
Abstract
Zoonotic pathogens have caused the majority of emerging infectious disease events in the past 6 decades. With most emerging infectious diseases arising from animal origins, including many of the select agents identified as most likely candidates for bioterrorism, linking human and animal surveillance systems will be critical to effective disease identification and control in the future. Lack of this linkage has been the focus of a number of important policy papers in recent years. These have expressed concern over the continued lack of preparedness for addressing zoonotic threats and have called for a new approach to integrating biosurveillance. However, these studies have been mainly Western-centric in viewpoint and have overlooked the example of the Russian Federation (RF) Anti-Plague System (AP system). In this article we submit that the RF AP system has select components that effectively address recent concerns and inform the US and UK intersectoral efforts on human-animal health surveillance, forming a basis for US, UK, and RF collaboration.
Most emerging infectious disease events in the past 6 decades have been caused by zoonotic pathogens. Thus, linking human and animal surveillance systems is critical to effective disease identification and control. Recent studies that have expressed concern over the failure to address zoonotic threats have called for a new approach to integrating biosurveillance. But these studies have been mainly Western-centric in viewpoint and have overlooked the example of the Russian Federation's Anti-Plague System. This article describes that system's approach to human-animal health surveillance.
Inability to detect and respond quickly to emerging zoonoses can be costly both from a fiscal and a human-animal health perspective. A 2009 IOM committee found that a needed investment of $800 million pales in contrast to the economic losses from emerging, highly contagious zoonotic diseases that have exceeded $200 billion over the past decade. 7
Recognition of current limitations has prompted investment into novel surveillance systems. Google.org's Predict and Prevent Initiative has provided millions of dollars in support of efforts to identify hot spots where diseases may emerge, detect new pathogens circulating in animal and human populations, and respond to outbreaks before they become global crises. 8
What few realize is that what is viewed as new and innovative by the West has been practiced in the Russian Federation (RF) for more than 100 years. Faced with serious zoonotic threats at the turn of the century, the Russians created a unique, integrated, ecologically based zoonotic disease surveillance system known as the Anti-Plague System (AP system). While this system has been evaluated from a proliferation threat perspective, 9 its epidemiologic power has not been fully appreciated by the public health community. As the world struggles to meet the challenge of emerging zoonoses, it is worth looking at a system that has served the RF for many years. Recommendations found in recent policy papers are already in place in the RF.
In this article we address several questions:
• Why was the AP system originally created as an integrated human-animal surveillance system for zoonotic threats? • How did this innovative approach sustain itself during 100 years of tremendous technological, scientific, political, economic, and social change? • How did the AP system operate historically, and how does it operate now? • What lessons can be learned from the RF by those now attempting to create integrated surveillance systems in the Western world and in developing countries?
Background
The Nuclear Threat Initiative (NTI) previously funded research on the AP system in Central Asia. Recognizing that the Soviet Union historically had a unique approach to zoonotic threats that might inform current Western efforts, NTI engaged with experts from the animal and human health systems in Russia, Kazakhstan, the UK, and the US to determine the status of current national infectious disease surveillance systems and provide recommendations for high-level engagement of Russian and US experts aimed at improving integration between human and animal health. This project was implemented in cooperation with experts from the international disease control and related communities. NTI hosted an experts workshop in Moscow in June 2009 to discuss their respective approaches to the human-animal interface. The following is an analysis of the RF approach to zoonotic threat detection and response.
Russian Federation System for Epidemiologic Surveillance
The RF has a 3-level system of epidemiologic surveillance and control for especially dangerous infectious disease at the federal, subfederal, and regional levels (Figure 1). Two main entities control and supervise veterinary and public health: (1) Rosselkhoznadzor, which reports to the Ministry of Agriculture (MoA), and (2) the Federal Service for Surveillance in Consumer Rights Protection and Welfare (FSSCRPW), or Rospotrebnadzor (also formerly known as Sanitary and Epidemiologic Service [SES]), which reported to the Ministry of Health (MoH) until 2012 and directly to the government of the Russian Federation since 2012.10-17
FSSCRPW (Rospotrebnadzor) consists of a network of former SES facilities, with centers in cities or regions, and special federal entities including 1 Anti-Plague Center, 5 scientific and research Anti-Plague Institutes, and several Anti-Plague stations (APS) located throughout the country. In general, the SES system deals with many traditional public health functions, while the specialized Anti-Plague system's main responsibilities have to do with preventing outbreaks caused by especially dangerous pathogens (EDP), including outbreaks of zoonotic infections 18 (Figure 2). What is unique about the RF AP system is that a single agency has jurisdiction over humans and animals in regards to zoonotic threats.
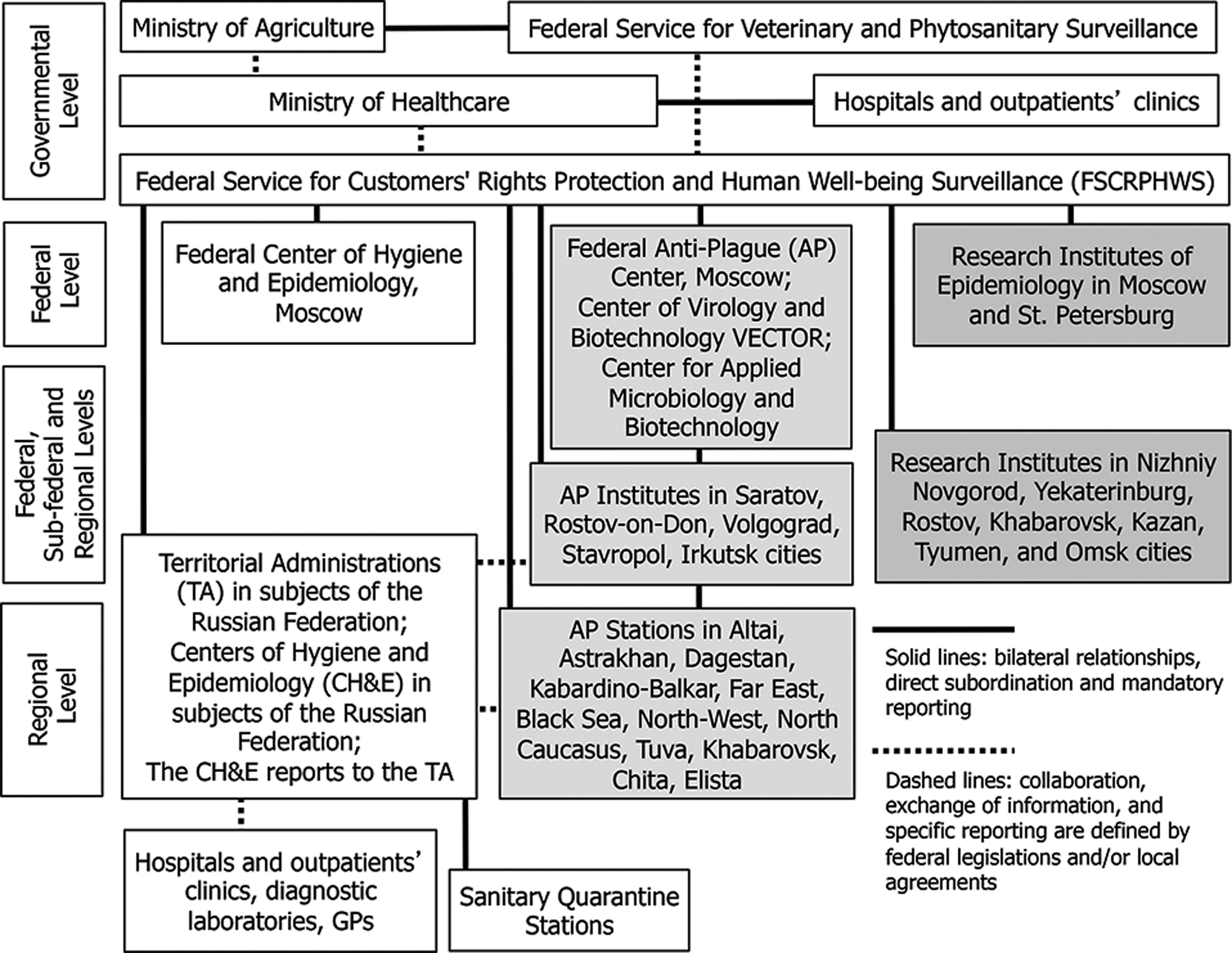
Structure of Russian Federal Service for Customers' Rights Protection and Human Well-being Surveillance Including Anti-Plague System. Russian government consists of 21 ministries and 20 federal services and agencies including at the “government level” Federal Service for Customers' Rights Protection and Human Well-being Surveillance (FSCRPHWS). Its institutions serve the whole country and constitute the federal level of management, whereas at the subfederal level there are the institutions that serve large parts of Russia. The regional level means the level of so-called subjects of the Russian Federation, called Republic, Krai, Oblast, or Autonomous Okrug. Currently there are 83 subjects of the Russian Federation.
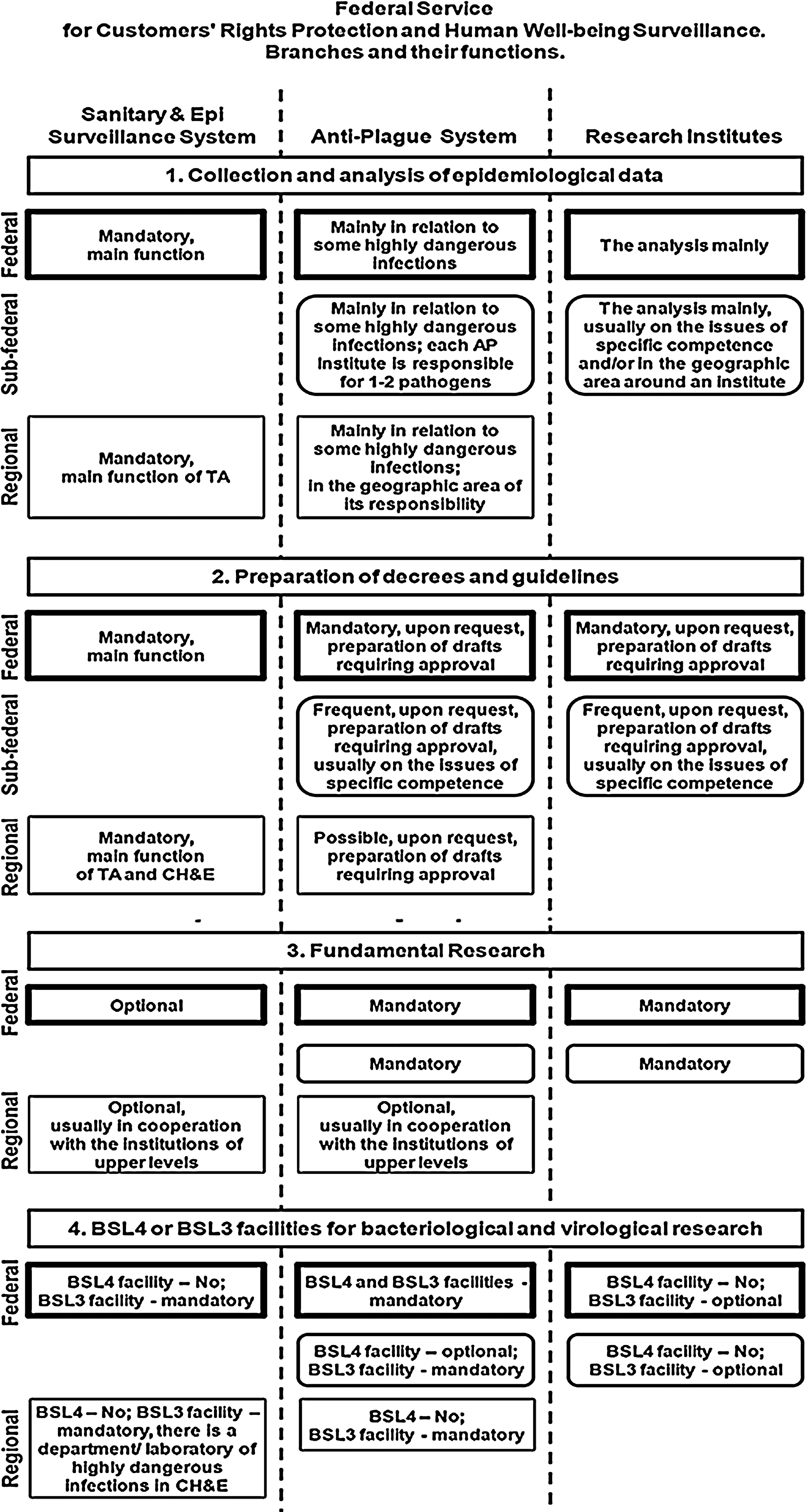
Functions of Federal Service for Customers' Rights Protection and Human Well-being Surveillance. Among the 3 major branches, 1 deals mainly with routine sanitary and epidemiologic surveillance and control (left); the research institutes are charged mainly with academic science (right), whereas the AP system involves both in practical investigation and control of extremely dangerous diseases and the fundamental studies of these infections.
The AP system evolved as a result of the considerable historical threat posed to public health by plague (Yersinia pestis). In the beginning, the main focus of the AP system was on plague, but today it covers many viral and bacterial agents such as tularemia, brucellosis, and cholera.
Unlike the West, where human, animal, and environmental health activities are the responsibility of separate agencies, the investigation and control of diseases in all 3 domains have been mandatory for the AP system since its creation. Russian federal law mandates that the AP system have authority over any activity “related to shedding of pathogenic microorganisms by humans, animals or by the environment, detection and treatment of people displaying symptoms of infectious diseases, as well as scientific, educational and productive activities involving use of agents of infection.” 19 (p2)
The AP system has always had an environmental focus on the study of zoonoses, and its work has involved obtaining samples from the environment, wild rodents, and birds. On an annual basis, the AP system collects approximately 50,000 animal samples (mainly rodents), 100,000 ticks and mosquitoes, and 10,000 water samples. Roughly 10,000 to 20,000 virological investigations and up to 100,000 microbiological investigations are performed. The AP system represents a rare example of systematic, sustained, well-supported, integrated biosurveillance for zoonotic threats. No parallel exists in the West.
History of the Anti-Plague System
The AP system was created by Czar Nicholas II in the 1890s to respond to numerous outbreaks of plague. Czarist Russia and the former USSR had 43 “natural foci” of plague covering 550 million acres of land.9,20,21 From the turn of the century to 1925, more than 177 outbreaks occurred affecting 2,105 people.
In response, anti-plague institutions were organized in Russia from 1898 to 1915. These included the State Commission for Prevention and Control of Plague Infection, 2 research laboratories in St. Petersburg and Kronstadt City, 10 regional anti-plague laboratories, and 45 regional anti-plague stations in areas of plague activity.
In 1921 another outbreak in the Russian Far East prompted the creation of special anti-plague trains. These trains consisted of 8 to 11 cars with a kitchen, a storeroom, a pharmacy, a laboratory, an isolation ward, an observation ward, a disinfection chamber, and cars for staff, quarantine guards, and the deceased. The staff of the train included 2 doctors, 4 medical assistants, a disinfection specialist, 10 nurses, 6 quarantine guards, and a conductor. The trains examined the populace in high-risk areas, removed suspected cases of plague and placed them in an isolation ward, and later moved them to a secured quarantine site. 22 This work is an extraordinary example of field epidemiology at its best. The anti-plague train-laboratory was a historical prototype of modern day mobile response teams known as SAETs (sanitary and anti-epidemic teams).
After the revolution, the Regional Institute of Microbiology and Epidemiology was organized in Saratov City (in the Volga region). The main tasks of the institute included plague surveillance and prevention, field studies of zoonotic cases, and development and manufacturing of laboratory tests and therapeutic and prophylactic vaccines and sera. This institute is now known as “Microbe” and is the core of the Russian anti-plague system. It serves as a reference center for plague and other dangerous zoonotic infections.
In 1924, AP specialists shifted from response to prevention of zoonotic outbreaks. Fourteen field epidemiology teams were created to inspect the steppes and deserts to detect epizootic outbreaks. 8 From 1926 to 1940, the majority of plague epidemics and epizootics were in the European part of the USSR, particularly in the Caspian steppe, where 151 outbreaks affecting 592 people were recorded. The Soviet AP system was established from 1929 to 1935 to address the situation. Structural and legislative work was finished in 1939, when the statutes and instructions for anti-plague institutions governed by the Soviet ministry of health were issued.
The total eradication of rodent reservoir hosts and vectors of plague, the tarbagan (Marmota sibirica) and the little souslik (Citellus pygmaeus), was started in the mid-1930s. Anti-plague stations in endemic areas investigated rodent populations every year. If the infection rate increased, the eradication measures were intensified. Teams were sent into the field twice a year to monitor and obtain baseline information on rodent and flea populations and to systematically map natural foci of plague, a formidable accomplishment of the AP system (see Figure S1, supplementary material, at www.liebertonline.com/bsp).11,23
Both in czarist Russia and in the early years of the USSR, the integrated approach to zoonoses was to some extent forced by the limited number of trained specialists in a large country. By necessity, the small workforce needed to work with both human and animal threats. However, there was also a firm scientific basis for such an approach. In 1939, Evgeny Pavlovsky, the father of Russian epidemiology, introduced his concept of “natural nidality of disease.”24-27
“According to Pavlovsky, ‘nidus’ is a translation of the root word ‘ochag,’ meaning a hearth. Thus a nidus of disease is its nest, home, or habitat (equivalent to the Latin ‘focus’).”
28
(p913) He pointed out that certain diseases occur naturally in wildlife and are transmitted from wildlife to humans by insect, tick, or mite vectors when humans intrude on their territory. Later, he showed that the type of disease present could often be predicted from the type of landscape. His nidality concept, which is just being rediscovered by the West, “led to the emergence of the contemporary science of landscape epidemiology.”
27
(p462) The theory behind landscape epidemiology is that
knowing the vegetation and geologic conditions necessary for the maintenance of specific pathogens in nature, one can use the landscape to identify the spatial and temporal distribution of disease risk. Key environmental elements, including elevation, temperature, rainfall and humidity, influence the presence, development, activity, and longevity of pathogens, vectors, zoonotic reservoirs of infection, and their interactions with humans.
29
This is the type of environmental information that was and is routinely collected by the AP system. The science-based, integrated approach of the AP system to diseases at the human-animal-ecosystem interface is one only now being explored by the West, which is attempting to predict emerging zoonoses in hot spots of disease activity. Pavlovsky's nidality of disease concept, which looked at wildlife vectors and the ecosystem as a means of predicting infectious disease outbreaks, was written 74 years ago, but the approach is as fresh and applicable today as it was then.
When the Communist party came into power, it decided to keep and enhance the AP system. In the 1940s, new endemic areas were found as anti-plague institutes and stations grew and expanded their surveillance of hosts and added serology to classic bacteriologic methods. In the late 1950s, special commissions on plague were established. These studied “known natural plague foci and investigated whether other unknown foci existed in the USSR.” 30 (p52) The research agenda of these commissions included “studies of hosts and vectors that carried and transmitted plague bacteria, diseases that afflicted the plague hosts, and decontamination methods. To accomplish this ambitious research agenda, numerous regional and field AP stations were set up in regions in which natural plague foci existed.” 30 (p52)
In 1966 the plague enzootics appeared again in the trans-Baikal region and later in the Caspian steppe (in 1972). At that time the system was primarily engaged in defending the country against endemic and exotic diseases.
By the late 1970s, the system was enlisted in a biological warfare program and was composed of 87 facilities engaged in disease surveillance, research, production and testing of vaccines and laboratory equipment, and training of civilian and military personnel. Most important, the AP system stretched beyond Russian borders into Central Asia, the Caucasus, Ukraine, and Moldova, with facilities strategically located in 11 republics.
31
In its heyday, before the collapse of the Soviet Union, the AP System employed 14,000 people including 7,000 scientists whose expertise broadened beyond plague to other endemic zoonotic diseases, such as anthrax, brucellosis, tularemia and Crimean-Congo hemorrhagic fever. They had a formidable workforce capable of both surveillance and response to zoonotic threats.
18
From 1990 to 2009, most changes related to the new techniques for EDP diagnostics and investigation of the evolution of the organisms, but the ruling principles and organizational structure of the AP system were kept in the post-Soviet Russian Federation.
Today, there are 12 anti-plague stations in the Russian Federation, as well as 5 anti-plague research institutes, most of which are found in plague-endemic areas or regions connected with plague-endemic areas. The AP system is governed by the Federal AP Center in Moscow. Institutes are designated as reference centers, meaning that they handle the state collection of strains, do their final identification, and develop and supervise procedures. Although they can work with any EDP, institutes will usually specialize in a pathogen—for example, Saratov for plague and Stavropol for Crimean-Congo hemorrhagic fever. Sanitary regulations stipulate safety procedures for handling EDP and procedures for record keeping and storage, transfer, and transportation of microorganisms. 19 There are also roughly 60 anti-plague facilities in Central Asia and the Caucasus, where the largest and most active natural disease foci are concentrated. Because of post-Soviet difficulties, there were human cases in neighboring countries (Kazakhstan, Uzbekistan) and an increase in epizootics in these countries. The danger of importation of plague from Central Asia, Mongolia, and China still exists.
Strengths of the Anti-Plague System
Education and Training
The AP system has addressed some of the concerns of the IOM report on implementation of joint human and animal health field epidemiology training programs and multisectoral coordination and communication in producing a workforce capable of carrying out zoonotic surveillance.7,9 The AP system has a long tradition of training medical and paraprofessional staff (biologists) in the recognition, handling, and response to zoonotic pathogens. 32 Beginning in the 1940s, all AP employees received training in a 6-month specialization course at the Microbe Institute.9,18
The head of FSSCRPW approves the programs for training specialists in IHR (2005) and sanitary protection of the Russian Federation territory. The mandatory sanitary and anti-epidemic team personnel training includes baseline specialization and regular advanced training at the Microbe and Stavropol AP Institutes, as well as annual seminars and workshops at their institutes. 32 Annually 500 to 1,000 people receive formal training and are certified. Another 1,000 to 1,500 specialists attend lectures. A strength of this training is that it includes not only the epidemiologic investigation and diagnostics of human disease outbreaks but also the investigation of emergent situations in domestic animals and wildlife if these zoonoses pose a threat to public health.
Structured Reporting Framework
The RF health system has a very well-defined and timely reporting hierarchy for suspect zoonotic threat cases. This is supported by the federal legislation that regulates the reporting timeline in case of an epidemiologic emergency. 33 According to the legislation, any medical facility that sees a suspect case of an EDP must send an emergency special report to the local Sanitary and Epidemiologic Services office within 2 hours (Figure 3). The regional Rospotrebnadzor authority must report the emergency to the federal Rospotrebnadzor office within 24 hours. Decisions for response beyond the regional level, such as deployment of mobile sanitary and anti-epidemic teams, are made at the federal level by Rospotrebnadzor. 34 Detection of unknown infectious diseases is viewed as an emergency and requires urgent transfer of information to the federal level in the form of 2 consecutive messages: a preliminary one, provided urgently within 24 hours, and a final report within 15 days after an emergency situation is restored to normal.19,33,35,36
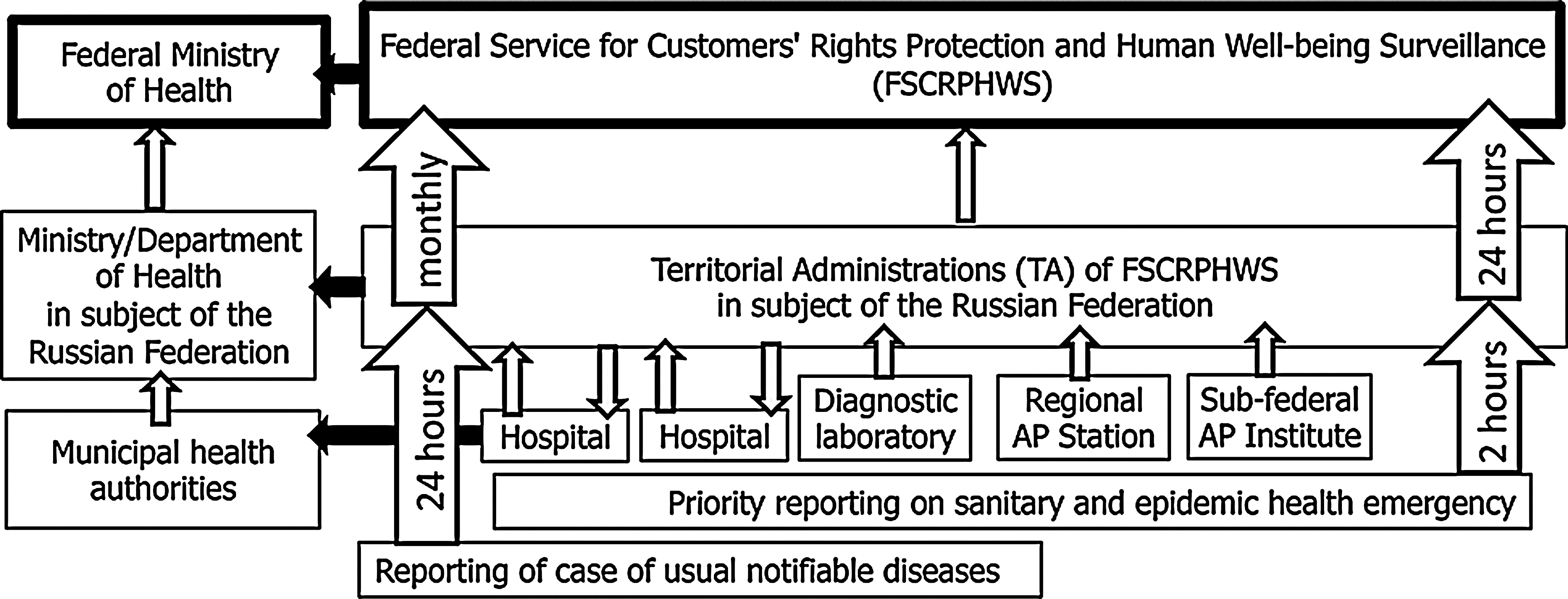
The Timing and Flow of Clinical Case Reporting in the Russian Federation. This scheme and timing is mandatory for all medical and epidemiologic facilities according to Russian legislation.
There is a single reportable disease list. Different diseases have different triggers for reporting. For example, every case of plague, SARS, West Nile fever, Crimean-Congo hemorrhagic fever, rabies, anthrax, typhus, and legionellosis must be reported, whereas every 3 cases of brucellosis are reportable. 33
Biological agents of greatest pathogenicity are classified as Groups I or II. Other microorganisms are in Groups III and IV. 19 Samples taken by physicians from suspect reportable disease cases are sent by courier from the local hospital to the nearest Center of Hygiene and Epidemiology or an AP affiliate, where serologic studies, PCR, and bacteriologic and virus isolation may be performed. Subsequent vertical flow of highly pathogenic pathogens in the FSSCRPW is depicted in Figure 4.
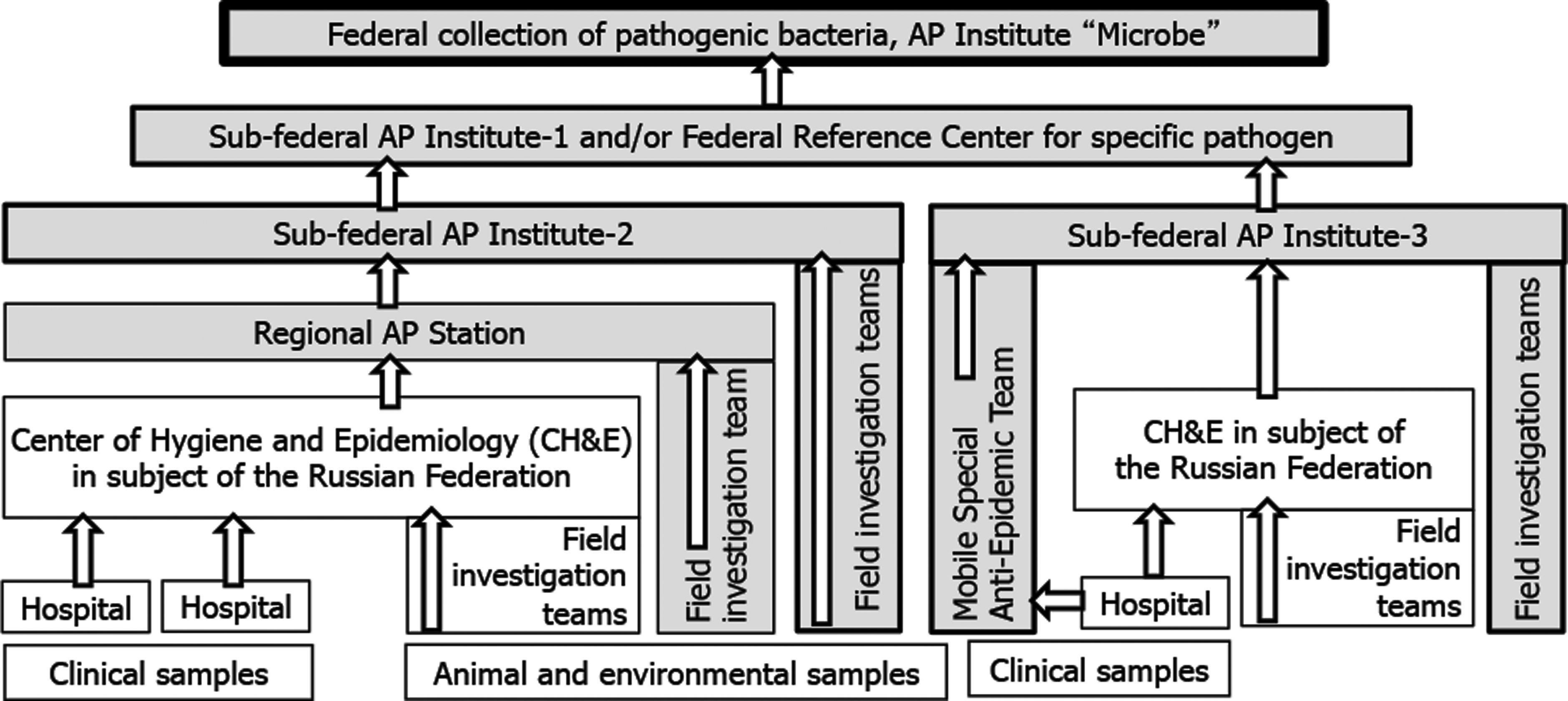
The Flow of Highly Pathogenic Strains in Federal Service for Customers' Rights Protection and Human Well-being Surveillance. (1) Mobile Special Anti-Epidemic Teams operate only in a case of emergency and/or in the regions with scarce diagnostic facilities. (2) Only AP institutions, but not Centers of Hygiene and Epidemiology, are involved in handling and investigation of plague strains. (3) Strains of less pathogenic species may be sent by Centers of Hygiene and Epidemiology directly to Federal Reference Centers for specific pathogens usually operated by the Research Institutes.
Intersectoral Cooperation
The WHO report called for the creation of “intersectoral committees for zoonoses preparedness and control in each country.” 1 (p46) Another strength of the RF system is that it already has effective interdisciplinary bodies at the regional and sometimes federal levels known as emergency committees. Special anti-epidemic and anti-epizootic commissions may be organized by the Russian government or by regional governments of provinces (Oblasts and Republics). 37
Most regional governments have permanent sanitary anti-epidemic and anti-epizootic commissions that include representatives of the local offices of the ministry of health (clinical treatment); Rospotrebnadzor (epidemic control); Rosselkhoznadzor; the ministry of internal affairs (police); the federal security service; the ministry of extraordinary situations; the office of public prosecutor; housing and communal services (waterborne outbreaks); air and railway transport (distant spread of infection); and the ministry of education (outbreaks in schools and universities). Commissions are chaired by a governor of the region or his or her deputy. Such intersectoral committees make immediate and widespread implementation of the epidemiologists' recommendations possible. For example, if the governor imposes quarantine in the region, it will be supported by all of the abovementioned ministries and services. In addition to emergency situations, these commissions meet regularly to coordinate preventive measures.
Defined Responsibilities
Unlike many countries in which jurisdictional issues in a zoonotic outbreak remain unclear, the responsibilities of the Russian authorities are well defined. The course of action is determined by the type of infection and is sanctioned by the province governor. The AP system (as a subordinate of Rospotrebnadzor) can impose a quarantine, order livestock expropriation, introduce other special restrictions in the affected area on a regional level, and promote the organization of anti-epizootic and anti-epidemic emergency committees.
In cases of plague, the AP system, not the ministry of agriculture, is responsible for monitoring the disease in rodents and arthropods. If a case of plague were diagnosed in a camel by the ministry of agriculture, they would report it to the anti-plague station, which would then carry out all field studies, evaluate clinical and pathological materials of suspect cases, and implement anti-epidemic measures. Patients with suspected or confirmed infection are tested, vaccinated, and quarantined.
The responsibilities are distributed similarly if a human case of anthrax is diagnosed. The state sanitary and epidemiologic service conducts a full outbreak investigation with limited assistance from the veterinary service. 36 The most recent equine anthrax outbreak started in the Omsk region in June 2010 and resulted in 6 human cases with 1 fatality. Anthrax strains were isolated from sick horses by veterinarians (Rosselhoznadzor, ministry of agriculture) and the blood of a patient by the Regional Center of Hygiene and Epidemiology, Rospotrebnadzor. The strains were studied by Stavropol API (Russian Reference Center) and were found to be genetically the same. 38
In cases of brucellosis, the ministry of agriculture informs state sanitary and epidemiologic control authorities of livestock cases. The ministry of agriculture undertakes anti-epizootic control measures, but Rospotrebnadzor will, together with specialists from the veterinary service, conduct a field investigation, vaccinate personnel on the farm, perform medical evaluations of people who came into contact with a source of infection, and enforce other anti-epidemic measures. If a human case is detected, Rospotrebnadzor is notified of the emergency within 12 hours. Evaluation of the workplace where the infection occurred is conducted jointly by veterinary and public health personnel. 35
Defined Response Teams
The 2008 WHO/FAO/OIE Joint Consultation on emerging zoonotic diseases recommended that when a new zoonotic agent emerges,
two multidisciplinary teams should be dispatched wherever necessary: one to investigate and contain the human health threat, and the second to investigate the ecology of the agent. Longer-term research should be undertaken to identify all factors contributing to the emergence of the new agent and the scope of the agent's host range, so that appropriate control and prevention strategies can be developed.
1
(p9)
This recommendation describes the combined efforts of the RF anti-plague stations, anti-plague institutes, and mobile sanitary and anti-epidemic teams. Russian authorities consider the teams to be mobile, autonomous, multifunctional, highly technological, modular, safe and are intended for prophylactic, anti-epidemic and sanitary measures in cases of natural or man-made disasters, including epidemics and bioterrorism.14,34,39
The teams are trained to rapidly deploy to an outbreak location. They work at the national, regional, and local levels and, most important, work across the human-animal interface. Sanitary and anti-epidemic teams were founded in 1965 and have been deployed more than 100 times since then. 40
They are multidisciplinary and are composed of epidemiologists, microbiologists, zoologists, entomologists, and other specialists and support staff (Figure S2, supplementary material at www.liebertonline.com/bsp). Each team has a reserve crew waiting at an anti-plague institute if staff need to be replaced. Crews work 24/7 when deployed. 14
The head of a sanitary and anti-epidemic team is always an epidemiologist appointed by the director of the corresponding anti-plague institute. Upon receiving an urgent report, the teams are put on high alert, deployed as full or partial teams, relocated, replaced with a new team, or returned to the permanent base by order of the head of Rospotrebnadzor. Sanitary and anti-epidemic teams are staffed with personnel from the AP system (institutes and stations) and other health professionals that pass the training, which includes 6 months of baseline specialization and regular advanced training at Microbe and Stavropol AP Institutes as well as annual seminars and workshops at their institutes.19,32
Sanitary and anti-epidemic teams coordinate with local authorities and involved agencies; perform epidemiologic reconnaissance, surveillance, analysis, and forecasting of the epidemiologic situation in the area of emergency; organize delivery of samples from people and the environment for research; perform laboratory diagnostics; detect pathogens in the environment; perform laboratory control of food and water for contamination; participate in the development and implementation of anti-epidemic measures including disinfection and rodent and pest control activities; ensure biosafety requirements when conducting diagnostic studies; provide daily reporting; and participate in emergency commissions32,33 (see Figure S3, supplementary material at www.liebertonline.com/bsp).
From 2005 to 2009, automated pathogen identification systems and modern means of securing biosafety were introduced to sanitary and anti-epidemic teams. 14 They now have technical facilities that enable them to function independently of local facilities (Figure S4, supplementary material at www.liebertonline.com/bsp). Five special purpose anti-epidemic teams have been upgraded with new lab equipment. In addition to classic low-tech microbiological and animal-based virological techniques traditionally used by the AP system, they now use ELISA and real-time PCR machines. 40
Today, there are 10 sanitary and anti-epidemic teams. Training of the reserve crews is still in progress but there are approximately 500 to 600 certified sanitary and anti-epidemic team specialists.14,32,41
An example of a sanitary and anti-epidemic team in action is when they were deployed to the republic of North Ossetia on August 9, 2008, immediately after war broke out. On August 10, 6 sanitary and anti-epidemic team vehicles with 24 people arrived at Vladikavkaz and Alahir and on August 11 at Tzkhinval. Team personnel included the director of the institute heading the operations; an epidemiologist (the team head); the deputy head, responsible for logistics; an epidemiologic unit with 2 epidemiologists, 1 zoologist, and 1 sanitary doctor; a bacteriologic unit with 6 doctors, 2 laboratory technicians (also working in the food unit), and 1 disinfection specialist; technical support with 2 engineers (electrician and a diesel operator) and 6 drivers-disinfectors.32,40-43 The situation was fraught with a high risk of zoonotic disease outbreaks, as 100% of households were infested with rodents. Waterborne infections were also a great concern, as only 2 wells were operational. Interruption of waste collection resulted in large groups of scavenging dogs and rodents.
The task of the sanitary and anti-epidemic teams was to prevent an epidemic of enteric and other infections. The first thing the teams did was conduct door-to-door visits to identify infected people. The teams launched PCR, sanitary-hygienic, and bacteriological studies. They also disinfected and monitored the water supply and offered a number of technical solutions to optimize the supply of chlorinated water. Total eradication of rats in Tskhinval was performed, and rabies prophylaxis was administered to the population as needed. Between August 11 and September 3, the team surveyed 78 sites and completed 780 laboratory tests. Through their efforts, spread of enteric infections was stopped and those foci that existed were isolated and eliminated. 43
Weaknesses of the Anti-Plague System
While the Russian AP system has features that are worth emulating, including its integrated approach to zoonoses, well-defined reporting structure, rapid response teams, multidisciplinary training, and fusion centers, it also has weaknesses, partly linked with its advantages. As a bureaucracy, it responds best to known threats but is struggling to impart necessary flexibility to respond to emerging threats. Also, as a vertically organized structure, with vertical transmission of data, information is not always released to the general public in a timely manner. There is no public input into the priorities set by the AP system. In addition, as a “do what you are ordered” system, it requires complete, up-to-date, and consistent legislation for effective performance. For example, current communication between public health entities and the ministry of agriculture is admittedly poor. A key reason for this is that regulations governing the organizations became obsolete because of structural changes as a consequence of administrative reforms. This has yet to be addressed.
Discussion
The Russian public health system has demonstrated the ability to diminish the threat of dangerous zoonoses. There have been no plague cases and only sporadic cases of anthrax and rabies in the past few decades. The incidence rates of brucellosis, Q fever, leptospirosis, and tularemia are stable at fewer than 4 cases per 1,000,000 of population and usually fewer than 2 cases per 1,000,000. This is a real achievement for an economy “in transition” and in a country where practically all rural areas are endemic for a number of zoonotic diseases. The Russian AP system contributed greatly to this achievement and confirmed its usability and sustainability during the century, full of social and epidemiologic challenges. In contrast to most Soviet institutions, it still operates in the modern Russian state.
The Russian AP system was created in a country with many natural foci of zoonotic diseases and therefore may be most applicable to less developed nations in Asia, Africa, and the Middle East, which are similarly challenged and have been the focus of recent zoonotic disease outbreaks. These resource-limited countries often have inadequate or no healthcare facilities. Consequently, these countries do not have adequate domestic disease detection or response capabilities. 44
The Russian experience in emergency response is extremely useful. Rapid response teams have recently been formed in Africa 45 and Asia 46 to address cross-border disease surveillance. In Asia, the Mekong Basin Disease Surveillance (MBDS) network was formed because the lower-income countries in the region had weak health systems, 46 and those weaknesses threatened the entire region. MBDS includes Cambodia, China (Yunnan and Guangxi), Lao PDR, Myanmar, Thailand, and Vietnam. Lao PDR has developed Rapid Response Teams (RRTs), and Thailand has Surveillance and Rapid Response Teams (SRRTs). In 2008, Thailand MBDS responded to a devastating cyclone in Myanmar by forming multidisciplinary rapid response teams that included physicians, psychologists, and environmentalists. While this is progress, many countries in Southeast Asia continue to be resource-poor and have limited infrastructure. 47
In Africa, the East African Integrated Disease Surveillance Network (EAIDSNet) was formed in recognition of the difficulty of responding to disease outbreaks due to fragmented disease interventions and poor lab capacity. EAIDSNet has pulled together cross-border surveillance and response committees that are now in place between Kenya and Tanzania, Kenya and Uganda, and Rwanda and Uganda. There are plans to develop similar response teams between Tanzania and Rwanda, Tanzania and Burundi, and Rwanda and Burundi. 45 However, a field exercise revealed continued weaknesses in coordination of response activities, poor communication, and inadequate biosecurity measures. 45
The RU AP system has extensive and time-proven experience in developing zoonotic disease response systems that is applicable to these regions. Its tradition of education, training, and monitoring are valuable for Africa, Asia, and other epidemiologically active regions. Governments in these parts of the world do not necessarily have well-developed veterinary or public health systems that would be resistant to change. The RF AP system is unique in its multidisciplinary approach, which includes ecologists and biologists with extensive knowledge of animal behavior, biology, and landscape ecology. Could this not serve as an opportunity to take an integrated and multidisciplinary approach to zoonotic threats when building health systems?
It should also be noted that until relatively recently, the AP system functioned with basic, low-tech classic microbiological methods and well-trained personnel, which might suit the fiscal challenges of these areas. 18 Additional strengths of the AP system are a clear and orderly (albeit bureaucratic) system for sample collection, handling, biosafety, reporting of zoonoses, decision making, and distribution of responsibilities; well-defined response protocols that apply to both humans and animals; and specially trained medical and paraprofessional personnel. These might serve as a template for other countries as they try to develop integrated biosurveillance systems.
In conclusion, in times when the world is constantly challenged by a full spectrum of biological threats, it would be improvident to dismiss the rich experience and century-old history of the Russian AP system.
Footnotes
Acknowledgments
This work was undertaken as part of the biological program at NTI, a Washington, DC–based NGO, and we are grateful to the Russian Federation, Central Research Institute of Epidemiology, for hosting the global scholars who contributed to this comparative analysis. For AEP, this work was supported in part by the contract with the Ministry of Education and Science of the Russian Federation No. 14.515.11.0011. We would also like to thank Matthew Finn, NTI intern, for his research and dedicated refinement of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.