
Abstract
During routine screening in 2011, US Customs and Border Protection (CBP) identified 2 persons with elevated radioactivity. CBP, in collaboration with Los Alamos National Laboratory, informed the Food and Drug Administration (FDA) that these people could have increased radiation exposure as a result of undergoing cardiac Positron Emission Tomography (PET) scans several months earlier with rubidium Rb 82 chloride injection from CardioGen-82. We conducted a multistate investigation to assess the potential extent and magnitude of radioactive strontium overexposure among patients who had undergone Rb 82 PET scans. We selected a convenience sample of clinical sites in 4 states and reviewed records to identify eligible study participants, defined as people who had had an Rb 82 PET scan between February and July 2011. All participants received direct radiation screening using a radioisotope identifier able to detect the gamma energy specific for strontium-85 (514keV) and urine bioassay for excreted radioactive strontium. We referred a subset of participants with direct radiation screening counts above background readings for whole body counting (WBC) using a rank ordering of direct radiation screening. The rank order list, from highest to lowest, was used to contact and offer voluntary enrollment for WBC. Of 308 participants, 292 (95%) had direct radiation screening results indistinguishable from background radiation measurements; 261 of 265 (98%) participants with sufficient urine for analysis had radioactive strontium results below minimum detectable activity. None of the 23 participants who underwent WBC demonstrated elevated strontium activity above levels associated with routine use of the rubidium Rb 82 generator. Among investigation participants, we did not identify evidence of strontium internal contamination above permissible levels. This investigation might serve as a model for future investigations of radioactive internal contamination incidents.
During routine screening in 2011, US Customs and Border Protection identified 2 people with elevated radioactivity. They informed the FDA that these people could have increased radiation exposure as a result of undergoing cardiac Positron Emission Tomography (PET) scans several months earlier with rubidium Rb 82 chloride injection from CardioGen-82. The authors conducted a multistate investigation to assess the potential extent and magnitude of radioactive strontium overexposure among patients who had undergone Rb 82 PET scans. This investigation might serve as a model for future investigations of radioactive internal contamination incidents.
I
The rubidium Rb 82 generator (CardioGen-82) produces radioactive rubidium-82 (Rb-82), which may be infused into patients for myocardial perfusion imaging. Because of Rb-82's short half-life, it must be produced using the rubidium Rb 82 generator at the imaging site. The generator has strontium-82 (Sr-82) adsorbed onto a stannic oxide column, which decays into Rb-82 and is eluted shortly before administration. The column also contains strontium-85 (Sr-85), a byproduct from the manufacture of Sr-82. During normal generator operation, a small amount of Sr-82 and Sr-85 may be present in the Rb-82 chloride eluate for injection—a phenomenon known as strontium breakthrough.1,4 The US Nuclear Regulatory Commission (US NRC) and Agreement States 5 regulate these concentrations and have set permissible limits during administration to a ratio of no more than 0.02 kiloBecquerel (kBq) of Sr-82 per megaBecquerel (MBq) of Rb-82 and 0.2 kBq of Sr-85 per MBq of Rb-82. 6 To monitor the amount of strontium breakthrough for each generator, nuclear medicine technologists are expected to perform manufacturer-outlined quality control and assurance procedures daily. 1
The estimated committed effective dose from an Rb 82 PET scan is up to 13.5 millisieverts (mSv); in comparison, the estimated effective dose from a typical chest x-ray, by some estimates, is 0.02 mSv. 7 Any unnecessary exposure to radiation is undesirable. 1 Exposure to higher doses of radiation due to excess breakthrough may increase cancer risk, since this represents a radiation dose that is in excess of routine Rb 82 chloride injections for PET scanning. 3 While Rb-82 has a short physical half-life of 75 seconds, Sr-82 has a half-life of 25 days and Sr-85 has a half-life of 65 days. 4
The FDA determined that higher-than-permissible levels of strontium breakthrough may have occurred in the people initially identified by CBP. In July 2011, the FDA reported that the manufacturer was voluntarily recalling the rubidium Rb 82 generator from the US market.1,8 The FDA did not know whether widespread strontium breakthrough above permissible levels and resultant strontium overexposure had occurred at other US clinical sites that performed Rb 82 PET scans.
Our investigation's objective was to assess the magnitude (ie, dose related to strontium breakthrough) and extent (ie, determine whether excessive strontium breakthrough had occurred at different clinical sites) of internal contamination with radioactive strontium in people who underwent Rb 82 PET scans between February 2011 (corresponding to the period of time during which people identified by CBP received their PET scans) and July 2011 (when the product was voluntarily recalled by the manufacturer).
Methods
Study Design
Between October and November of 2011, we conducted a multistate, multicenter investigation. The selection of states and clinics represented a convenience sample based on interest in participation in the investigation, Rb 82 scan usage information, and public health and radiation protection capacity to conduct the investigation. The states that ultimately agreed to participate were Alabama, Florida, Pennsylvania, and Tennessee. Using state licensing records, state health officials identified potentially eligible clinics; clinical sites performing fewer than 20 Rb 82 PET scans from February through July 2011 were excluded. None of the clinics that participated in the investigation had reported incidents of strontium breakthrough to their state radiation licensing programs.
We used participating clinical site records to identify eligible participants, defined as people who had had Rb 82 PET scans between February and July 2011. Because of the large number of eligible participants in Florida, Tennessee, and Alabama, we used a random number generator to generate a random-order list of eligible participants and enrolled a quota that was based on the resources available to the investigators in each state. Because of the small number of eligible participants in Pennsylvania, everyone receiving Rb 82 PET scans between February and July 2011 was contacted to inquire about enrolling in the investigation.
Either state health officials or CDC personnel obtained informed consent for participation and enrolled 308 participants from 8 clinics in the 4 states. From a combination of interviews and clinic record reviews, we collected participant data, including demographic characteristics and Rb 82 PET scan procedure information such as date of procedure and total Rb-82 dose. The information that was collected regarding participation in the investigation included the total number eligible for the investigation at each clinic and the total number enrolled in the investigation at each clinic; using these data, the proportion of enrolled out of the total eligible at each clinic was determined.
Radiation Assessment
The investigation protocol involved a combination of radiation detection methods. Drawing on resources available in the state, all participants received portable, direct radiation screening. Lanthanum bromide radioisotope identifiers were used in Alabama, and high-purity germanium radioisotope identifiers were used in the other 3 states. Additionally, the laboratory at CDC's National Center for Environmental Health developed a urine bioassay method for detection of radioactive Sr-85 during the investigation. Investigation personnel requested urine samples (≥70 cc) from consenting participants at the direct radiation assessment visit. These urine samples were shipped to CDC for the detection of radioactive strontium isotopes by a high-purity germanium gamma detector using 3-hour count times with a 50-mL geometry for Sr-85. For the majority of urine samples, analytical results were batched by state, and minimum detectable activities (MDAs)—ranging from 2.4 to 2.8 Bq/L—were calculated for each batch. In the case of 1 sample, analysis occurred significantly earlier than for the remainder of the samples from that state. The MDA for that sample was determined separately (2.5 Bq/L).
Participants selected for whole body counting (WBC) were from the states with individuals who were identified with direct radiation results that were at least twice the level of background measurements at 514 keV. A rank-ordering of direct radiation screening results was developed for all participants from these states. Participants were contacted in descending order, starting at the highest screening results. Ultimately, 23 people consented to whole body counting at Oak Ridge (TN) National Laboratory. Figure 1 shows a flow chart of the various investigation steps.
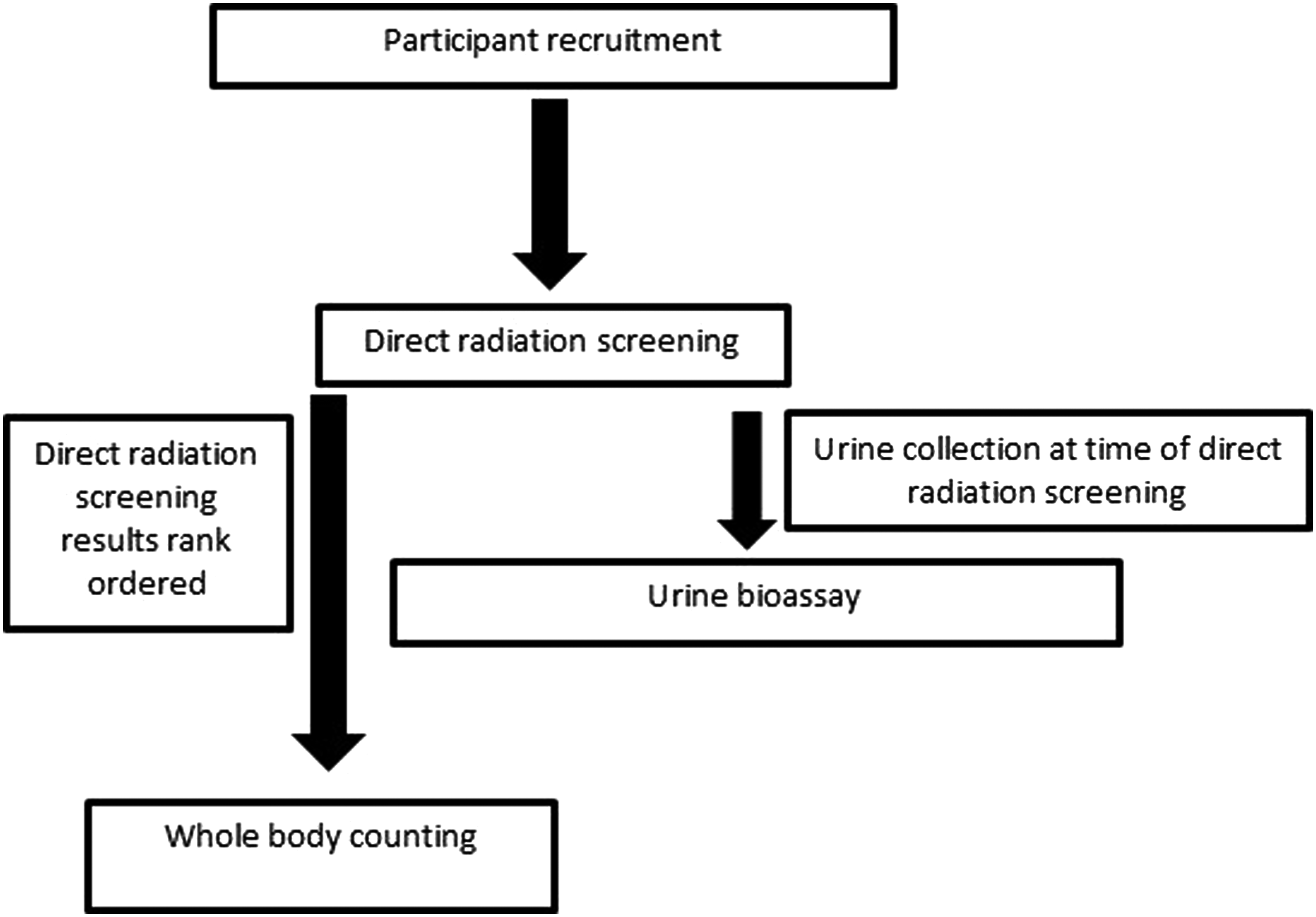
Flowchart of Rb 82 PET Scan Investigation
Statistical Analysis
We used descriptive statistics to summarize demographic variables, Rb 82 PET scan procedure and generator information, direct radiation screening results, urine bioassay results, and data regarding Sr-85 activity, including the estimated committed effective dose, for people who underwent WBC. The median number of days (and range) from date of Rb 82 PET scan to date of interview was determined, as was the median number of days (and range) from date of Rb 82 PET scan to date of WBC. Measured Sr-85 activity for the participants who underwent WBC was evaluated relative to the number of days from date of Rb 82 PET scan to date of WBC. To analyze the relationship between the log (Sr-85 activity at time of whole body counting) and the time (in days) between the original Rb 82 PET scan and whole body counting, Spearman's correlation test was performed. Analyses were performed using SAS 9.3 (SAS Institute, Cary, NC) and Excel 2010 (Microsoft, Redmond, Washington).
Results
Between October and November 2011, we enrolled 308 participants who met the investigation eligibility criteria. Participants were from 8 clinical sites in Alabama (n=51), Florida (n=119), Pennsylvania (n=31), and Tennessee (n=107). The percentage of enrolled participants compared to the total number of people who had undergone Rb 82 PET scans during the period of interest at each of the clinical sites ranged from 3% to 40% at the 8 clinical sites. Table 1 provides demographic characteristics for study participants overall, as well as stratified by state. The median participant age was 68 years (range 35-90) at time of enrollment, 52% of whom were male. Rb 82 PET scans were performed using a median Rb-82 infusion dose of 3.1×10 9 Bq (Table 2). The median time between the participants' Rb 82 PET scan to date of interview was 166 days (range 75-262 days).
Study Participant Demographics, Total and by State, Rb 82 PET Scan Investigation
Rb 82 PET Scan Total Infused Rb-82 Dose, Whole-Body Count Measured Sr-85 Activity, and Estimated Committed Effective Dose from Sr-85
Note. 1 MBq=1,000,000 Bq.
Source: clinic records.
Source: WBC.
Source: calculated from WBC results.
Direct Radiation Screening
Of 308 participants, 292 (95%) had direct screening results that were indistinguishable from background as established at each investigation site in the 514 keV region of interest. Sixteen participants, from Florida and Tennessee, had levels above twice the level of background measurements. The highest net radiation measurement among all participants was 55.4 counts per minute (cpm) at 514 keV using a high-purity germanium isotopic detector with a relative efficiency of 13% to 14% (Ortec Detective EX, Advanced Measuring Technology, Inc., Oak Ridge, TN).
Urine Radiobioassay Analysis
Of the 265 participants (86%) providing an adequate urine sample, 261 (98%) had urine Sr-85 radiobioassay results below the minimum detectable activity (MDA) level for the bioassay method. Urine bioassay identified 4 persons (1.3%) at or above MDA. The highest urine bioassay result was 5.7 Bq/L, while the remaining 3 (range 2.5-2.7 Bq/L) were at, or just above, MDA. The person with the highest urine bioassay result was also the person with the highest direct screening result (55.4 net cpm). Of 23 individuals undergoing WBC, 21 had sufficient urine for bioassay, and only 1 of these 21 individuals had a urine bioassay result above MDA. This individual also had the highest urine bioassay result (5.7 Bq/L).
Whole Body Counting
Twenty-three participants consented to and underwent WBC. The median time between the participants' Rb 82 PET scan to date of WBC was 207 days (range 110-262 days). All 23 participants were below MDA for Sr-82 (Sr-82 MDA range: 419-711 Bq). Twenty-one (91%) had detectable Sr-85 activity. Among these 21 participants, the median activity of Sr-85 was 92.1 Bq, (range 57.4-4824 Bq) and the median estimated committed effective dose from Sr-85 was 0.005 mSv (range 0.001-0.5 mSv) (Table 2). Additionally, bone marrow and bone surface represented the 2 organs/tissues that received the highest estimated committed equivalent doses from Sr-85. The median estimated committed equivalent dose from Sr-85 to bone marrow was 0.0127 mSv (range 0.00354-1.29) and to the bone surface was 0.0125 mSv (range 0.00349-1.28) (Table 2).
The amount of detected Sr-85 activity did not appear to correspond with having undergone WBC closer to the date of the Rb 82 PET scan. The highest Sr-85 activity was recorded in a person who underwent WBC 251 days after Rb 82 PET scan. The lowest detectable Sr-85 activity was recorded in a person who underwent WBC 214 days after Rb 82 PET scan. The 2 people for whom no Sr-85 activity was detectable had undergone WBC 162 and 175 days after the Rb 82 PET scan. The Spearman's correlation coefficient for the relationship between log (Sr-85 activity) and days from Rb 82 PET scan to WBC was 0.27 and nonsignificant (p=0.21).
Using the total Rb-82 activity infused and the participant's scan date, the highest Sr-85 to Rb-82 infusion activity ratio was approximately 0.20 (0.197 kBq Sr-85/MBq Rb-82). Of note, this person was at, but not above, the NRC permissible limit for infused Sr-85 dose and was the person with the highest results for direct radiation screening and urine bioassay result. When considering all 3 modalities, among these 21 participants, only 1 had direct radiation screening greater than twice background, a detectable urine bioassay, and detectable Sr-85 activity by WBC.
Discussion
The radiation assessment protocol developed for this investigation involved a combination of direct measurements using isotope identifiers, urine bioassay methods, and whole body counting. This was due to the fact that while WBC is a highly accurate method for determining internal contamination with some radionuclides, there are logistical challenges associated with arranging for WBC. 9 Approximately 5 nonoccupational clinical facilities in the country accept patient referrals for WBC; therefore, we needed to balance the risks and benefits of transporting an elderly population for this specialized test. In addition, the types of isotope identifiers varied among the participating states, and isotope identifiers can vary in resolution. 10 Also, the states and clinics selected represented a convenience sample of sites interested in participating and with the capacity to conduct the public health and radiation protection investigation. These factors were important since it was necessary to conduct the investigation rapidly, using the resources at hand. Of note, because of the potential limitations with direct screening and limited availability of WBC, the urine strontium radiobioassay served as an alternative method to assess internal contamination that could be more feasibly deployed to a larger population. Among the individuals referred for WBC, only 1 person had a urine bioassay result above MDA, which limits the ability to correlate urine bioassay and WBC results. Also, other investigations occurred at the sites where the original people identified by CBP with elevated radioactivity had undergone Rb 82 PET scans.2,11 The sites in our investigation had not previously reported incidents of strontium breakthrough to their state radiation licensing programs. As such, our investigation could be viewed as complementary to these other investigations.
Another recent example of a multicomponent radiation screening algorithm was the one developed by CDC and its partners following the March 2011 earthquake and tsunami in Japan that resulted in a core meltdown at the Fukushima Daiichi Nuclear Reactor Complex. In conjunction with CBP partners, a screening algorithm was developed to supplement CBP's standard monitoring methods. In this enhanced protocol, individuals found by screening to be above a prespecified screening threshold underwent external decontamination and repeat radiation rescreening. Immediate notification of state radiation control staff occurred if screening remained ≥20×background counts. Otherwise, for radiation counts less than 20×background, follow-up could occur with state public health and radiation control officials at the traveler's destination. During that follow-up, interventions could include collection of epidemiologic data and, if necessary, repeat radiation screening and collection of urine for bioassay. Using this multimodal screening protocol, between March 23 and April 30, 2011, approximately 543,000 passengers were screened, and no individuals were identified with contamination levels warranting public health action. 12
With these considerations in mind, this study did not identify any participants with strontium internal contamination above permissible limits. Using direct radiation screening and urine bioassay, measurements from a majority of participants were either indistinguishable from background radiation levels or below MDA, respectively. Among the subset of participants referred to WBC, the participant who had the highest direct screening, highest urine bioassay result, and highest estimated committed effective dose from Sr-85 by WBC was at, but not above, the NRC Sr-85 to Rb-82 infusion ratio limit.
The negative findings of this investigation are reassuring given that, by some estimates, 45,000 Rb 82 PET scans are performed annually. 3 It is important to consider that alternative nuclear cardiac imaging tests, such as a thallium scan, may be associated with a higher radiation dose to the patient than that associated with routine Rb 82 PET scans. 3 While a larger sample size may have increased the likelihood of identifying individuals with substantially higher Sr-82 or Sr-85 activity, the time required to enroll additional participants needed to be considered given the continuous decay of radioactive strontium. At the onset of the investigation, we hypothesized that, due to its shorter half-life, Sr-82 would not likely be detected among participants and that if a radioisotope were detected, it would more likely be Sr-85. The median time from the Rb 82 PET scan to direct radiation screening of 166 days corresponded to over 6 half-lives of radioactive decay for Sr-82 and fewer than 3 half-lives of radioactive decay for Sr-85. Further, there is a natural peak in the background spectrum of all detectors used in this study at the exact energy of the gamma emission associated with Sr-82 (511 keV), which makes all of the detectors less sensitive to the signal from Sr-82. 13 Consistent with this information, the radiation assessment methods employed identified the Sr-85 isotope, but not Sr-82. During future radiation-related public health investigations, it is important to remain cognizant that detection of radioisotopes becomes more challenging when multiple half-lives have elapsed from the time of presumed radioisotope exposure for the isotope under investigation.
In December 2011, the US NRC reported that potential medical events occurred at the clinical site where 1 of the 2 index patients had received the CardioGen-82 PET scan. 14 The US NRC and Agreement States use the term medical event to describe potential problems in a medical facility's use of radioactive materials that require further investigation but do not necessarily indicate patient harm. 15 Medical events, however, may serve as a marker for the frequency with which potential problems occur with radioactive materials used in medical facilities. Between 2002 and 2011, 421 nationally reportable medical events have been related to errors in which patients received an unintended radiation dose or a complication related to receipt of a radioactive substance. 11 With this in mind, the investigation reported here also can serve as a model for future radiation-related epidemiologic investigations that involve internal contamination with gamma-emitting radionuclides. The collaboration between public health and radiation protection health officers allowed for rapid collection of both epidemiologic and radiologic measurement data. We conducted the investigation in multiple states and at clinics other than the clinical sites of the original cases detected by CBP. That a random selection of states and clinics was not performed needs to be kept in mind when considering the applicability of these results to other US sites. The use of WBC to confirm the results of direct screening and urine bioassay in a subset of participants provided a highly accurate standard reference method for internal contamination by which to extrapolate results to participants who did not have WBC. Given that, in this investigation, both urine bioassay and direct screening identified the participant with the highest level of internal contamination with radioactive strontium, further study into the use of combination radiation screening with urine bioassay and direct screening should be performed. Such combined screening may permit a less resource-intensive method by which to identify the highest risk participants and those to consider for WBC referral in future radiologic investigations—similar to what has been described following large-scale radiation emergencies. 16
With the previously mentioned caveats in mind and based on the results from direct radiation screening, urine bioassay, and WBC, we did not identify people with Sr-85 internal contamination above what might be expected and permissible with Rb 82 PET scans. Although we did not find any evidence of Sr-82 internal contamination, we could not exclude the possibility of Sr-82 exposure associated with the Rb-82 chloride injection due to its shorter half-life. While not representative of the entire population of people who received a Rb 82 PET scan nationally during the study period, our multisite, multistate investigation did not identify any individuals with evidence of Sr-85 internal contamination above permissible levels. Thus, the investigation provided reassurance to participants and public health officials that widespread excessive strontium exposure had not occurred. The ability to conduct this investigation in a rapid fashion, using collaborative state and federal personnel and resources, as well as radiation control and public health expertise, provides a model for conducting future radiation-related public health investigations.
Footnotes
Acknowledgments
The authors thank Cindy Chiu, Andres Espinosa-Bode, Colleen Martin, Michelle Podgornik, Lynn Evans, Carol McCurley, Kevin Caspary, Adam Pomerleau, Ziad Kazzi, Shannon Sullivan, Charles Dodson, Kathleen Caldwell, Judith Qualters, Jeffrey Nemhauser, Michael Gronostaj, Megan Casey, David Allard, Tim Jones, Patricia Eachus, Julie Cobb, Claude Ouimet, David Turberville, Myron Riley, Cason Coan, Nick Swindall, Sarah Matthews, David McLaughlin, Mathew Hayes, Sean Kice, Kathy Brown, John Lott, and all other colleagues at the Alabama, Florida, Pennsylvania, and Tennessee local health departments who assisted in this investigation. Funding was provided by the National Center for Environmental Health, Centers for Disease Control and Prevention. The opinions expressed by the authors do not necessarily reflect the opinions of the Centers for Disease Control and Prevention.