
Abstract
This article summarizes major points from a newly released guide published online by the Office of the Assistant Secretary for Preparedness and Response (ASPR). The article reviews basic principles about radiation and its measurement, short-term and long-term effects of radiation, and medical countermeasures as well as essential information about how to prepare for and respond to a nuclear detonation. A link is provided to the manual itself, which in turn is heavily referenced for readers who wish to have more detail.
This article summarizes major points from a newly released guide published online by the Office of the Assistant Secretary for Preparedness and Response. It reviews basic principles about radiation and its measurement, short-term and long-term effects of radiation, and medical countermeasures as well as essential information about how to prepare for and respond to a nuclear detonation.
“Two decades after the end of the Cold War, we face a cruel irony of history—the risk of a nuclear confrontation between nations has gone down, but the risk of nuclear attack has gone up.”
Since 2001, government at all levels, academic institutions, and professional organizations have worked to enhance the nation's ability to prepare for and respond to a nuclear detonation. In the public health and medical arena, many notable achievements include the following publications and websites: Planning Guidance for Response to a Nuclear Detonation, 1 a 10-paper series on “Scarce Resources for a Nuclear Detonation,” 2 health and medical education material available from the Centers for Disease Control and Prevention (CDC), 3 and just-in-time material including algorithm-based management available on the Radiation Emergency Medical Management (REMM) website. 4
In the wake of the Fukushima nuclear power plant crisis in 2011, experts noted the need for a publication covering the basic elements and essential points that would help decision makers understand and manage a major nuclear or radiological disaster. Under the leadership of the Department of Health and Human Services (HHS), Office of the Assistant Secretary for Preparedness and Response (ASPR), and in collaboration with the Center for Biosecurity of UPMC, 14 related background reference documents, authored by top experts in nuclear medical response consequence management, have been combined into a manual, available at http://www.phe.gov/nuclearresponsemanual. The manual is designed as a practical guide that distills and translates key pieces of work on protective actions and medical response and resources to make them more accessible and easier for state and local officials to implement. This article provides an overview of the manual and highlights a few of the key points in each of the papers. The information in this article provides additional background for the UPMC Rad Resilient City project (www.radresilientcity.org/index-original-09-26.html).
Radiation Terminology and Measurement
A brief overview of the basics of radiation and nuclear terminology acquaints readers with concepts useful for understanding the issues addressed in this article. Animations illustrating these concepts are available on the REMM website. 4
Ionizing radiation is radiation that is energetic enough to strip electrons from (ionize) atoms on which it encroaches. When it penetrates body tissues, the resulting damage of the genetic material in cells can have short- and long-term health consequences. Low levels of ionizing radiation are present everywhere on earth as a result of cosmic radiation from space. Ionizing radiation is also emitted from naturally radioactive elements in the earth's crust. Ionizing radiation has many uses: as a tool for medical diagnosis and cancer treatment and for medical instrument sterilization. Ionizing radiation is also used as a source of energy in nuclear reactors and is released by nuclear detonations.
Radiation from a nuclear explosion can be categorized as initial prompt radiation, composed of gamma radiation and neutrons and released nearly instantaneously with the flash from the detonation, and residual radiation, radiation emitted over an extended time from radioactive by-products that can be carried by winds in the upper atmosphere and potentially deposited at great distances from the incident site as radioactive fallout.
People and objects receiving prompt radiation have direct radiation exposure, and they do not pose a health risk to others, just as someone who has had a diagnostic x-ray for medical purposes cannot harm others as a consequence of the exposure. Fallout-emitting radiation, on the other hand, can be hazardous, as it may contaminate the environment, including water, soil, and foods, and then come into contact with people who may inhale or ingest it.
Radioactive Isotopes/Radionuclides
Some forms of certain elements spontaneously release ionizing radiation. These are termed radioactive isotopes of the elements, or radionuclides. When nuclei of some radionuclides, especially uranium-235 and plutonium-239, are bombarded with neutrons, they can split and release vast amounts of energy. This phenomenon is referred to as nuclear fission and is the basis of nuclear reactors and fission-type nuclear bombs. When these nuclei split, they release more neutrons and thus create a chain reaction of nuclear fission that can be self-sustaining. The isotopes resulting from this splitting are called fission products and may themselves be radioactive. In a nuclear reactor, the chain reaction is controlled (by controlling the rate of neutron transfer or neutron flux), but not so in a nuclear bomb.
Measurement
The amount of radiation and its effects depend on processes that can be measured:
• The number of particles produced by a radioactive source over a period of time (activity [disintegrations per second] and rate of decay [half-life]) • The rate of ionization in air produced by the radiation (roentgens, kerma) • The energy of particles absorbed in a substance (absorbed dose; gray, rad) • The biological effect of particles absorbed in living tissue (sieverts, rem)
Understanding radiation can be challenging, in part because of 2 different nomenclature systems. The United States uses the following units: curie (Ci) or fractions of it to describe the rate of decay of an isotope, rad to describe absorbed dose, and rem to describe the (damaging) biological effects of the absorbed dose. The more common international system includes becquerel (Bq), gray (Gy), and sievert (Sv). Because the 2 systems are conceptually but not numerically equivalent, confusion can result, especially during emergency communications. Table 1 provides information about the conversion between the 2 systems.
Units of Measure of Radiation
Sv and Gy are roughly equivalent, as are rem and rad, for a given radiation exposure with gamma and beta radiation. Throughout this article we will use the newer, international system, and we will refer to the biological effect of radiation in sieverts.
Preparedness and Planning for a Nuclear Detonation
A nuclear detonation produces both physical damage and radiation exposure. While the blast, heat, and radiation zones from the detonation overlap in regions closest to the epicenter, major zones can contain some physical injury without radiation (eg, upwind with glass breakage and related injuries), and others can contain radiation with little or no physical damage to structures (eg, fallout areas). In general, responders would be unlikely to enter the severe damage zone (see below).
The medical response activities after a nuclear detonation can be understood to relate to the 3 physical damage zones (severe, moderate, and light damage zones) (Figure 1). 5 With respect to radiation, a dangerous fallout zone (10 R/hr) is recognized, as well as a radiation caution zone (>10 mR/h 1 ). In the latter zone, response and rescue activities can occur, but responder time may be limited because of the potential dose from exposure.* The Radiation TRiage, TReatment, and TRansport (RTR) system overlays a functional response on these response zones. 6
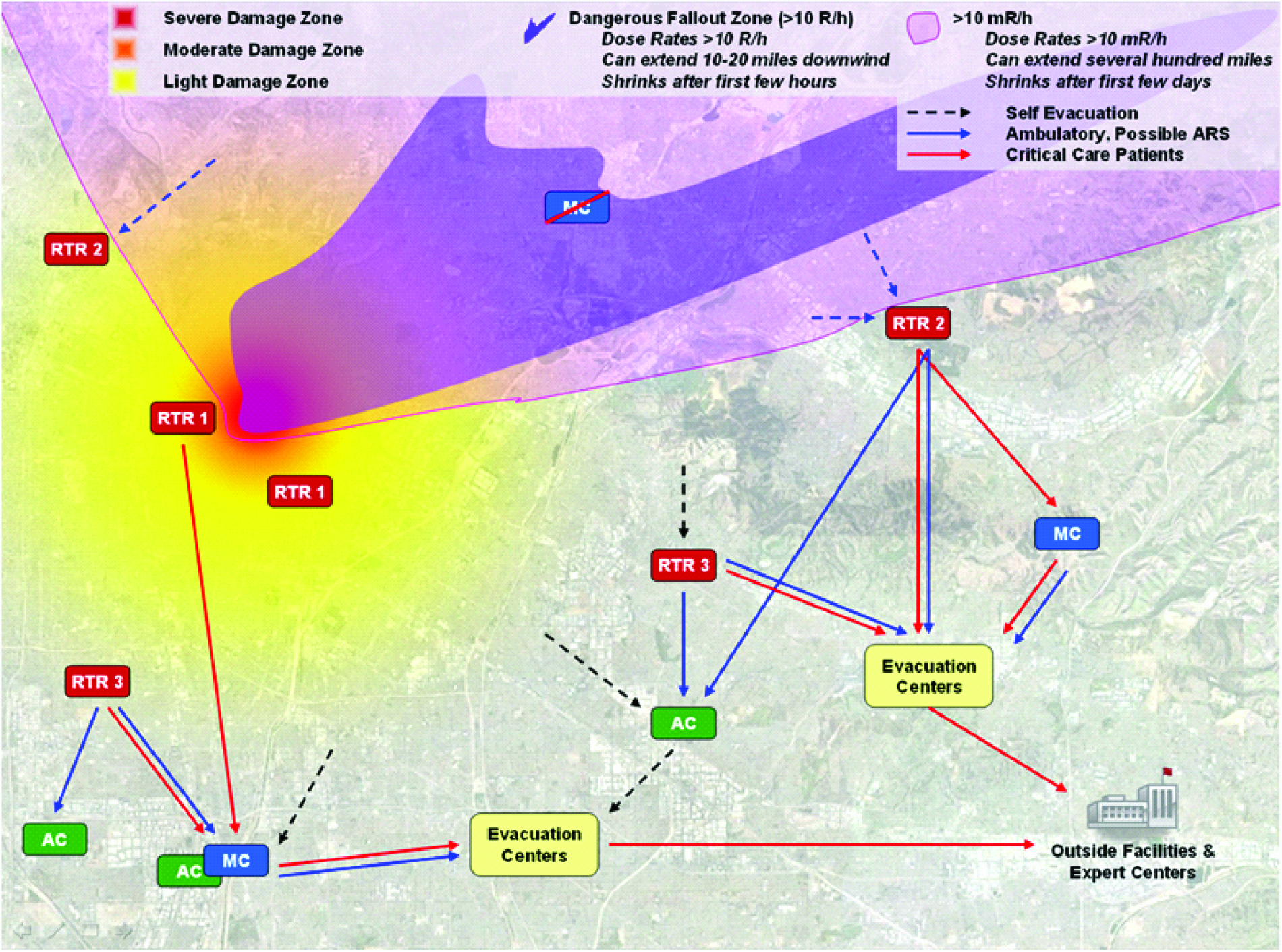
Physical Damage, Radiation, and RTR Zones. Color images available online at www.liebertonline.com/bsp
Damage Zones
• Severe damage (SD) zone—extensive structural damage and few survivors
• Moderate damage (MD) zone—initially difficult access due to debris and variable to low levels of radiation (if present, radiation levels decrease fairly rapidly over time in the first hours to days, which can allow rescue and life-saving operations)
• Light damage (LD) zone—mostly passable; most damage is glass breakage and light debris, with little or no radiation other than where fallout areas overlap the LD zone.
• Dangerous fallout (DF) zone—by dose rate, 10 R/h (100 mSv/h) or greater; may overlap the above zones. The DF zone shrinks rapidly as radioactivity of fallout (and consequent exposure risk) decays rapidly.
• Radiation caution (RC) zone—outside the DF zone, a secondary perimeter of 10 mR/h (0.1 mSv/h) or greater may be established within which time and dose for people working are monitored (like the boundary of the DF zone, this initial perimeter may be moved inward fairly rapidly as decay occurs).
Functional Response System
The RTR system helps in understanding the potential organization of the medical response activities (Figure 1). 6 This system includes several types of sites.
Spontaneously forming RTR sites (casualty collection points):
• RTR1—at or near major physical damage with significant radiation present early • RTR2—limited physical damage and varying radiation present that declines over the first few hours, usually in light damage and/or adjacent DF zones • RTR3—minimal damage and no radiation
Predesignated sites for medical care (nonmedical facilities used as community reception centers
5
are discussed below, along with population monitoring):
• Medical care (MC) sites, including alternative medical care sites • Assembly centers (AC), some of which may be co-located near MC sites for people who do not require medical care • Evacuation centers (EC)
Resource availability and need (staff, space, supplies) will vary by proximity to the incident and will change over time. For example, hospitals closest to the detonation will be quickly overwhelmed by a surge of casualties and will rapidly exhaust resources and medical personnel. The plan, therefore, is to distribute patients as quickly as possible to medical assistance further away from the affected area, where replenishment of supplies and staff will be easier. Key strategies for managing medical care in scarce resource settings are summarized in Figure 2.
Strategies for Scarce Resource Situations
In the chaotic, mass casualty, scarce-resource environment resulting from a nuclear detonation, effective coordination and use of nontraditional emergency response resources (eg, private practices, skilled nursing, commercial labs, etc) will enhance the otherwise strained medical capabilities. An understanding of the quantity, location, and availability of these resources, and an ability to access and pay for them in a coordinated, timely manner, is crucial for both planning and response.
Preplanned resource support and logistical plans for coordinating federal, regional, state, and local entities will be important. Plans for how various agencies can be deployed to predesignated and “newly designated” local and regional staging areas will attempt to optimize resource availability and mitigate bottlenecks and confusion in the hours and days after an incident.
Effective resource planning also requires an updated state-by-state, region-by-region list of all potentially available IND (improvised nuclear device) response assets. To some extent, this has been partially done by the Emergency Management Agency Compact (EMAC) and other mutual aid programs, such as the Midwest's huge Mutual Aid Box Alarm System; by some individual states; by FEMA under the All-Hazards Approach; and by some ASPR regional offices.
Local planning is most effective when it is integrated across the tiers of response,7,8 including state and federal partners. Integrated planning is facilitated through the use of planning and response tools such as the HHS resource mapping tool, MedMap. 9 MedMap facilitates sharing situational awareness with the local and regional responders and can show locations of healthcare facilities in relation to other overlays and demographic information. Designated local and state government partners can request access to MedMap through their HHS/ASPR Regional Emergency Coordinators.
Protective Actions in a Nutshell: What to Do, What Not to Do, and Why
Shielding from immediate radiation effects (completed in seconds after detonation) is accomplished only by being inside a heavy building or very far away. Protection from radiation in fallout, however, can be achieved with proper response behavior. Fallout is generated when the dust and debris generated by the explosion combine with radioactive fission products produced in the nuclear explosion and are drawn upward by the rising fireball. Ground-level detonations generate more fallout, comparable to air bursts, because of the “excavated” debris. This cloud climbs rapidly through the atmosphere, potentially up to 5 miles or higher for very large detonations, forming a “mushroom cloud” from which highly radioactive particles coalesce and drop back down to earth as it cools.
Winds at different elevations may carry and drop fallout in a manner difficult to predict. Present understanding of the capabilities of terrorists would suggest that a nuclear explosion that could be improvised would be relatively low-yield (low kT), implying a relatively small mushroom cloud with relatively little cloud-rise.
The following points about fallout are important (graphics are available at http://www.remm.nlm.gov/nuclearexplosion.htm#plume):
• The radiation hazard comes principally from exposure to the ionizing radiation that fallout particles give off as they decay. This happens continually as the particles are being deposited from the air and remain there afterward. External exposure to the emitted gamma rays from fallout is generally more dangerous than inhalation of fallout particles, since most particles are too large to be effectively inhaled into the deep lung. Nonetheless, precautions are recommended to prevent or minimize both inhalation and ingestion of radionuclides. • Radiation levels from these particles will decrease quickly. Most (∼55%) of the potential exposure to people occurs in the first hour, and 80% occurs in the first day. These percentages apply to fallout that is received close to the detonation site. The exposure from fallout that is deposited at much greater distances away from the detonation site will decrease less rapidly after the fallout is deposited, since much of the radiation it produced was given off by rapidly decaying isotopes while it was in transit in the atmosphere; radiation that remains on later deposition will be from the more slowly decaying isotopes. • Although highly dependent on weather conditions, the most dangerous concentrations of fallout particles are likely to occur within 10 to 20 miles of the incident and may be clearly visible as they fall, often the size of fine sand, table salt,
10
or ash.
11
• Cleanup of fallout is beyond the scope of this manuscript.
Protective Actions: Shelter and Evacuation
Two principal protective action recommendations (PARs) may be implemented to protect the public and responders from fallout. The first is to take shelter followed later by evacuation. 1
Take Shelter
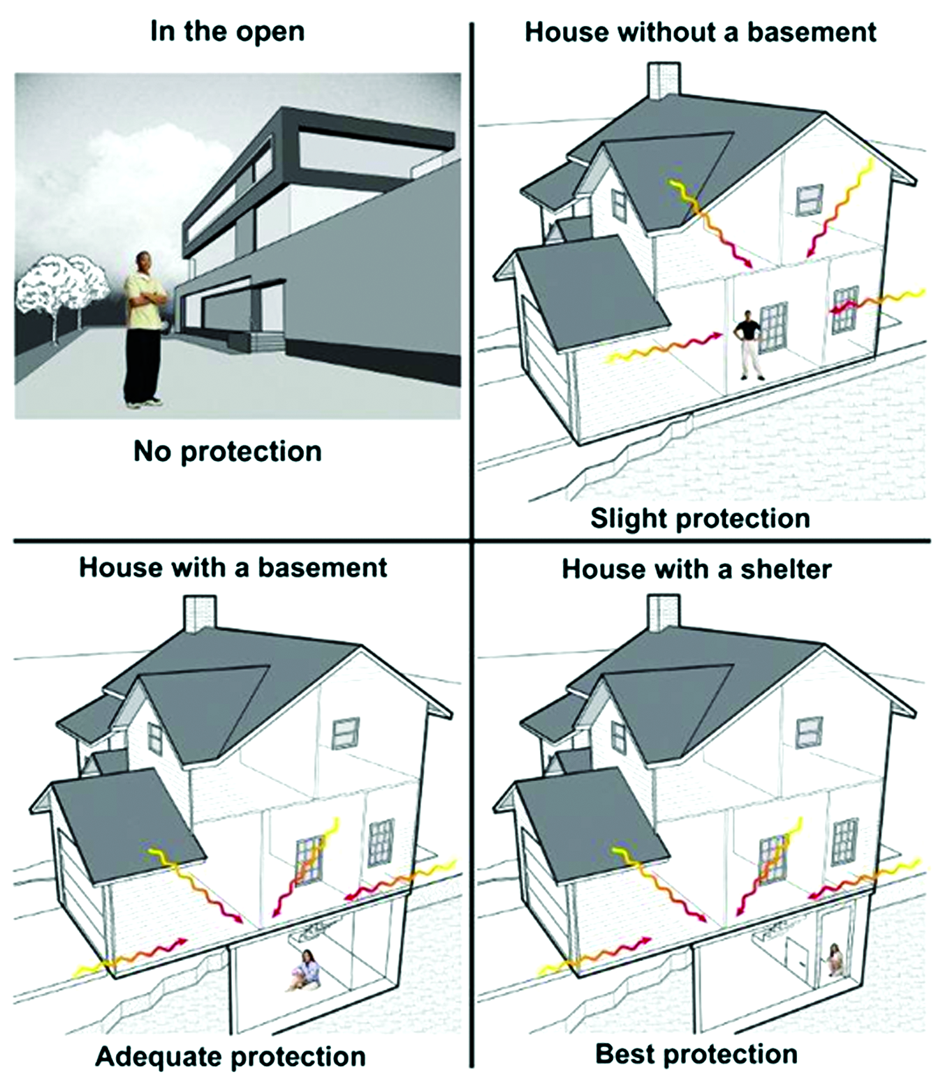
Although any shelter will provide some protection (shielding) from radiation dose, some shelter locations are more effective than others. Generally, a below-ground location (eg, a basement or underground garage) is better than above-grade locations (see Figure 3), large buildings are better than small, further interior is better than nearer the exterior, and heavy concrete or masonry walls are better than wood. Shelters such as houses with basements, large multistory structures, and underground parking garages or tunnels can generally reduce doses from fallout by a factor of 10 or more (see Figure 3). These structures would generally provide adequate shelter. Vehicles and single-story wood frame houses without basements provide only minimal shelter and should not be considered adequate shelter. The worst situation would be for a survivor to be caught outdoors when fallout arrives or to choose to go outdoors in the early hours when fallout is most dangerous.

Protection by Structures. Color images available online at www.liebertonline.com/bsp
Evacuate
Immediate evacuation has serious drawbacks as a protective action in the early hours after detonation of an IND.
• The first 2 hours produce the highest dose rate from the fallout; postponing evacuation for 2 hours or longer, if possible, would result in more protection.
• Prediction of precise dose levels from fallout will be difficult. Meteorologic information, especially wind direction and force, may help predict the most likely directions and amount of fallout deposition. Care is advised to prevent uninformed evacuations that might move people into or through areas of dangerous contamination.
• Cars offer little protection from exposure to gamma rays emitted from fallout, and those evacuating on foot would have no protection.
• All evacuations take time; moving any number of people even a few miles will take many hours given the likelihood of damaged structures, debris obstruction, and traffic accidents and congestion. During this time risk of radiation exposure is high.
• Informed evacuation can limit time in fallout zones and thereby keep the radiation dose as low as possible.
What to Do
Because the fallout radiation hazard is so high early after the detonation and within about 20 miles of ground zero, and because the deposition of fallout is unpredictable, immediately taking shelter in an adequate shelter is the unequivocal recommendation of the federal government. 1
The best initial action immediately following a nuclear explosion is to take shelter in the nearest and most protective building or structure and listen for instructions from authorities. You may have up to 10 minutes before fallout arrives if you are not in the MD or LD zones. Go below ground if that option is available or to the center of the shelter structure. Shelter for 24 hours and attempt to access media or other emergency broadcasts (eg, National Weather Service, Emergency Alert System).
Preparing the Home for Sheltering in Place
Every American family should prepare his or her home for the possibility of a disaster. 12 Preparation is especially important to minimize exposure that could accompany a nuclear detonation or for those who may be in the path of hazardous fallout. Families can take 4 steps to be better prepared to shelter.
1. Psychologically Prepare
Individuals must recognize that nuclear terrorism is possible, understand key protective actions, and put plans in place to support these actions. Being motivated to create a safe room is one part of psychological preparedness. It is equally important to address psychological issues that could interfere with people's willingness to remain in a safe room. Following a disaster, a typical urge is to connect with loved ones to check on their welfare. Parents in particular often feel a strong pull to immediately reunite with their children and bring them home. 13 When fallout is present, rushing to pick up children may jeopardize the health of both the child and the parent. Therefore, parents must have confidence that schools, for example, have identified adequate shelters to ensure their children's safety. They also need to know the school's plan for reuniting them with their children. If these measures are in place, parents are more likely to remain sheltered long enough for radiation levels to diminish.
2. Choose a Safe Room
The safest place in a home following a nuclear detonation incident is a centrally located room or basement with the fewest number of windows. The rooms in a home that give the highest fallout protection are the ones that put the most earth, building material, and distance between you and the fallout (Figure 4).
Selecting a Safe Room. Color images available online at www.liebertonline.com/bsp
The needs of any pets should be considered (to prevent contamination, pets should not go outside). Note that locations that are safest in other dangerous situations, such as tornados, are also safest for protection from fallout; such a place can have broad utility.
3. Stock a Safe Room
The safe room should be stocked with enough supplies to last for up to 3 days. (For a list of supplies to consider, see www.ready.gov/america/getakit/index.html.)
4. Maintain a Safe Room
All family members should know where the shelter is and understand its purpose. Supplies should be routinely checked as suggested in Table 2.
Safe Room Maintenance
Community Reception Centers and Population Monitoring
The focus of this section is on population monitoring that takes place away from the immediately affected area at locations referred to as Community Reception Centers (CRCs). 14 These sites are intended to provide minimal treatment, at most, and generally are not built on a medical model. Injured or ill people should be directed to sites that offer medical care. Community reception centers may be a mixture of assembly centers and RTR3 (minimal damage casualty collection) sites. Some may be many miles away from the incident site. Displaced people should be directed to nearby CRC locations for assistance before proceeding to stay with family or friends or to seek temporary housing at public shelters (which local communities must establish to receive and care for this population). State and local agencies should plan to accommodate the needs of pets and service animals in CRCs and shelters. Contaminated pets can present a health risk to their owners, especially children who pet them.
As stated in the National Response Framework (NRF) Nuclear/Radiological Incident Annex, “decontamination of possibly affected victims is accomplished locally and is the responsibility of state, tribal, and local governments.” 15 A prudent assumption is that after a large-scale nuclear emergency, local resources will primarily provide population-monitoring services in host communities distant from ground zero. Therefore, local communities everywhere must include population monitoring after a radiation emergency as part of their all-hazard preparedness planning.
CRCs should be opened within 24 to 48 hours after a radiation emergency (or sooner if resources are available) in locations outside the affected areas. The following basic services are offered at a CRC:
• Screening people for radioactive contamination; • Assisting people with washing or decontamination; • Collecting epidemiologic data, including exposure risk and any prior or current symptoms of illness; • Registering people for reunification, tracking, and long-term follow up; and • Prioritizing people for further care and/or medical evacuation.
CRCs are modeled closely after points of dispensing (PODs), which many public health departments have already incorporated into their response plans for biological threats. They are staffed by local government employees and by organized volunteers such as members of the Medical Reserve Corps. 16 Unlike PODs, however, CRCs need radiation detection equipment and trained radiation protection personnel who can perform and interpret the radiation screening, as well as resources to assist with decontamination. Radiation detection equipment will be needed at a number of locations.
Establishing and operating a CRC is a community effort involving local emergency management, law enforcement, and public health agencies, as well as other local response and volunteer organizations. In addition to providing vital services to people who need them, CRCs can help reduce the burden on hospitals and maximize use of scarce medical resources. In providing an alternative location for initial attention, they can reduce the number of patients presenting to hospitals and identify those in need of further interventions or countermeasures that can reduce subsequent morbidity and mortality.
In addition, because people reporting to public shelters like CRCs need to be monitored for contamination, operation of public shelters after a nuclear detonation depends on the successful implementation of population monitoring activities at these CRCs, which can be co-located with public shelters. CDC and Oak Ridge Institute for Science and Education (ORISE) have developed a standardized CRC model that is modular and can be adapted to the needs and resources of each community (www.orau.gov/rsb/vcrc/).
Population Monitoring After a Nuclear Detonation
Population monitoring begins with expeditious screening of a population potentially exposed to radiation or contaminated with radioactive material, assisting with decontamination, evaluating information related to their exposure history, and registering people for subsequent follow-up. The general process of population monitoring is described in detail in the CDC guide to population monitoring. 14 Considerations that are particularly applicable to a nuclear detonation scenario are discussed in detail in the federal Planning Guidance for Response to a Nuclear Detonation. 1 Because of the large number of displaced people and the widespread geographic distribution of this population, communities throughout the country should incorporate population monitoring in their response plans even if they do not perceive themselves to be a likely nuclear target.
The primary considerations regarding screening, decontamination, and monitoring of the population after a nuclear detonation are described below.
Collection of Data for Tracking and Health Studies
If resources are available at the CRC, pertinent information can be collected to assist in monitoring the health status of the affected population, in identifying the most important health needs, and in counting people with illnesses and radiation contamination. Familiarity with previously conducted studies of exposed people is useful to identify risk factors in the population involved in the incident and can suggest ways public health officials can help to reduce those risks. Information about the exposed population, combined with results from environmental radiation contamination assessments, healthcare providers, and laboratory testing, may enable public health officials to assess population-level radiation exposure, contamination, and the potential for associated health effects. These assessments will identify populations most likely to need medical care and treatment both immediately and in the years to come and can enable study of long-term health effects.
Figure 5 provides a sample of the type of detailed data that could be collected at a CRC following a radiation emergency. A more complete question bank is available from CDC. 5
Sample Data Elements that Could Be Collected at Community Reception Centers
Note: A more complete question bank and example forms are available from CDC. 5
Medical Management of Acute Responses to Radiation
People exposed to high levels of whole-body ionizing radiation (greater than about 1-2 Sv) over a short period of time may develop acute radiation syndrome (ARS). Symptoms may include vomiting, diarrhea, headache, dizziness, weakness, bleeding, and redness of the skin, depending on the severity of exposure. In a mass-casualty setting, efficient triage of irradiated casualties is essential. It will be important to identify those who have received clinically significant but not invariably lethal doses of radiation—roughly 2-10 Sv of whole-body exposure. These are the victims who need specialized, resource-intensive, complex, and sometimes urgent care.
In resource-scarce settings, symptomatic care (eg, pain relief) is recommended, if possible, but to conserve resources and provide the greatest good to the greatest number, life-sustaining measures should be withheld from casualties with nonsurvivable trauma, thermal burns, and/or radiation exposures. Extensive triage algorithms that emphasize fairness were recently published to guide the selection of appropriate candidates for life-sustaining care in resource-limited settings in order to maximize survivability for the overall population. 17
Management of ARS
Current management of ARS does not substantially differ from the management of pancytopenia in other settings, such as after treatment with high-dose myelosuppressive chemotherapy for cancer. Administering myeloid cytokines to appropriately selected victims of short-term external exposure is recommended, but it is not recommended for those with only high levels of ongoing, internal contamination. 18 This strategy offers 2 potential benefits after a mass-casualty radiation incident. It may reduce morbidity and mortality from neutropenic complications, and it can lessen the need for subsequent or continued hospitalization during the postincident period when medical resources and personnel may be extremely limited.
The current challenge is that the capacity to administer cytokines (and supportive care) is likely to fall far short of serving those who might benefit from them after an IND detonation because of the limited supply of personnel, cytokines, and supplies where they are needed. Therefore, appropriate triage (for both trauma and radiation injury) will be important, with a goal of ensuring that the greatest good is done for the greatest number of victims. Those who may not need myeloid cytokines immediately should be referred for later evaluation and possibly treatment in a more resource-rich environment. Those who are unlikely to survive should be given palliative care, but not resource-intensive care, which is reserved for those most likely to survive.
Candidates for myeloid cytokines include patients with the following characteristics:
• Laboratory-measured neutropenia (<500 cells per cc) developing after the IND detonation; • History of whole-body radiation exposure likely to have been above a certain level (eg, 200 cGy, based on geography of the person and known radiation level maps of the incident), even without a confirmed dose estimate from a valid biodosimetry tool; and • Physical symptoms or injuries strongly suggesting combined injury (radiation plus survivable trauma and/or burn).
Studies of medical management of neutropenia in nonhuman primates suggest that initiating myeloid cytokines within 24 hours of exposure may improve outcomes. Myeloid cytokines [granulocyte-colony stimulating factor (G-CSF; filgrastim), granulocyte monocyte-colony stimulating factor (GM-CSF; sargramostatin), or pegylated G-CSF (pegfilgrastim)] may reduce the duration of neutropenia, hospital length of stay, and overall costs.
Myeloid cytokines should be initiated as soon as evidence indicates a casualty has developed or will develop neutropenia (ie, less than 500 neutrophils per mm3). Specific indications for initiating myeloid cytokines prior to the onset of neutropenia include a projected whole-body dose of 2 Sv or more based on (1) physical dose reconstruction using geographic information; (2) clinical signs; and/or (3) lymphocyte-depletion kinetics. Drugs should be continued for 14-21 days or until normalization of the granulocyte count. Supply and continuity of administration of these agents is a key planning challenge.
Supportive care measures are also important for managing victims. Antiemetics for vomiting (REMM 19 ) will help in the early hours as nausea and vomiting may occur in many people—even those without radiation exposure. Hydration will be needed for radiation and trauma. Antimicrobials will be needed to prevent infections during the neutropenic period and have been shown to improve survival in animal models of ARS.
Radiation Injury Treatment Network
The Radiation Injury Treatment Network (RITN) is a collaboration of 61 medical centers and hospitals with expertise in the management of myelosuppression, blood donor centers, and umbilical cord banks. 20 It was established through collaboration between the American Society for Blood and Marrow Transplantation (ASBMT) and the National Marrow Donor Program (NMDP). RITN is supported financially by the US Office of Naval Research, the Health Resources and Services Administration (HRSA), and ASPR. RITN has established standard operating procedures and treatment guidelines that can be used by medical professionals outside the RITN network who are participating in the incident response. These guidelines have been developed based both on the medical expertise of RITN leadership in clinical oncology and the abundant literature available in this field.21-30
RITN has 2 primary goals: (1) provide facilities and staff for intensive supportive care in the aftermath of a marrow-toxic mass-casualty incident; and (2) educate hematologists, oncologists, stem cell transplant practitioners, and nursing and support staff about their potential involvement in the response to such an incident. Many patients at risk for radiation-induced neutropenia and thrombocytopenia can be observed and monitored as outpatients, as is done routinely in cancer care.
RITN centers are referral centers only. They are neither first-receiving nor decontamination facilities. Initial decontamination and the treatment of life-threatening injuries must be completed prior to RITN involvement. Transport of casualties from the incident site would be organized through the National Disaster Medical System (NDMS). 31 RITN centers have existing infrastructure and expertise for managing casualties with bone marrow toxicity. Most of these casualties would require supportive care, either as inpatients or outpatients, and would not undergo hematopoietic cell transplantation. Besides direct care of inpatients or monitoring and care of outpatients, RITN sites could also serve as consultants to other sites providing care.
In April 2011, RITN performed a survey to determine the willingness of RITN centers to voluntarily accept irradiated casualties across a range of hypothetical circumstances. As outlined in Figure 6, the number of casualties accepted by centers increased markedly with either (1) use of partner hospitals to offload existing patients and/or irradiated casualties, or (2) clearly defined austerity measures. These austerity measures included the treatment and housing of casualties in nontraditional sites.

RITN Research Results on Scarcity. Color images available online at www.liebertonline.com/bsp
All of these treatments depend on having adequate supplies of medical countermeasures, staff, and other resources. Issues of compensation, licensing, and liability are also among the important considerations. The availability of needed resources will vary by time and distance from the nuclear detonation.
Providing MCMs in a Scarce Resources Setting
The initial medical response to a nuclear detonation would be in local facilities and undertaken by local responders. The ability to provide the necessary supplies will require preparation and innovative approaches. Potential sources for replenishing medical supplies and medical countermeasures (MCMs) are illustrated in Figure 7.
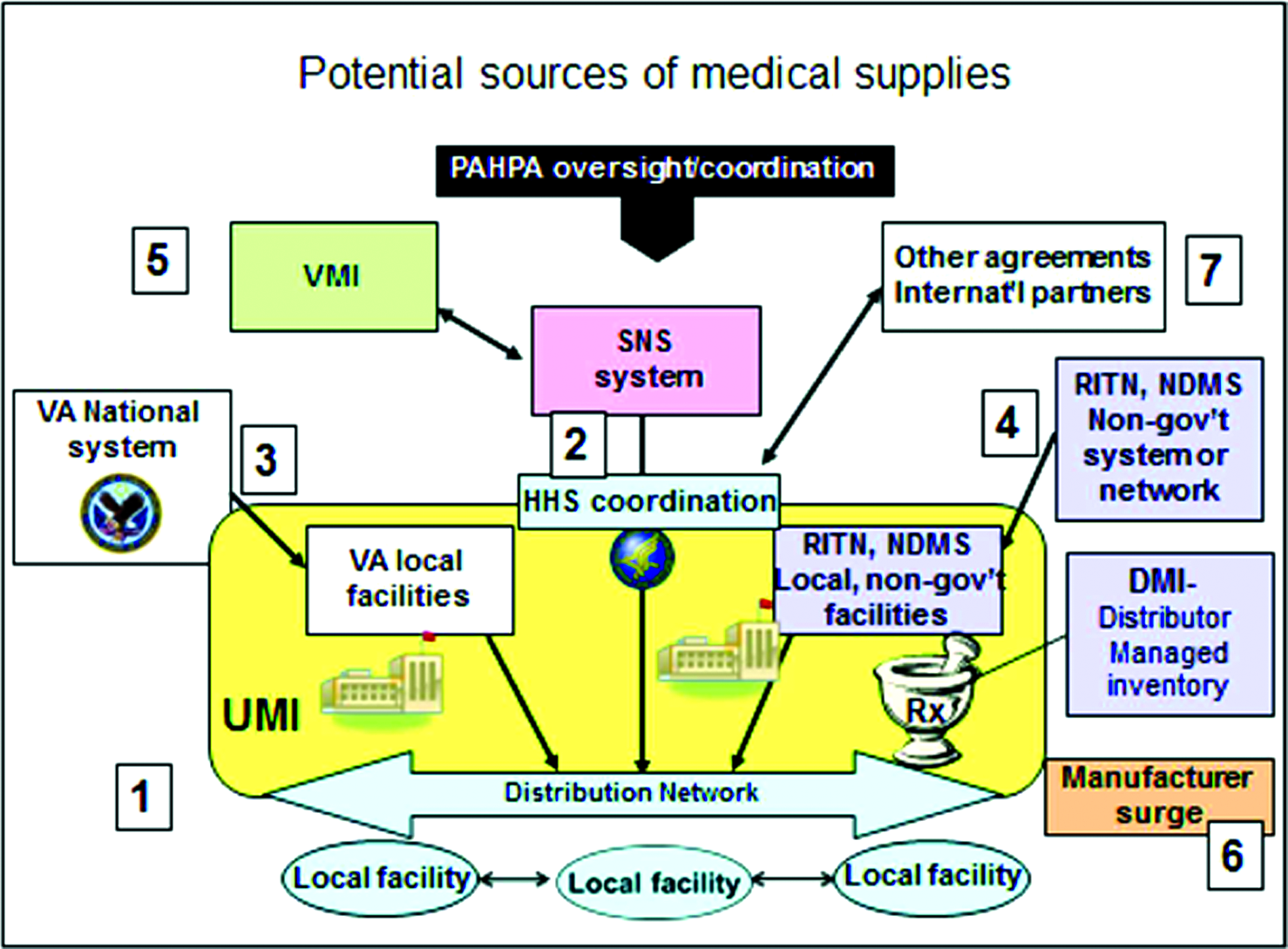
MCM Availability. This is a theoretical approach under development. Color images available online at www.liebertonline.com/bsp
In general, hospitals keep very low inventory and use just-in-time inventory management for obtaining resources. Working from the level of the local facility up, supplies could be supplemented in one or more of the following ways:
1. Local distribution networks could include a specific bubble in the supply line—that is, a user-managed inventory (UMI, #1) or distributor-managed inventory (DMI).
32
Since the cytokines have a multiyear shelf life and are used routinely, it might be possible to keep a 3- to 12-month supply on hand that could be used before it expires even if no incident requiring massive use were to occur. This would provide many more “first doses” than otherwise possible with the just-in-time inventory approach. Potential participants in UMI include the VA (#3) and the RITN (#4, Figure 7).
20
2. Materiel from the Strategic National Stockpile (SNS),
33
a national repository of pharmaceuticals, medical supplies, and equipment, can be deployed during a public health emergency for use by local, state, and regional responders. Initial supplies can reach the affected area within 12 to 24 hours of the federal decision to deploy. As part of its operational plan, the SNS also has agreements with manufacturers to provide some pharmaceuticals and supplies on request, called vendor-managed inventory (VMI) (#5, Figure 7). 3. Manufacturer surge capacity would likely occur either voluntarily in response to the obvious need or by request of the local, state, or federal government (#6). This will likely take days to weeks. 4. Medical supplies or drugs may be obtained from international partners, in special circumstances (#7), although importing drugs is complicated and requires complex approval among governments as well as by the FDA.
A current approach to developing MCMs for terrorism and mass casualty response is to prioritize drugs or supplies that have a use in routine medical care. Products with utility for both mass casualty emergencies and for routine medical use can be considered “dual-utility” products. † Dual utility ensures familiarity with the MCMs by the clinicians who use them for routine purposes and affords the potential cost savings of avoiding expiration of stockpiled supplies, if rotation into routine use is feasible. UMI, DMI, and VMI afford such rotation. Stockpiling in a central repository can be especially problematic for drugs with short shelf lives, as frequent replacement is necessary, unless the drug is eligible for the FDA's Shelf-Life Extension Program, and, even so, shelf-life extension incurs a cost. On the other hand, stockpiling may induce pharmaceutical manufacturers to produce drugs that may otherwise have a limited commercial market. Bone marrow cytokines can be considered “dual-utility” (see discussion below regarding use off label or under Emergency Use Authorization), as can antibiotics, antiemetics, and other products used in supportive care.
Planned pre-positioning of MCMs as close to an incident location as possible provides both time and logistical advantages for first responders. The benefits of UMI go beyond rapid deployment of MCMs by offering for some MCMs a more cost-effective approach for managing the inventory compared to central stockpiling. The UMI concept is characterized by 4 key features: (1) dual-utility MCMs would be used; (2) the UMI model would require storage at multiple medical facilities across the nation; participating medical facilities would store a sufficient inventory or “bubble” to help meet immediate surge MCM needs; (3) UMI-related MCMs would be managed to ensure the inventory would not expire before use, using first-in, first-out protocols (avoiding disposal and replacement costs); and (4) the UMI “bubble” inventory would be used locally to treat casualties in an emergency, including evacuees from other localities. The UMI “bubble” inventory could also be funneled locally to areas of greatest immediate need similar to central stockpiling and VMI. UMI implies a dynamic response system, linking the local, state, regional, and federal responses while providing the potential for a more rapid response and more efficient management of limited resources; however, UMI would not eliminate the need for other stockpiling options and would not be a good fit for all MCMs. An ancillary benefit of UMI is that the on-site supply bubble can help buffer against temporary shortages due to unusual fluctuations in routine demand.
An additional advantage of UMI is that it expands widespread storage of MCMs, reducing the risk of mass MCM destruction at a single storage facility. The VA medical care system is a natural fit for UMI, given its expanded role in civilian emergency response, existing network of facilities and resources, and a well-developed pharmacy-management system. With experience, data, and further development, UMI could be considered for major medical centers, retail pharmacies, and distribution networks.
Prescription drugs are approved by the FDA for treatment of a specific indication described in the drug's labeling. While physicians routinely use prescription medications “off-label” in their daily practice, a large-scale emergency will have no or limited physician-patient relationships allowing this to occur. An Emergency Use Authorization (EUA) 34 would be requested if the drug is used for any purpose other than those covered by the information found in the labeling. The EUA authority allows the FDA commissioner to allow MCMs to be used in an emergency caused by biological, chemical, radiological, or nuclear agents, in the absence of adequate and available MCMs are fully approved for the purpose, if the anticipated benefit is greater than the assessed risk under the circumstances.
At present, no drugs have a specific indication for treatment of ARS; however, ARS treatment guidelines are based on extensive prior medical experience with treating bone marrow suppression due to other causes. As a result, drugs would need to be used “off label,” at the discretion of the physician, if the incident is small and an established physician-patient relationship exists, or under an EUA granted by the FDA commissioner for a large-scale incident. When feasible, packets of information are prepared in advance to expedite establishment of EUAs after an emergency is declared.
A great deal of thought has gone into exploring the ethical and practical issues associated with delivering medical care in a scarce-resource environment. Limited resources may affect the treatment priority of the injured and ill. In-depth discussion of this important topic is provided in the manual and previously published papers. 2 Figure 8 illustrates how triage category for radiation-only injury would change as the resource availability and related standards of care change. As resources decrease from normal to poor, the triage category for those with severe radiation changes from immediate to delayed to expectant. The priority for receiving MCMs also changes.
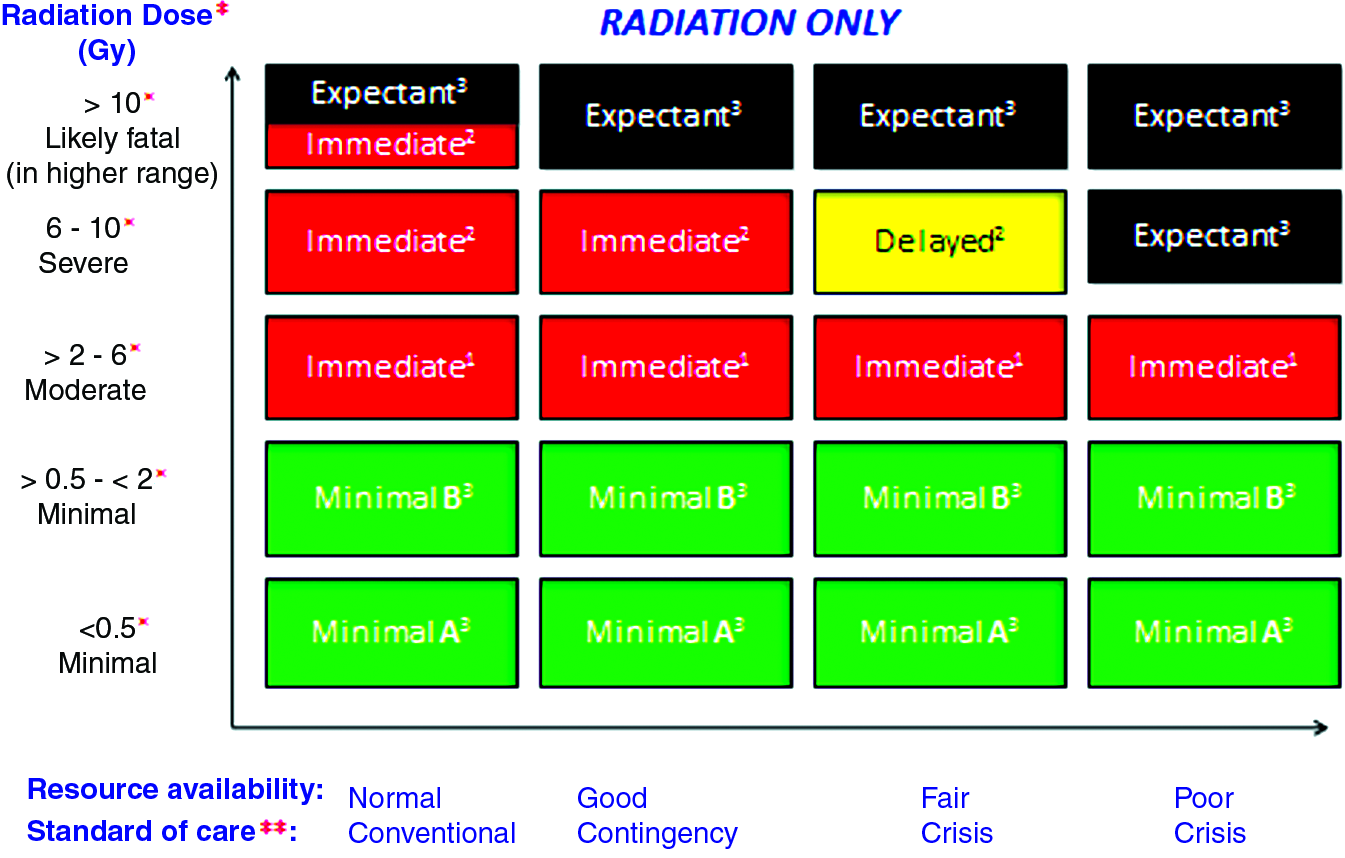
Triage Category Affected by Radiation Dose and Resource Availability. Color images available online at www.liebertonline.com/bsp
MCM Research and Product Development
As noted earlier, medical response to radiological and nuclear incidents includes supplies for treating trauma and burns; drugs for vomiting, pain, and infection; blood products; and specific medical countermeasures for radiation injury. In addition, rapid and accurate biodosimetry tools are needed to estimate absorbed doses of radiation. Innovative diagnostic approaches, including point-of-care and high-throughput biodosimetry tools, are being identified, optimized, and validated to provide enhanced response capability for triage applications, field-deployable laboratories, and reference laboratories. A range of existing and developing technologies are being considered for incorporation into a Radiation Laboratory Network (RadLN) or an Integrated Clinical Diagnostics System (ICDS) that is under development. The ongoing approaches to MCMs, including biodosimetry capabilities, and to RadLN development, involve a continuum of activities from basic science, through advanced development, to preclinical and clinical assessment, all in the context of guidelines and review by the FDA.
Leading the US government's effort to develop and gain FDA approval of medical countermeasures to prevent, mitigate, or treat radiation injury are components of HHS: NIH, particularly the National Institute of Allergy and Infectious Diseases (NIAID),35-40 and ASPR, including the Office of Policy and Planning (OPP) 41 and the Biomedical Advanced Research and Development Authority (BARDA).42,43 NIAID supports the development of the research infrastructure and the advancement of basic science in radiobiology that is built on basic radiation biology research programs such as those in NIH's National Cancer Institute, as well as programs in the Department of Defense (DoD), the Department of Energy (DoE), and National Aeronautics and Space Administration (NASA). OPP works through the Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) 42 to develop civilian MCM requirements and policy initiatives. BARDA supports the advanced product development, FDA approval, and acquisition of MCMs through contracts with developers and companies.39,40
MCMs are characterized in 3 classes:
• Protectors—given before exposure to radiation to lessen effects. These are relevant to first responders and military personnel, who may have knowledge or risk of impending exposure, but they are not relevant to general civilian use, for which exposure would be unanticipated.
‡
• Mitigators—given after exposure to reduce severity of effects before clinical manifestation. • Treatments—given after the effects to be treated have developed clinically.
An MCM such as a myeloid cytokine—for the hematological ARS syndrome—can be both a mitigator and a treatment.
A few MCMs for radiation-related indications are FDA approved—decorporation and blocking agents that facilitate removal of internalized radionuclides or blocking of their incorporation—but currently no MCMs are FDA approved to treat individuals with ARS or delayed effects of acute radiation exposure (DEARE), such as lung or kidney fibrosis. Some MCMs approved for other indications might be useful to treat ARS 29 or DEARE; these could be used off label or under an EUA (http://www.fda.gov/emergencypreparedness/counterterrorism/ucm182568.htm).
MCMs that are currently being researched, evaluated, and developed for ARS, radionuclide decorporation, and biodosimetry are listed in Figure 9.
Figure 9. Types of Radiation/Nuclear Medical Countermeasures under Development (through NIAID and BARDA)
• Mechanisms of action
○ Antioxidants
○ Anti-inflammatories
○ Antiapoptotics
○ Growth factors and cytokines
○ Cell-based therapies
○ Others
• Radiation syndromes
○ Acute radiation syndromes (hematologic, gastrointestinal, central nervous system)
○ Delayed effects of radiation exposure (skin, lung, kidney, others)
• Radionuclides
○ Blocking agents
○ Decorporation agensts
Diagnostics
Medical teams require the ability to make accurate radiation dose assessments for the prompt treatment of exposed individuals and for optimum use of a limited supply of radiation MCMs. The primary capacity will come from the local laboratories and local or regional agreements, but the need for a larger system is recognized.
To that end, the Rad-LN (or ICDS) is a concept under development by multiagency experts coordinated by ASPR with other HHS and federal partners. 40 The Rad-LN would provide increased cytogenetic dicentric chromosome assay (DCA) capabilities, enhanced capacities for the CDC Radiobioassay Laboratory, and hematology surge capacities, by networking-capable labs, increasing mobile capacity, providing certified protocols and guidance, and leveraging international collaboration. Because techniques such as cytogenetics are routinely done in hospitals, regional and state networks can help provide surge capacity with some training in the DCA and exercising, as demonstrated in Connecticut 43 and in progress in the US. The proposed Rad-LN could also serve as a test bed for assessment and interlaboratory comparison for novel biodosimetry devices and potential biomarkers and as a node for ensuring adequate oversight, balancing investment, and optimizing or improving existing capabilities.
No biodosimetry assays or devices to determine if individuals were exposed to radiation are currently FDA approved. However, current laboratory triage techniques using lymphocyte depletion kinetics can provide an early estimate of dose but require serial readings over several days to be most accurate (see REMM 44 ). Dose estimates by DCA have been used as the gold standard for assessment of absorbed dose in radiation accidents for decades. It is currently the tool of choice for estimating radiation dose in the short term. However, the DCA is labor-intensive and time-consuming, and strategies are needed to increase assay throughput for use efficiently in a mass casualty scenario. Rapid and accurate biodosimetry methods that can be used in a mass casualty incident are needed for immediate triage, medical management, and risk assessments. In their absence, clinical assessments will provide the only basis for initial triage and treatment decisions.
Health Risks from Exposure to Radiation
Health consequences from radiation exposure can include both early consequences in which the severity of the condition is related to exposure (eg, ARS, discussed earlier) and late consequences, particularly radiation-induced cancer, in which the likelihood of occurrence is related to exposure. 45 Following a nuclear detonation or radiation release, many more people would be exposed to relatively low doses of radiation than those who would be exposed to high doses. Therefore, many more people may face an increased lifetime risk of cancer than suffer from ARS.
Radiation Dose
The “dose” of ionizing radiation refers to the amount of energy absorbed by the body that is of sufficient strength to ionize atoms. The phenomenon of ionization distinguishes x-ray and gamma radiation from ultraviolet radiation from the sun, which has sufficient energy to damage skin but cannot ionize the atoms of the body. While many molecules in the body can be ionized by x-rays and gamma rays, damage to DNA leads to mutation, if the cell is not too heavily damaged, or to cell death if the damage is extensive. Cells that die from extensive radiation damage cannot produce cancer. The lowest dose typically received over the course of a year by Americans is about 1 mSv and is primarily from radiation emitted from minerals in the ground. Doses to Americans are close to about 6 mSv, on average, when all sources of natural and background radiation are included as well as the radiation from diagnostic and therapeutic medical care. 46
A dose of 1 Sv over the whole body, if received over a short time (a few minutes or less), is usually considered the minimal single-exposure threshold for ARS. Between the levels of annual dose that everyone receives from daily activities (about 6 mSv) and the levels sufficient to cause ARS (1 Sv or more in a short time) is a wide range in which radiation risk varies according to the dose received and the time over which it is received. In the US and other developed nations, a system of radiation protection regulations limit long-term cancer risk to radiation workers by allowing for annual occupational exposures to be only a few times greater than background radiation. In the US, radiation workers are allowed up to an annual occupational exposure of 50 mSv, or about 8 times the average dose received by Americans.
Radiation Risk after a Nuclear Detonation
Following a nuclear detonation, people receiving less than 1 Sv of radiation would be expected to have few if any acute effects. This would be the largest group of victims and would have a small but real increased risk for future cancers. Cancer is a ubiquitous illness that affects approximately 40% of people in the United States and is fatal to over 20% of the US population (not including nonmelanoma skin cancers). 47 Additional radiation exposure, whether it be from medical radiation or a nuclear incident, will increase a person's lifetime risk of developing cancer, though small increments of radiation impart only a very small additional risk to each person. As an example, exposure to 1 Sv might result in a 5% to 8% incremental increase in the absolute cancer rate.48,49 This means that the individual cancer risk among people exposed to 1 Sv might increase from 40% to about 45% or 48%. Most people who survive a nuclear incident would receive doses much less than 1 Sv. The most common dose of radiation among the A-bomb survivors was 5 to 10 mSv, or about equal to 1 or 2 years of exposure to natural background radiation. A person receiving 10 mSv would have an increased incremental risk of 0.05% to 0.08%. In other words, the cancer risk would go from the approximate background risk of 40% to about 40.05% to 40.08%. The most common increase in risk for people surviving a nuclear detonation will not be large compared to the background cancer risk.
Federal Medical Response Structure and Plans
To facilitate the coordination of efforts by local, state, regional, tribal, and federal resources, a series of documents have been developed to clarify roles and responsibilities. For a broader discussion of the structure and plans, readers are referred to the online handbook. Here we focus on nuclear detonation–specific planning.
Guidance on the nation's approach to conducting response efforts is detailed in the National Response Framework (NRF). 8 The Nuclear/Radiological Incident Annex (NRIA) 15 to the NRF addresses the responsibilities and coordination requirements for releases of radiological material and a nuclear detonation. Agency roles, responsibilities, and authorities are specifically described for each type of incident. Additionally, an integrated concept of operations and unique organization, notification, and activation processes and specialized incident-related actions are discussed.
In the NRIA, HHS responsibilities through Emergency Support Function #8 (ESF #8), public health and medical, include coordination (but not conduct) of long-term population monitoring, certain laboratory analyses, guidance and technical assistance for population decontamination and internal contamination monitoring, provision of medical countermeasures from the SNS, coordination of fatality management, and provision of medical surge. § Responders and planners can use tools developed by HHS and based on the National Response Framework, the National Incident Management System (NIMS), and ESF guidance to navigate through response planning complexities.
ASPR, as the federal lead for medical and public health preparedness and response, and in collaboration with subject matter experts and partner agencies, developed the IND playbook and also a prototype state and local planners' playbook for a nuclear detonation to enhance collaboration and interoperability between federal and nonfederal planners and responders (www.phe.gov). (Note: An HHS all-hazards playbook with specialized information for the specific type of incident, for internal use, is in preparation.)
Medical Playbooks and Ethical Issues
The HHS playbooks are designed to provide a framework for the ESF #8 response and inform senior leadership about response operations that will require complex coordination of numerous entities and their assets in a time-phased manner. The playbooks include sections that focus on a spectrum of anticipated planning requirements and operations:
• Scenario • Concept of operations • Action steps/issues • Pre-scripted mission assignment subtasks • Essential elements of information
The State and Local Planners Playbook for Medical Response to a Nuclear Detonation 50 describes the key principles of the medical and public health response to a nuclear detonation. The playbook is intended to be scalable and customizable based on the specific jurisdiction's capabilities, requirements, and needs, and it will be improved and updated periodically to reflect the most current knowledge, lessons, and changes in capabilities. The action steps section of the playbook is the key section that provides sequential guidance to coordinate the medical response to a nuclear detonation at all levels. It is written in plain language intended to better align the ESF #8 IND playbook and jurisdictional planning methods and capabilities. The section provides detailed time-phased, sector-oriented approaches to response activities with linked references. To use the playbook, planners have the option of downloading an electronic copy of the text itself or using the interactive version online (www.phe.gov).
Involving the Community
Another important aspect of community planning is involving the public in a discussion about difficult ethical issues. The order of triage depends on the medical condition and also on the scarcity of resources, as discussed by Coleman et al. 17 As resources become increasingly scarce, the resource-rich order of “sickest first” may be modified by goals of population-based treatment.51,52 To initiate such discussions and attempts at consensus-building prior to a catastrophic incident, public health officials and disaster response professionals are encouraged to begin a process to develop a body of information about the interests and preferences of various public and specialized medical, religious, and other communities related to use of medical scarce resources. These group discussions can be useful in developing a bank of information, building consensus where possible, and providing immediate direction for local hospitals related to clinician training and distribution of information to the public. (See 2012 Institute of Medicine report for more information about ethical issues involved in resource allocation under conditions of scarcity. 53 )
Communicating About the Possibility of Nuclear Detonation
Community members should engage in discussions about the potential for a nuclear detonation, protective actions to take if a detonation occurs nearby, and things they can do to help other people in the event it takes place away from their home community. To be truly prepared, a community needs to have this discussion before a nuclear detonation and needs a plan for how to communicate with the public following a detonation, including consideration of the possibility that conventional communication capabilities could be compromised.
In the vicinity of a detonation or in the path of fallout, the fear and confusion following a nuclear detonation may lead people to take actions that inadvertently put them in harm's way. Lack of understanding of radiation, its effects, and how it is measured can exacerbate both short- and long-term anxiety. Communicating clear and effective messages is challenging but critical to reducing panic and saving lives. Pre-scripted messages, expert spokespersons, credible experts, multiple message dissemination methods, and rapid restoration of communications infrastructure can all contribute to timely and effective communication.
People will be affected in different ways and thus will have different information needs associated with proximity to the blast and fallout plume:
• Blast Damage and Dangerous Fallout (DF) Zones: People in these areas need life-saving information. Anyone who might be in the path of the radioactive plume must quickly get inside and stay inside to avoid a potentially fatal dose of radiation. Shelter orders may have to be issued broadly during the initial period of uncertainty and refined as information about the plume is gathered and its specific implications determined. • Surrounding Area: People in this area will be concerned for their immediate health and safety and will want to know what they should do. People in the surrounding area will also have concerns about contaminated people and vehicles entering their communities, and they must understand the relative risk from incidental contamination to prevent potential obstruction of entry or evacuation movement. These communities will also serve as reception communities for evacuees. • National and International Communities: People in other parts of the nation and across the world will be seeking information and trying to get in touch with loved ones who may be in affected areas. Concern will exist about a possible second attack. This is an opportunity to provide situation and response updates and to educate the population about appropriate safety measures, as well as to address concerns about health and other risks perceived by people outside the affected areas.
Communicating About Protective Actions and Radiation
Messages prepared, tested, and practiced in advance are fundamental to conveying clear, consistent information and instructions during an emergency. Many of the questions the public will have after a nuclear detonation can be anticipated, and answers can be prepared in advance. Education in advance can provide even greater leverage on a community's preparedness, ability to respond effectively, and resilience; school and community education programs should be considered.
When anticipating questions, planners must keep in mind both the broad audiences as well as audiences with special communication needs—for example, non–English speakers, hospital and nursing home staff and patients, the homeless population, and people who are hearing impaired. To some extent, each community will have specialized information needs; messages need to be tailored to meet those needs.
In a nuclear incident, first and foremost, people will be concerned with protecting themselves and their families. Protective action messages should provide simple, direct instruction to people in the affected areas about how to do this. Audience research provides the following recommendations for messages:
54
• Write short, concise, simple messages. • Use directive, authoritative language. • Provide prioritized instructions and directions in each message. • Provide information for a variety of environments. • Encourage people not to leave their homes to check on loved ones in schools, daycare centers, and elder-care facilities until an ability to do so without inadvisable radiation exposure is clear. • Avoid or define unknown terms and phrases.
Figure 10 illustrates an immediate lifesaving message.
Example of an Immediate Lifesaving Message
Communications Infrastructure
A significant concern following a nuclear detonation incident will be the integrity of the communications infrastructure. How will officials communicate messages to affected audiences? The difficulty that will inevitably follow a nuclear detonation drives home the importance of pre-incident preparedness. Officials anticipate the infrastructure issues discussed below. 1
Blast Damage Area
In the physically damaged areas (see Figure 1), there would be minimal, if any, ability to send or receive communications. The blast would cause physical damage to electrical, telephone, and cellular systems. An electromagnetic pulse (EMP) would damage electronics in the physically damaged area including televisions, computers, and cell phones. Some cell phones in the blast area could possibly survive the EMP if they were sufficiently sheltered underground, and this might also imply that the phone might be in the possession of a survivor; however, the deep shelter may itself block cellular reception. Communications capabilities may take days to be reestablished.
Along with commercial systems, public safety systems (eg, land and mobile radio and 911 call centers) may also suffer communications failures. Although these systems are typically more robust and less susceptible to failure than their commercial counterparts, they can be expected to be severely damaged or degraded in the immediate blast area and somewhat in the surrounding areas. These systems are critical to emergency responders in performance of life-saving and rescue operations; they need to be restored as quickly as possible and redundancies identified and employed if these centers or major 911-switching locations are directly affected.
As part of the federal response to a major disaster, FEMA will activate the Communications Annex of the NRF, ESF #2, to coordinate with the private sector, state, and local entities in restoring the commercial communications infrastructure and public safety and emergency responder networks. 8 Industry continually monitors its own networks for outages and reduced capabilities and will usually begin recovery operations quickly. Commercial providers typically have transportable restoration capabilities (eg, cellular on wheels) strategically located around the country to minimize response times. With proper planning, public safety and emergency responder networks can be augmented and/or temporarily restored by using assets that the state, national guard, and surrounding localities may be able to provide. FEMA can typically have communications assets on the ground in the contiguous 48 states within 24 to 48 hours after an incident.
Surrounding Area
The surrounding area may include surrounding communities or counties, bordering states, and people in the path of the radioactive plume, including the dangerous fallout zone and the radiation caution zone. The EMP should have limited, if any, direct effect on electronic devices in the surrounding area outside of the blast damage zone, regardless of radiation. Electronic devices may only require resetting switches and circuit breakers. However, the potential exists for cascading effects caused by EMP along transmission lines, including large-area power outages. An important audience in the surrounding areas for communications will be communities receiving evacuees. Although these areas may not have significant infrastructure issues, connectivity will be essential for these communities to coordinate reception for potentially thousands of evacuees.
National and International Communities
For any major national emergency, a sudden increase in the need for information and human connectivity severely stresses and sometimes exceeds the capacity of the communications infrastructure. This stress will hinder the ability to communicate into or out of the physically damaged areas, the regional area that will be affected by the dangerous fallout, and potentially other areas in the vicinity. Planners must know what types of systems are available to enable responder communications in case normal communications methods are unavailable.
Communication Channels
Following a nuclear denotation, every available outlet must be used to gather information about the health and safety issues that the community and responders face, to provide health and safety guidance to affected populations, and to address health, economic, safety, and other concerns of people across the country and throughout the world. Information outlets include electronic billboards, 911 systems, short-wave radio, siren warning systems, radio, television, newspapers, flyers, public announcement (PA) systems, text messages, and social media and other websites. Planners must consider the allocation of resources to supply information to these outlets and which outlets to use to gather information for situational awareness.
Radio broadcasts may be the most effective means to reach people closest to the nuclear explosion in areas without physical damage that would have destroyed belongings such as radios. The Emergency Alert System, National Oceanic and Atmospheric Administration (NOAA) weather radio broadcasts, reverse 911 systems, flyers, public address systems, short-wave radios, and siren warning systems may be useful in rapid dissemination of emergency information in the affected area. Although additional outlets, particularly electronic outlets, are more likely to be useful away from the blast site, these outlets should be considered in emergency communications plans. Effectively using social media will also be essential.
Educating Responders and Planners
High-impact radiation emergencies are receiving increasing attention from the leadership of the medical planning and healthcare response communities. 55 However, radiation-specific training has lagged behind that for other types of emergencies in the wider response community.
Responders and planners need to acquire and maintain radiation-specific knowledge and skills over and above what they know from “all-hazard” emergency training, including the following topics:
• The basics of radiation physics,
56
especially the differences between contamination and exposure;
57
• The types of mass-casualty radiation incidents that could occur;
58
• The basics of radiation medicine, especially radiation triage and how to diagnose and manage exposure and contamination;
59
• Special skills for managing public health, medical response venues, radiation survey equipment, logistics, decontamination, and waste during the various kinds of radiation emergencies; • How responses to “small” and “large” incidents differ; and • Public communication.
Radiation knowledge gaps among responders and planners have complicated the development of regulation-compliant, implementable, and integrated local, regional, state, and hospital radiation emergency plans. The statutes and regulations that govern federal, state, and local authorities and responsibilities during such incidents are complicated. 60 Moreover, few emergency or healthcare personnel have ever responded to any type of radiation mass-casualty emergency. Education and training can fill this knowledge gap, using both traditional (ie, face-to-face, synchronous classroom learning) and nontraditional (ie, online/electronic) means, as well as exercises where feasible.
Classroom courses are currently available from many local, state, and federal agencies,61,62 as well as professional societies, educational institutions, hospitals, and occupational associations. Resource materials for these courses are usually vetted by the offering agency, professional society, or government agency. These courses teach basic concepts, along with practical skills like proper selection and use of radiation survey equipment, personal protective equipment, and personal dosimeters; and how to work in teams, especially within the incident command system (ICS) 63 and hospital incident command system (HICS). 64
Strategies to increase the availability and effectiveness of radiation-specific education include having government agencies and professional organizations couple traditional learning with required recertification. Medical credentialing entities can formally present this material during initial training and include questions about radiation emergencies in certification exams. These are detailed in the manual. HHS has at least 3 web portals that are helpful for both healthcare planners and responders for radiation emergencies:
• Radiation Emergency Medical Management (REMM)—primarily for healthcare providers and planners (http://www.remm.nlm.gov/); • CDC/Radiation Emergencies—focusing on public health issues (http://emergency.cdc.gov/radiation/); and • ASPR/Public Health Emergencies—focusing on all-hazard preparedness and responses as well as specific hazards (http://www.phe.gov/preparedness/pages/default.aspx).
The REMM website provides extensive links to vetted resource materials from a variety of government and nongovernment sources, including the peer-reviewed medical literature. Many other entities have useful information as well.
Increasingly, mobile platforms on smartphones and tablet devices are being used for planning and response. Future developments may also include the ability to create and implement health records using field devices like these, along with applications that can help with triage. Although the response to radiation emergency mass-casualty incidents is complex, new and efficient ways are available to assist the responder and planning communities.
International Agencies and Networks
In the wake of the radiation release from the damaged Fukushima nuclear power plant complex in March 2011, the US provided consultation to the American embassy and to Japan. Concerns about radiation levels in the US illustrated that any atmospheric release of radiation can become an international issue because of the presence of sensitive radiation detectors worldwide that monitor for potential nuclear testing and can detect very low levels of radiation above background. The lowest levels of radiation that can be detected are well below the amount that requires any protective actions; however, given the fear of radiation, when radiation is detected it often requires investigation, explanation, and public education.
The World Health Organization (WHO) and International Atomic Energy Agency (IAEA), both under the United Nations (UN), develop recommendations for planning and preparedness and assist with networks that have expertise and laboratory capability for biodosimetry (REMPAN) and medical response (RANET). Individual countries set their own protective action guidelines (projected doses used to limit exposure to workers and the public) based on expertise from professional societies such as the National Council for Radiation Protection (NCRP) and the International Commission on Radiological Protection (ICRP). While all the guidelines are scientifically based, minor differences in dose and in radiation units used can lead to confusion. For international response, the US has the United States Agency for International Development (USAID) Disaster Assistance Response Team (DART) and the Radiation Emergency Assistance Center/Training Site (REAC/TS) from DoE, as well as experts from other federal agencies including HHS, DoD, and the Nuclear Regulatory Commission (NRC). Ideally, data-sharing among the various groups will facilitate a coordinated response. However, initial uncertainties from limited data early on and minor differences in protective action guidelines among nations may lead to speculation and confusion. The communications and nuclear experts must avoid or actively address these problems to prevent them from interfering with effective communication and response.
International Atomic Energy Agency
The prime objectives of the IAEA's Response System are to facilitate the exchange of official real-time information among states (countries) and relevant international organizations; to provide assistance and advice to states or relevant international organizations on request; and to provide relevant, timely, truthful, consistent, and appropriate public information.
Emergency Notification and Assistance Technical Operations Manual (ENATOM)
ENATOM 65 defines the roles and responsibilities of IAEA, the state parties, and the IAEA member states regarding preparation and response to nuclear accidents and radiological emergencies. The IAEA maintains an Incident and Emergency Centre (IEC) that fulfills the functions that are placed on the IAEA by the conventions and by relevant safety standards and decisions of the policy-making organizations.
IAEA's Response and Assistance Network (RANET)
RANET 66 is a network of states capable and willing, on request, to rapidly deploy trained, equipped, and qualified personnel to nuclear or radiological incidents and emergencies. RANET's major objectives are to strengthen IAEA's ability to provide assistance and advice, to coordinate the provision of assistance as specified in the framework of the assistance convention, and to promote emergency preparedness and response capabilities for nuclear or radiological emergencies or incidents among IAEA member states. In the US, REAC/TS is currently the only deployable response team that supports RANET.
World Health Organization
WHO works closely with IAEA to prepare for and respond to nuclear accidents and radiological emergencies—principally to provide, coordinate, and consult on medical assistance to victims of incidents involving severe radiation exposure. WHO can also advise national authorities on how to prepare for and respond to such radiation accidents and offer advice on what kind of public health actions may be needed.
WHO's Radiation Emergency Medical Preparedness and Assistance Network (REMPAN)
Emergency medical support for radiation-exposed individuals is provided through WHO's REMPAN, 67 a network of 40 medical and research institutions designated to provide emergency medical and public health assistance to people overexposed to radiation. It also facilitates long-term care and follow-up of radiation accident victims and conducts research in radiation emergency medicine, radiotherapeutics, biodosimetry, and radiation epidemiology. REMPAN is activated following notification from IAEA or directly to WHO of a radiation accident with casualties (even in the case of a single victim with severe exposure).68,69 REMPAN's objectives are to promote medical preparedness for radiation emergencies among WHO member states; to provide medical and public health advice and assistance and coordination of medical management at international and regional levels in nuclear or radiological emergencies; and to assist in follow-up studies and rehabilitation.
Assistance provided by REMPAN in radiation emergencies may include the following resources:
• Human resources specialists: Specialists in radiation medicine, health physics, radiology, hematology, and other appropriate specialties (eg, burns), as well as skilled nurses and technicians • Equipment: In most centers, substantial resources to provide special medical assistance to overexposed people, including portable equipment for radiation monitoring • Medical services: Assistance for the diagnosis, prognosis, medical treatment, and medical follow-up of people affected by radiation • Scientific services: Expertise to assess radiation doses to exposed people (most of the REMPAN institutions have biodosimetry laboratories) • Transportation: Advice on the transportation of affected people • Specialized teams: Capability for WHO to organize multinational teams to render medical assistance onsite
WHO BioDoseNet
WHO's BioDoseNet70,71 is a global network of biodosimetry laboratories whose role is to support management and decision making in cases of large radiation emergency incidents in which the capability of an individual laboratory is likely to be overwhelmed. In preparing for such incidents, BioDoseNet focuses on harmonization of methodology, quality assurance, knowledge sharing, and laboratory intercomparison exercises.
International Assistance Provided by the United States
Radiation Emergency Assistance Center/Training Site (REAC/TS)
REAC/TS, 62 operated by Oak Ridge Institute for Science and Education (ORISE), provides assistance regarding medical and health physics problems associated with radiation accidents in local, national, and international incidents. Through a team of leading experts in emergency management and radiation incident response, REAC/TS provides training and consultation to its clients, such as DoE and CDC, and is recognized as the leader in the management of medical accidents involving radiation, both nationally and internationally. REAC/TS can provide the following resources:
24/7 Availability
A radiological emergency response team consisting of physicians, nurses, health physicists, and coordination and necessary support personnel is on 24-hour call to provide first-line responders with consultative or direct medical and radiological assistance at the REAC/TS facility or at the incident site. The team has expertise in and is equipped to conduct:
• Medical and radiological triage; • Decontamination procedures and therapies for external contamination and internally deposited radionuclides; • Diagnostic and prognostic assessments of radiation-induced injuries; • Treatment for internalized radionuclides, including DTPA and chelation therapy; • Radiation dose estimates by methods that include cytogenic analysis, bioassay, and in vivo counting.
Training
The REAC/TS facility serves not only as a treatment facility, but also as a central training and demonstration unit at which US and foreign health personnel receive training in medical management for radiation accidents. The following courses are among those available:
• Pre-Hospital Radiation Emergency Preparedness (PREP) • Radiation Emergency Medicine (REM) • Health Physics in Radiation Emergencies (HPREM)
Advanced Radiation Medicine (ARM) International Response
REAC/TS participates with the international community via its designation as a WHO collaborating center of REMPAN and IAEA RANET. REAC/TS is prepared to perform the following functions:
• Serve as a focal point for advice and possible medical care in cases of human radiation injury; • Facilitate the progressive establishment of a network of equipment and specialized staff in human radiopathology; • Assist in the establishment of medical emergency plans to respond to large-scale radiation accidents; • Develop and carry out coordinated studies on human radiopathology and epidemiologic studies that may be appropriate; • Assist in the preparation of relevant documents and guidelines; and • Provide direct or consultative services to foreign governments at the request of WHO or IAEA in the case of an actual radiation incident.
USAID, Office of the US Foreign Disaster Assistance, Disaster Assistance Response Team
OFDA (Office of the US Foreign Disaster Assistance) is the office in USAID responsible for facilitating and coordinating US government emergency assistance overseas. 72 OFDA deploys Disaster Assistance Response Teams (DARTs) in response to all types of disasters in which lives or livelihoods are threatened. These teams are assembled as needed and include a range of experts, depending on the situation, including representatives from federal, state, and local governments, as well as members of the private sector. For example, in response to the nuclear accident in Japan, OFDA deployed a DART consisting of urban search and rescue teams and technical experts in nuclear issues from across the US government.
Global Health Security Initiative
The Global Health Security Initiative (GHSI)
73
is an informal international partnership among countries to strengthen public health preparedness and response to threats of CBRN terrorism and pandemic influenza globally. This initiative was launched in November 2001 by Canada, the European Union, France, Germany, Italy, Japan, Mexico, the United Kingdom, and the United States. WHO serves as an expert advisor to GHSI. Technical and policy subject matter experts participate in the following working groups around specific areas of expertise:
• Risk Management and Communications Working Group • Pandemic Influenza Working Group • Chemical Events Working Group • Radiological-Nuclear Threats Working Group • Communicators Network • Laboratory Network
Members of the Radiological-Nuclear Threats Working Group (RNWG) meet regularly in person or via teleconference to share information on public health preparedness for radiological and nuclear threats in their countries or organization. HHS expertise on radiological and nuclear response is available from ASPR, NIH, and CDC, whose experts will assist in international incidents by providing advice and deployment, if requested.
Conclusion
Whether a radiological or nuclear incident occurs domestically or abroad, the United States must be prepared to assist in planning and response. Although many of the authors of this article and the manual have played, and continue to play, major roles in distilling major scientific lessons and participating in responses to save lives in the event of a nuclear or radiological emergency, many challenges remain. Maintaining adequate radiological-nuclear expertise capable of meeting these challenges in the future is key. The manual (http://www.phe.gov/nuclearresponsemanual) aims to facilitate preparedness and response by offering key principles and practices in a concise format that links to more detailed information.
Footnotes
Acknowledgments
Editing was provided by C. Norman Coleman, Eric Toner, Ann Norwood, and Judith Bader, with editorial assistance from Kendra May, Alicia Livinski, and Paula Murrain-Hill. M. Carol McCurley assisted with the section on communication.
Author Affiliations
National Institutes of Health, Bethesda, MD
Office of the Assistant Secretary for Preparedness and Response (ASPR), Washington, DC
Centers for Disease Control and Prevention, Atlanta, Georgia
Other Federal Affiliations
Non-Federal Affiliations
Key Acronyms
*
Note: milliRoentgens per hour (mR/h) is a measure of exposure to radiation in air. The international system has no equivalent simple unit (it would be Columbs per kilogram per hour, where 1 mR/h=2.58×107 C/kg/h). The unit of “air exposure” is widely used because it can be measured by relatively simple instruments. Instruments that provide a readout in the international system would likely use mSv/h, where 1 nR/hr is approximately equal to 0.01 mSv/h.
†
This term should not be confused with “dual-use,” which refers to research that can be used for nefarious purposes as well as beneficial ones.
‡
These would need to be nontoxic to not adversely affect responders; none are presently available other than for radiotherapy for oncology.
§
HHS has resources to enhance state and local medical responders, but they are limited. Other agencies can provide assets such as the Department of Veterans Affairs (Medical Emergency Radiological Response Team) and the Department of Energy (Radiological Assistance Program and Radiation Emergency Assistance Center and Training Site).