
Abstract
On the morning of June 9, 2009, an explosion occurred at a manufacturing plant in Garner, North Carolina. By the end of the day, 68 injured patients had been evaluated at the 3 Level I trauma centers and 3 community hospitals in the Raleigh/Durham metro area (3 people who were buried in the structural collapse died at the scene). Approximately 300 employees were present at the time of the explosion, when natural gas being vented during the repair of a hot water heater ignited. The concussion from the explosion led to structural failure in multiple locations and breached additional natural gas, electrical, and ammonia lines that ran overhead in the 1-story concrete industrial plant. Intent is the major difference between this type of accident and a terrorist using an incendiary device to terrorize a targeted population. But while this disaster lacked intent, the response, rescue, and outcomes were improved as a result of bioterrorism preparedness. This article discusses how bioterrorism hospital preparedness planning, with an all-hazards approach, became the basis for coordinated burn surge disaster preparedness. This real-world disaster challenged a variety of systems, hospitals, and healthcare providers to work efficiently and effectively to manage multiple survivors. Burn-injured patients served as a focus for this work. We describe the response, rescue, and resuscitation provided by first responders and first receivers as well as efforts made to develop burn care capabilities and surge capacity.
An explosion at a manufacturing plant in Garner, North Carolina, resulted in 68 injured patients who were evaluated at the 3 Level I trauma centers and 3 community hospitals in the area. This article discusses how bioterrorism hospital preparedness planning, with an all-hazards approach, became the basis for coordinated burn surge disaster preparedness.
A
An investigation concluded that the explosion resulted from a gas leak. Once the gas leak found an ignition source, the ensuing conflagration and explosion sent a shock wave through the concrete building, causing exterior walls to collapse, crushing cars parked next to the building, and blowing large holes in the ceiling. As these walls and ceiling sections collapsed, they ripped open additional supply lines of gas and ammonia and exposed electrical lines in multiple sections of the building, culminating in a horrific and deadly scene.
The subsequent investigation concluded there had been no purposeful intent, and terrorism was ruled out. Nevertheless, one method of terrorizing a population is to purposefully explode an incendiary device to injure, mutilate, and kill people and to destroy buildings and infrastructure. 1 While this disaster lacked purposeful intent, the response, rescue, and outcomes reflected many of the efforts of the past decade in which terrorism and bioterrorism preparedness had been a priority for emergency responders and the healthcare system.
This article discusses the events that occurred at the industrial plant (identified on Figure 1 as A1 and pictured in Figure 2), the preparedness activities that drove many of the decisions that day, and the outcomes. We will briefly review the care and management of the patients with burn and blast injuries, based on the regional planning and preparedness activities and the potential impact of patient outcomes following the explosion.

The Raleigh Durham metro area is home to 3 large healthcare systems with multiple hospitals. The disaster occurred at point A1. The closest burn center is located at the main campus of UNC Hospitals and Healthcare, identified as H2. The closest Level 1 Trauma Center is WakeMed Health and Hospitals (main campus) identified as H3. Rex Healthcare is identified as H4, Duke Raleigh is identified as H5, WakeMed Cary is identified as H6, and Duke University Medical Center (main campus) is identified as H7. The distance between A1 and H2 was approximately 36 miles and primarily involved interstate highways. (Color graphics available online at www.liebertonline.com/bsp)
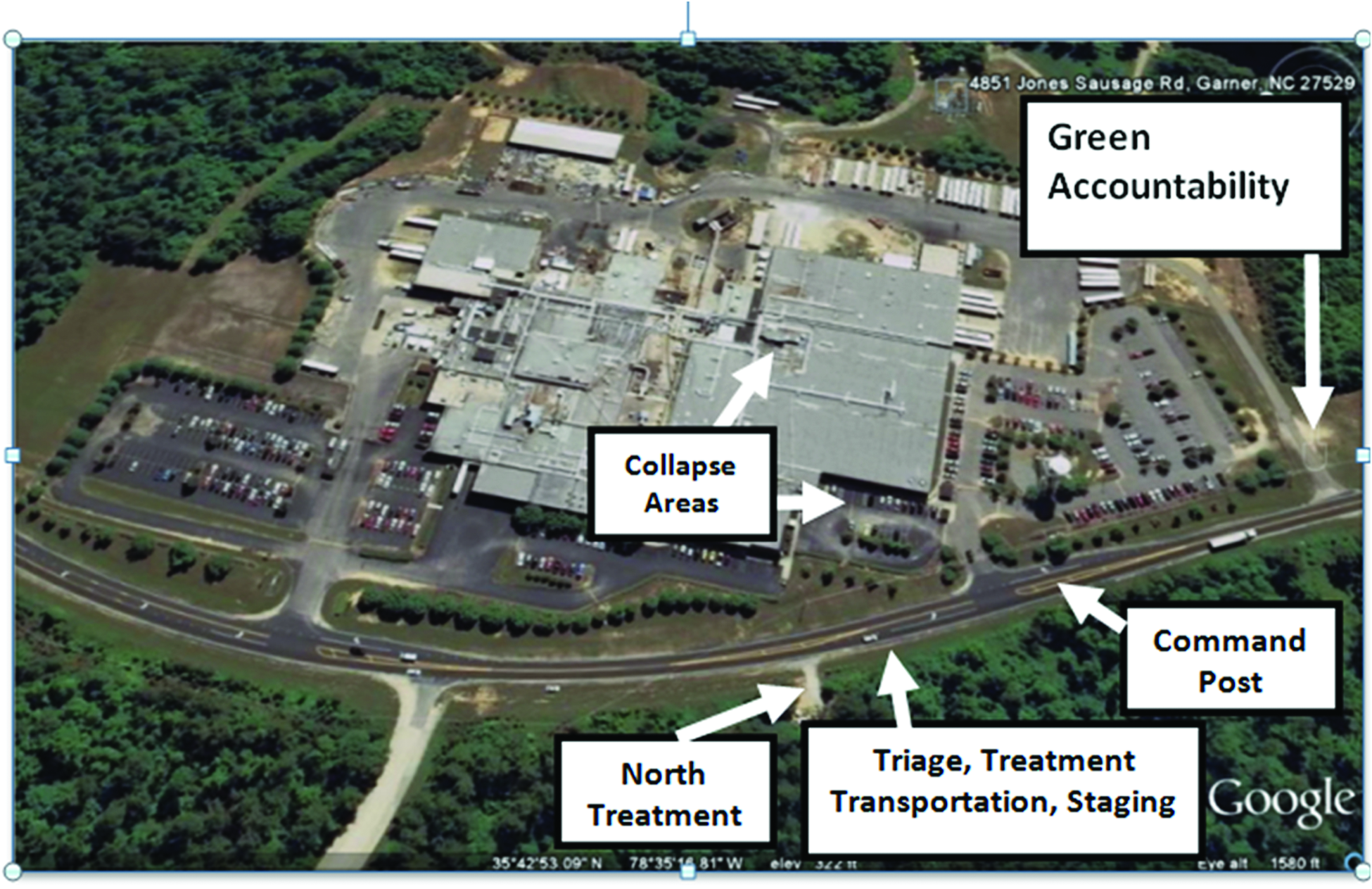
The aerial image capture relied on Google Maps October 2009 of the ConAgra Plant in Garner, NC. The damage is not seen in the image but the areas of interest regarding command, treatment, staging, accountability, and collapse areas are identified with the text boxes. The street in front of the building is Jones Sausage Road, a two-lane connector between Interstate 40 and the town of Garner. (Color graphics available online at www.liebertonline.com/bsp)
Background
Following the September 11 attacks, there was a great sense of urgency to build a more resilient healthcare system capable of responding to and preparing for terrorism and bioterrorism attacks.2,3 The Bioterrorism Hospital Preparedness Program (HPP) was one of the programs aimed at offering national guidance (and financial support) for state and local solutions. 4
Since 2002, multiple planning and preparedness efforts have developed across the nation. These efforts included surge planning and preparedness as a critical component of the HPP in response to a terrorist attack. 4 National funding and guidance for the HPP is provided through the Department of Health and Human Services (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR). Each state administers HPP through either Public Health or Emergency Medical Services (EMS).
The HPP includes burn surge as a component of surge planning. 5 In North Carolina, burn surge planning was developed in conjunction with an array of components developed to create a state medical response system (SMRS). The burn surge program evolved out of this effort to include clinician education, surge planning for EMS agencies, and community and regional hospitals as well as statewide EMS protocols. 6 (Initially, the Bioterrorism HPP began in the Health Resources Services Administration; it was transitioned to ASPR when the latter organization was created in 2006. The name was shortened to HPP.)
The Event
Tuesday, June 9, 2009
At approximately 11:00
Concurrently, the NC USAR Task Force 8 9 was conducting a quarterly training exercise in southern Wake County. This 36-person team includes specially trained regional fire and rescue personnel who are available to respond to particularly difficult rescue situations, such as those occurring with structural collapse. (Their equipment is similar in quantity and quality to that of the Federal Emergency Management Agency [FEMA] designated USAR 10 teams used for large-scale national disasters.11-13 The NC USAR teams were developed following the September 11 attacks, using a Department of Homeland Security [DHS] grant program.)
At 11:27
Callers on the 911 audio recordings pleaded for help, asking for “everything you can send” and specifically describing survivors with burns and orthopedic injuries. 14 The first arriving EMS crews were met by many of the approximately 300 employees who were evacuating the building, fearing additional explosions or that more sections of the large concrete building could collapse.
Cause of the Explosion
Investigators would later determine that the explosion resulted from a natural gas purge that was performed while a hot water heater was being replaced. 15 The purging had occurred intermittently for approximately 2 hours, with the gas eventually finding “one of many ignition sources around 11:25 EDT.” 15 While several safety steps were taken, including cutting off the gas source that directly supplied the water heater, the common practice of using the “sense of smell” to recognize when the gas concentrations had reached unsafe levels did not alert the workers. 15 Once the gas source was shut off, it was believed the residual gas in the line would dissipate into the building. Unfortunately, the concentration of vented gas remained dangerously high until it reached an ignition source.
First Responders/Emergency Medical Services
The first response was led by the Wake County EMS System. 8 The EMS system includes 41 ambulances immediately available for 911 response. In this county, there are an additional 60+ licensed ambulances across all services, with approximately 100 available at peak times and including a medical helicopter and a county AmBus. This agency is also the home for one of the NC Ambulance Strike Teams (including the AmBus) and NC State Medical Assistance Teams, both developed through the HPP program; both were involved in response or manpower supply.
All of these resources fall under the county EMS umbrella for continuity of care, standards of care, and continuity of practice (Table 1). These resources provide a formidable response to a mass casualty incident. 16
First Responders and Emergency Medical Services
Because the train-related activities had occurred less than an hour prior to the explosion, there were multiple agency vehicles still on the road returning to their stations at the time of the Garner explosion. In addition to the medical responders, fire departments, rescue agencies, and various law enforcement officers had responded earlier as well, resulting in a large-scale force that was in the process of demobilizing and on the road.
Given the nature of the explosion alarm and structural collapse and the uncertainty surrounding the cause of the blast (ie, purposeful or accidental), the NC USAR Task Force 8 team left their training exercise and responded to the incident. They arrived within minutes of the explosion and led the search and rescue efforts for missing employees.9,10,17
On-Scene Medical Operations and Triage
The first responders on the scene initially encountered hundreds of distressed workers; they were guided to a makeshift medical evaluation area adjacent to the industrial site (identified in Figure 2). As the triage process began, those who had no identifiable injuries were sorted from those with more obvious medical needs. Several EMS officers assumed a command role in unified command and organized the medical branch of the incident. They coordinated the flow of resources and response activities during the early stages of the response. The physician medical director (for the local EMS system) was one of the first to arrive, and he provided triage oversight with subsequent support of clinical decision making before the injured were transported to area hospitals. 18
It has been our experience that there is considerable downstream success when triage goes well.19,20 When triage does not go well, it can set off a cascade of problems that are difficult to resolve in the midst of a disaster.21,22 Each NC EMS agency is required to have a “triage and destination plan” that includes predetermined destinations, based on HPP guidance, for trauma and burn patients. 23 The county EMS system's mass casualty plan follows the HPP guidance and also reflected the Israeli experience. This includes a focus on minimal on-scene treatment and rapid, coordinated transportation to appropriate hospitals with an emphasis on equal patient distribution when possible.24-27
Ambulance Triage and Transport Decisions
The most critically injured patients were triaged for transport to WakeMed, the closest Level I trauma center to the site of the disaster (shown in Figure 1 as H3). One patient with critical burn injuries, and potential concomitant internal hemorrhage, was triaged first to the closest trauma center for an initial evaluation. The remaining 3 burn-injured patients were transported directly to the closest burn center (at UNC Hospitals, shown in Figure 1 as H2, which is co-located with another regional Level I trauma center). 28
The first 12 patients triaged as either “red tag” or “yellow tag” were transported within the first hour following the explosion. 29 Another 31 “worried well” patients were transported within the next several hours to area hospitals, including Rex Healthcare, a 433-bed hospital also located in the area.30,31 In aggregate, the distribution of injured patients by EMS included approximately 12 to WakeMed, 10 to Rex Hospital (shown in Figure 1 as H4), 11 to WakeMed Cary (shown in Figure 1 as H6), 7 to Duke Raleigh (shown in Figure 1 as H5), and 3 with critical burn injuries to the Burn Center at UNC Hospitals. The EMS phase of the operation ended at approximately 14:30, with the remaining EMS resources converting to a supportive role for ongoing rescue and recovery operations and incident assessment activities. (An additional 24 nonemergency patients presented in the hours or days following the disaster to the various hospitals in the metro area outside of the EMS system. The Chemical Safety Board identified and reported 68 total patients, with 43 known to have been transported by the county EMS system. 15 See Table 2.)
Research Triangle and Raleigh Durham Metro Area Hospitals
First Receivers/Area Hospitals
The 3 Level I trauma centers located within 35 minutes of the scene include WakeMed Health and Hospitals, 32 in Raleigh, Duke University Health System in Durham (shown in Figure 1 as H7), 33 and the University of North Carolina (UNC) Hospitals and Healthcare System in Chapel Hill. 28 UNC Hospitals includes the NC Jaycee Burn Center as well as a Level 1 trauma center. Other community and regional hospitals in the area include Rex Healthcare, Duke Hospital Raleigh, Durham Regional Hospital, WakeMed Cary, WakeMed Apex, WakeMed North (Apex and North are freestanding emergency departments), and Holly Hill Hospital, a Behavioral Health Hospital located adjacent to the WakeMed Raleigh campus.
All of the area hospitals were alerted to the disaster by the State Medical Asset Resource Tracking Tool (SMARTT). SMARTT is a state-based electronic program for tracking bed availability and other resources during a disaster. The creation and ongoing operation of SMARTT is funded through the HPP. The trauma centers and the Raleigh area community hospitals all activated their emergency operations plans and opened their emergency operations centers. Based on disaster planning and preparedness activities they have developed based on the HPP, each was prepared for a surge of patients.
Hospital Status at the Time of Disaster
The morning of the explosion, the burn center had 39 inpatients. Given that there are 36 beds allocated for the care of burn-injured patients, the service line was already functioning in excess of its peak capacity prior to the incident. Excess capacity is routinely managed by admitting additional burn-injured patients to the burn service line but placing them in overflow beds from other specialties that are in physical proximity to the burn center. In this case, a patient's care is still managed by a burn surgeon, but the training of the nursing staff is generally more aligned with postsurgical care or other similar conditions.
This overflow system was already in use when the hospital received alerts at 12:03, 12:05, and 12:10
The morning of June 9 was an otherwise typical morning at UNC Hospitals, with a full operating schedule well under way, a busy emergency department, and an inpatient census that was near capacity. In anticipation of the surge, systems were rapidly operationalized to create additional operating room, intensive care unit, and trauma/burn specialty resources. The 3 ambulances associated with the initial set of alerts arrived at the emergency department between 12:25 and 12:32
Operational tactics that are designed to optimize staffing requirements and bed availability may show signs of failure when a system is unexpectedly stressed by a sudden surge of unanticipated patients.19,34-38 Regional disasters like the Garner explosion can easily overload a healthcare system. This surge can lead to system failure through immediate introduction of multiple high-acuity patients. This threat underscores the need for proactive plans to distribute the surge of patients and ease the associated burdens.39,40
Transport Decisions for the Patients with Burn Injuries
The 3 patients with critical burn injuries were triaged from the scene and sent directly to the burn center, with a fourth going to the nearby trauma center with a potential internal hemorrhage before being transferred later to the burn center. Three additional patients with less severe burn injuries were initially evaluated and managed at an area hospital before subsequently being transferred to the burn center later that evening. A total of 7 patients with burn injuries would eventually be transported or transferred to the burn center in the first 8 hours after the explosion.
Data from the Burn-Injured Patients
Specific patient data for the 7 patients with burn injuries were reviewed (based on UNC IRB 05-1545). This review and analysis involved Burn and Trauma Registry data and relevant EMS prehospital patient care reports. Patient demographic data, initial care provided at the scene, transport destinations, transport times, the total body surface area (TBSA) assessment of the burn injuries, and patient days in the hospital were also included. The review also covered key objectives discussed during the burn surge education programs, compliance with prehospital treatment protocols, adequacy of field TBSA reporting (rule of 9s) when compared to subsequent assessments, initial airway management, oxygen therapy, and pain management prior to hospital arrival as well as patient outcomes.
Results
The disaster occurred in a metropolitan suburb, with 3 Level I trauma centers and 1 burn center located in the immediate area. There were more than 300 employees in the building at the time of the explosion, and, of these, 68 sought medical care. Seven patients suffered burn injuries. Of these 7 survivors with burn injuries, the 3 most critically injured were triaged and taken directly to the region's burn center. Their injuries included TBSA burns ranging from 45% to 57%, and all presented with concomitant inhalation exposure. The 2 intrastate burn centers were evaluating available capacity within 30 minutes of the explosion. In addition, burn centers in neighboring states were contacted regarding their potential capacity within 2 hours of the explosion.
Data
• Of the 71 people in the building at the time of the explosion, 7 suffered some form of burn injury (9.9%).
• Four of those 7 patients also had inhalation injuries (57.1%).
• The 3 patients with critical burn injuries were transported directly from the disaster scene to the burn center, consistent with the triage and destination plan.
• Of the 7 patients, 4 were male and 3 female.
• Ages ranged from 30 to 65 years,
• Total Body Surface Area (TBSA) burn injury=(2%≤×≤52%) and (
• Patient weight at admission in kilograms=(69kg≤×≤110kg) and (
• Length of stay/patient days=(6≤×≤159) and (
Prehospital Interventions
The common approach for all thermal burn injuries in the NC EMS protocols includes airway management/oxygen support, TBSA assessment, fluid resuscitation based on the TBSA assessment, wound management with clean dry dressings, pain assessment/management, and transport directly to the closest burn center where the distance is predetermined to be reasonable by the system medical director. 41
For the 3 patients transferred directly from the scene to the burn center by EMS:
• A TBSA assessment relying on rule of 9s was completed and reported for each patient, 60% to70% TBSA. • An intravenous line was established using 0.9% NaCl solution on all 3 patients (it should be noted this EMS system does not have lactated Ringer's stocked on the ambulances; 0.9% NaCl solution was the available fluid). • Oxygen was administered to all 3 patients by non-rebreather masks at a rate of 12-15 liters per minute (lpm) during transport, and an airway assessment was conducted to determine if an advanced airway should be placed. • Follow-up and ongoing assessments were conducted in the ambulance to reevaluate traumatic injuries, and none were noted. • Pain management assessment was completed on all patients, with all patients reporting pain of 10 on a scale of 1 to 10. • Morphine sulfate (MS) was administered intravenously to 2 patients, who each received a total of 15 mg during transport. The third patient had IV access complications, and the MS was delayed until arrival at the hospital.
Burn Center Arrival Times
The 3 most critical patients arrived at the burn center between 12:25 and 12:32
Activity in the Emergency Department
The 3 critically injured patients who were transported directly from the scene to UNC Hospitals were seen in the emergency department and transferred to the burn center within 45 minutes of arrival. Their continued care included reassessing for traumatic injuries, airway assessment, changing fluids to lactated Ringer's solution, inserting a Foley catheter for all patients, obtaining a tetanus history, and wound management including monitoring core body temperatures.
Activity at the Burn Center
All surgeons who cover for the burn center service line, including the 4 physician assistants and 2 residents, were notified. Trauma surgeons were also notified of the incident and incoming alerts. An operating room was made available and held, and available trauma ICU, flex, and step-down beds were identified.
All 3 of the critical patients were in the burn center and undergoing lifesaving care within 45 minutes of arrival. This care included airway management, resuscitation efforts, and surgical debridement including escharotomies and fasciotomies. The fourth patient with burn injuries, who had initially been seen at the nearby trauma center, arrived within 3 hours of the blast.
The burn center includes a 21-bed dedicated intensive care unit and an additional 15-bed acute burn and wound care unit. This is a busy burn center, and the staff are accustomed to an ever-changing census. This includes triaging burn admissions and caring for patients and sometimes relying on beds and resources in areas of care adjacent to the burn center. All burn patients requiring resuscitation or with special burn care needs are admitted to the burn ICU. The morning of the explosion, every burn ICU bed was occupied. Upon notification of incoming patients and a potential burn mass casualty incident, nursing administration and bed coordination worked to determine bed availability. Three burn ICU beds were cleared, with multiple crews from housekeeping, central supply, and equipment playing key roles in cleaning and preparing the rooms for new patients.19,42
A distinct challenge with critically injured burn patients is the length of stay and long-term care requirements. The 3 most critically injured had average initial inpatient stays of 121 days each, totaling 362 patient days, before discharge (1 patient expired). The long-term impact on staff following large disasters has been discussed before and remains an important consideration when weighing the need to keep or transfer patients in the hours and days following a burn disaster.34,43
Nursing, respiratory, and other support staff were asked to discuss splitting shifts and surging to assure coverage during the days and weeks that would follow the surge of patients. Historically burn disasters have created staffing instability, and it was essential to keep the staffing hours reasonably distributed to avoid this problem experienced by others. 43
Discussion
The bioterrorism HPP originally focused on surge capacity and building capacity for scarce resources, including pediatric, trauma, and burn care, in response to a terrorist attack.44,45 Managing burn injuries in the context of a greater disaster was envisioned as a significant threat. While this disaster lacked intent, the balance of the concerns played out in this scenario.
When the state burn surge disaster plan was created, organizers recognized that there was a greater issue than capacity that would undermine any programmatic success if left unaddressed. 34 Unlike the case for blunt and penetrating trauma, a distinct undertone of discomfort existed for non–burn facilities to manage even a single burn-injured patient for any extended period of time. 5 During initial meetings conducted around the state to invite stakeholder input on the details of a potential plan, it was determined that any successful effort would have to include a component of burn care education. 46
Conclusions
The statewide bioterrorism planning efforts included plan development, extensive statewide education, revision of statewide EMS protocols and destination guidelines, and regional hospital coordination. All of these efforts contributed to an effective response and positive patient outcomes. Time on scene and in transit, care in transit, time in the ER, and entry into the burn center were optimized and better than those reported with previous disasters.
The county EMS system is operationally and clinically an outstanding organization. For this disaster, components of local and state planning and preparedness efforts played out effectively. The successes reflect the local, state, and national efforts to create a more resilient and prepared healthcare system.
Given the total resources in the region, and the size and scope of this disaster, this was a small event. Nevertheless, there were valuable lessons that have broad application for future disasters, including managing the flow of vehicles on a 2-lane road, such as the one in front of the industrial plant, to reflect the need for ambulances to leave with patients and while more fire, rescue, and emergency resources were arriving.
While this explosion was not an act of terrorism, the same elements, other than intent, were present. It should be noted that this disaster occurred in a jurisdiction in which the stakeholders in medical disaster response (EMS, community hospitals, trauma and burn centers) are accustomed to working closely with one another and have been actively involved in the medical disaster planning process. Nevertheless, early in the disaster it was clear it would challenge everyone involved. Early notification of adjacent burn centers to determine capacity aided decision making at the burn center where casualties were initially received. The high survival rate was a product of excellent initial EMS care and triage decisions and outstanding medical care provided at all of the area hospitals.
While this was not a large disaster in terms of total patient numbers, the elements involved were significant. From an explosion involving 300 people and a concrete building to a wide array of injury patterns, this was catastrophic for those injured and their families. The outcomes also affirm that preparedness and planning make a difference.
Footnotes
Acknowledgments
Thanks to the related healthcare systems and data registry systems for providing relevant patient care information. Vehicle counts and system demographics were derived from the Emergency Medical Services, Performance Improvement System (EMSPIC). This work is supported in part by the US DHHS/ASPR HPP Grant CDC-RFA-TP12-1201 through the NCOEMS Contract 00027162. This support also includes educational programs through FEMA Grant EMW-2011-FP-01131.