7-point Likert scale (1=extremely liberal to 7=extremely conservative).
Frequencies of Demographic Variables and Vaccination Intention
Missing data excluded
Trust in government actions during the H1N1 pandemic: Seven items addressed level of trust in the government's handling of the H1N1 pandemic (see Table 2). 27 Using 4-point Likert scales (with higher numbers indicating more trust), the items measured participants' attitudes toward openness, honesty, commitment, caring and concern, and competence of the government in addressing H1N1; the extent to which participants believed the government's actions in response to swine flu were in their personal interest; and how much participants believed the government would protect them from the swine flu. For the analysis, we created a composite scale by averaging across all 7 items (Cronbach's alpha=.927).
Descriptive Statistics of Trust in Government Action and Trust in Information Sources
Trust in government spokespersons: Seven items measured trust in the H1N1 information delivered by spokespersons (see Table 2). These included local and state elected officials, local or state health officials, officials from the Centers for Disease Control and Prevention (CDC), the Secretary of Health and Human Services (Kathleen Sebelius), the Secretary of Homeland Security (Janet Napolitano), and President Obama. These items were measured on 4-point Likert scales (1=do not trust at all to 4=trust totally).
Attention to H1N1 news: Participants were asked how closely they were following the news accounts about H1N1, and the item was measured on a 5-point Likert scale ranging from 1=not at all closely to 5=very closely.
Quality of communication: The following items measured the quality of H1N1 communication on a 4-point Likert scale from 1=strongly disagree to 4=strongly agree:
1. Overall, the information I have heard about swine flu has been clear. 2. I understand that information about swine flu will change as scientists learn more about the virus. 3. Overall, the information I have heard about swine flu has been consistent. 4. I appreciate when federal officials are open about what they are still learning about swine flu.
Role model: We examined the impact of a highly visible role model with a role model composite score created by averaging 2 items using a 4-point Likert scale (1=strongly disagree to 4=strongly agree):
1. Knowing that President Obama had his daughters vaccinated gives me more confidence in the safety of the vaccine. 2. Knowing the president had his daughters vaccinated would increase my willingness to have my children vaccinated.
Information sources: Using a 4-point Likert scale (1=none at all to 4=a lot), we measured the quantity of H1N1 information from: (1) local TV news, (2) website of the local TV or newspaper, (3) national network TV news, (4) cable news, (5) newspaper, (6) the internet, (7) National Public Radio, (8) local radio stations, (9) healthcare provider, (10) family and friends, and (11) other.
Vaccine uptake and intention: The participants were asked if they had taken the H1N1 vaccine (yes/no response) and, if not, whether they were intending to receive the H1N1 vaccine in the next month (yes/no/don't know response).
Analyses
A sequential multiple regression was performed on each trust-in-government-action and trust-in-information-source predicted by each communication variable, one at a time, after adjusting for demographic variables using a complex survey design in STATA 11.2. Demographic variables were entered first and communication variables were entered in the second step. R2 for demographic variables and change in R2 are reported for each communication variable. A sequential multinomial logistic regression was performed on vaccination intention predicted by each communication variable one at a time after adjusting for demographic variables using a complex survey design. The participants who had already received the H1N1 vaccine (N=396, 19.5%) were left out of the analysis to avoid any bias that would have been introduced by their vaccine decision. Demographic variables were entered first, followed by communication variables. Pseudo R2 and change in pseudo R2 are reported for each model. Alpha was set at .05. Descriptive statistics and frequencies were performed to examine distribution of variables.
Results
Descriptive statistics of the survey outcomes are shown in Tables 1, 2, and 3. Table 1 reports the survey participants' demographic information, whether they received the vaccine, and their intention to receive the vaccine. Table 2 reports the mean responses of the survey participants to the questions regarding trust in government actions and trust of different information sources, and Table 3 shows the mean responses from the participants to the question about which sources were used to receive information about swine flu. Notably, as shown in Table 3, although trust in spokespersons generally did not differ significantly by race, minorities did evidence higher trust in President Obama.
Descriptive Statistics on Quality of Communication, Role Models, and Information Source Variables
The extent to which demographic variables explained trust in government actions and trust in spokespersons varied from 2% to 21% (Table 4). The largest effect size was with President Obama, with demographic variables accounting for 21% of variability in trust in information from the president. Demographic variables accounted for far less (3-5%) of the variability in trust in government spokespersons such as officials from local government, state government, local health agencies, and CDC.
Table of Regression Coefficients in Predicting Trust in Government Actions and Trust in Spokespersons
Demographic variables include race/ethnicity, gender, age, education, income, political party, and political ideology.
Note: Boldface indicates an effect size of medium or larger.
About 4% to 8% of the variability in trust in government actions and trust in spokespersons, except President Obama, were explained by use of information sources, specifically local and national network TV news. Interestingly, none of the information sources affected trust in President Obama (ΔR2≤.02). The internet also had low effect on the trust in government actions and trust in information sources (ΔR2≤.02).
The mean for the quality of communication scale was 2.92 out of 4. We initially examined the scale as a composite score and found there was no significant difference between the use of the composite score and the individual items in their correlation with trust in government actions. Therefore, to provide further information about key aspects of communication, we examined items individually in our analyses. There were high levels of agreement with most of the quality of H1N1 communication items, with means ranging from 2.73 to 3.07 out of 4 (Table 3). The mean on the question “How closely are you following H1N1 news?” was 2.60 on a 5-point scale (SD=1.11) (weighted mean=2.58), indicating that on average most respondents were not following the news too closely. The inclusion of the communication variables, which consisted of quality of communication items, how closely one followed the news, and the role model items, resulted in significant increases in prediction of trust in government actions and trust in spokespersons (Table 4). The greatest increase in the proportion of variability of trust in government actions and trust in spokespersons were by clear and consistent quality of H1N1 communication and role models (ΔR2≥.09). The 2 items—change and openness—included in the quality of H1N1 communication items had the next strongest effect; both items had moderate effects on local health officials and the CDC. Additionally, the openness of communication affected trust in Secretary Sebelius as a source of information about H1N1.
The attention to H1N1 news was moderately correlated (from r=.25 to .38) with information sources and role model variables, except where respondents chose the other category of information sources. Attention to H1N1 news had a slightly lower correlation with the quality of H1N1 communication items. The 2 quality of H1N1 communication items (openness and clarity) were moderately correlated with the role model items. However, other quality of H1N1 communication items had only small correlations with the role model items. The quality of H1N1 communication items only had small correlations with information sources, except in the case of the clarity of communication and local and national network TV news.
A sequential multinomial logistic regression was performed on vaccination intention by demographics, quality of communication, trust in government actions, and trust in spokespersons. About 6% of variability in vaccination intention was explained by demographic variables (Table 5). Both role model variables, which examined the impact of President Obama's daughters being vaccinated on confidence and willingness to take the vaccine, had a moderate effect (Δ pseudo R2≥.04). Both role model variables swayed the participants from “no” to either “yes” or “don't know.” The participants were about 2 to 2.5 times more likely to either agree to vaccination or were unsure about H1N1 vaccination for each unit increase in role model variables.
Relative Risks of Predicting Vaccination Intention by Demographic and Communication Variables
Demographic variables include race/ethnicity, gender, age, education, income, political party, and political ideology.
p<.05, **p<.01, ***p<.001.
The participants who received more information about H1N1 from local TV news were more likely to agree to vaccination. However, local TV news did not affect vaccination intention for those participants in the “no” and “don't know” categories. Many of the quality of H1N1 communication items moved the participants from “no” responses, shifting them more strongly to the “yes” than “don't know” (higher odds ratio for the “yes” response than “don't know” responses). Participants were about 3 and 4 times more likely to get the vaccine for each unit increase in openness and consistent quality of H1N1 communication items, respectively. The sources of H1N1 information had small effects. However, these sources were more likely to move the participants into the “yes” response to the H1N1 vaccination intention than “don't know” responses. There is a minimal increase in prediction of the vaccination intention by trust in government actions and trust in information sources (ΔR2≤.01).
Discussion
This is the first US study to empirically explore perceived quality of communication and trust in government actions and government spokespersons during an actual pandemic and to examine the association of quality of communication, trust, and a new variable—role models—with vaccination intention midway through the pandemic.
Given our focus, a brief summary of communications about H1N1 at the time the survey was administered is necessary. Results of a Lexis-Nexis search of media appearances by key spokespersons during the 8 weeks leading up to the survey are presented in Figure 1. The search terms “H1N1” and each spokesperson were entered and searched for all US news sources. Generally, CDC appeared in the media more frequently than all other spokespersons during this 8-week period, but less frequently as time passed. The term “governor,” used as a proxy for state government spokespersons, was generally the second most prevalent spokesperson appearing in the media, followed closely by President Obama. Secretary Napolitano, Secretary Sebelius, and “public health department” all had minimal appearances in the media between December 2009 and January 2010. We found that local TV and national network TV news were the most common sources of information for the public.
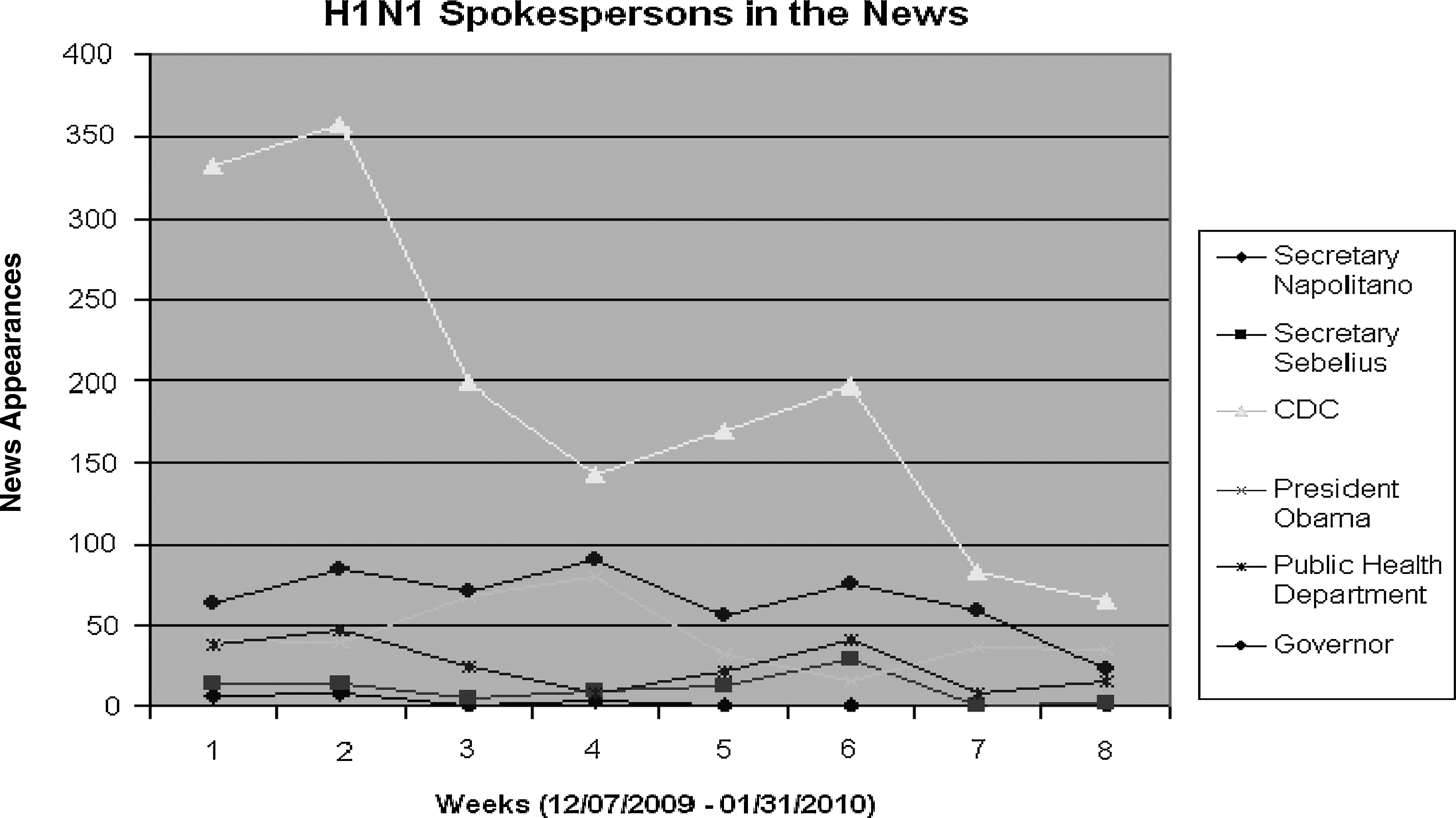
H1N1 Spokespersons in the News from Early December 2009 to Late January 2010
In this context, we found public health officials were the most highly trusted spokespersons, with CDC officials as the most trusted, followed by state and local public health officials and Secretary Sebelius. Interestingly, while elected officials were typically less trusted than public health authorities, President Obama was the next most trusted after the HHS secretary. When we examine only government spokespersons, these findings in the middle of the pandemic are consistent with our results in the early phase of the pandemic, 13 suggesting that there was some stability over time for trust in public health spokespersons at the national, local, and state levels as well as for the president.
Local and state elected officials did not fare as well as trusted spokespersons either early 13 or in the midst of the pandemic. In a pandemic, it is neither uncommon nor inappropriate for elected officials to garner media coverage. It may behoove them to adopt the “Giuliani model,” 30 based on then-Mayor Giuliani's behavior after the 2001 anthrax attacks: He conveyed empathy, compassion, and grasp of the complex situation and made excellent use of his team of experts, each speaking to his or her specific area of responsibility. His demonstration of key components of the trust determination model, including concern, empathy, honesty, and his implicit trust in the team's expertise, offers lessons for elected officials, who would do well to team with public health officials in a pandemic.
In general, we found very high agreement with the quality of communication items. With a random representative sample, we can extrapolate to the larger public, with our results suggesting they found communication to be clear and consistent. An overwhelming majority (92%) reported they were appreciative of the openness of government officials who shared their evolving understanding of the pandemic. Several studies have emphasized the importance of honesty, openness, and transparency with regard to decision making and trust in communication in a pandemic.6,10,18
A review of CDC press briefings gives additional context and reveals the extent to which CDC demonstrated the use of crisis and emergency risk communication best practices as they prepared the public and media for impending changes in their understanding of the pandemic and evolving recommendations. In a press briefing on April 24, 2009, CDC's acting director, Dr. Richard Besser, addressed uncertainty:
I want to acknowledge the importance of uncertainty. At the early stages of an outbreak, there's much uncertainty, and probably more than everyone would like. Our guidelines and advice are likely to be interim and fluid, subject to change as we learn more. We're moving quickly to learn as much as possible and working with many local, state, and international partners to do so. I want to recognize that while we're moving fast, it's very likely that this will be more of a marathon than a sprint. I want to acknowledge change. Our recommendations, advice, approaches will likely change as we learn more about the virus and we learn more about its transmission.
31
By directly addressing uncertainty early in the crisis, it appears the government was able to influence the public's acceptance of future changes in understanding and behavioral recommendations. In our results, we saw over 90% agreement with the item “I understand that information about swine flu will change as scientists learn more about the virus.” While some might question whether social desirability might affect respondents' willingness to acknowledge they did not understand, we believe this result reflects the public's understanding of changing information, which is an improvement over previous emergency situations.
Equally critical is managing the media's ability to understand and accept uncertainty. In a 2009 newspaper article, reporter Lawrence Altman offered an explanation for the uncertainty of evolving disease outbreaks and described some questions that would need to be answered in order for health officials to provide more definitive answers. 32 Because the ability to manage uncertainty well is key to maintaining trust during a pandemic or other public health emergency, the responses of spokespersons, the media, and the public are promising.
Consistent with Freimuth et al, 13 who investigated trust during the early phase of the pandemic, we found that closely following the news, the quality of communication, and role models were associated with higher trust in government actions and spokespersons. Additionally, we found that the perceived quality of communication has an impact on trust in government actions. Trust and quality of communication are clearly linked, but our findings suggest a need for future research about the directionality of this relationship. Vaughn and Tinker 6 argue that trust influences how the public hears and responds to communication and the extent to which they comply with recommendations. Do people trust certain spokespersons because they provide good information, or do people trust certain information as credible because of the source? Does the public trust the government's actions in a pandemic and, therefore, trust its spokespersons, or does trust in official spokespersons lead to trust in government action? Selective exposure theory posits that people's choice of information sources in a pandemic will confirm their preexisting beliefs and predispositions and that whether someone chooses official sources in a pandemic may be determined well in advance of the event. 33 This speaks to the importance of building trust in and loyalty to official sources as well as educating people about what to do in a pandemic (eg, hygiene, vaccination, social distancing, etc) in advance of a pandemic. Clearly, there is a need for further research to understand how quality of communication affects trust, how trust affects perceived quality of communication, and specifically how the varying components of trust affect trust in the message and the messenger.
The relationship between trust and communication and the higher trust in public health officials at multiple levels reinforces the importance of communication training—such as the CDC-developed Crisis and Emergency Risk Communication (CERC) training—for such officials. However, we would argue that training needs to focus on the key components of trust and the recognition that the importance of components may change at different points in the pandemic.
Although initial surveys showed that the general US population expressed relatively high intentions to receive the H1N1 vaccine, actual vaccine coverage estimates were much lower. In September 2009, 50% of adults intended to receive the vaccine, but by the end of January 2010, only 24% of the US population reported having received the vaccine; 34 19.5% of our sample reported having received the vaccine. From the end of January to the end of June, only another 3% were vaccinated, for a total of 27% of adults vaccinated nationally. 35
Our findings point to the importance of clear and consistent communication about vaccination, including the value of role models. Participants who agreed more strongly with the quality of communication and role model questions were more likely to have received the vaccine. The participants were 2.5 to 4 times more likely to get the vaccine for each unit increase in the quality of H1N1 communication items. In addition, participants were almost 2.5 times more likely to get the vaccine for each unit increase in the role model items. Although it is possible that those who were vaccinated agreed with the quality of communication items to reduce any cognitive dissonance around their decision, we believe that the strength of these associations suggests the importance of effective communication in the vaccine decision.
Trust in government actions was weakly associated with intent to get the vaccine in both our previous study and this study. So, why didn't the trust in government translate into higher vaccination rates? The primary reason was likely the relatively low perceived severity of the pandemic itself, which may have reduced demand for vaccination. Second, there was lag time between the first messages from government sources and the availability of vaccine, so people may not have been able to sustain involvement and behavioral intention.
Other factors may have affected the relationship between trust in government and vaccination rates. Government sources were less visible and less vocal as the pandemic wore on. Typically, media outlets turn to government sources almost exclusively in the initial stages of a crisis, but over time they devote more space and airtime to other sources. 36 Also, much like climate change, vaccination is an issue where reporters tend to give equal weight to “both sides” despite a preponderance of scientific data on one side. 37 Reporters need to be made aware (gently) of the need to temper “balance” with the equally important role of vetting the credibility of sources and contextualizing facts for the audience.4,36 Public health officials should strive to build relationships with media outlets in advance of future pandemics, through editorial board meetings and other means of educating journalists about pandemic risks and vaccine safety and efficacy. 4
Expanding beyond Meredith et al's term, “credible models,” 10 we used the term “role models” when we examined the reaction to the president's disclosure of his daughters' immunizations because we believe the impact of the president's actions extend beyond what one would expect from a credible source, from whom we would expect knowledge or expertise that conveys credibility. In our study, President Obama's disclosure had a powerful effect on decisions about vaccination regardless of party affiliation, even when the level of trust in government actions and, specifically, in President Obama differs. Thus, it appears the president's actions to vaccinate his children may have transcended typical political divisions and allowed the public to see him as a parent making decisions on behalf of his family. This suggests that having highly visible role models may be an effective communication strategy, particularly as it may reflect the emphasis on fiduciary responsibility (defined as believing that government officials are committed to the public good) and fairness as a critical component of trust in the context of vaccination decisions. 10 As one way to demonstrate this, the president's public announcement that his daughters had been immunized supports a message that the vaccine was safe and important. Our findings are consistent with a report from the United Kingdom that asserted that then–Prime Minister Tony Blair's unwillingness to disclose the vaccination status of his young son during the controversy over the MMR vaccine undermined the government's own message about the safety of the vaccine. 38
There is a need for further research in several areas: (1) How do components of trust interact with each other? (2) How do those components affect trust, and how might that differ over time? (3) To what extent can careful monitoring and evaluation during a crisis help public health officials modify and address messages and actions to improve their trustworthiness? (4) How can improving the quality of communication further enhance the public's trust and ability to manage uncertainty in a pandemic?
The interaction between quality of communication and trust in government actions in the context of H1N1 gives public health officials food for thought for future emergencies. Because the challenges of communication often vary over the course of an event or pandemic, there is a consistent need to pay close attention to both communication content and delivery and effectively prepare public health officials at all levels to be effective communicators.
Footnotes
Acknowledgments
This study was supported by Public Health Adaptive Systems Studies, a Centers for Disease Control and Prevention Preparedness and Emergency Response Research Center, CDC Grant No. 1P01TP000304-01 (PI, Potter). Drs. Quinn and Musa were also supported by the Research Center of Excellence in Minority Health and Health Disparities (NIH-NCMHD: P60MD000207; PI, Thomas). The opinions expressed by authors contributing to this article do not necessarily reflect the opinions of the Centers for Disease Control and Prevention or the institutions with which the authors are affiliated. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Minority Health and Health Disparities or the National Institutes of Health. The authors also want to acknowledge Erica Casper for her editorial assistance.